Questions
1. 221. The following are potential complications of aortic valve endocarditis:
1. A. Aortic root abscess
2. B. Supra-annular mitral regurgitation
3. C. Aneurysm of mitral–aortic intervalvular fibrosa
4. D. Aneurysm of anterior mitral leaflet
5. E. All of the above
2. 222. The following statements are true about patent foramen ovale except:
1. A. Pick-up rate is higher with saline contrast compared to color Doppler imaging
2. B. Transesophageal echocardiogram (TEE) is more sensitive than transthoracic echocardiogram
3. C. Yield is higher with leg injection compared to arm injection for saline contrast
4. D. Present in about 50% of normal population
3. 223. Saline contrast echocardiography in a patient with cirrhosis of the liver showed appearance of contrast in the left atrium five beats after its appearance in the right atrium. This is suggestive of:
1. A. Normal physiology
2. B. Hepatopulmonary syndrome
3. C. Patent foramen ovale
4. D. Portopulmonary syndrome
4. 224. Which type of aortic valve is least likely to be repairable for correction of severe aortic regurgitation?
1. A. Failure of leaflet coaptation due to severely dilated ascending aorta with structurally normal leaflets
2. B. Bicuspid aortic valve with prolapse of the conjoint cusp
3. C. Aortic intramural hematoma with extension to the base of right coronary cusp causing it to prolapse
4. D. Rheumatic aortic valve disease
5. 225. TEE was performed intraoperatively following coronary artery bypass grafting (CABG) because of failure to wean from cardiopulmonary bypass. It showed akinetic inferior wall with 3+ mitral regurgitation originating at the medial commissure. These findings were not present preoperatively. The inferior wall looked excessively bright. Most likely problem in this patient is:
1. A. Air embolism into right coronary artery (RCA)
2. B. Thrombosis of RCA graft
3. C. Excessively high blood pressure
4. D. Excessive intravascular volume
5. E. Poor myocardial preservation
6. 226. The image is suggestive of: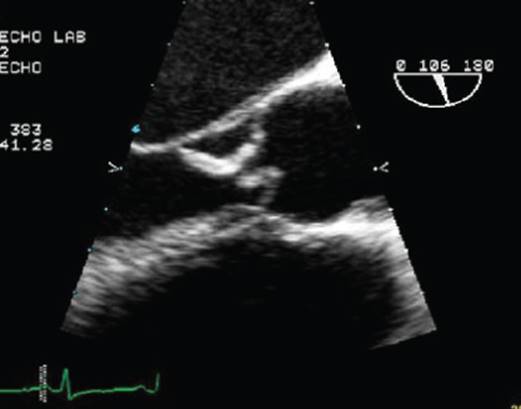
1. A. Aortic dissection
2. B. Aortic valve endocarditis
3. C. Unicuspid aortic valve
4. D. Hypertrophic cardiomyopathy
7. 227. Continuous wave Doppler shown here could be a result of: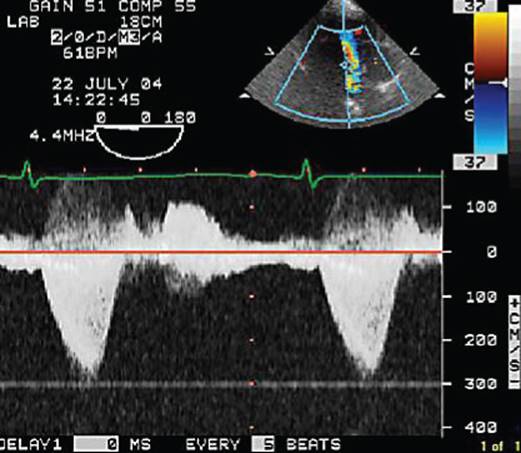
1. A. Hypertrophic obstructive cardiomyopathy
2. B. Severe mitral regurgitation
3. C. Tricuspid regurgitation
4. D. Ventricular septal defect
8. 228. In this figure, number “1” denotes: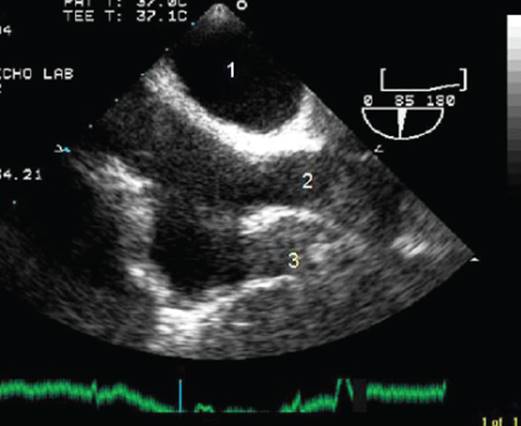
1. A. Left atrium
2. B. Right atrium
3. C. Aorta
4. D. Right pulmonary artery
9. 229. In the figure, number “2” is:
1. A. Superior vena cava
2. B. Inferior vena cava
3. C. Pulmonary artery
4. D. Aorta
10. 230. In the figure, number “3” denotes:
1. A. Left atrium
2. B. Right atrial appendage
3. C. Inferior vena cava
4. D. None of the above
11. 231. This image shows: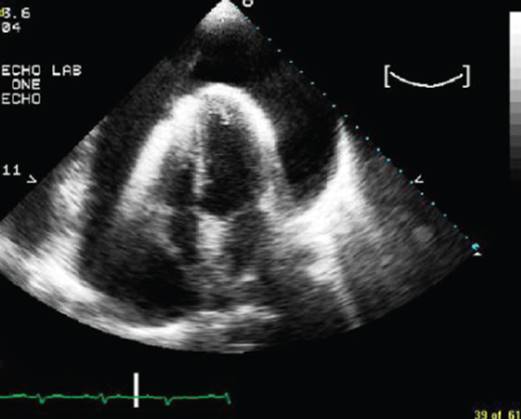
1. A. Large left pleural effusion
2. B. Large pericardial effusion with no evidence of tamponade
3. C. Large pericardial effusion with features of tamponade
4. D. Mirror image artifact
12. 232. This mitral inflow pattern is consistent with: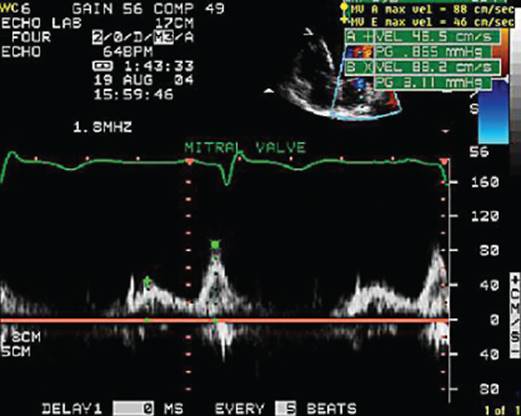
1. A. Abnormal left ventricular (LV) relaxation with elevated left atrial (LA) pressure
2. B. Abnormal LV relaxation with normal LA pressure
3. C. Pseudonormal filling
4. D. Restrictive LV filling
13. 233. The part of the flow curve denoted by the arrow in this pulmonary vein flow is caused by: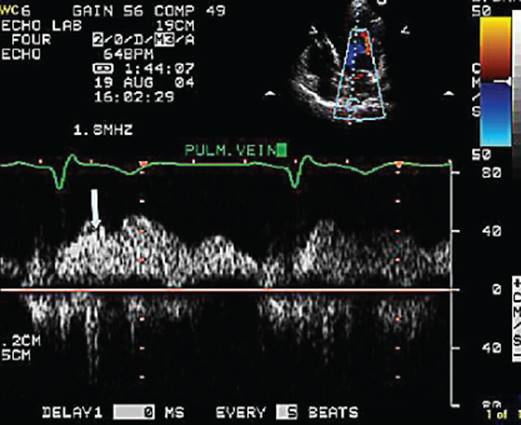
1. A. Left atrial relaxation
2. B. RV ejection
3. C. Mitral valve opening
4. D. Mitral annular descent
14. 234. The patient shown here has: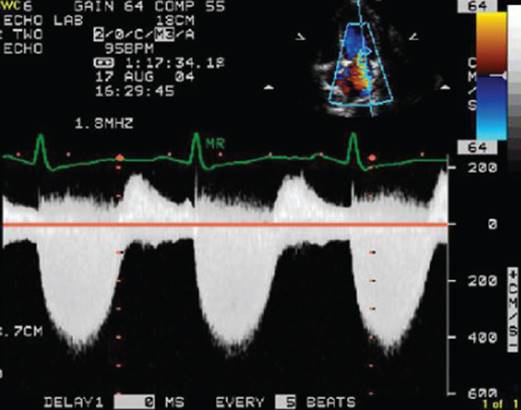
1. A. Severe mitral regurgitation
2. B. Severe mitral stenosis
3. C. Severe aortic stenosis
4. D. Mild mitral regurgitation
15. 235. The mitral inflow pattern is consistent with: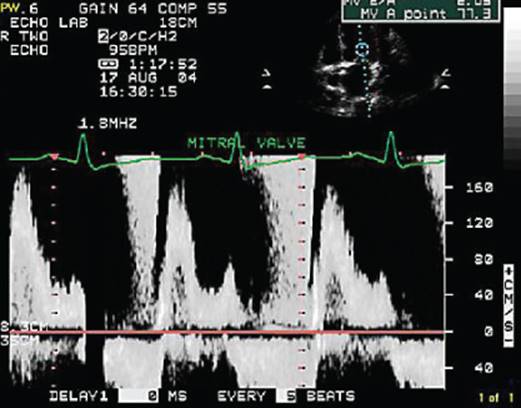
1. A. Severe mitral regurgitation
2. B. Severe mitral stenosis
3. C. Prosthetic mitral valve
4. D. Atrial fibrillation
16. 236. In the image shown here, the arrow denotes: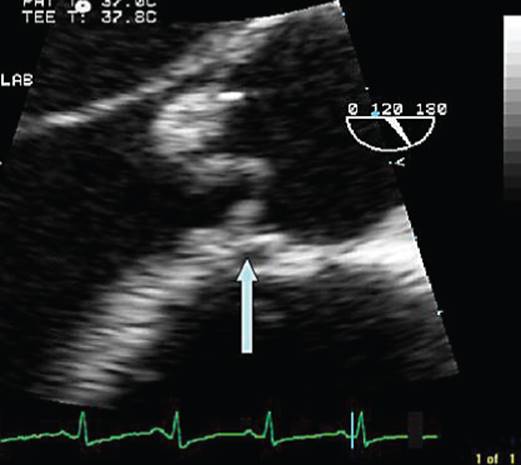
1. A. Right coronary artery
2. B. Coronary sinus
3. C. Aortic ring abscess
4. D. Prosthetic valve dehiscence
17. 237. The aortic valve shown here is: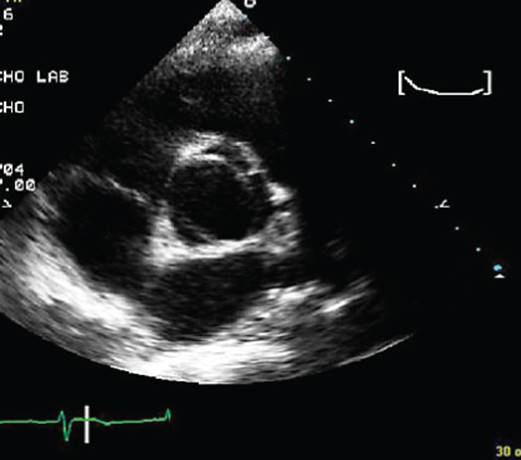
1. A. Tricuspid
2. B. Unicuspid
3. C. Bicuspid with conjoint right and left cusp
4. D. Bicuspid with conjoint left and noncoronary cusps
18. 238. The TEE image shows: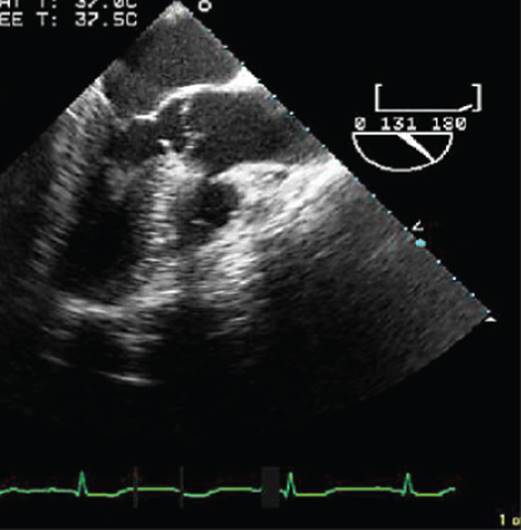
1. A. Subaortic membrane
2. B. Vegetation
3. C. Artifact
4. D. Aortic aneurysm
19. 239. The Doppler signal is indicative of:
1. A. Significant mixed aortic valve disease
2. B. Significant mixed mitral valve disease
3. C. Significant mixed tricuspid valve disease
4. D. Hypertrophic obstructive cardiomyopathy
20. 240. For the patient in the above question the LV end diastolic pressure is likely to be:
1. A. Low
2. B. Normal
3. C. Elevated
4. D. Cannot comment
Answers for chapter 12
1. 221. Answer: E.
All of the above. In addition, patients may get aorto-LV fistula, aorto-RV fistula, aorto-RA fistula, anterior mitral leaflet perforation, rupture of the mitral aortic intervalvular fibrosa, atrioventricular blocks, pyogenic pericarditis, etc.
2. 222. Answer: D.
It is present in about 25% of the normal population. Detection rate is higher with TEE and saline injection especially from the leg, which simulates the direction of flow during fetal life.
3. 223. Answer: B.
Owing to the formation of pulmonary A–V fistulae (caused by “hepatic factor”). This is called hepatopulmonary syndrome. Portopulmonary syndrome refers to pulmonary hypertension secondary to chronic liver disorders. Late appearance of bubbles in the left atrium is indicative of transpulmonary rather than inter atrial shunting.
4. 224. Answer: D.
For valve sparing surgery, leaflets should be structurally near normal. In situation A, replacement of ascending aorta may eliminate AR, and in situation C, prolapsing leaflets can be resuspended during repair.
5. 225. Answer: A.
Akinetic wall signifies ischemia, and brightness indicates air embolism into RCA, the common artery to be affected because of its anterior origin from the aorta. Poor myocardial preservation would cause global hypokinesis. Mitral regurgitation (MR) in this patient is typically ischemic because of inferior wall motion abnormality.
6. 226. Answer: B.
Large vegetations are seen on the aortic valve. Ascending aorta is normal sized with no visible flap. Unicuspid aortic valve can be diagnosed only in the short axis view showing only a single cusp and a single commissure. In this example, there is a large vegetation on the noncoronary cusp and a smaller one on the right coronary cusp.
7. 227. Answer: A.
Late peaking systolic signal is indicative of dynamic LV outflow tract obstruction, which is most severe in end systole when the LV volume is minimal. The timing corresponds to LV ejection and begins following a period after the onset of the QRS signal. There is a gap between the end of the signal and onset of mitral inflow. The MR signal occupies not only the ejection period but also the isovolumic contraction and relaxation periods and is a longer duration signal and is continuous with the mitral inflow without any intervening gap. The tricuspid regurgitation (TR) signal is similar but tends to be broader with a lower velocity inflow. The cursor position, if visible, is also helpful to identify the origin of the signal. The ventricular septal defect signal is holosystolic but generally tends to have a presystolic component due to left atrial contraction.
8. 228. Answer: A.
This TEE long axis view of the left atrium and right atrium is also popularly called a bicaval view; the left atrium is immediately anterior to the esophagus.
9. 229. Answer: A.
In a vertical or near vertical plane, the right side is cephalad and the left side is caudal.
10. 230. Answer: B.
Right atrial appendage.
11. 231. Answer: C.
This figure shows pericardial effusion with features of tamponade (right atrial collapse).
12. 232. Answer: B.
Abnormal LV relaxation pattern includes prolonged LV isovolumic relaxation time (>100 ms), E/A ratio < 1, and E-wave deceleration time > 250 ms.
13. 233. Answer: A.
The arrow denotes the S1 wave, which is caused by left atrial relaxation. RV ejection and mitral annular descent generate the S2 wave, which follows the S1 wave. The mitral valve opening generates the D-wave, which is synchronous with the mitral E-wave.
14. 234. Answer: A.
The timing of the signal starts with the QRS complex and the end, being continuous with the onset of mitral inflow, suggests MR. A density approaching that of mitral inflow suggests this to be severe. Other clues to severe MR could be a “V-wave cut-off sign” and mitral inflow suggestive of high LA pressure.
15. 235. Answer: A.
The presence of an A-wave excludes atrial fibrillation, mitral stenosis, and prosthetic mitral valve. The E-wave deceleration will be slow. The inflow pattern shown here indicates high left atrial pressure typified by E/A ratio > 2 and E-wave deceleration of <150 ms and is consistent with severe MR.
16. 236. Answer: C.
This patient has native aortic valve endocarditis with an anterior aortic ring abscess shown by the arrow. In patients with aortic valve endocarditis it is imperative to look for aortic root, ring, or the mitral aortic intervalvular fibrosa. TEE is superior to transthoracic echocardiogram for this purpose.
17. 237. Answer: D.
Bicuspid with conjoint left and noncoronary cusps.
18. 238. Answer: A.
Note the membrane attached to the ventricular septum beneath the aortic valve. This is thin and uniformly membranous in appearance.
19. 239. Answer: A.
The systolic signal does not begin with the onset of QRS, which is typical of MR or TR. Hence, this is indicative of aortic stenosis (AS) with aortic regurgitation (AR). The AS signal is midpeaking, which correlates with a slow rise in aortic pressure, as the kinetic energy associated with the jet is very significant and this results in a corresponding drop in potential energy. Note that the end of the AS signal is continuous with the AR signal and vice versa. This indicates the origin of the signals at the same valve.
20. 240. Answer: C.
Note the rapid deceleration of the AR signal and the late diastolic gradient between LV and aorta is only 16 mmHg when applying the simplified Bernoulli equation to the late diastolic AR velocity.