![]()
Erythroxylum coca

An Andean man with a coca offering in Cuzco, Peru. Among the Inca and their descendents, coca is a sacred plant.
Coca grows as a perennial shrub with simple, oval, hairless dark green leaves. It reaches a height of 2 to 3 meters in cultivation and can grow taller if left unpruned. Small whitish five-petaled flowers appear on short stems arising from the leaf nodes and produce olive-shaped, pea-size fruits that turn red at maturity (figure 6.1). The leaves are harvested for medicinal use. The genus Erythroxylum contains hundreds of species, only a handful of which are used medicinally. E. coca, the most widely cultivated type, exists in two geographically distinct varieties. E. coca var. coca grows in the humid tropical mountain forests in the eastern Andes region of South America, currently occupied by Ecuador, Peru, and Bolivia. E. coca var. ipadu grows in the lowland Amazon basin. The closely related E. novogranatense is cultivated in drier forest and desert areas in Venezuela, Colombia, Ecuador, and Peru.1
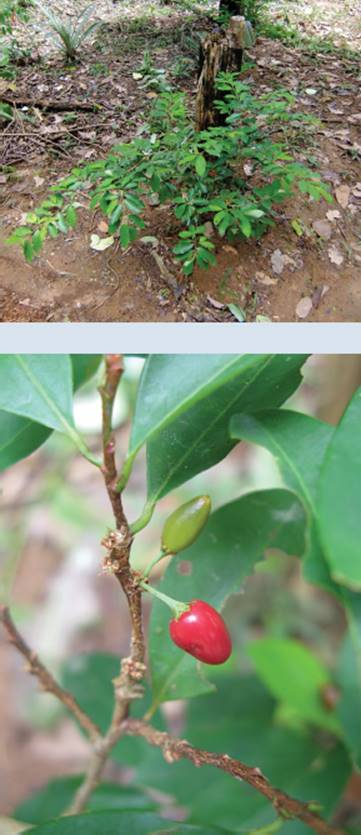
FIGURE 6.1 Coca: (top) plant; (bottom) fruit.
ANCIENT USE IN THE ANDEAN REGION
Ancient people recognized the stimulating properties of coca, and the practice of chewing its leaves is at least 2000 years old (figure 6.2).2 Coca produces a feeling of increased energy and suppresses thirst and hunger, properties that must have been useful in societies established around mountain life. Even in the modern era, individuals facing strenuous mountain hikes chew coca leaves to sustain their endurance and cope with changes of altitude.
Archaeological relics and folklore indicate that coca had deep spiritual significance for people in northern South America. Artifacts from Peru including human figures and decorated vessels dating to at least 500 C.E. depict what are thought to be priests chewing coca, a connection between the plant and religious practice. Among ancient peoples and their descendents, coca was thought to be a physical manifestation of the divine.3
Evidence of coca use is present in Andean mummies predating by many centuries the rise of the dominant Inca Empire. During the time of the early Inca civilization in roughly the thirteenth century, agriculturalists began growing coca in plantations and systematically harvesting the leaves for use in trade. The Incas probably used coca as a sort of tribute to the hierarchy of nobles and as a reward to workers and travelers, sustaining their difficult labors. Much of the Inca Empire extended high into the Andes and deep into gold and silver mines, and coca served to reenergize tired muscles and enhance endurance.
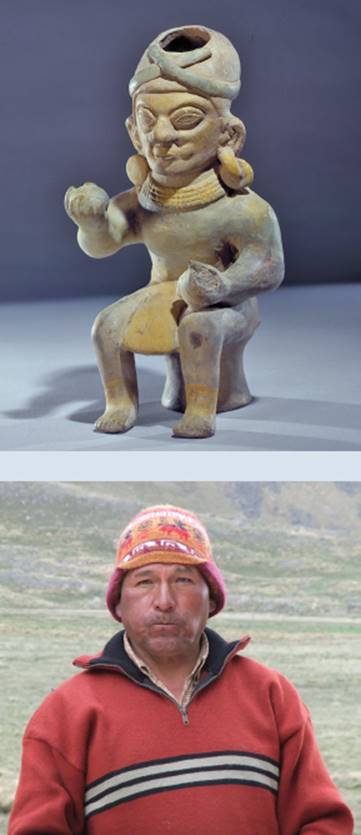
FIGURE 6.2 Coca chewing: (top) Andean peoples produced statuettes depicting coca chewing more than 1000 years ago; note the bulging cheeks in this Jama-Coaque clay figurine, ca. fifth century; (bottom) a coquero of the South American high plains. ([top] Photograph © Justin Kerr K7886, www.mayavase.com)
Traditionally, coca has been consumed by chewing the fresh leaves mixed with a small amount of crushed sea-shells, limestone, or ashes.4 Coqueros (leaf chewers), as the Spanish explorers called them, typically carried with them a pouch containing coca leaves and another holding the alkaline powder needed to release the stimulant more effectively. Fresh coca leaves contain 0.5 to 2 percent of the psychoactive alkaloid cocaine, which is released from the leaves by the abrasive action of the gritty powder and chemically transformed by its basic (rather than acidic) property (figure 6.3).5 In its basic form, cocaine readily passes into the bloodstream through the coquero’s gums and tongue. (Although the oral route of coca consumption is usually called “chewing,” it is more properly characterized as “sucking,” since the user keeps the coca leaf quid in his mouth for thirty or more minutes and swallows the juices that form by mixing with his saliva.)6
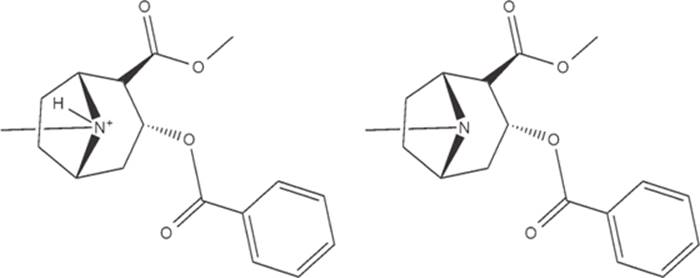
FIGURE 6.3 Cocaine can be converted between its acid (left) and base (right) forms.
COCA AND THE SPANISH CONQUEST
During the sixteenth century, the explorer Francisco Pizarro (1476?–1541) and his countrymen began to disassemble the Inca Empire and bring it under Spanish domination. As part of the process, the coca plantations came under European ownership, and many Inca were converted to Christianity. While many natives did not have access to gold and silver (much of it confiscated for shipment back to Spain), they did have ready supplies of coca, which the authorities accepted as payment for taxes and church tithes.7 Under Spanish rule, coca became a cash crop and means of exchange among the subjugated Inca. The Spanish established gold and silver mines to extract the mineral wealth of the former Inca territories, and the mine workers were a chief source of demand for coca.
At Potosí (in modern-day Bolivia), the colonial government operated a silver mine employing forced labor (figure 6.4). The indigenous laborers were poorly fed and overworked, and they struggled against harsh conditions in a mine at an elevation of approximately 4800 meters. All the while, they were well supplied with coca, which staved off hunger and provided temporary relief from fatigue and pain. Indeed, records indicate that mine workers spent twice as much on coca as on food and clothing.8
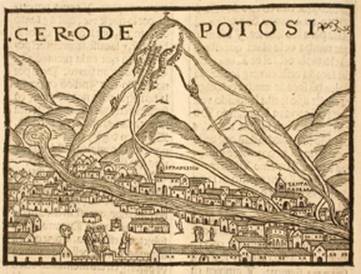
FIGURE 6.4 Indigenous workers in Spanish mines survived the difficult conditions by chewing coca. (Woodcut of the mines at Potosí, from Pedro de Cieza de Léon, Chrónica del Péru [1553]; Courtesy Lilly Library, Indiana University, Bloomington, F3442.C29)
Under colonial rule, coca served to ease the discomforts of hard work and lack of self-determination. As an indigenous product, it retained its long-standing spiritual significance and embodied the shared cultural heritage of Andean peoples. Coca chewing continued in rural and urban areas as a form of connection to a storied past, providing a stimulating diversion from the workday in its chewed form; today it is also packaged as an herbal tea, mate de coca.
In their missionary zeal, some Spanish colonialists treated ancestral practices involving the revered coca leaf as an abomination. Beginning in the 1560s, officials of the Spanish state and Catholic Church issued dozens of edicts targeted at stamping out indigenous coca use, epitomized by a 1569 pronouncement by the bishops of Lima that called coca “a deception of the devil.”9 However, the attempts to suppress coca use were unsuccessful, as the indigenous people ignored such decrees, and the local administrative structures continued to embrace the coca leaf as currency. Meanwhile, a number of writers recorded coca’s diverse health benefits, informed by the local people. For example, the Spanish physician Nicolás Monardes (1493–1588) compiled reports of coca’s hunger- and thirst-suppressing properties in a 1565 treatise on New World medicinal plants.10 Another sixteenth-century colonial writer recorded that coca “preserves the body from many infirmities,” can “ease and assuage the inflammation, or swelling of the wound,” expels “colds from the body,” and “is good also to cleanse great wounds of worms.”11
ISOLATION OF COCA’S ACTIVE PRINCIPLE
Although coca’s value in Andean commerce and indigenous spiritual and medical practice was recognized in the years following the Spanish conquest, coca use remained the custom of certain regions of South America without garnering much attention beyond. This circumstance is likely related to the long voyages necessitated by early transatlantic trade. While fresh coca leaves are rich in cocaine (figure 6.5), the leaves travel poorly; when coca leaves first reached European botanists and chemists in the eighteenth century, they had deteriorated and lost nearly all their medicinal properties. This rapid degradation presented problems for those interested in studying the plant’s possible usefulness. European doctors took an interest in reports of the plant’s stimulating effects, but until the problem of leaf freshness could be resolved, any scientific study had to occur in South America.

FIGURE 6.5 Coca leaves for sale at a market in Peru.
The Swiss naturalist Johann von Tschudi (1818–1889) undertook a four-year (1838–1842) journey through Peru and wrote a description of the people, plants, and animals he encountered—he was among the first trained scientists to do so—and became a coca proponent. He interviewed indigenous coca chewers and took coca himself by chewing and as a tea. He returned to Europe considering that coca was “in no way detrimental” and “may even be very conducive to health.”12
To understand better the stimulating properties of coca, chemists wanted to purify the active principle from the leaf. The German chemist Albert Niemann (1834–1861) was the first to accomplish this task, and he wrote his doctoral dissertation in 1859/1860 on the isolation of the chemical he called cocaine. As cocaine degenerated so quickly in leaves, he needed to import 27 kilograms of coca leaves from Peru to perform his analysis.13
The extraction process that Niemann pioneered is used in the modern day largely unchanged. Once isolated from the coca leaves, cocaine is stable and can be subsequently distributed and manipulated with efficiency. To extract cocaine, the coca leaves are harvested, mashed, and soaked in water with added alkali (such as lime) for three to four days. Cocaine in its acidic form is soluble in water, but in its basic form it is much more soluble in an organic solvent such as ether, gasoline, or kerosene (see figure 6.3). To extract fully the basic cocaine, an organic solvent is added to the mashed leaves, mixed well, and withdrawn to another container. On the addition of an acid, such as hydrochloric acid, the cocaine salt (cocaine hydrochloride) precipitates from solution as a pure, white powder.14
The cocaine acid’s salt form passes moderately well through the moist mucous membrane surfaces of the nose and mouth and, being water soluble, lends itself well to injection or drinking. Indeed, the primary methods of medical use during the late nineteenth century were application to the surface of the body, injection by syringe, and drinking mixed with water or alcohol. Cocaine hydrochloride is not suitable for smoking, because it breaks down (rather than vaporizes) when heated, rendering it ineffective. During the 1970s and 1980s, illicit cocaine distributors in the United States developed a novel form of cocaine that vaporizes with heat, thereby retaining its physiological effects when smoked. By dissolving cocaine hydrochloride in water, adding an alkali such as ammonia, and extracting in an organic solvent such as ether, they produced cocaine in its free base form. After evaporating the solvent, the hard, caked, whitish substance is amenable to smoking in the form of small rocks rolled into cigarettes or burned in the bowls of pipes. The smoke of this variety of cocaine, called crack after the sound it makes when heated, contains vapors of the free base that pass quickly through the lung membranes into the bloodstream, producing a rapid physiological response.15
The scientific attention given to cocaine during the nineteenth century gave rise to an extraction procedure still used in the modern day and an understanding of the chemical properties that govern how cocaine is consumed. It also spawned enormous curiosity in the medical community, which saw cocaine as a powerful new potential therapeutic chemical. The second half of the nineteenth century witnessed a great deal of cocaine experimentation.
COCAINE IN NINETEENTH-CENTURY EUROPEAN MEDICINE
The chemical isolation being rather straightforward and medical interest mounting, the German pharmaceutical firm Merck began extracting cocaine in 1862, adding to its catalog of plant-derived stimulants alongside caffeine and nicotine.16 Among the earliest uses of coca during the 1860s is in sports medicine, when it was employed frequently, usually by ingestion, as a health supplement and performance enhancer.
Of increasing popularity during the nineteenth century were health tonics and potions produced by pharmacists (or entrepreneurs claiming medical authority) and advertised to cure a wide range of real or imagined ailments. One of the more famous of these elixirs was produced by the Corsican businessman Angelo Mariani (1838–1914) beginning in 1863.17 His Vin Mariani was the first coca wine, cheap red wine spiked with cocaine.18 It is estimated that each glass of Vin Mariani contained 25 milligrams of cocaine, meaning that one or two glasses would have an appreciable stimulant effect and convince consumers of its medicinal merits. Mariani became a master at self-promotion, with innumerable celebrity and doctor endorsements, big-budget advertising, and worldwide distribution. His success also spawned many imitators selling coca wines and sherries (figure 6.6).19
Mariani soaked coca leaves in wine to extract some of its cocaine into the beverage; however, the process also leached unpleasant flavors into the wine. Pharmacists responded to this complaint by selling “essences” (alcohol solutions) of cocaine for consumers to add to wine on their own. These variously marketed medicinal coca wines and Peruvian wines of coca were of increasing cocaine potency and remained popular past the turn of the twentieth century. They undoubtedly presented risks to their consumers: unknown to medicine at the time, cocaine taken with alcohol produces in the body a substance called cocaethylene, nearly as stimulating as cocaine, longer lasting, and much more toxic (figure 6.7).20
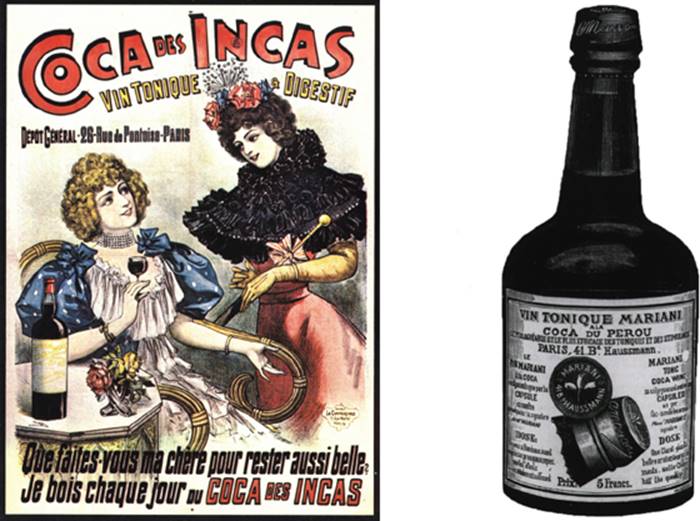
FIGURE 6.6 Coca wine, a nineteenth-century medicinal tonic: (left) an advertisement for a beverage called Inca Coca, 1896 (the text reads: “What do you do, my dear, to stay so beautiful? Every day, I drink Inca Coca”); (right) an advertising print for Vin Mariani, ca. 1890. ([left] National Library of Medicine, 216167; [right] National Library of Medicine, 139407)
COCA-COLA
One of Mariani’s imitators was John Stith Pemberton (1831–1888), a pharmacist with medical training who established a drugstore in Columbus, Georgia, in 1855. He later moved his business to Atlanta and, inspired by the success of the coca wines, formulated Pemberton’s French Wine Coca in 1884.21 He marketed his coca wine, a complex mixture of medicinal herbs, as containing Peruvian coca, African cola nuts,22 and “true Damiana.”23 Advertisements for Pemberton’s coca wine claimed that it could cure mental and physical exhaustion and served as “a most wonderful invigorator of the sexual organs.”24 The coca wine sold well in Georgia during its first few years; however, when Atlanta outlawed alcohol in 1885, Pemberton was forced to reformulate his product. While Atlanta’s prohibition lasted only a year, the new soft coca drink, Coca-Cola, remained.
Drugstore and restaurant soda fountains, growing in popularity during the 1890s and 1900s, provided Pemberton ample sales venues to young and old customers alike. While he continued to claim the health benefits of his cola drink, he did not need to sell it as medicine alone. Actually, Coca-Cola during this period had very little cocaine—perhaps 1 to 2 milligrams per ounce, probably too little to cause much of an effect—and no alcohol. By 1903, cocaine was dropped from the Coca-Cola formula and additional caffeine added to produce a more significant stimulant effect. The Coca-Cola formula continued to use coca leaves (as it does today, in decocainized form) as flavoring.25
While Mariani’s coca wine and Pemberton’s Coca-Cola claimed health benefits from the relatively low levels of coca extract present in their tonics, other widely advertised medicines and home remedies provided cocaine in much higher doses. Around the turn of the twentieth century, Dr. Tucker’s Asthma Specific was a patent medicine for respiratory ailments containing up to 450 milligrams of cocaine per ounce (the equivalent of nine “lines” of powder cocaine).26 Meanwhile, Coca-Bola, a quack medical chewing gum, packed 710 milligrams of cocaine per ounce, a potentially lethal dose.27
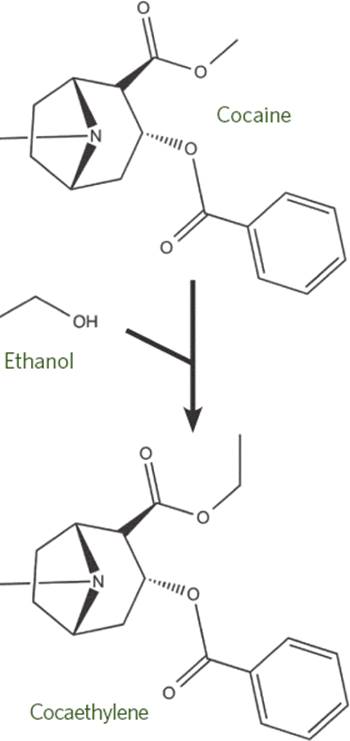
FIGURE 6.7 The enzymatic conversion of cocaine and ethanol into the longer-lasting product cocaethylene.
SIGMUND FREUD AND THE PROMOTION OF COCAINE
The medicinal claims about cocaine would not have been possible without the energetic endorsement years earlier by a young doctor in Vienna, Sigmund Freud (1856–1939 [figure 6.8]). In 1884, he published a review of the available literature on cocaine, supplemented with self-experimentation, called Über Coca (On Coca).28 In it, he proposed that the drug could be used as
• A mental stimulant
• A treatment for digestive disorders
• An appetite stimulant in cases of wasting disease
• A treatment for morphine and alcohol addiction
• A treatment for asthma
• An aphrodisiac
• A local anesthetic
Freud worked closely with his friend the Vienna ophthalmologist Karl Koller (1857–1944 [figure 6.9]), reportedly injecting cocaine into themselves and testing muscle strength, among other attributes. Indeed, Freud’s personal use of cocaine as an antidepressant and aphrodisiac contributed to his vigorous promotion of these therapeutic uses. Koller tested the use of cocaine as a local anesthetic for eye surgery and presented its success at a surgical conference in 1884. Shortly thereafter, cocaine use spread widely as the first effective local anesthetic applied directly to tissue for nose, mouth, urogenital, and other surgeries.29 When injected under the skin, in contact with nerve fibers, it numbed the surrounding region as a peripheral nerve block and allowed the first relatively painless dental procedures. The impact of Koller’s discovery is enduring: cocaine is still used as a topical anesthetic in certain eye, nose, and throat procedures, although because of the risk of adverse reaction, cocaine has largely been replaced with synthetic anesthetics.30
FIGURE 6.8 Sigmund Freud, 1891. (Wellcome Library, London, L0015371)

FIGURE 6.9 Karl Koller, early twentieth century. (Photograph by Alman Company; National Library of Medicine, 182026)
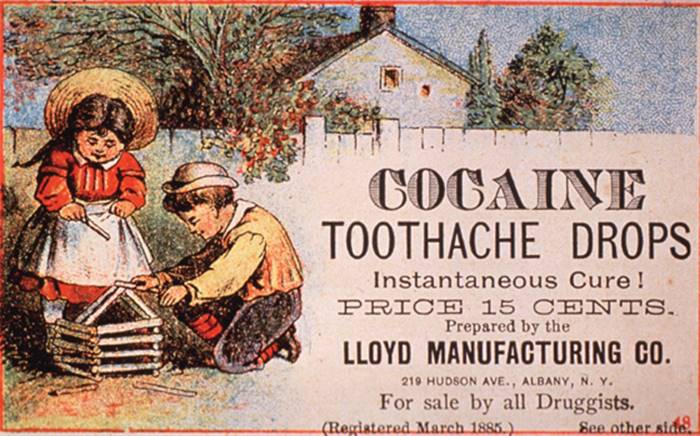
FIGURE 6.10 Cocaine-based anesthetics made their way into American homes during the late nineteenth century, as seen on this trade card. (National Library of Medicine, 148130)
The consequences of the work of Freud and Koller, among a cohort of physicians who experimented with cocaine during this time, were dramatic. The German pharmaceutical firm Merck, which was the largest manufacturer of its era, produced only 300 grams of cocaine in 1882, and then 1.41 kilograms in 1883, a number that advanced to 30 kilograms in 1884 and 70 kilograms in 1885; by 1886, annual production had increased to 257 kilograms.31 Cocaine sales underwrote the success of the large, now multinational Merck pharmaceutical firm, along with the German company Boehringer and the American firms Parke-Davis and Squibb.32 It is interesting that during the late nineteenth and early twentieth centuries, cocaine production greatly outweighed the established medical need.33 No doubt, many individuals leaned on cocaine for self-medication and recreation in an era when medical products were readily available, without a prescription, by mail order and in shops (figure 6.10).
PATH TO CRIMINALIZATION IN THE UNITED STATES
By the second decade of the twentieth century, many Americans had succumbed to cocaine or morphine dependencies through medical or recreational use of extracts and patent medicines. Increasingly in the public eye, cocaine and morphine together formed a class of potentially dangerous drugs whose regulation was in the national interest.34 However, federal legislation to restrict individual freedoms in medical or recreational choice was unheard of in the United States during this period. Through a series of carefully crafted public messages, printed in such newspapers as the New York Times, anti-cocaine campaigns effectively linked cocaine use by black Americans to unspeakable dangers to the white community.35 Vilified in this way, cocaine was outlawed for all but a small number of medical uses by the Harrison Narcotics Tax Act of 1914.36
The United Nations widened the ban worldwide with the Convention on Narcotic Drugs (1961, extended in 1988), which prohibits the export of coca or cocaine by all signatory countries and permits its domestic production and consumption only where local law allows. While much of South America has maintained restrictions to varying degrees on coca production and use, some countries permit coca chewing and mate de coca drinking for cultural reasons. Recent populist politicians in South America, such as the president of Bolivia, Evo Morales (b. 1959), and the late Venezuelan leader Hugo Chávez (1954–2013), have swept to power on platforms that promoted unhindered access to coca. To many in South America, defense of coca equates with support for indigenous culture, human rights, and self-determination.
MECHANISM OF ACTION
Cocaine, in its various forms, can be taken by mouth, by injection, by application to thin skin, or by smoking. Cocaine causes numbness and constricts blood vessels when it comes into contact with the mucous tissues of the mouth, nose, eyes, or genitals. From there, it is slowly absorbed through the skin into the blood. Once in the bloodstream, it acts in the brain to increase heart rate and blood pressure and gives the user a feeling of elevated energy and mood. It also produces a sense of pleasure and reward, which is responsible for its addictiveness.
Cocaine exerts its effects through several mechanisms. As a local anesthetic, it blocks the transmission of electrical signals along the axons of sensory neurons.37 As a vasoconstrictor, it causes blood vessels to tighten strongly on contact.38 The constriction of blood vessels contributes to raising the blood pressure, which is further enhanced by its central stimulant effects. Acting in the brain, cocaine induces an increase in heart rate and blood pressure and a redirection of blood flow from the skin and organs to the muscles.39 This redirection of blood flow may account for the feelings of power associated with cocaine use.
PHARMACOLOGICAL EFFECTS OF COCAINE
Local anesthesia
Vasoconstriction
Increase in blood pressure
Increase in heart rate
Bronchodilation
Increase in body temperature
Dilation of the pupils
Euphoria
Cocaine’s central effects are attributable to the blockage of the reuptake of dopamine, norepinephrine, and serotonin at presynaptic neuron terminals, which increases the concentration of these neurotransmitters in the synapse and causes a higher level of signaling at the postsynaptic neurons. The neurons most strongly influenced by cocaine are those of the pons and midbrain, which send projections through many parts of the brain.40 The increase in heart rate, blood pressure, and bronchial dilation can be attributed in part to the psychostimulatory effect of norepinephrine signaling, and the elevation of mood to the serotonin system. Cocaine’s attraction as a compound of abuse stems from the increased level of dopamine signaling it initiates, particularly in the limbic system—the reward center of the brain. The euphoria and strength of reward felt during cocaine use is nearly unrivaled among drugs of abuse.
The effects of cocaine on the body depend largely on the dose and route of administration. Coqueros receive a dose of approximately 20 to 50 milligrams per session, with a slow absorption noticeable within about ten minutes. Cocaine hydrochloride (“snow” or “crystal”) provides a typical dose of about 100 to 200 milligrams per session when placed on the gums (felt within ten to thirty minutes) or insufflated (snorted) into the nose in lines of about 50 milligrams or less each (felt within two to three minutes). When rubbed in the mouth or snorted, cocaine restricts its own uptake to some extent by constricting blood vessels and leaving cocaine on the surface to be absorbed more slowly. Intravenously injected cocaine hydrochloride gives a powerful dose of 25 to 200 milligrams or more (felt within one minute). By far the quickest route of administration is smoking the cocaine free base (crack), which typically provides a dose of 250 milligrams or more in a readily absorbed form (felt as an intense euphoria within ten seconds).41
At low doses of 25 to 75 milligrams among low-frequency users, cocaine increases alertness, motor hyperactivity, heart rate, blood pressure, and dilation of air passages. It also dilates the pupils and activates the stress responses, elevating blood glucose levels, increasing blood flow to the muscles, and raising body temperature. Psychologically, it produces a rapid sense of euphoria, overexcitement, and enhanced self-consciousness. The cocaine high later gives rise to a sense of anxiety that lasts hours, delayed sleep turning to fatigue, and a desire for more cocaine.
At higher doses, cocaine intensifies these physiological responses but carries with it more severe rebound depression and anxiety. At the highest doses during long-term exposure, it produces around-the-clock anxiety, sleeplessness, suspiciousness, and an altered sense of reality called toxic paranoid psychosis. Cocaine use also physically damages the body. Snorted cocaine initially constricts blood vessels in the nose but leads to a bloody and stuffy nose as the effect wears off. When taken orally or nasally, cocaine constricts blood vessels and numbs the tissue. Sensitive tissues die when their blood supply is cut off for too long, and injuries are more likely to go unnoticed in numb tissue.42 Cocaine use can cause a wide range of secondary effects, including heart attack and cardiac arrhythmias, renal deficiencies, and hemorrhage.43
As a traditional medicinal herb in the Andes, coca served as a practical stimulant for long and high mountain climbs. It evolved into a commodity of royal tribute among the Inca and became a form of currency under Spanish rule. To this day, indigenous people in South America consider coca a living connection to their ancient heritage. Following the isolation of its active principle, cocaine, European physicians promoted it as a treatment for conditions as diverse as low libido and indigestion. Among its numerous medicinal effects, cocaine’s utility as a local anesthetic allowed previously impossible delicate surgeries. Cocaine and the local anesthetics it inspired remain important pharmaceuticals in the operating room and dentist’s office. Meanwhile, cocaine’s potent psychoactive properties have led countless peoples’ lives toward addiction, and in the wake of illicit cocaine’s advance, society has struggled to confront its numerous legal, economic, and health-related consequences.