Contributed by Peter Chin-Hong, MD
CHAPTER CONTENTS
Introduction
Esophagitis
Gastritis
Diarrhea (Gastroenteritis, Enterocolitis)
Appendicitis
Diverticulitis
Enteric Fever Such as Typhoid Fever
INTRODUCTION
Infections with a variety of agents can occur in any part of the gastrointestinal (GI) tract from the mouth to the anal canal. Infections can range in severity from self-limited to life-threatening, particularly if infection spreads from the gut to other parts of the body. Infections are typically caused by the ingestion of exogenous pathogens in sufficient quantities to evade host defenses and then cause disease by multiplication, toxin production, or invasion through the gastrointestinal mucosa to reach the bloodstream and other tissues. In other cases, members of the normal flora of the GI tract can cause disease.
ESOPHAGITIS
Definition
Esophagitis is an inflammatory process that can damage the esophagus.
Pathophysiology
Inflammation caused by infection, typically by fungi such as Candida or viruses such as herpes simplex virus, causes the symptoms of esophagitis. Most cases occur in immunocompromised patients, especially those with reduced cell-mediated immunity. The extent of damage to the esophagus is typically related to the severity of symptoms.
Clinical Manifestations
Odynophagia (pain on swallowing) and dysphagia (difficulty in swallowing) are the key clinical manifestations of esophagitis.
Pathogens
Candida is the most common etiology, particularly among human immunodeficiency virus (HIV)-infected patients and other immunocompromised hosts (Figure 73–1). Less common pathogens include herpesviruses such as cytomegalovirus and herpes simplex virus. Noninfectious causes also occur, such as acid reflux from the stomach and medication-induced disease (e.g., doxycycline).
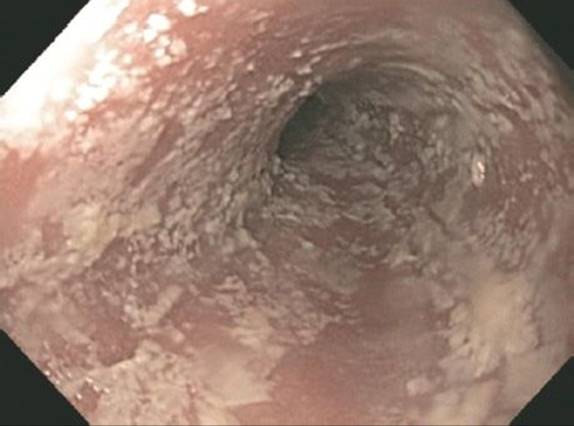
FIGURE 73–1 Candida esophagitis. Note the many whitish lesions on the esophageal mucosa seen on endoscopy. (Reproduced with permission from McKean SC et al. Principles and Practice of Hospital Medicine. New York: McGraw-Hill, 2012. Copyright © 2012 by The McGraw-Hill Companies, Inc.)
Diagnosis
Diagnosis may be empiric after a trial of fluconazole results in improvement for presumed Candida esophagitis. If an empiric course of fluconazole does not work, then endoscopy for visualization and biopsy could be helpful, particularly in immunocompromised hosts. Biopsy samples should be analyzed by using pathologic and microbiologic tests.
Treatment
In a typical patient (e.g., HIV-infected patient) presenting with odynophagia and retrosternal pain, an empiric diagnosis of esophageal candidiasis is made and fluconazole therapy instituted. If there is no effect on symptoms and if Candida resistance is not suspected, then further diagnostics as outlined earlier may identify a specific organism that could be targeted for treatment.
Prevention
One option to prevent recurrent esophageal candidiasis is by using fluconazole prophylaxis. However, this is not generally advised given the high risk of selecting for fluconazole-resistant Candida. Immune restoration in HIV-infected patients may decrease the incidence of esophageal and oropharyngeal candidiasis.
GASTRITIS
Definition
Gastritis refers to inflammation of the mucosa of the stomach. It may be erosive or nonerosive, depending on histologic and endoscopic findings. A break in the gastric and adjacent duodenal mucosa defines peptic ulcer disease.
Pathophysiology
The mechanism by which one of the main pathogens, Helicobacter pylori causes peptic ulcer disease has been largely elucidated. Following attachment to the gastric mucosa, H. pylori causes direct mucosal damage by the combination of ammonia production (from the action of the organism’s urease on urea) and the host inflammatory response. The ability of the organism to survive is enhanced by the neutralization of the stomach’s acid by the ammonia produced.
Clinical Manifestations
Patients with gastritis typically complain of dyspepsia (epigastric pain, burning), nausea, and vomiting. In the case of peptic ulcer disease, epigastric pain is the primary symptom. Some patients may report alleviation of pain with food, particularly those with duodenal ulcers. Gastrointestinal bleeding is a complication of peptic ulcer disease. Some patients with gastritis may be asymptomatic.
Pathogens
Infectious and noninfectious etiologies are possible. Among infectious causes, H. pylori is the most important. Viruses such as cytomegalovirus and fungi such as Mucor may rarely cause ulcer disease as well, particularly among immuncompromised patients. Following ingestion of raw fish, larvae of Anisakis species may become embedded in the gastric mucosa and cause severe abdominal pain. Mycobacteria (tuberculosis and nontuberculosis mycobacteria), Giardia, and Strongyloides may also cause gastritis. Noninfectious causes such as alcohol and medications (e.g., nonsteroidal anti-inflammatory drugs) are also implicated.
Diagnosis
Upper endoscopy with gastric biopsy is the definitive diagnostic strategy. If abnormal findings are detected, pathologic analysis and further directed testing may be performed. For the most common infectious cause of peptic ulcer disease, H. pylori–associated ulcers can be confirmed using a urease test on the biopsy specimen or using noninvasive tests such as the urea breath test or stool antigen test.
Treatment
Treatment is directed at the underlying pathogen, taking the host immune status into consideration. For H. pylori, combination therapy with two antibiotics, such as ampicillin and clarithromycin, plus a proton pump inhibitor, such as omeprazole, or bismuth is used with varying success.
DIARRHEA (GASTROENTERITIS, ENTEROCOLITIS)
Definition
It is useful to think of diarrhea as acute (lasting <2 weeks) or chronic (persisting >4 weeks). We will focus on acute diarrhea in this chapter because most of the etiologies are infectious in nature. We can further categorize acute diarrhea as noninflammatory (watery, nonbloody) or inflammatory (bloody). Bloody diarrhea is also known as dysentery. For example, bloody diarrhea caused by Shigella is often called bacillary dysentery. Table 73–1 describes the important features of watery and bloody diarrhea. Table 73–2 lists the important organisms that cause either watery or bloody diarrhea.
TABLE 73–1 Characteristics of Watery Diarrhea Compared to Bloody Diarrhea
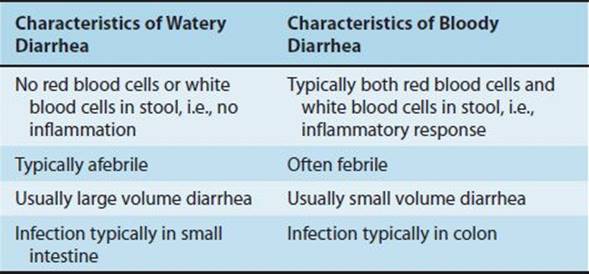
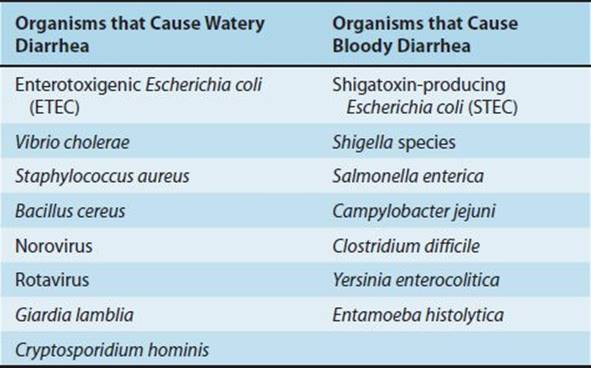
TABLE 73–2 Important Organisms that Typically Cause Either Watery or Bloody Diarrhea
Diarrhea must be calibrated against the patient’s normal bowel movements but is usually considered to be greater than three to five bowel movements per day. Most of the infectious agents that cause diarrhea act at the small intestine (where the majority of fluid normally gets absorbed) or the colon.
Pathophysiology
Pathogens or their associated toxins disrupt the normal absorption and secretory processes in the small intestines. Acute diarrhea is usually caused by preformed exotoxins in food or by the infectious agents in the intestinal tract (via either enterotoxin and cytotoxin production or mucosal invasion). Pathogens that produce preformed exotoxins include Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens. Other pathogens that cause noninflammatory acute diarrhea by enterotoxin production include enterotoxigenic Escherichia coli (ETEC) and Vibrio cholerae. Chapter 7 describes the mechanism of action of these toxins.
Pathogens that cause acute inflammatory diarrhea include Salmonella, Shigella, Campylobacter (via mucosal invasion), Shiga toxin–producing E. coli (STEC) such as E. coli O157:H7, and Clostridium difficile (via cytotoxin production). Antibiotic use predisposes to pseudomembranous colitis caused by C. difficile. Chapter 18 provides additional information on these enteric gram-negative rods, and Chapter 17 discusses C. difficile.
Clinical Manifestations
Table 73–3 describes the clinical presentation caused by important GI tract pathogens. Patients complain of diarrhea accompanied by urgency, abdominal bloating, and cramping. In the case of acute inflammatory diarrhea, there is also blood or pus seen in the stool, and patients can be febrile. If vomiting is a major feature of the clinical presentation, this suggests S. aureus food poisoning or viral gastroenteritis. If symptoms begin within 6 hours after ingestion of suspected contaminated food, then preformed toxin of S. aureus or B. cereus should be suspected. On physical examination, patients may also show signs of dehydration with tachycardia and orthostatic changes in blood pressure.
TABLE 73–3 Clinical Presentation, Diagnosis, and Treatment of Diarrhea Caused by Important Gastrointestinal Tract Pathogens

Children infected with STEC often have bloody diarrhea and may progress to hemolytic–uremic syndrome (HUS). HUS occurs when Shiga toxin produced by STEC enters the blood stream. The symptoms of HUS include hemolytic anemia, thrombocytopenia, and renal failure. Distorted red blood cells called schistocytes can be seen in blood smears. The use of ciprofloxacin increases the risk of HUS. Ingestion of undercooked hamburger or contaminated produce or contact with animals at petting zoos predisposes to disease caused by STEC.
Pathogens
Most cases of mild, acute diarrhea of short duration are caused by viruses. These include norovirus, rotavirus, and less commonly, adenovirus and astrovirus. ETEC is another important cause.
Most cases of severe diarrhea, however, are caused by bacteria. Pathogens such as Salmonella, Shigella, Campylobacter, STEC, and C. difficile are implicated in this category. Diarrhea caused by these bacteria is typically bloody.
Protozoa, such as Giardia, Entamoeba histolytica, Cryptosporidium, and microsporidia, are less common causes of diarrhea but are suspected in certain scenarios (e.g., in returning travelers or immunocompromised patients). Of these protozoa, Giardia is the most common cause of diarrhea in the United States. Giardiasis typically occurs in young children in day care, in men who have sex with men, and in hikers who drink untreated ambient water. In HIV-infected patients with very low CD4 counts, Cryptosporidium causes prolonged diarrhea and may cause extraintestinal disease involving the biliary and respiratory tracts.
Diagnosis
Diagnosis is generally focused on deciding who and when to test (i.e., determining when a test result may potentially impact the outcome). Because many causes of acute diarrhea are self-limited, this is an important issue. In general, we seek a diagnosis in cases of severe watery diarrhea, in cases of bloody diarrhea, if the patient is febrile, or if the patient is elderly or immunocompromised. Routine stool cultures will identify Salmonella, Shigella, and Campylobacter. If diarrhea is bloody, a special culture would need to be specifically set up to rule out STEC. The basis for the special culture is that STEC strains typically do not ferment sorbitol. The definitive laboratory diagnosis of an STEC strain is made by either polymerase chain reaction (PCR) test or immunoassay for the Shiga toxin.
Also, if bloody diarrhea is associated with antibiotic use, laboratory tests for the presence of the C. difficile toxin in the stool should be done. Colonoscopy may reveal the characteristic yellowish plaques seen in pseudomembranous colitis (Figure 73–2).
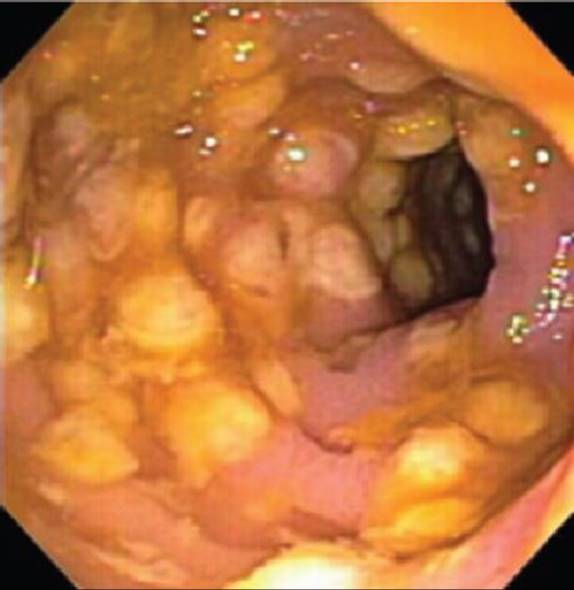
FIGURE 73–2 Pseudomembranous colitis caused by Clostridium difficile. Note yellowish pseudomembranes seen on colonoscopy. (Reproduced with permission from Longo DL et al [eds]: Harrison’s Principles of Internal Medicine, 18th ed. New York: McGraw-Hill, 2012. Copyright © 2012 by The McGraw-Hill Companies, Inc.)
Sending stool samples for analysis of ova and parasites (O&P) is generally not cost effective, except in immunocompromised patients, patients with a history of recent foreign travel, or when diarrhea is associated with community waterborne outbreaks. Stools for O&P are usually sent on 3 consecutive days given that some parasites only intermittently shed eggs or cysts in the stool.
Treatment
The most important treatment modality in diarrhea is hydration. Oral rehydration solution containing water, salt, and sugar has been life-saving in many parts of the world. In general, for most cases of community-acquired diarrhea, empiric treatment with antimicrobials is not beneficial. The drug of choice for mild or moderate colitis caused by C. difficile is metronidazole. Severe infections should be treated with oral vancomycin.
Prevention
Most of the preventative strategies are directed at travelers to developing countries. They are advised to avoid potentially contaminated water sources as well as fresh fruit and vegetables if not washed in boiled water. One current approach is to provide the traveler with a supply of antimicrobials, such as ciprofloxacin, to be taken in the event of a diarrheal episode.
APPENDICITIS
Definition
Appendicitis is inflammation of the vestigial vermiform appendix. It is one of the most common causes of acute abdomen requiring surgical exploration.
Pathophysiology
Obstruction of the appendix by one of a variety of causes (e.g., fecaliths, infection such as parasites, tumor) leads to an increase in luminal and intramural pressure. Bacterial overgrowth is accompanied by inflammation. If there is necrosis, perforation followed by diffuse peritonitis caused by bacteria of the normal colonic flora (e.g., E. coli and Bacteroides) may occur.
Clinical Manifestations
Clinical manifestations include abdominal (especially periumbilical migrating to right lower quadrant) pain, anorexia, nausea, and vomiting. Initial symptoms may be missed because they may be nonspecific (e.g., indigestion). A standard abdominal computed tomography (CT) scan with contrast is often used when appendicitis is suspected.
Pathogens
Early in the course of the disease, the predominant organisms are anaerobic. In late disease, mixed organisms predominate. E. coli, Peptostreptococcus, Bacteroides fragilis, and Pseudomonas are commonly isolated. Yersinia, Campylobacter, and Salmonella can cause an acute ileitis and mesenteric adenitis that can mimic appendicitis.
Diagnosis
Clinical manifestations combined with imaging are typically used to make a decision as to whether a patient should be taken to the operating room.
Treatment
Surgery is the definitive treatment for appendicitis, usually in concert with perioperative antibiotics. A course of antibiotics alone (without surgery) is sometimes used, but there is an increased risk of recurrent appendicitis.
DIVERTICULITIS
Definition
Diverticulitis is inflammation of a sac-like protrusion of the colonic wall, usually in the sigmoid colon (Figure 73–3). Perforation of the diverticulum with consequent abscess formation or peritonitis may occur.
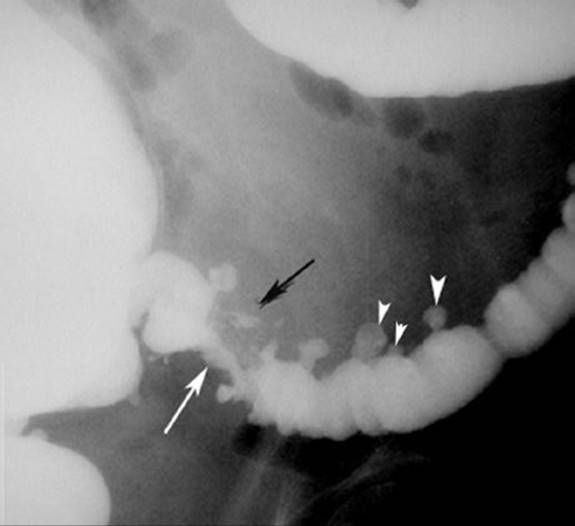
FIGURE 73–3 Diverticulitis. Several diverticula can be seen (white arrowheads). The white arrow indicates a narrow lumen that is the result of spasm caused by the inflammation resulting from a perforated diverticulum and the resulting abscess (black arrow). (Courtesy of the Surgery Department at the Loyola University of Chicago School of Medicine.)
Pathophysiology
Colonic diverticula may occur following years of a diet deficient in fiber.
Clinical Manifestations
There is a range of symptoms depending on the degree of perforation. Patients usually present with dull, aching, left lower quadrant abdominal pain. This is often accompanied by a low-grade fever, leukocytosis, nausea, and vomiting. Diarrhea or constipation may be present. If perforation occurs, patients can present with generalized peritoneal signs with diffuse abdominal pain and shock.
Pathogens
Bowel flora such as anaerobes, i.e., B fragilis, and those in the Enterobacteriaceae family, such as E. coli, are typically involved.
Diagnosis
Abdominal CT will show colonic diverticula and associated wall thickening, fat infiltration, abscesses, and extraluminal air or contrast medium.
Treatment
Oral antibiotics with excellent anaerobic activity (e.g., amoxicillin with clavulanate or a combination of ciprofloxacin plus metronidazole) are used in mild cases. In more serious cases requiring hospitalization, intravenous fluids and antibiotics are given with bowel rest as needed. If there is an associated abdominal abscess or signs of peritonitis, surgical evaluation must be undertaken.
Prevention
Prevention involves increasing the amount of fiber in diet.
ENTERIC FEVER SUCH AS TYPHOID FEVER
Definition
Enteric fever is a clinical syndrome comprised of constitutional symptoms, such as fever and headache, and nausea, vomiting, and abdominal pain. Although enteric fever can be caused by several Salmonella species, “typhoid fever” refers to enteric fever caused by the Salmonella typhi. S. typhi is also known as Salmonella enterica serotype Typhi. Typhoid fever is a significant global health problem.
Pathophysiology
Following the consumption of contaminated food, Salmonella bacteria enter through the intestinal mucosal epithelium by transcytosis. The microbes then replicate in the macrophages of Peyer patches, mesenteric lymph nodes, and the spleen. Bacteremia then occurs with dissemination to lungs, gallbladder, kidneys, or central nervous system.
Humans are the only reservoir for S. typhi, so contamination of food or water by human feces should be suspected.
Clinical Manifestations
A prodromal phase is characterized by constitutional symptoms such as malaise, together with abdominal pain, constipation, and headache. Fever increases over the next several days. During the second week of disease, a typical transient rash of pink maculopapular lesions (rose spots) may be seen. Splenomegaly occurs more commonly than hepatomegaly, but both may occur. Relative bradycardia and leukopenia are often observed. Diarrhea is uncommon.
The chronic carrier state occurs in approximately 3% of patients with typhoid fever. The organisms typically reside in the gallbladder and are excreted in the stool, serving as a source of infection for others.
Pathogens
S. typhi and other Salmonella species, such as Salmonella paratyphi A and S. paratyphi B, cause typhoid fever.
Diagnosis
A history of travel to endemic areas, together with a compatible clinical presentation, is often used initially. Any fever in a returning traveler should prompt blood cultures and a clinical suspicion for enteric fever. Early in the disease, blood cultures are typically positive and stool cultures are often negative. Later in the disease and in the carrier state, stool cultures are positive and blood cultures are negative. Stool cultures are positive at this stage because bile from an infected gallbladder carries organisms into the stool.
Treatment
Oral or intravenous ciprofloxacin is often used. Intravenous ceftriaxone is another effective treatment modality. Ciprofloxacin for 4 weeks can also be used to eliminate the carrier state. Cholecystectomy should be considered for those chronic carriers who do not respond to antimicrobial therapy.
Prevention
Hygienic measures to protect the food and water supply from human fecal contamination are an important public health intervention. Immunization may not always be effective but can be considered in epidemic outbreaks, for travelers to endemic countries, and for household contacts of typhoid carriers.
Two vaccines against typhoid fever are available in the United States, both providing approximately 50% to 80% protection. The vaccine containing the Vi capsular polysaccharide of S. typhi has the advantage of being administered once, intramuscularly. The other vaccine contains live attenuated S. typhi organisms and is administered orally. It has the advantage of stimulating gut immunity thereby interrupting transmission.