Despite advances in medicine, pneumonia remains a major cause of morbidity and mortality. It affects six million American adults each year. With a mortality rate of 13.4 per 100,000, it is the sixth most common cause of death in the United States (1). Community-acquired pneumonia (CAP) in previously healthy individuals is caused by bacteria in 25% of patients, atypical pathogens (including mycoplasma) in 25%, and viruses in 20%. A few percent more feature multiple causative organisms, but many patients are treated without conclusive evidence.
In hospitalized adults with pneumonia, 60% to 80% are due to Streptococcus pneumoniae, up to 20% are caused by gram-negative bacteria, a few percent result from Staphylococcus aureus, and the remainder are due to viruses and Mycoplasma. For nosocomial or hospital-acquired pneumonia, gram-negative organisms are responsible for 35% to 40%, S. pneumoniae for 10%, S. aureus for 3%, and no agent is identified in approximately 40%.
The diagnosis of pneumonia is based on a combination of clinical history and examination, serologic tests, and diagnostic imaging (2,3,4,5,6) (Boxes 5.1 and 5.2). It is usually not possible to identify the etiology based on clinical or radiologic findings alone. Serologic tests require a few days. It is therefore important that the clinician and radiologist work together, pooling information and resources to narrow the differential diagnosis. The radiologist’s role is to detect abnormality, define its location and extent, evaluate for complications, and monitor response to therapy. As in most clinical settings, the radiologist is significantly aided by having relevant clinical information.
Box 5.1: Common Features of Bacterial Pneumonias
· Respiratory symptoms predominate
· Acute onset of symptoms
· Focal signs on clinical examination
· Correlation between clinical and radiologic findings
· Pathologic changes in a focal area or areas of lung parenchyma
Box 5.2: Features of Atypical and Viral Pneumonia
· Systemic symptoms predominate over respiratory symptoms
· No response to usual antibiotic therapy
· Discrepancy between the severity and location of clinical signs and radiologic findings
· Pathologic changes mainly in the bronchial tree and interstitial parenchyma
Clinical Clues to the Cause of Pneumonia
Accurate early treatment is important in many of the bacterial pneumonias if complications (and even death) are to be avoided. The choice of an appropriate antibiotic rests on the radiologic and clinical findings. Several factors help to narrow the diagnostic possibilities. Patient age is one such factor. Viruses are the usual cause of pneumonia in children. Mycoplasma occurs mainly in children and young adults. Bacteria most commonly cause adult pneumonias.
Clinical symptoms can also be useful. An acute history of productive cough, pleuritic chest pain, and chills is characteristic of bacterial pneumonia (7). On physical examination, focal signs are often present, and there is a high incidence of radiologic findings. In atypical pneumonias systemic symptoms such as fatigue, malaise, arthralgias, and low-grade fever predominate, with a more gradual onset (8). There is often a discrepancy between the clinical and radiologic findings.
Predisposing factors may point to specific organisms. Alcoholism, dementia, neuromuscular disease, swallowing disorders, and general anesthesia predispose to aspiration pneumonia. Anaerobic organisms, gram-negative bacteria, and S. aureus are most often isolated. Chronic obstructive pulmonary disease (COPD) exacerbations are often caused by Hemophilus influenzae or Branhamella catarrhalis. Pneumonia complicating influenza is often caused by S. aureus. S. pneumoniae is common in sickle cell disease and in patients who have previously undergone splenectomy. Pseudomonas aeruginosa and S. aureus are commonly responsible agents in cystic fibrosis. Immunocompromised patients are considered separately in Chapter 6.
Imaging Modalities
Chest radiographs (CXR) are the first line of defense and the mainstay for imaging suspected pneumonia. If pneumonia is confirmed clinically and radiologically, therapy is generally begun. In elderly patients and heavy cigarette smokers, follow-up CXR is advised to complete resolution of disease, thereby excluding postobstructive pneumonia. Radiologic resolution may lag behind clinical improvement by as much as 6 to 8 weeks (and even longer in elderly and COPD patients). Ultrasound can be used to evaluate pleural opacity seen on CXR. The largest areas of pleural fluid can be marked radiologically for aspiration.
Radiologic resolution of bacterial pneumonia often takes 6 to 8 weeks.
Chest computed tomography (CT) can be helpful in patients with pneumonia that resolves too slowly or fails to resolve. A small mass may be obscured by obstructive atelectasis on CXR. CT is better at detecting small calcifications and enlarged intrathoracic nodes. CT with contrast enhancement helps to differentiate lung abscess from empyema when CXR is equivocal.
Radiologic Signs of Pneumonia
Opacification
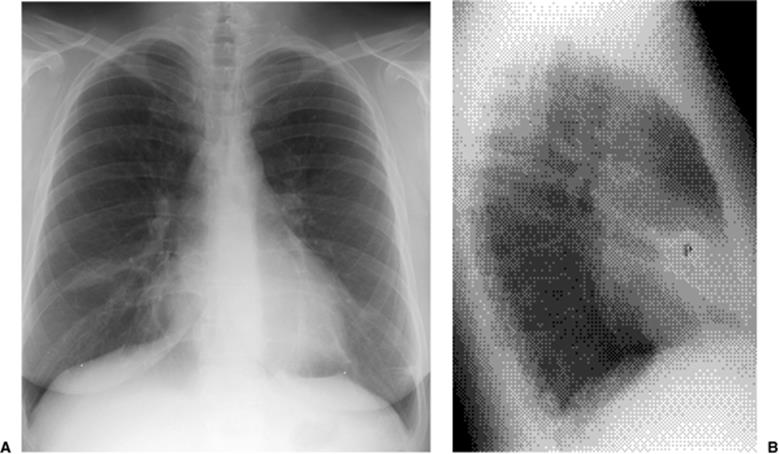
Focal opacity may be visible, especially when comparing one lung with the other on the frontal projection. On the lateral projection attention should be directed over the thoracic spine, the cardiac silhouette, and the retrosternal and retrocardiac regions, where faint opacity may otherwise escape detection (Figs. 5.1 and 5.2).
|
|
|
Figure 5.1 Opacity in pneumonia. (A) Posteroanterior and (B) lateral chest radiographs: minimal right basilar opacity, much better seen on the lateral view overlying the heart (P). |
|
|
|
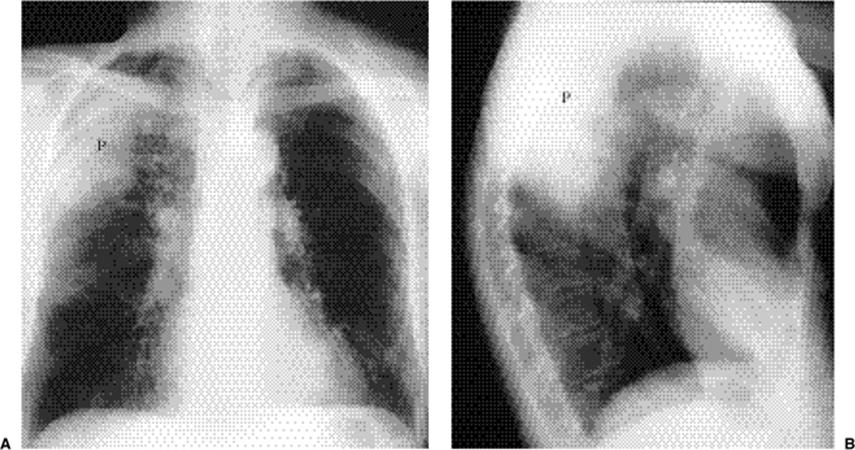
Figure 5.2 Opacity in pneumonia. (A) Posteroanterior and (B) lateral chest radiographs: vague retrocardiac abnormality (P) with corresponding increased opacity over the lower thoracic spine on the lateral view (arrows). |
|
|
|
Figure 5.3 Silhouette sign of middle lobe pneumonia. A. Posteroanterior chest radiograph: loss of visualization of right heart border. B.Lateral chest radiograph: corresponding middle lobe pneumonia (P). |
Silhouette Sign
Lung opacity contacting a mediastinal or diaphragmatic border will obliterate or silhouette that border (“silhouette sign”). Right middle lobe opacity can be subtle on the frontal CXR, necessitating careful scrutiny of the right heart border (Fig. 5.3). Lingular disease obliterates the left heart border (Fig. 5.4), whereas lower lobe opacity may obscure a hemidiaphragm.
Airspace Diseaes
This describes replacement of the airspaces with fluid or exudate without gross destruction or displacement of lung morphology. Signs of airspace disease (Chapter 14) (Fig. 5.5) occur. At CT early airspace disease may manifest as ground glass opacity, with increased attenuation but with pulmonary vessels still visible.
|
|
|
Figure 5.4 Silhouette sign of lingular pneumonia. Partial loss of visualization of lower left heart border. |
|
|
|
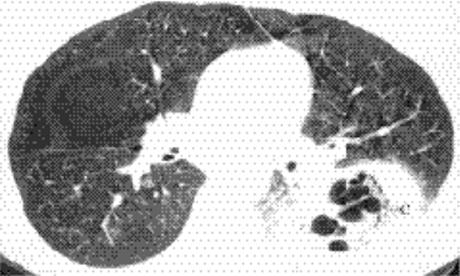
Figure 5.5 Airspace disease at computed tomography. Pneumonia shows air bronchograms (arrowheads), lobar distribution (arrowsdenote major fissure), and ill-definition anteriorly. |
Peribronchial Thickening
Perceptible thickening of a bronchus is most commonly seen in viral infections. It can often be discerned by comparing the bronchus diameter with its accompanying pulmonary artery.
Atelectasis
This describes loss of lung volume (Fig. 5.6), and the term collapse is used when a whole lobe or lung is involved. Mild atelectasis occurs in many patients, especially those with interstitial pneumonia. It usually manifests as linear or discoid atelectasis.
|
|
|
Figure 5.6 Atelectasis with pneumonia. Depression of major fissure (arrows) and silhouetting of right heart border indicate combined right middle and lower lobe atelectasis. |
|
|
|
Figure 5.7 Bronchopneumonia. Multifocal central linear and patchy opacities. |
Radiologic Classification of Pneumonia
Pneumonia is recognized to have different radiologic appearances. These generally have no bearing on the final diagnosis, because the same organism may produce several patterns. In addition, the early use of antibiotics alters the evolution of these patterns. The patterns are as follows:
Bronchopneumonia: This is the most common pattern. Here, the inflammatory exudates are mainly related to the central bronchovascular structures and may be multifocal (Fig. 5.7). Some acini may be spared, resulting in a patchy distribution of opacity. There is often associated volume loss.
|
|
|
Figure 5.8 Lobar pneumonia. (A) Posteroanterior and (B) lateral chest radiographs demonstrate airspace opacity filling much of the left upper lobe (P). |
Lobar pneumonia: The exudate begins distally and spreads circumferentially, giving rise to more homogeneous opacity (Figs. 5.8 and 5.9). It may eventually involve the whole lobe. The airways are not principally involved, so there is little volume loss, and air bronchograms are generally present.
|
|
|
Figure 5.9 Lobar pneumonia. (A) Posteroanterior and (B) lateral chest radiographs demonstrate opacification of virtually the entire middle lobe (P). |
Interstitial pneumonia: This consists of peribronchial thickening and ill-defined reticulonodular opacities (Fig. 5.10). This pattern is typical of Mycoplasma and viruses. Patchy distribution of atelectasis is often seen.
Round pneumonia: Some pneumonias have this configuration initially. There is usually an ill-defined border (Fig. 5.11). Air bronchograms are frequently present.
|
|
|
Figure 5.10 Interstitial pneumonia. Bilateral widespread ill-defined opacities. |
|
|
|
Figure 5.11 Round pneumonia (P), demonstrating a sharp margin inferiorly (arrows) and an ill-defined border superomedially. |
Differential Diagnosis of Pneumonia
Acute airspace disease has a reasonably brief differential diagnosis. Pneumonia generally differs from pulmonary edema in its more focal distribution. There is generally not associated cardiac enlargement in pneumonia. At CT pneumonia demonstrates nondependent opacity (as opposed to the dependent pattern of pulmonary edema). Pulmonary edema also improves or worsens in hours as opposed to days in the case of pneumonia.
Adult respiratory distress syndrome (ARDS) is often indistinguishable from pneumonia on a single radiographic study. Over time changes will occur more slowly in ARDS, and it is often more widespread than pneumonia. CT will show dependent changes in ARDS.
Subsegmental atelectasis may be indistinguishable from early pneumonia. The more linear the radiographic abnormality, the less likely it represents pneumonia. Associated clinical signs and symptoms may be helpful; transmitted breath sounds are often amplified in pneumonia but not in atelectasis.
The radiographic appearance of pulmonary infarct may be quite similar to pneumonia. Enlargement of a pulmonary artery or attenuated peripheral vessels may suggest a vascular etiology. Infarct is more likely to be well marginated at its borders and typically evolves more rapidly than pneumonia.
The appearance of pulmonary hemorrhage is very similar to pneumonia. There is often a history of frank hemoptysis. Clearance of opacity usually occurs more quickly than in pneumonia.
Some neoplasms, such as lymphoma and bronchoalveolar carcinoma, produce airspace opacification indistinguishable from pneumonia. Serial studies show more chronic abnormality with gradual change. Lymph node enlargement at CXR would be more typical of lymphoma than pneumonia.
Radiologic Clues to the Cause of Pneumonia
Lobar consolidation is often due to bacteria. Postobstructive pneumonia needs to be considered in patients at risk for lung carcinoma. Expansive consolidation occurs in Klebsiella pneumonia (“Friedlander pneumonia”) (Fig. 5.12) but can also be seen with S. pneumoniae.
Cavitating consolidation (Figs. 5.13 and 5.14) suggests bacteria or fungi. S. aureus, Klebsiella, anaerobes, and Mycobacterium tuberculosiscommonly cause cavitation. Pneumatoceles may result in a similar appearance (Fig. 5.15) and suggest S. aureus or S. pneumoniae.Emphysematous bullae within consolidated lung may mimic cavities.
|
|
|
Figure 5.12 Pneumonia (P) enlarging the right upper lobe, suggesting the correct diagnosis of Klebsiella pneumonia. (A)Posteroanterior and (B) lateral chest radiographs: note bowing of major fissure (arrows). There is an associated pleural effusion (E). |
|
|
|
Figure 5.13 Cavitary pneumonia. (A) Posteroanterior, and (B) Lateral chest radiographs: cavity with a gas-fluid level (arrows) in the superior segment of the right lower lobe. |
Nodular or spherical pneumonia is usually due to pneumococcal, Legionella, Q fever, or fungal pneumonia. Hematogenous dissemination ofS. aureus can cause spherical pneumonia or septic emboli. Reticulonodular opacity and peribronchial thickening are typical of viruses andMycoplasma.
|
|
|
Figure 5.14 Cavitary pneumonia (C) at computed tomography. |
|
|
|
Figure 5.15 Diffuse pneumonia with pneumatocele formation (P). |
Patchy consolidation with a dependent distribution occurs with aspiration pneumonia. This is usually bilateral. Patchy upper lobe disease is suggestive of tuberculosis (TB) or histoplasmosis, especially if there is associated cavitation. Miliary opacities occur with overwhelming tuberculous or fungal infection.
Dependent pneumonia suggests aspiration, whereas cavitary upper lobe disease raises the possibility of TB.
Pleural effusions may develop with anaerobic bacteria, gram-negative bacteria, S. aureus, and S. pyogenes. Empyema should be suspected when pleural effusion is large or loculated or develops late in the course of disease.
Complications
Pleural effusions/empyema: these are indistinguishable radiographically.
Cavitation: if enlarging or greater than 4 cm in diameter, an indication for intervention.
Pneumatoceles: usually self-limiting and resolve within 4 weeks. They resemble bullae and blebs.
Pneumothorax: seen in Pneumocystis carinii pneumonia (Chapter 6).
Lymph node enlargement: seen with fungal and mycobacterial infections. In patients at risk, also consider bronchogenic carcinoma.
Bone destruction: may occur in actinomycosis, nocardiosis, fungal infections, and TB.
Abscess: may be difficult to distinguish from empyema. CT sometimes helpful to differentiate these two entities
Bronchiectasis: any chronic or severe infection may cause bronchiectasis, and in cystic fibrosis patients, upper lung bronchiectasis tends to occur.
· Expansive consolidation:
o Klebsiella
o Haemophilus influenzae
o Pneumococcal pneumonia
o Plague pneumonia
o TB
o Lung abscess: S. aureus, Klebsiella
o Lung mass
· Cavitating pneumonia:
o S. aureus
o Klebsiella
o TB
o Aspiration
o Actinomycosis
o Nocardiosis
o Histoplasmosis
o Aspergillosis
o Coccidioidomycosis
o Echinococcosis
o Amoebiasis
· Pneumatoceles:
o S. aureus
o S. pneumoniae
o Escherichia coli
o Klebsiella
o H. influenzae
o P. carinii
o Legionella pneumophila
Bacterial Pneumonia
Streptococcus pneumoniae (Pneumococcus)
This gram-positive coccus is responsible for anywhere from 10% to 80% of cases of CAP (9,10). It is the most frequent organism resulting in hospitalization for pneumonia. It is common in healthy young adults, typically presenting with chills, fever, and cough productive of rust-colored blood-tinged sputum. Spread is by the airborne route. Diagnosis can be made by sputum or blood culture, although pneumococci are found in the sputum of 10% to 40% of normal patients. Sputum cultures are negative in nearly half of patients with positive blood cultures. Most patients are diagnosed presumptively, based on clinical and radiographic presentation, without the need for cultures.
Pneumococcus is the organism most frequently resulting in hospitalization for pneumonia.
Homogeneous airspace disease confined to a single lobe with an irregular margin (Fig. 5.16) is the most common radiographic pattern, seen in about one-third of patients. Pneumococcal pneumonia is one of the causes of expansive consolidation with bowing of fissures. More widespread patchy bronchopneumonia is seen in another one-third, usually confined to a single lobe. Interstitial opacification simulating viral or atypical pneumonia occurs in one-fourth of patients. The remainder show a mixed patchy and interstitial pattern. There is a predilection for the lower lobes. Pleural effusions are seen in one-third. Consolidation in pneumococcal pneumonia is said to clear by central “lysis.” Patients with shorter clinical histories tend to show more rapid radiographic resolution. As in all pneumonias there is a lag period between clinical resolution and radiologic resolution, which can be several weeks.
Staphylococcus aureus
This gram-positive coccus is an uncommon but serious cause of CAP (11,12,13). It has a fulminant course with fever, cough, dyspnea, purulent sputum, hemoptysis, and chest pain. Spread occurs by the airborne or hematogenous route. When acquired via inhalation, S. aureus pneumonia is often a complication of influenza during epidemics. Airborne spread is also implicated in debilitated patients. Hematogenous spread occurs secondary to soft tissue infections, valve prostheses, hemodialysis, and intravenous drug use. Morbidity is high, with a reported mortality rate of 7% to 19%.
|
|
|
Figure 5.16 Pneumococcal pneumonia. (A) Posteroanterior and (B) lateral chest radiographs: homogeneous middle lobe pneumonia (P), possibly with slight expansion of the lobe, with associated right pleural effusion (E). (C) Later posteroanterior chest radiograph and (D)computed tomography: subsequent development of pneumatoceles (arrows) resulting in bronchopleural fistula with hydropneumothorax. P, pneumothorax; E, pleural effusion. Arrowheads mark gas–fluid level. |
Initially, radiographs most commonly (75%) show multilobar homogeneous airspace disease (Fig. 5.17). Subsequent radiographic deterioration is often seen. Bilateral changes are noted in 35%. Cavitation or abscess formation (25%), pneumatoceles (40%), pleural effusions (33%), and pneumothorax (20%, often associated with pleural effusion or empyema) are other common findings. Pneumonia with pneumatocele or pneumothorax should suggest S. aureus as the cause.
|
|
|
Figure 5.17 Staphylococcus aureus pneumonia. (A) Posteroanterior and (B) lateral chest radiographs demonstrate airspace disease in the right upper lobe and both lower lobes (P). |
Bacillus anthracis
This is a gram-positive sporulating nonmotile organism. It is endemic in the soil of Texas, Oklahoma, and the lower Mississippi valley (14). Cutaneous disease accounts for over 90% of cases, with gastrointestinal and inhalational disease causing 5% each. Inhalational disease results from industrial or agricultural exposure to animal hides, hair, wool, or bone meal of contaminated livestock. The disease is most prevalent among herbivores such as cattle, sheep, horses, and goats. Prior radiation exposure, alcoholism, and underlying pulmonary disease are thought to be risk factors. Spores of 2 to 5 μm reach the alveoli. Macrophages engulf the spores and transfer them to mediastinal and hilar nodes. Germination occurs with production of large amounts of anthrax toxin. This spills over into the systemic circulation with resultant edema, hemorrhage, necrosis, and septic shock. Massive hemorrhagic mediastinitis occurs. Inhalational anthrax manifests as an initial flu-like illness followed by rapidly progressive respiratory failure and death.
CXRs show widening of the mediastinum due to hemorrhagic mediastinitis and lymphadenitis (15,16). Pleural effusions also occur. Focal hemorrhagic pneumonia is only seen in one-fourth of patients. CT better demonstrates hemorrhagic mediastinitis and necrosis. It also excludes other etiologies of widened mediastinum.
Klebsiella
This gram-negative bacillus is also known as Friedlander bacillus (17). It is found in the upper respiratory tract of 2% to 25% of healthy persons. It is an uncommon cause of pneumonia and a well-known cause of biliary and urinary tract sepsis. Middle-aged men are most commonly affected, and many patients have predisposing conditions such as alcoholism, malnutrition, and diabetes. Chronic pulmonary diseases such as asthma and bronchiectasis may also predispose to Klebsiella infections. The incubation period is short. Cough, pleuritic pain, and fever are frequent initial symptoms, with malaise, chills, and shortness of breath also occurring. The mortality rate is high, estimated at 70% to 80%. Of the remainder, a few recover slowly, whereas others suffer chronic disease with a clinical course similar to TB.
Radiographs most commonly show scattered lobular foci of airspace disease that may coalesce to form larger opacities (18,19). Typically, opacity has a sharp advancing border. This pattern is indistinguishable from other bacterial pneumonias. The upper lobes are involved in two-thirds of cases. Healing generally leaves residual scarring and distortion of lung. Radiographs may show expansion of a lobe (Fig. 5.12) due to “drowned lung.” Shift of the mediastinum to the opposite side may occur with whole lung involvement. Small pleural effusions are thought to occur because pleural thickening often remains after resolution of acute changes. Empyema occurs in about 6%. These patients have the worst clinical course. Klebsiella deserves consideration whenever opaque, extensive, expansive airspace disease is seen.
Klebsiella should be considered with opaque, extensive, expansive airspace disease.
Pseudomonas aeruginosa
This gram-negative organism is a rare cause of CAP in healthy persons (20,21). Pseudomonas colonizes bronchiectatic airways, especially in cystic fibrosis. It is sometimes present on normal skin and is also a secondary contaminant in wounds. Prematurity, chemotherapy, antibiotics, steroids, immunosuppressants, old age, and debility increase the risk of Pseudomonas. Neutropenia increases the risk of severe disease. Most cases occur in hospitalized patients, especially those on ventilators. Organisms have been cultured from sinks, catheters, receptacles, ventilator equipment, and staff. Pseudomonas is the most common pathogen isolated from the lower respiratory tract of ventilated patients and is implicated in 25% of ventilator-associated pneumonias. Mortality in these patients is in the 80% to 100% range. Pneumonia is usually secondary to aspiration of oropharyngeal contents in intensive care unit patients. Sedation, endotracheal intubation, and intermittent positive pressure ventilation predispose to infection. Person-to-person contact has been implicated in hospitals.
|
|
|
Figure 5.18 Pseudomonas pneumonia. (A) Posteroanterior and (B) lateral chest radiographs demonstrate airspace disease (P) predominantly in the posterior segment of the right upper lobe. |
Pseudomonas is implicated in 25% of ventilator-associated pneumonias, with 80% to 100% mortality.
Radiographs most commonly demonstrate segmental or lobar disease (22) (Fig. 5.18). Abnormality is multilobar in 80% and bilateral in 65%. The lower lobes predominate. Pleural effusions are seen in 25%. Lucencies are seen in up to 20%, representing cavities or abscesses in necrotizing pneumonia, interspersed normal areas of lung, or pneumatoceles. Cavitation in a ventilated patient suggests Pseudomonas.
Legionella pneumophila
This gram-negative organism is responsible for sporadic cases and outbreaks of pneumonia (23). The first reported outbreak of 182 cases occurred at an American Legion convention in 1977, after which the organism is named. It is thought to be an airborne infection with bacterial growth detected in cooling towers and air conditioning systems. L. pneumophila accounts for over 90% of cases of legionellosis. Diagnosis is based on sputum culture, urinary antigen detection, and rising antibody levels on paired serologic tests. Legionellosis has been classified as an atypical pneumonia due to the clinical prodrome of malaise and headache, the radiologic findings, and the poor correlation between these findings and clinical signs. It runs a long clinical course, taking even longer to resolve in debilitated patients. Death has been reported in a few cases.
Chest radiographic findings lag behind the clinical findings by a few weeks and cannot be used to differentiate legionellosis from other causes of pneumonia. Over 80% of patients have patchy airspace disease initially. In two-thirds of cases this is unilobar (Fig. 5.19). The lower lobes are involved in 75% of cases. The apices are rarely involved. Small pleural effusions are ultimately seen in over 60% of patients. Cavitation is very rare and occurs predominantly in immunocompromised patients. Enlarged lymph nodes have not been reported. Radiologic resolution is slow, and initial worsening of findings is often seen.
|
|
|
Figure 5.19 Legionella pneumonia. (A) Posteroanterior and (B) lateral chest radiographs demonstrate unilobar involvement of the right lower lobe (P) with prominent air bronchograms (arrows). |
Aspiration Pneumonia
This may occur subsequent to the intake of solid or liquid materials into the lungs. Predisposing factors include impaired consciousness, alcoholism, general anesthesia, dementia, neuromuscular disorders, tracheoesophageal fistula, pharyngeal diverticulum, gastroesophageal reflux, achalasia, and hiatal hernia. Clinical and radiologic manifestations vary from asymptomatic to life-threatening disease (24). The most commonly involved lung sites are the posterior segments of the upper lobes and superior segments of the lower lobes in the recumbent position. The basal segments of the lower lobes, especially in the right lung, are most commonly involved when aspiration occurs in the upright position (Fig. 5.20). Chemical pneumonitis may occur, varying from mild bronchiolitis to pulmonary edema.
Aspiration of infected contents in hospitalized patients or those with poor oral hygiene may cause necrotizing pneumonia due to anaerobic organisms. P. aeruginosa is most commonly implicated. Complications include cavitation and empyema.
Actinomyces
These slow-growing, filamentous, gram-positive bacteria are found normally in the oropharynx, especially in patients with poor dental hygiene (25). They form mycelium-like colonies that resemble fungi. Three disease patterns are described: cervicofacial, abdominopelvic, and thoracic. The latter accounts for 15% to 45% of cases. Men are affected three to four times more often than women. Thoracic infections may occur in the setting of trauma, surgery, alcoholism, COPD, or after aspiration. The primary lesion is based in the peribronchial tissues and spreads from lung to pleura, mediastinum, and chest wall with no regard for anatomic barriers. Direct spread relates to bacterial proteolytic activity. The organism can also disseminate hematogenously. Thoracic disease may also result from direct spread of disease in the neck or below the diaphragm. Diagnosis is difficult and often relies on demonstration of characteristic sulfur granules in sputum smears, consisting of conglomerate masses of mineralized organisms.
Actinomycosis does not respect anatomic barriers.
In acute infections, nonsegmental airspace disease (Fig. 5.21) is the usual CXR pattern, with peripheral and lower lobe predominance in over 75%. This may be multifocal and may cross fissures. Pleural thickening or small pleural effusions are found in most patients. Hilar and mediastinal lymph node enlargement is seen in one-third of patients. In chronic disease, spread to chest wall soft tissues can be well seen by CT.
|
|
|
Figure 5.20 Aspiration pneumonia. Lower lobe distribution with increased opacity over the lower thoracic spine (P), silhouetting the posterior hemidiaphragms. |
|
|
|
Figure 5.21 Actinomycosis. Nonsegmental airspace disease in the left upper lobe (A), silhouetting the left heart border. |
Nocardia
This is a gram-positive filamentous bacterium with some similarity to Actinomycetes. It is present in soil and decaying organic matter and is acquired in humans by inhalation (26). Nocardia asteroides is responsible for 80% to 90% of all cases of nocardiosis. Pulmonary infection is the main clinical manifestation. About half of those affected are immunocompetent. The clinical syndrome is subacute, with productive cough, fever, weight loss, and malaise. Half of those infected develop disseminated disease. The central nervous system is affected in 25% of cases, and skin and subcutaneous tissues are commonly involved. Disseminated disease should be considered when the triad of pneumonia, central nervous system disease, and subcutaneus nodules occurs. With disseminated disease, the mortality rate is 80% to 90%, and death is especially likely when there is central nervous system involvement. Mortality is 38% without dissemination.
Radiographic manifestations are varied, including solitary and multiple nodules, airspace disease, and interstitial reticular opacities. Cavitation may occur. Pleural effusion and enlarged hilar and mediastinal lymph nodes may be seen.
Chlamydia pneumoniae
This organism has recently been identified as the cause of 6% to 12% of adult CAP (27). Before the advent of specific serologic tests, these infections were classified as “atypical” pneumonia or erroneously attributed to ornithosis. Two types of acute disease occur, primary (first exposure) and recurrent (in a previously exposed individual). Chronic lung disease is more common in those patients with the recurrent form. Transmission is by droplet spread. Symptoms include cough, fever, sore throat, hoarseness, and sinusitis.
Radiographs in the acute form show airspace disease, usually confined to one lung (Fig. 5.22) and in a single lobe in 75%. Interstitial opacities or mixed interstitial and airspace opacities are less common. Pleural effusions are seen in over half of patients as disease progresses. In patients with recurrent disease findings are more variable, with bilateral disease in 63% and pleural effusions more likely. Hilar and mediastinal lymph node enlargement is uncommon.
|
|
|
Figure 5.22 Chlamydia pneumonia. (A) Posteroanterior and (B) lateral chest radiographs: multilobar pneumonia (P) confined to one lung. |
Mycoplasma pneumoniae
This is a common cause of CAP, responsible for 10% to 30% of cases (9,28,28). It belongs to the group of organisms responsible for atypical pneumonia and is thought to cause up to 50% of such cases. Transmission is via the respiratory route, with most cases occurring in the fall and winter. Localized outbreaks in military camps, schools, families, and community groups have been described, cycling every 4 to 5 years. Mycoplasma is typically a disease of children and young adults and carries a good prognosis. The clinical course is often insidious, with malaise, fever, chills, headache, anorexia, and nonproductive cough. Complications include large pleural effusions, pleuropericarditis, myocarditis, ARDS, Guillain-Barré syndrome, lymph node enlargement, cold agglutinin-induced hemolytic anemia, and aseptic meningitis. Diagnosis is made by detecting a significant rise in serum cold hemagglutinins.
Mycoplasma is thought to cause up to 50% of atypical pneumonias.
A common chest radiographic feature is segmental airspace disease (Fig. 5.23), occurring in 30% to 50% of patients. This may be dense or patchy in appearance. Involvement is unilateral in half to two-thirds, with lower lobe predominance in 77%. Reticulonodular opacities are said to occur just as often. Less commonly, perihilar bronchovascular thickening is seen. Pleural effusions are present in less than 10% of patients in most studies. Hilar lymph node enlargement is uncommon at CXR.
Mycobacterium tuberculosis
This bacillus, an obligate aerobe, is related to nocardia (30). It has a cell wall that resists staining by the usual Gram stain method. After accepting fuscin dyes it resists decolorization by acid-alcohol, hence the term acid-fast. Prevalence is highest in developing nations. Annual incidence is 200 to 250 cases per 100,000 in sub-Saharan Africa and Southeast Asia. Annual incidence in industrialized nations averages 23 per 100,000. In developing nations, 80% of cases affect adults in their productive years. In industrialized nations, most cases result from endogenous reactivation of remote infection, with rates highest in the elderly. Incidence is higher in non-white racial and ethnic groups and in immigrants.
|
|
|
Figure 5.23 Mycoplasma pneumonia. (A) Posteroanterior and (B) lateral chest radiographs: segmental airspace disease (P) in the lateral segment of middle lobe. |
Primary TB is transmitted by the airborne route. Particles measuring 1 to 5 mm can remain airborne for prolonged periods of time. Implantation of particles occurs preferentially in the middle and lower lung zones. Alveolar macrophages ingest and kill mycobacteria with variable success depending on host resistance and organism virulence. Macrophages may be overwhelmed and may burst, with released bacilli spreading via lymphatics and the bloodstream. Bacillary growth is usually arrested by the development of cell-mediated immunity and delayed hypersensitivity. Ninety percent of persons develop immunity and are asymptomatic. In 5% immunity is inadequate and active TB infection develops within a year (progressive primary disease). This is similar in morphology and course to postprimary disease. Another 5% will develop latent reactivation at a later stage. Progression to clinical disease is more likely with defects in T-cell or macrophage function, including acquired immunodeficiency syndrome, malnutrition, drug abuse, alcoholism, diabetes, immunosuppressive therapy, steroids, and silicosis.
Postprimary TB results from endogenous reactivation of previously acquired disease or, less commonly, exogenous reinfection. There is a predilection for the upper lung zones in postprimary TB, thought to relate to higher oxygen tensions and impaired lymphatic drainage. Cell-mediated immunity attacks TB via macrophage ingestion of particles. Delayed hypersensitivity causes caseous necrosis of TB-laden macrophages with local tissue destruction. Healing occurs with resorption of caseous material and accompanying fibrosis. Dystrophic calcification occurs in both primary and postprimary TB but does not necessarily indicate complete sterilization of infection. Endobronchial TB occurs along with pulmonary involvement and is believed to result from infected sputum, spread from adjacent parenchyma, eroded lymph nodes, and/or infected cavities. Miliary TB occurs when tubercle bacilli discharge into the bloodstream with distal organ dissemination. This can occur at the primary or postprimary stage. Symptoms of active TB include low-grade fever, anorexia, fatigue, cough, hemoptysis, chest pain, night sweats, and weight loss.
Miliary TB occurs both with primary and postprimary infections.
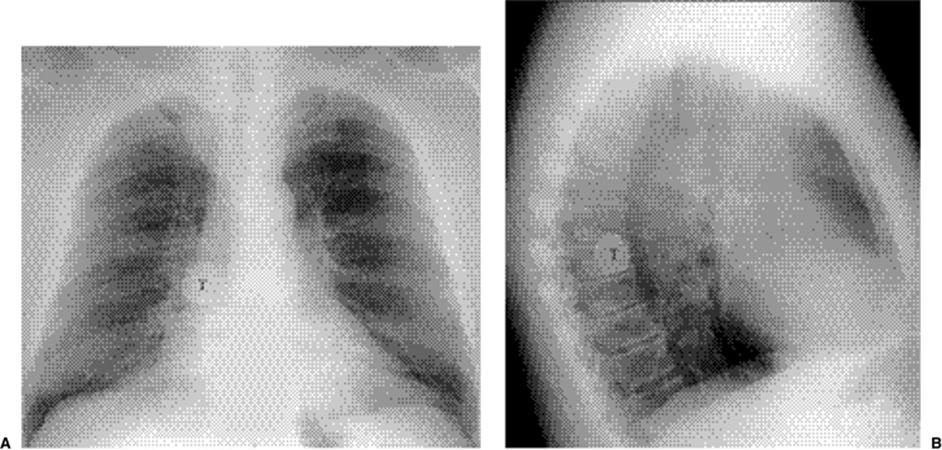
The CXR in primary TB commonly reveals lymph node enlargement (Fig. 5.24), especially involving the right paratracheal and hilar lymph nodes. The prevalence of lymph node enlargement decreases with age, from 40% of young adults to 10% of the elderly. Homogeneous consolidation in a segmental or lobar distribution is the most common parenchymal abnormality (Fig. 5.25). Patchy, linear, or nodular disease occurs less commonly. There is said to be a slight right lung predominance, but no zonal predominance. In contrast to lymph nodes, parenchymal disease increases in frequency with age. The initial site of parenchymal involvement at the time of first infection is known as the Ghon focus. The Ghon focus and enlarged regional lymph node together are known as the Ranke complex. Simon foci are apical nodules, frequently calcified, that result from hematogenous seeding at the time of initial infection. Prevalence of pleural effusion increases with age. Effusion is seen in one-third of adults, often on the side of parenchymal abnormality. Effusions are usually unilateral, with bilaterality in 15% of cases. In 5% effusion is the sole abnormality.
|
|
|
Figure 5.24 Primary tuberculosis. (A) Posteroanterior and (B) lateral chest radiographs demonstrate right hilar and paratracheal lymph node enlargement (N). |
|
|
|
Figure 5.25 Primary tuberculosis. Right upper lobe airspace disease (A). |
Contrast-enhanced CT may show a characteristic appearance in mediastinal tuberculous lymphadenitis, with central nodal low attenuation (Fig. 5.26) and peripheral enhancement. This appearance also occurs with atypical mycobacterial infections, lymphoma, metastases, and Whipple disease. CT is more sensitive for detection of calcification.
|
|
|
Figure 5.26 Primary tuberculosis. Computed tomography demonstrates low attenuation of a subcarinal lymph node (arrow). |
|
|
|
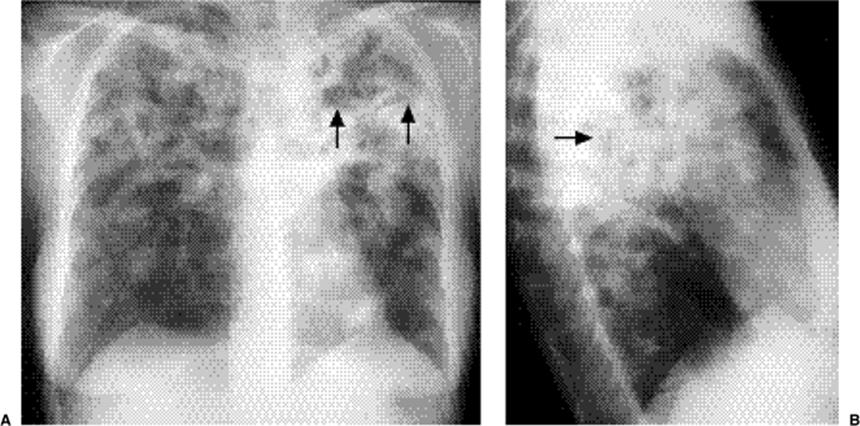
Figure 5.27 Postprimary tuberculosis. (A) Posteroanterior and (B) lateral chest radiographs demonstrate extensive bilateral upper lobe airspace disease, primarily posteriorly, with areas of cavitation (arrows). |
Radiographs in postprimary TB show parenchymal opacities in the apical and posterior segments of the upper lobes (Fig. 5.27) in over 80% and in the superior segments of the lower lobes in 10% to 15%. These opacities are most commonly heterogeneous, and cavitation (Fig. 5.28) is observed in 40% to 45%. Wall thickness is variable, and gas–fluid levels are sometimes seen (Fig. 5.29). Bronchogenic spread may occur with resulting ill-defined nodules, typically involving the lower zones (“upstairs–downstairs” pattern). In 3% to 6% of patients tuberculomas subsequently develop (Fig. 5.30), often with calcification and generally ranging from 0.5 to 4 cm. Lymph node enlargement is uncommon in postprimary TB, seen in only 5%. Pleural effusion is present in 16% to 18% of cases and is usually unilateral. Radiographic evidence of the original primary infection, including calcified lymph nodes and granulomas, is seen in 20% to 40%. Upper lobe fibrotic changes (Fig. 5.31) are seen in a similar percentage of patients. Noncalcified miliary nodules are the hallmark of miliary TB (Fig. 5.32).
|
|
|
Figure 5.28 Postprimary tuberculosis. (A) Posteroanterior and (B) lateral chest radiographs demonstrate a large cavity (C) in the apicoposterior segment of the left upper lobe. |
|
|
|
Figure 5.29 Postprimary tuberculosis. (A) Posteroanterior chest radiograph and (B) computed tomography with left upper lobe gas–fluid levels (arrows) and bilateral upper lobe disease. |
|
|
|
Figure 5.30 Tuberculoma (T). (A) Posteroanterior and (B) lateral chest radiographs demonstrate a solitary calcified right lower lobe nodule. |
|
|
|
Figure 5.31 Postprimary tuberculosis with upper lobe fibrotic changes. A. Initial posteroanterior chest radiograph: exudative and cavitary upper lobe airspace disease, similar to Fig. 5.27. B. Posteroanterior chest radiograph 1 year later: marked resolution of exudative and cavitary disease, with residual linear, retractile abnormality. |
CT demonstrates internal details of cavities better than CXR. Bronchogenic spread, evidenced by centrilobular nodules and a tree-in-bud pattern (Fig. 5.33), is shown in 95% of cases of postprimary TB. Other findings on CT include lobular airspace disease and interlobular septal thickening. Postprimary tuberculous effusions may show the “split pleura” sign on contrast-enhanced CT (Fig. 5.34). Miliary disease may be seen at high resolution CT before it is apparent on the CXR.
|
|
|
Figure 5.32 Miliary tuberculosis. A. Posteroanterior chest radiograph: subtle nodular pattern in the lower lungs. B. Computed tomography: innumerable tiny miliary bilateral nodules. |
|
|
|
Figure 5.33 Bronchogenic spread of tuberculosis. Computed tomography demonstrates tree-in-bud pattern (arrows). |
|
|
|
Figure 5.34 Tuberculous empyema (E) with split pleura sign (arrows). |
Complications of TB such as bronchiectasis are well demonstrated by CT. Dilated bronchi or cavities may be colonized by aspergillus species, resulting in aspergilloma(s) (Fig. 5.35). Rasmussen aneurysms are pulmonary artery pseudoaneurysms caused by erosion from an adjacent cavity. These are uncommon but may be shown on helical contrast-enhanced CT. Broncholiths occur when calcified lymph nodes erode into or obstruct bronchi (Fig. 5.36). Distal atelectasis and bronchoceles may ensue. A normal CXR cannot exclude TB, nor can imaging studies differentiate active from inactive disease. Stability on follow-up studies generally indicates, but does not prove, inactivity.
|
|
|
Figure 5.35 Tuberculous cavity with aspergilloma (A) and air crescent sign (arrows). |
|
|
|
Figure 5.36 Broncholith (arrows) in tuberculosis. |
Nontuberculous Mycobacteria
Multiple species of nontuberculous mycobacteria (NTMB) exist. These are ubiquitous organisms that constitute part of the normal environmental flora. They have been isolated from lakes, streams, other natural waters, soil, milk and other foodstuffs, and domestic animals. Unlike TB, NTMB are not acquired by person-to-person spread (31). Rather, they are acquired from the environment by inhalation of aerosolized water droplets. Mycobacterium avium intracellulare and Mycobacterium kansasii account for the bulk of NTMB pulmonary infections. M. avium intracellulare is responsible for 61% of cases of NTMB infections alone. M. avium intracellulare is most prevalent in the southeastern United States, whereas M. kansasii is most prevalent in the midwestern and southwestern United States. Unlike M. aviumintracellulare, M. kansasii responds favorably to antituberculous therapy. Clinical and radiographic findings in NTMB infections vary widely (32). The findings fall into two main groups, with three other discrete entities.
Classic Form of Infection
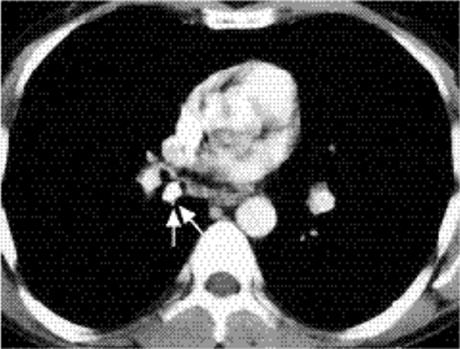
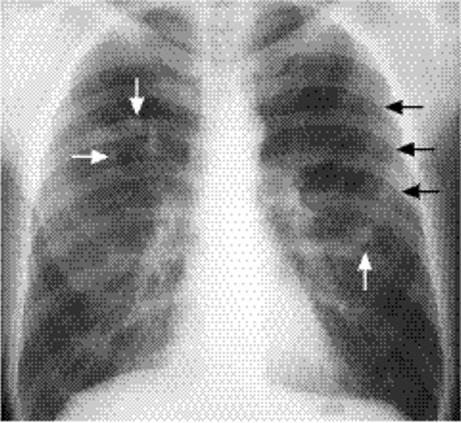
This form of infection is seen predominantly in middle-aged white men with predisposing illnesses. These include COPD, previous TB, lung fibrosis, silicosis, and asbestosis. Other risks are smoking, alcoholism, cardiac disease, and chronic liver disease. Symptoms are insidious and include cough (60% to 100%), hemoptysis (15% to 20%), weight loss, and weakness. Fever (10% to 13%) is notably uncommon as it is in all NTMB pulmonary infections. Radiographs reveal fibrotic and nodular opacities indistinguishable from postprimary TB (Fig. 5.37) Cavitation occurs in the majority (80% to 95%), and adjacent pleural thickening is frequent (37% to 56%). Bronchogenic spread to the lower lobes may occur, with patchy and nodular alveolar opacities. Pleural effusion is uncommon (5% to 20%), and enlarged lymph nodes (Fig. 5.38)are even less common (< 4%). Bronchopleural fistula may occur.
Nontuberculous mycobacterial infections are often radiologically indistinguishable from postprimary TB.
|
|
|
Figure 5.37 Classic appearance of nontuberculous mycobacteria, closely resembling upper lobe postprimary tuberculosis. (A)Posteroanterior and (B) lateral chest radiographs. |
Nonclassic Form of Infection
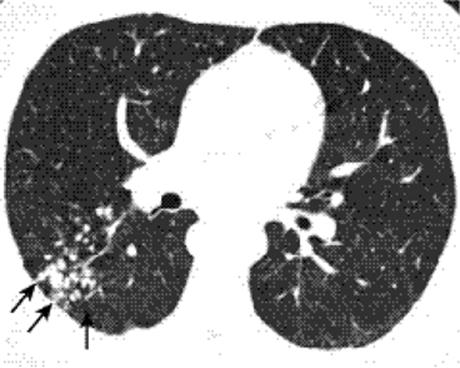
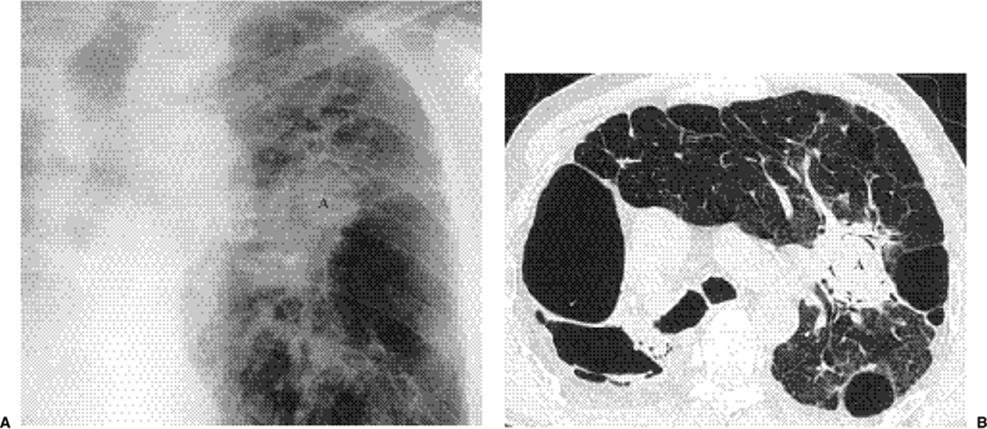
This accounts for 20% to 30% of NTMB pulmonary infections in immunocompetent adults. Unlike the classic form, it is seen predominantly in elderly white women without predisposing illnesses. Clinical symptoms are similar, with chronic cough and hemoptysis. Fever is rare, and other constitutional symptoms are uncommon.
|
|
|
Figure 5.38 Atypical appearance of nontuberculous mycobacteria. A. Posteroanterior chest x-ray: large right hilum (H) with adjacent right lower lung airspace disease (arrow). (B) Computed tomography: enlarged low attenuation right hilar lymph node (N) with enhancing rim (arrows). |
Radiographically, multiple bilateral nodular and interstitial opacities are randomly distributed. Bronchiectasis is sometimes seen. CT demonstrates linear opacities and clusters of opaque nodules predominantly in the lower zones, particularly in the lingula and middle lobe. Bronchiectasis is predominantly seen in the lingula and middle lobe. Volume loss is occasionally present. The high attenuation nodules likely represent peribronchial granulomas or mucous plugs in small airways. Branching centrilobular opacities (tree-in-bud) can be seen on high resolution CT. Patchy airspace disease or ground glass opacities may also be seen. Pleural thickening may develop adjacent to areas of bronchiectasis. Mediastinal lymph node enlargement is occasionally present.
Asymptomatic Nodules
Solitary or multiple granulomas may occur, as in granulomatous infections such as TB and histoplasmosis. When multiple, they may be in clusters. This helps to differentiate them from metastases, which usually have a more random distribution. Patients are usually asymptomatic and stability is shown on follow-up radiographic studies.
Achalasia Patients
The mechanism of infection in these patients is thought to be chronic aspiration. M. fortuitum-chelonei complex is almost always implicated. Radiographically, patchy alveolar airspace opacities are seen with a basal distribution, resembling aspiration pneumonia.
Immunocompromised Patients
The features of NTMB infection in patients with acquired immunodeficiency syndrome are discussed in Chapter 6.
Fungal Infections
Table 5.1 lists the various radiographic features of fungal infections.
|
Table 5.1: Summary of Radiographic Features in Fungal Infections |
||
|
Histoplasma
Histoplasmosis is a common granulomatous infection in parts of the United States (33). Histoplasma capsulatum is a fungus that exists as a mold in the soil. Soil rich in bird droppings encourages growth of this organism. Birds do not harbor the organism, but mammals such as bats may. Infection is acquired by inhalation of windborne spores blown from sources such as bird roosts or bat haunts. It is epidemic in the central United States in a triangular area extending from Ohio to Nebraska to Louisiana and encompassing the Mississippi, Missouri, and Ohio River valleys. Virtually all inhabitants of this area will acquire the infection.
Virtually all inhabitants of the triangular region from Ohio to Nebraska to Louisiana will be infected by Histoplasma capsulatum.
Most infections are asymptomatic, with clinical pneumonia occurring in those exposed to a large number of infecting spores. Illness is mild with cough, fever, headache, and chest pain. At body temperature, inhaled spores germinate into yeast forms that are phagocytized by macrophages. The yeasts multiply in the macrophages, resulting in bronchopneumonia with granulomatous inflammation. The parasitized macrophages migrate to regional nodes and disseminate hematogenously to the reticuloendothelial system, especially the spleen. Within 1 to 2 weeks hypersensitivity develops with involution, encapsulation, and eventual calcification. Immunity to histoplasmosis is gradually lost over the next few years. However, in endemic areas the infection will be acquired again and again during a life span.
In symptomatic patients, radiographs demonstrate bilateral extensive nonsegmental areas of lobular airspace disease (Fig. 5.39). Hilar lymph node enlargement may also be seen. After the findings resolve there are generally pulmonary and hilar calcifications (Fig. 5.40). Calcifications tend to be larger and more numerous than in TB.
|
|
|
Figure 5.39 Acute histoplasmosis. Extensive bilateral airspace disease resulting from a large inhaled inoculum during caving. |
|
|
|
Figure 5.40 Histoplasmosis. Numerous small calcified lung nodules. |
Disseminated disease is rare and usually occurs in immunocompromised individuals. The very young and elderly are at increased risk for disseminated disease. This ranges from an acute rapidly fatal infection to a chronic intermittent illness. Radiographs are often normal. Multiple diffuse small nodular opacities are the most common abnormality (Fig. 5.41). Limited or diffuse linear or irregular opacities also occur. Airspace disease is less commonly seen.
Chronic histoplasmosis is rare and usually occurs in middle-aged white men. Disease is self-limiting and nonfatal. Most patients have a history of cigarette smoking and emphysema. Symptoms are similar to postprimary TB with malaise, cough, and night sweats. Like TB the apical and posterior segments of the upper lobes are most commonly affected (Fig. 5.42). However, true cavitation rarely occurs. Infection begins adjacent to blebs and bullae with lucencies due to emphysematous spaces in an area of disease. Lymph node enlargement does not occur. Bronchogenic spread of cavitary contents from the upper lobes may occur, resulting in airspace disease in the lower lobes.
|
|
|
Figure 5.41 Miliary histoplasmosis. Miliary nodules are best visualized in the lower lungs. They were new from a chest x-ray 2 months earlier and resolved without therapy 4 months later. At that time, the patient died of Addison disease, and autopsy confirmed disseminated histoplasmosis as the cause. |
|
|
|
Figure 5.42 Chronic histoplasmosis. (A) Posteroanterior and (B) lateral chest radiographs: abnormality indistinguishable from postprimary tuberculosis and classic nontuberculous mycobacteria. |
Delayed manifestations of histoplasmosis occur in a small number of patients for unknown reasons. These include histoplasmomas, broncholithiasis, and fibrosing mediastinitis.
In some individuals the calcified nodule of previous histoplasmosis continues to enlarge, termed a histoplasmoma. These are most common in the posterior lower lobes, peripheral and adjacent to the pleura. Growth is slow, with diameter increases of 0.5 to 3 mm per year (Fig. 5.43). Laminated calcific rings occur, with lack of peripheral calcification indicating further growth potential. In 20% of cases, histoplasmomas are associated with fibrosing mediastinitis.
|
|
|
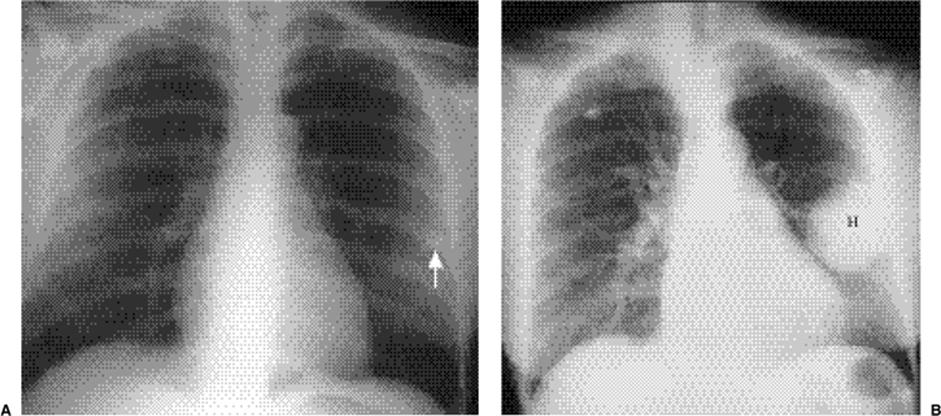
Figure 5.43 Histoplasmoma. A. Posteroanterior chest radiograph 1975: small opaque left lung nodule (arrow). B. Posteroanterior chest radiograph 1984: same nodule (H) has enlarged considerably. |
|
|
|
Figure 5.44 Fibrosing mediastinitis. Computed tomography reveals calcified lymph nodes (C) and noncalcified infiltrating soft tissue (F). |
Broncholithiasis occurs when peribronchial calcific nodal disease produces bronchial obstruction. A calcified node may erode into the bronchus and directly obstruct it, or associated inflammation may cause obstruction. Clinically, hemoptysis, fever, chills, and productive cough occur. Broncholiths are more common on the right because of airway anatomy and lymph node distribution. Distal atelectasis, air trapping, and mucus-filled bronchi may occur. Calcified nodes will be seen on radiographs, with atelectasis and dilated branching structures representing fluid-filled bronchi. Chest CT may show the relationship between the calcified lymph node and the dilated bronchus. Bronchiectasis may also be shown.
Fibrosing mediastinitis occurs when nonmalignant fibrous tissue encroaches on and obliterates vasculature and airways of the mediastinum. This process may be focal or generalized, with the former more common. Pathogenesis is unknown. Pathologically, enlarged lymph nodes surrounded by a fibrous capsule are found. Subcarinal and right paratracheal nodes are most commonly involved. Bilateral extension from the subcarinal region carries the worst prognosis. Radiographs show a widened mediastinum from fibrosis or enlarged collateral veins, with lung opacities due to atelectasis or infarcts. Calcification of nodes is usual at CT (Fig. 5.44). The nodes also demonstrate septa that enhance with contrast, separated by low attenuation areas.
Coccidioides immitis
This infection is endemic to the southwestern United States, including southern California, Arizona, New Mexico, southern Utah and Nevada, and western Texas. Thousands of military personnel and their families as well as millions of tourists are exposed to the disease annually. Coccidioidomycosis is acquired by inhalation of arthrospores. The primary target for infection is the lung, and in about 60% of cases the patient is asymptomatic. Symptoms include fever, malaise, substernal or pleuritic chest pain, and cough. Skin rashes occur in two-thirds, including toxic erythema, erythema nodosum, and erythema multiforme.
Chest radiographs may be normal. The most common abnormal radiographic finding is segmental airspace disease (Fig. 5.45) extending out from the hilum (34). This is indistinguishable from other atypical or viral pneumonias. Progression of acute findings to a nodule may be seen over an extended time period. Nodules are usually noncalcified (Fig. 5.46). Hilar lymph node enlargement (Fig. 5.47) is found in 20%, with small unilateral pleural effusions also seen in 20%. Cavitation is seen in 15%, with thin-walled cavities slightly more common than thick-walled ones.
|
|
|
Figure 5.45 Coccidioidomycosis. Multifocal segmental airspace disease, extending out from the hila (P). |
|
|
|
Figure 5.46 Coccidioidomycosis. Archaeology graduate student returned to the University of Michigan from a summer excavation in Arizona with multiple bilateral nodules (arrows). |
|
|
|
Figure 5.47 Coccidioidomycosis. (A) Posteroanterior and (B) lateral chest radiographs demonstrate bilateral hilar lymph node enlargement (N). |
Aspergillus
Aspergillosis results in a spectrum of disease dependent on the virulence and number of organisms and the patient’s immune and pulmonary status (35). Aspergillosis is caused by a ubiquitous soil fungus, usually Aspergillus fumigatus.
Noninvasive aspergillosis occurs when Aspergillus colonizes a preexisting cavity without tissue invasion (Figs. 5.35 and 5.48). Intertwined fungal hyphae mixed with mucus and cellular debris form an aspergilloma or fungus ball. Predisposing causes include TB and sarcoidosis as well as bronchogenic cysts, sequestrations, and pneumatoceles. Patients are usually asymptomatic, with hemoptysis being the most common symptom. Life-threatening hemoptysis is an indication for surgical resection or bronchial artery embolization.
A solid round or oval mass is seen at radiography (35,36). An air crescent is usually visible between the aspergilloma and wall of the cavity. Aspergillomas are usually single. CT shows the relatively high attenuation aspergilloma within the cavity. Change in position of the aspergilloma is usually seen with change in patient position.
Semiinvasive aspergillosis occurs in subjects debilitated by chronic illness, diabetes, malnutrition, alcoholism, advanced age, corticosteroids, or COPD. Clinical symptoms include chronic cough, sputum production, fever, and hemoptysis. The radiographic presentation is unilateral or bilateral segmental airspace disease with or without cavitation and adjacent pleural thickening (35,36). Pleural thickening may be the earliest sign of infection. Multiple nodules may also be seen.
Invasive aspergillosis occurs most commonly in immunocompromised patients and is discussed in Chapter 6.
Allergic bronchopulmonary aspergillosis occurs in patients with longstanding asthma (35). It is an allergic response to inhaled spores, with types I and III hypersensitivity reactions. Aspergillus organisms proliferate in the airway lumen, providing a supply of antigen. Immediate hypersensitivity reaction mediated by IgE occurs. IgG is also produced, and antigen–antibody immune complexes are deposited in the bronchial mucosa. Bronchial wall necrosis and dilation occur with eosinophilic infiltrates. Excess mucous production and abnormal ciliary function lead to mucous impaction. Expectoration of mucous plugs containing aspergillus organisms and eosinophils occurs. Symptoms include wheeze, cough, sputum production, chest pain, and low-grade fever.
Allergic bronchopulmonary aspergillosis causes central bronchiectasis and mucoid impactions.
Radiographically, the characteristic appearance is of central mucoid impactions with tubular often branching structures in a bronchial distribution (“finger-in-glove” appearance) (Fig. 5.49). These represent bronchi plugged with mucus, organisms, and eosinophils. Lobar or segmental atelectasis may be seen. Central bronchiectasis is usually present from previously expectorated mucous plugs. Patchy peripheral consolidations may be seen if there is concurrent eosinophilic pneumonia (Fig. 5.49). CT demonstrates dilated mucous-filled bronchi, often with high attenuation or calcified contents. Upper lobe central bronchiectasis is also well shown.
Nontuberculous mycobacterial infections are often radiologically indistinguishable from postprimary TB.
|
|
|
Figure 5.48 Aspergilloma (A) in a preexisting cavity on (A) chest radiograph and (B) computed tomography. |
|
|
|
Figure 5.49 Allergic bronchopulmonary aspergillosis. Finger-in-glove appearance of mucoid impactions (arrows) and peripheral airspace disease from eosinophilic pneumonia (P). |
Viral Infections
Influenza
Influenza A virus still causes significant morbidity and mortality despite major efforts at prevention and treatment (37,38). Although only a small percentage of infected patients develop pneumonia, those who do have a mortality rate of about 30%. Pneumonia occurs more commonly in the elderly and in those with chronic pulmonary disease. Comorbid illnesses such as diabetes, renal disease, heart disease, and immunosuppression are common. Dyspnea occurs along with the well-known influenza symptoms of fever, chills, myalgias, and cough. Superimposed bacterial infections occur in up to 50%, with S. pneumoniae and S. aureus most commonly isolated. Radiographs generally show bilateral diffuse alveolar (Fig. 5.50) or interstitial opacities. Lobar disease also occurs.
Rubeola (Measles)
Measles is rare in adulthood, and pneumonia is even rarer. Lymph node enlargement occurs before appearance of the rash and regresses shortly after. Pulmonary disease appears at the same time or just before the skin rash and regresses more slowly. Giant cell pneumonia with degeneration and hyperplasia of endothelial cells lining bronchi and bronchioles occurs.
CXR shows increased interstitial opacities with lower lobe predominance (39,40). Marked mediastinal and hilar lymph node enlargement occurs in over two-thirds of cases. Pleural effusions are seen in one-third.
Varicella-Zoster
Pneumonia due to varicella infection in children is rare. In contrast, 10% to 30% of adults infected with chickenpox develop varicella-zoster interstitial pneumonitis. Affected patients are usually very ill, with dyspnea and cough. Diffuse, ill-defined, nodular, airspace opacities (Fig. 5.51) occur throughout the lungs (41). With coalescence, patchy segmental disease is seen. Pleural effusions and lymph node enlargement are not generally demonstrated. Clearing is slow, taking several months. Tiny punctate calcifications may develop in some patients.
|
|
|
Figure 5.50 Influenza pneumonia. Diffuse bilateral airspace disease. |
|
|
|
Figure 5.51 Chickenpox pneumonia. Typical appearance of widespread bilateral ill-defined nodules. |
Parasitic Infections
Echinococcus (Hydatid)
This parasitic infection is caused by the larval stage of the tapeworm Echinococcus. There are two main forms of disease, the most common being cystic unilocular disease caused by Echinococcus granulosis. This organism is widespread throughout the world and prevalent in most sheep- and cattle-raising countries. The parasitic life cycle involves two hosts, the definitive host (a canine, usually a dog) and an intermediate host (usually a grazing animal such as sheep or cattle). The mature adult tapeworm lives in the intestine of the definitive host. Ova are laid and pass to pastures where the intermediate hosts graze. This is the step where humans may be accidentally infected. After ova are ingested, digestive enzymes dissolve the coat, freeing the embryo, which burrows through the duodenal mucosa to enter veins and lymphatics. Most embryos are filtered by the liver, the lungs filter some of the remainder, and a small proportion reach distant organs.
If the host tissues do not destroy the embryos, they transform into tiny cysts. Most (65% to 75%) occur in the liver, with 10% to 25% in the lungs and 10% to 15% in other body tissues. In the thorax, most cysts are intrapulmonary, with only 2% to 5% occurring in the mediastinum, pleura, or diaphragm. Hydatid cysts have three “layers.” The outer pericyst is composed of vascularized connective tissue formed by the host’s response. The ectocyst is the laminated outer layer of the parasite. The innermost layer is the endocyst, consisting of germinating membrane from which daughter cysts and cyst fluid arise.
Most patients are asymptomatic, with incidental discovery of lesions. If cysts rupture, there is abrupt onset of cough, fever, expectoration, and acute hypersensitivity. Occasionally, anaphylaxis occurs. With rupture, viable scolices may be discharged into the peritoneum, mesentery, lung parenchyma, pleura, liver, and/or spleen, causing secondary hydatidosis.
Growth rate of hydatid cysts varies, with sizes more than 20 cm reported. In 60% they are solitary, and in 40% multiple. The lower lobes and posterior lungs are the most frequent sites. In 20% of patients, cysts are bilateral. Calcification of lung cysts is very rare.
Radiographs of an intact “simple” cyst demonstrate a smooth, homogeneous, round or oval well-demarcated nodule or mass (42) (Fig. 5.52). On contrast-enhanced CT and magnetic resonance imaging, the pericyst may enhance. If infarction, hemorrhage, or infection occurs, the clear demarcation with adjacent parenchyma is lost and the hydatid cyst may simulate pneumonia or carcinoma. In these cases a dense or hyperintense halo is seen on CT and magnetic resonance imaging, representing surrounding inflammatory change (43).
|
|
|
Figure 5.52 Echinococcosis. A. Computed tomography at the level of the right pulmonary artery: cyst (C) apparently involving right lower lobe and pleura, with calcification (arrow). B. Computed tomography of upper abdomen: additional cyst (C) between tip of liver (L) and right kidney (K), also calcified (arrow). |
If air enters a cyst after invasion of an airway, a lucent “air crescent” occurs between the pericyst and ectocyst (42). This is a sign of impending cyst rupture. As more air enters a cyst, the parasite shrinks and ruptures with expulsion of cyst contents and entry of air between ectocyst and endocyst. Two air crescents may then be visible with the ectocyst in between, known as the Cumbo sign. CT shows small air lucencies to advantage.
With further collapse, the endocyst membrane may be seen floating on top of any remaining fluid, simulating a water lily (the Camalote sign) (42). On CT and magnetic resonance imaging, the crumpled membranes are seen as curvilinear structures within the pericyst wall, variously called the “serpent sign,” “spin sign,” or “whirl sign” (43).
References
1. Mandell LA. Community-acquired pneumonia: etiology, epidemiology and treatment. Chest 1995;108:35S–42S.
2. Armstrong P, Wilson AG, Dee P, et al. Imaging of diseases of the chest. St. Louis: Mosby, 2000:163–253.
3. Katz DS, Leung AN. Radiology of pneumonia. Clin Chest Med 1999;20:549–562.
4. Franquet T. Imaging of pneumonia: trends and algorithms. Eur Respir J 2001;18:196–208.
5. Tanaka N, Matsumoto T, Kutamitsu, et al. High resolution CT findings in community acquired pneumonia. J Comput Assist Tomogr1996;20:600–608.
6. Tomiyama N, Müller NL, Johkoh T, et al. Acute parenchymal lung disease in immunocompetent patients: diagnostic accuracy of high resolution CT. AJR Am J Roentgenol 2000;174:1745–1750.
7. Genereux GP, Stilwell GA. The acute bacterial pneumonias. Semin Roentgenol 1980: 15:9–16.
8. Berkmen YM. Uncommon acute bacterial pneumonias. Semin Roentgenol 1980;15:17–24.
9. MacFarlane JT, Miller AC, Roderick Smith WH, et al. Comparative radiographic features of community acquired legionnaires disease, pneumococcal pneumonia, mycoplasma pneumonia, and psittacosis. Thorax 1984;39:28–33.
10. Kantor HG. The many radiologic facies of pneumococcal pneumonia. AJR Am J Roentgenol 1981;137:1213–1220.
11. Musher DM, Franco M. Staphylococcal pneumonia. Chest 1981;79:172–173.
12. Naraqi S, McDonnell G. Hematogenous staphylococcal pneumonia secondary to soft tissue infection. Chest 1981;79:173–175.
13. Macfarlane J, Rose D. Radiographic features of staphylococcal pneumonia in adults and children. Thorax 1996;51:539–540.
14. Shafazand S, Doyle R, Ruoss S, et al. Inhalational anthrax: epidemiology, diagnosis and management. Chest 1999;116:1369–1376.
15. Penn C, Klotz SA. Anthrax pneumonia. Semin Respir Infect 1997;12:28–30.
16. Earls JP, Cerva D, Berman E, et al. Inhalational anthrax after bioterrorism exposure: spectrum of imaging findings in two surviving patients. Radiology 2002;222:305–312.
17. Ritvo M, Martin F. The clinical and roentgen manifestations of pneumonia due to bacillus mucosus capsulatus (primary Friedlander pneumonia). AJR Am J Roentgenol 1949;62:211–225.
18. Holmes RB. Friedländer’s pneumonia. Radiology 1956;75:728–743.
19. Moon WK, Im JG, Yeon M, et al. Complications of Klebsiella pneumonia: CT evaluation. J Comput Assist Tomogr 1995;19:176–181.
20. Lipchik RJ, Kuzo RS. Nosocomial pneumonia. Radiol Clin North Am 1996;34:47–57.
21. Winer-Muram HT, Jennings SG, Wunderink RG, et al. Ventilator-associated Pseudomonas aeruginosa pneumonia: radiographic findings. Radiology 1995;195:247–252.
22. Shah RM, Wechsler R, Salazar AM, et al. Spectrum of CT findings in nosocomial Pseudomonas aeruginosa pneumonia. J Thorac Imag2002;17:53–57.
23. Tan MJ, Tan JS, Hamor RH, et al. The radiologic manifestations of Legionnaires disease. Chest 2000;116:398–403.
24. Franquet T, Gimenez A, Roson N, et al. Aspiration diseases: findings, pitfalls, and differential diagnosis. Radiographics 2000;20:673–685.
25. Kwong S, Muller NL, Goodwin JD, et al. Thoracic actinomycosis: CT findings in eight patients. Radiology 1992;183:189–192.
26. Marrie TJ. Pneumonia caused by Nocardia species. Semin Respir Infect 1994;9:207–213.
27. McConnell CT, Plouffe JF, File TM, et al. Radiographic appearance of Chlamydia pneumoniae (TWAR strain) respiratory infections.Radiology 1994;192:819–824.
28. Cameron DC, Borthwick RN, Philp T. The radiographic patterns of acute Mycoplasma pneumonitis. Clin Radiol 1977;28:173–180.
29. Reittner P, Muller NL, Heyneman L, et al. Mycoplasma pneumoniae pneumonia: radiographic and high-resolution CT features in 28 patients. AJR Am J Roentgenol 2000;174:37–41.
30. Leung AN. Pulmonary tuberculosis: the essentials. Radiology 1999;210:307–322.
31. Miller WT. Spectrum of pulmonary nontuberculous mycobacterial infection. Radiology 1994;191:343–350.
32. Rosenzweig DY. Nontuberculous mycobacterial disease in the immunocompetent adult. Semin Respir Infect 1996;11:252–261.
33. Gurney JW, Conces DJ. Pulmonary histoplasmosis. Radiology 1996;199:297–306.
34. Greendyke WH, Resnick DL, Harvey WC. The varied roentgen manifestations of primary coccidioidomycosis. AJR Am J Roentgenol1970;109:491–499.
35. Franquet T, Muller NL, Gimenez A, et al. Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findings.Radiographics 2001;21:825–837.
36. Aquino SL, Kee ST, Warnock ML, et al. Pulmonary aspergillosis: imaging findings with pathologic correlation. AJR Am J Roentgenol1994;163:811–815.
37. Olivera EC, Marik PE, Colice G. Influenza pneumonia. A descriptive study. Chest 2001;119:1717–1723.
38. Janower ML, Weiss EB. Mycoplasmal, viral and rickettsial pneumonias. Semin Roentgenol 1980;15:25–32.
39. Quinn JL. Measles pneumonia in an adult. AJR Am J Roentgenol 1964;91:560–563.
40. Margolin FR, Gandy TK. Pneumonia of atypical measles. Radiology 1978;131:653–655.
41. Sargent EN, Carson MJ, Reilly ED. Roentgenographic manifestations of varicella pneumonia with postmortem correlation. AJR Am J Roentgenol 1966;98:305–317.
42. Balikian JP, Mudarris FF. Hydatid disease of the lungs. A roentgenologic study of 50 cases. AJR Am J Roentgenol 1974;122:692–706.
43. Von Sinner WN. New diagnostic signs in hydatid disease: radiography, ultrasound, CT and MRI correlated to pathology. Eur J Radiol1991;12:150–159.