Michael F. Murphy
Ron M Walls
Definition of the Difficult and Failed Airway
Although both difficult and failed airways are discussed in this chapter, the two concepts are distinct. A difficult airway is one for which a preintubation examination has identified attributes that are likely to make laryngoscopy, intubation, bag-mask ventilation (BMV), the use of an extraglottic device (EGD; e.g., Combitube, laryngeal mask airway [LMA]), or surgical airway management more difficult than would be the case in an ordinary patient without those attributes. Identification of a difficult airway is a key component of the approach to airway management for any patient and is a key branch point on the main airway algorithm (see Chapter 2). The key reason for this is that, in general, one should not administer a neuromuscular blocking medication to a patient unless one has a measure of certainty that gas exchange can be maintained if laryngoscopy and intubation fail.
If a difficult airway is identified, the difficult airway algorithm is used, and the approach to management is different from that taken when the patient is not anticipated to have a difficult intubation (see Chapter 2).
A failed airway situation occurs when a provider has embarked on a certain course of airway management (e.g., rapid sequence intubation [RSI]) and has identified that intubation by that method is simply not going to succeed, requiring the immediate initiation of a rescue sequence (the failed airway algorithm, see Chapter 2). Certainly, in retrospect, a failed airway can be called a difficult airway because it has proven to be impossible to intubate, but the terms “failed airway” and “difficult airway” must be kept distinct because they represent different situations, require different approaches, and arise at different points in the airway management sequence. Furthermore, it is crucial that the airway manager recognize when a difficult airway has transitioned to a failed airway and use the correct management algorithm.
“The difficult airway is something one anticipates; the failed airway is something one experiences.”
Airways that are difficult to manage are fairly common in emergency practice, with some estimates being as high as 20% of all emergency intubations. However, the incidence of intubation failure is quite low, generally less than 1% for medical intubations and less than 3% for trauma intubations. The true incidence of the disastrous “can't intubate, can't oxygenate” (CICO) situation is unknown in emergency intubations, but is estimated to represent between 1 in 5,000 and 1 in 20,000 operating room intubations.
This chapter explores the concepts of the failed and the difficult airway in the setting of emergency intubation. Recognizing the difficult airway in advance and executing an appropriate and thoughtful plan, guided by the difficult airway algorithm (see Chapter 2) will minimize the likelihood that airway management will fail. Furthermore, recognizing the failed airway promptly will optimize the chances that the failing technique will be abandoned and the failed airway algorithm will guide an approach that is reasonably anticipated to succeed.
The Failed Airway
A failed airway exists when either of the following conditions is met:
1. Failure to maintain acceptable oxygen saturations during or after one or more failed laryngoscopic attempts (CICO) or
2. Three failed attempts at orotracheal intubation by an experienced intubator, even when oxygen saturation can be maintained.
Clinically, the failed airway presents itself in two ways, depending on the urgency created by the situation:
1. There is not sufficient time to evaluate or attempt a series of rescue options, and the airway must be secured immediately because of an inability to maintain oxygen saturation by BMV. This is the CICO scenario (defined by the previous number 1).
2. There is time to evaluate and execute various options because the patient is in a “can't intubate, can oxygenate” situation (defined by the previous number 2).
The most important way to avoid airway management failure is to identify in advance those patients for whom difficulty can be anticipated with intubation, BMV, insertion of an EGD or cricothyrotomy.
The adage in anesthesia with respect to neuromuscular blockade and the orotracheal intubation of a patient who has some effective spontaneous ventilation has always been “Don't take anything away from the patient that you cannot replace,” which can be truncated to “Don't burn any bridges.” Although such advice is certainly sound in terms of elective anesthesia, this rigid principle is not always consistent with the realities of emergency airway management, where intubation is often required emergently regardless of the patient's underlying physiological condition or difficult airway attributes, and the approach must be chosen that is most likely to result in success. In fact, many patients with identified difficult airways are best managed using RSI, but the approach is customized and guided by the principles of the difficult airway algorithm (see Chapter 2).
The Difficult Airway
The emergency airway algorithms were introduced in Chapter 2. When one is presented with a patient who requires intubation, the first decision is whether this is a crash airway. If it is not a crash airway, one must ask, “Is this a difficult airway?” Asking the question presumes that one has a framework with which to answer it.
In clinical practice, the difficult airway has five dimensions:
1. Difficult BMV
2. Difficult laryngoscopy
3. Difficult intubation
4. Difficult EGD
5. Difficult cricothyrotomy
These five dimensions can be reduced to four technical operations:
1. Difficult BMV
2. Difficult laryngoscopy and intubation
3. Difficult EGD
4. Difficult cricothyrotomy
One might think of these four operations as the four corners of a box, the difficult airway box (Fig. 7.1). According to the main emergency airway management algorithm, RSI is the method of choice for airway management in the event airway management difficulty is not anticipated. This requires a reliable and reproducible method for identifying the difficult airway. This evaluation must be expeditious, easy to remember, and complete. A distinct evaluation is required for difficult BMV, difficult laryngoscopy/intubation, difficult EGD, and difficult surgical airway management, and each evaluation must be applied to each patient before airway management is undertaken.
|
|
|
Figure 7-1 • Difficult Airway Box. Note that the four corners represent the four dimensions of difficulty. |
Difficult Bag-Mask Ventilation: MOANS
Chapter 5 highlights the importance of BMV in airway management, particularly as a rescue maneuver when orotracheal intubation has failed. If the airway manager is uncertain that neuromuscular blockade–facilitated orotracheal intubation (RSI) will be successful, he or she must be confident that BMV is possible, gas exchange through an EGD is possible, or, at the very least, a cricothyrotomy can rapidly be performed.
The validated indicators of difficult BMV can be easily recalled for rapid use in the emergency setting by using the mnemonic MOANS. Perhaps one can recall this mnemonic by picturing the obtunded, moaning patient as in need of BMV, or conversely, the involuntary moans that might escape the lips of the provider when he or she is confronted by a patient on whom BMV is not possible.
|
M |
Mask seal: Bushy beards, crusted blood on the face, or a disruption of lower facial continuity are the most common examples of conditions that may make an adequate mask seal difficult. Some experts recommend smearing a substance, such as KY jelly, on the beard as a remedy to this problem, although this action may simply make a bad situation worse in that the entire face may become too slippery to hold the mask in place. |
|
O |
Obesity/obstruction: Patients who are obese (body mass index >26 kg/m2) are often difficult to ventilate adequately by bag and mask. Women in third-trimester gestation are also a prototype for this problem because of their increased body mass and the resistance to diaphragmatic excursion by the gravid uterus create elevated resistance to BMV. Pregnant or obese patients also desaturate more quickly, making the bag ventilation difficulty of even greater import (see Chapters 32 and 35). The difficulty bagging the obese patient is not caused solely by the weight of the chest and abdominal walls and the resistance by the abdominal contents to diaphragmatic excursion. Obese patients also have redundant tissues, creating resistance to airflow in the supraglottic airway. Similarly, patients with obstruction caused by angioedema, Ludwig's angina, upper airway abscesses (e.g., peritonsillar), epiglottitis, and others ought to be considered at this juncture. In general, edematous lesions (e.g., angioedema, croup, epiglottitis) are more amenable to bag and mask rescue if sudden obstruction occurs but not reliably so. Similarly, laryngospasm can usually be overcome with good bag and mask technique. In contrast, firm, immobile lesions such as hematomas, cancers, and foreign bodies are less amenable to rescue by BMV, which is unlikely to provide adequate ventilation or oxygenation if total obstruction arises in this context. |
|
A |
Age: Age older than 55 years is associated with a higher risk of difficult BMV, perhaps because of a loss of muscle and tissue tone in the upper airway. The age of 55 is not a precise cutoff, and some judgment can be applied with respect to whether the patient has relatively elastic (young) or inelastic (aged) tissue. |
|
N |
No teeth: An adequate mask seal may be difficult in the edentulous patient because the face tends to cave in. An option is to leave dentures (if available) in situ for BMV and remove them for intubation. Alternatively, gauze dressings may be inserted into the cheek areas via the mouth to puff them out in an attempt to improve the seal. |
|
S |
Stiff: This refers to patients whose lungs are themselves resistant to ventilation and require high ventilation pressures. These patients are primarily those with reactive airways disease with medium and small airways obstruction (asthma, chronic obstructive pulmonary disease) and those with pulmonary edema, acute respiratory distress syndrome, advanced pneumonia, or any other condition that reduces pulmonary compliance or increases airway resistance to BMV. A separate but unrelated S that connotes difficult BMV is a history of sleep apnea or snoring. This condition may not be detectable in the setting of an emergency intubation. |
Difficult Laryngoscopy and Intubation: LEMON
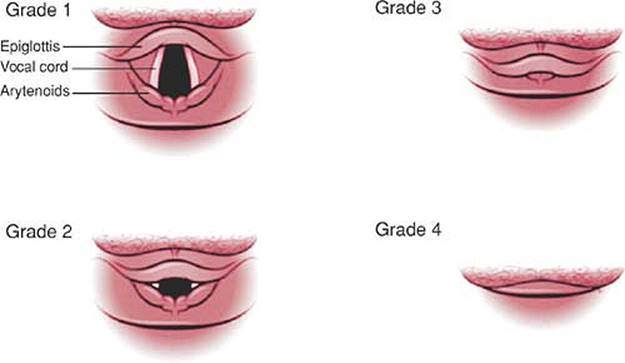
The concept of difficult laryngoscopy and intubation is inextricably linked to poor glottic view. Cormack and Lehane introduced the most widely used system of categorizing the degree of visualization of the larynx during laryngoscopy, in which an ideal laryngoscopic view is designated grade 1 and the worst possible view grade 4 (Fig. 7.2). Cormack-Lehane (C-L) view grades 3 (epiglottis only visible) and 4 (no glottic structures at all visible) are highly correlated with difficult or failed intubation. C-L grades 1 (visualization of the entire glottic aperture) and 2 (visualization of at least some portion of the cords or the arytenoids) are not typically associated with difficult intubation, although a patient with a grade 2 view in which only the arytenoids are visible is significantly more difficult to intubate than a patient with a grade 2 view in which any portion of the cords can be seen. Patients with a limited grade 2 view or a grade 3 view may greatly benefit by use of an endotracheal tube introducer such as the Eschmann introducer (EI), also known as the Eschmann stylet (or gum elastic bougie), or the Frova intubating stylet (see Chapter 6). The C-L grading system does not differentiate precisely the degree to which the laryngeal aperture is visible during laryngoscopy: a grade 2 view may reveal little of the vocal cords, or none at all if only the arytenoids are visible. This has led some authors to propose a 2a/2b system, wherein a 2a shows any portion of the cords and a 2b shows only the arytenoids. Grade 2b accounts for only about 20% of grade 2 views. However, when a grade 2b view occurs, two thirds of patients are difficult to intubate, whereas only about 4% of patients with grade 2a views are characterized as difficult intubations. A grade 1 view reveals the entire glottis and is associated with almost universal intubation success.
|
|
|
Figure 7-2 • Cormack-Lehane laryngeal view grade system. |
The question is often asked: how much of the cords must be visible during direct laryngoscopy to ensure intubation success? How much is enough? Although our discussion here focuses on direct laryngoscopy, many of the issues also apply, to some degree, to video laryngoscopy. The precise extent to which large-scale adoption of video laryngoscopy and other newer methods of intubation will transform our notions of difficult intubation is not known, but it is likely that a radical transformation will occur as direct laryngoscopy is gradually replaced by superior modern methods of intubation. In the context of emergency laryngoscopy, whether direct or by another method, one must first define best attempt. Updating concepts defined by Benumof, we might define the seven components of the best attempt as (a) performance by an adequately trained and experienced endoscopist, (b) adequate patient relaxation, (c) best possible positioning of the patient, (d) the use of external laryngeal manipulation (Backward, Upward, Rightward Pressure, or BURP), (e) length of the blade, (f) type of blade, and (g) type of laryngoscope. With this definition and no other confounding considerations, the optimal attempt at laryngoscopy may be achieved on the first attempt and should take no more than three attempts. Often, the circumstances of an emergency intubation preclude the first attempt being the best attempt. When an attempt at orotracheal intubation is unsuccessful and an additional attempt is contemplated, the operator should consider which of the seven attributes can be changed or improved on the subsequent attempt to enhance the chances of success.
Optimizing all seven components may not be possible in an emergency. For example, in the event the cervical spine is immobilized, it is not possible to place the patient in the sniffing position. Positioning the head and neck is an important step in optimizing conventional laryngoscopy as a prelude to orotracheal intubation. Although there is some debate about the relative role of simple head extension versus the sniffing position (head extension with neck flexion, see Chapter 6), in any case, optimal positioning of the patient for direct laryngoscopy improves laryngoscopic view. Patient positioning plays a much smaller role, if any, during video laryngoscopy.
Many researchers have attempted to determine with precision which patient attributes predict successful laryngoscopy and intubation and which predict failure. None have been able to do so. Lists of anatomical features, radiologic findings, and complex scoring systems have all been explored without success. In the absence of a proven and validated system that is capable of predicting intubation difficulty with 100% sensitivity and specificity, it is important to develop an approach that will enable a clinician to quickly and simply identify those patients who might be difficult to intubate so an appropriate plan can be made using the difficult airway algorithm. In other words, sensitivity (i.e., identifying all those who might be difficult) is more important than specificity (i.e., always being correct when identifying a patient as difficult) when we ask the question, “Does this patient's airway warrant using the difficult airway algorithm, or is it appropriate and safe to proceed directly to RSI?”
The mnemonic LEMON is a useful guide to identify as many of the risks as possible as quickly as possible to meet the demands of an emergency situation. The elements of the mnemonic are assembled from an analysis of the difficult airway prediction instruments in the elective anesthesia literature and are the subject of a validation study (NEAR III) by the investigators of the multicenter National Emergency Airway Registry project. The LEMON mnemonic is recalled by the popular idiom that a defective product is a “lemon”; thus, the difficult airway is a LEMON:
|
L |
Look externally: Although a gestalt of difficult intubation is not particularly sensitive (meaning that many difficult airways are not readily apparent externally), it is quite specific, meaning that if the airway looks difficult, it probably is. Most of the litany of physical features associated with difficult laryngoscopy and intubation (e.g., small mandible, large tongue, large teeth, short neck) are accounted for by the remaining elements of LEMON and so do not need to be specifically recalled or sought, which can be a difficult memory challenge in a critical situation. The external look specified here is for the “feeling” that the airway will be difficult. This feeling may be driven by a specific finding, such as external evidence of lower facial disruption and bleeding that might make intubation difficult, or it might be the ill-defined composite impression of the patient, such as the obese, agitated patient with a short neck and small mouth, whose airway appears formidable even before any formal evaluation (the rest of the LEMON attributes) is undertaken. |
|
E |
Evaluate the 3-3-2 rule: This step is an amalgamation of the much-studied geometric considerations that relate mouth opening and the size of the mandible to the position of the larynx in the neck in terms of likelihood of successful visualization of the glottis by direct laryngoscopy. This relationship was first articulated by Patil in 1983, when he associated a thyromental distance of less than 6 cm with difficult intubation. The thyromental distance is the hypotenuse of a triangle, the axis being the anteroposterior length of the mandibular space, and the abscissa being the distance between the chin-neck junction (roughly the position of the hyoid bone indicating the posterior limit of the tongue) and the top of the larynx. The 3-3-2 rule accounts for the three geometric keys to successful visualization of the glottis by direct laryngoscopy: |
· The mouth must open adequately to permit visualization past the tongue when both the laryngoscope blade and the endotracheal tube are within the oral cavity.
· The mandible must be of sufficient size (length) to allow the tongue to be displaced fully into the submandibular space.
· The glottis must be located a sufficient distance caudad to the base of the tongue that a direct line of sight can be created from outside the mouth to the vocal cords as the tongue is displaced inferiorly into the submandibular space.
The first “3,” therefore, assesses mouth opening. A normal patient can open his or her mouth sufficiently to accommodate three of his or her own fingers between the upper and lower incisors. The second “3” evaluates the length of the mandibular space by ensuring the patient's ability to accommodate three of his or her own fingers between the tip of the mentum and chin-neck junction (hyoid bone) (Fig. 7.3A). The “2” assesses the position of the glottis in relation to the base of the tongue. The space between the chin-neck junction (hyoid bone) and the thyroid notch should accommodate two of the patient's fingers (Fig. 7.3B). Thus, in the 3-3-2 rule, the first 3 assesses the adequacy of oral access, and the second 3 addresses the dimensions of the mandibular space to accommodate the tongue on laryngoscopy. The ability to accommodate significantly more than or less than three fingers is associated with greater degrees of difficulty in visualizing the larynx at laryngoscopy: the former because the length of the oral axis is elongated; and the latter because the mandibular space may be too small to accommodate the tongue, requiring it to remain in the oral cavity or move posterior, obscuring the view of the glottis. Encroachment on the submandibular space by infiltrative conditions (e.g., Ludwig's angina) is identified during this evaluation. The final 2 identifies the location of the larynx in relation to the base of the tongue. If significantly more than two fingers are accommodated, meaning the larynx is distant from the base of the tongue, it may be difficult to visualize the glottis on laryngoscopy. Fewer than two fingers may mean that the larynx is tucked up under the base of the tongue and may be difficult to expose. This condition is often inaccurately called “anterior larynx.”
|
|
|
|
Figure 7-3 • A: The second 3 of the 3-3-2 rule. B: The 2 of the 3-3-2 rule. |
|
|
M |
Mallampati score: Mallampati determined that the degree to which the posterior oropharyngeal structures are visible when the mouth is fully open and the tongue is extruded reflects the relationships among mouth opening, the size of the tongue, and the size of the oral pharynx, which defines access via the oral cavity for intubation, and that these relationships are loosely associated with intubation difficulty. Mallampati's classic assessment required that patients sit on the side of the bed, open their mouths as widely as possible, and protrude their tongue as far as possible without phonating. Figure 7.4 depicts how the scale is constructed. Although Class I and II patients are associated with low intubation failure rates, the importance with respect to the judgment of whether to use neuromuscular blockade rests with those in Classes III and IV, particularly Class IV where intubation failure rates may exceed 10%. By itself, the scale is neither sensitive nor specific; however, if it can be performed in an emergency, it may reveal important information about access to the oral cavity and the potential for difficult glottic visualization. Usually in the emergency situation, it is not possible to have the patient sit up and follow instructions. Therefore, a crude Mallampati measure is often all that can be assessed, by looking into the supine, obtunded patient's mouth with a tongue blade and light, or by using a lighted laryngoscope blade as a tongue depressor to gain an appreciation of how much mouth opening is present (at least in the preparalyzed state) and how likely the tongue and oral pharynx are to conspire to prevent successful laryngoscopy. Although not validated in the supine position using this approach, there is no reason to expect that the assessment would be any less reliable than the original method with the patient sitting and performing the maneuver actively. |
|
O |
Obstruction/obesity: Upper airway obstruction should always be considered as a marker for a difficult airway. The four cardinal signs of upper airway obstruction are muffled voice (hot potato voice), difficulty swallowing secretions (because of either pain or obstruction), stridor, and a sensation of dyspnea. The first two signs do not ordinarily herald imminent total upper airway obstruction in adults, but critical obstruction is much more imminent when the sensation of dyspnea occurs. Stridor is a particularly ominous sign. The presence of stridor is generally considered to indicate that the circumference of the airway has been reduced to less than 50% of its normal calibre, or to a diameter of 4.5 mm or less. Upper airway obstruction should always be considered a difficult airway and managed with extreme care. The administration of even small doses of opioids and benzodiazepines, for sedation or to manage anxiety, may induce total obstruction as the stenting tone of the upper airway musculature relaxes, and upper airway instrumentation in the context of inflamed, irritated supraglottic tissues can induce laryngospasm. Either possibility argues for a “double setup” with cricothyrotomy backup during examination or planned awake intubation of a patient with upper airway obstruction. Chapter 30 deals with this topic in detail, particularly in relation to the management of the patient with upper airway obstruction, the selection of rescue interventions, and the timing of those interventions. Although it is controversial whether obesity per se is an independent marker for difficult laryngoscopy or whether obese patients simply have attributes that can be identified by detailed evaluation (e.g., Mallampati score, the 3-3-2 rule), obese patients frequently have poor glottic views by direct laryngoscopy, and obesity, in itself, should be considered to portend difficult laryngoscopy. Glottic view may be difficult whether a direct or video laryngoscope is used. |
|
N |
Neck mobility: The ability to position the head and neck is one of the seven factors necessary to the achievement of the optimal laryngoscopic view of the larynx. Cervical spine immobilization for trauma, by itself, may not create a degree of difficulty that ultimately leads one to avoid RSI after applying the thought processes of the difficult airway algorithm. However, cervical spine immobilization will make intubation more difficult and will compound the effects of other identified difficult airway markers. In addition, intrinsic cervical spine immobility, such as in cases of ankylosing spondylitis or rheumatoid arthritis, can make intubation by direct laryngoscopy extremely difficult or impossible and should be considered as a much more serious issue than the ubiquitous cervical collar (which mandates inline manual immobilization). Video laryngoscopy requires much less (or no) head extension, and may provide a superior glottic view when head extension or neck flexion is restricted. A recent study also showed reduced cervical spine movement during intubation using the Shikani optical stylet versus direct laryngoscopy. |
|
|
|
Figure 7-4 • The Mallampati Scale. In Class I, the oropharynx, tonsillar pillars and entire uvula are visible. In Class II, the pillars are not visible. In Class III, only a minimal portion of the oropharyngeal wall is visible and in Class IV the tongue is pressed against the hard palate. |
Difficult Extraglottic Device: RODS
Extraglottic airway devices have emerged as invaluable rescue airway management devices, in addition to their role in routine airway management in the operating room. Devices such as the intubating LMA (Fastrach) and the esophageal tracheal Combitube (Combitube) have a substantial volume of literature attesting to their utility as rescue devices in emergency medical services, emergency medicine, the critical care unit, and anesthesia.
Studies have identified factors that predict difficulty in placing an EGD and providing adequate gas exchange. These can be assessed using the mnemonic RODS.
|
R |
Restricted mouth opening: Depending on the EGD to be employed, more or less oral access may be needed. |
|
O |
Obstruction: Upper airway obstruction at the level of the larynx or below. An EGD will not bypass this obstruction. |
|
D |
Disrupted or distorted airway: At least in as much as the “seat and seal” of the EGD may be compromised. Seal may be exceedingly difficult or impossible to achieve in the face of a fixed flexion deformity of the neck, or with the upper airway distortion of angioedema, for example. |
|
S |
Stiff lungs or cervical spine: Ventilation with an EGD may be difficult or impossible in the face of substantial increases in airway resistance (e.g., deadly asthma) or decreases in pulmonary compliance (e.g., pulmonary edema). There are reports of difficult LMA insertion in patients with limited neck movement. |
Difficult Cricothyrotomy: SHORT
There are no absolute contraindications to performing an emergency cricothyrotomy (see Chapter 16). However, some conditions may make it difficult or impossible to perform the procedure, making it imperative to identify those conditions in advance and allowing consideration of alternatives rather than simply relying on a rapidly performed cricothyrotomy as a rescue technique. The mnemonic SHORT is used to quickly assess the patient for features that may indicate that a cricothyrotomy might be difficult. The mnemonic can be recalled by remembering that a patient with a short neck is difficult to perform a surgical airway on, or that time is short when cricothyrotomy is indicated. The SHORT mnemonic is applied as follows:
|
S |
Surgery (or other airway disruption): The anatomy may be subtly or obviously distorted, making the airway difficult to find or impeding access to the anterior portion of it (e.g., halo device after spine surgery). |
|
H |
Hematoma (includes infection/abscess): A hematoma (postoperative or traumatic) or an infective process in the pathway of the cricothyrotomy may make the procedure technically difficult, but should never be considered a contraindication in a life-threatening situation. |
|
O |
Obesity (includes any access problem): Obesity should be considered a surrogate for any problem that makes percutaneous or open surgical access to the anterior neck problematic, such as a very short neck; large, descending pannus; and subcutaneous emphysema. Careful palpation of the relevant landmarks (see Chapter 16) will identify these issues. |
|
R |
Radiation distortion (and other deformity): Past radiation therapy may distort and scar tissues making the procedure difficult, or fixed flexion deformity of the spine may limit the working access to the anterior landmarks. |
|
T |
Tumor: Tumor, either in or around the airway, may present difficulty, both from access and bleeding perspectives. |
Summary
· When intubation is indicated, the most important question is “Is this airway difficult?” Considerations of pharmacologic agents for RSI, for example, do not come into play until the patient has been thoroughly assessed for difficulty (MOANS, LEMON, RODS, and SHORT) and the appropriate issues addressed using the algorithms.
· MOANS is always crucially important. The ability to oxygenate a patient with a bag and mask turns a potential CICO situation requiring urgent cricothyrotomy into a “can't intubate, can oxygenate” situation, in which many rescue options can be considered. The ability to prospectively identify and avoid situations in which bag ventilation will be difficult or impossible is critical to avoiding unnecessary emergency cricothyrotomy.
· When cricothyrotomy is necessary, the possibility will have virtually always been identified in advance, and application of SHORT will permit the operator to be mentally and physically prepared for the surgical airway.
· No single indicator, combination of indicators, or even weighted scoring system of indicators can be relied on to guarantee success or predict inevitable failure for oral intubation. Application of a systematic method to identify the difficult airway and then analysis of the situation to identify the best approach, given the anticipated degree of difficulty and the skill, experience, and judgment of the individual performing the intubation, will lead to the best decisions regarding how to manage the particular clinical situation. In general, it is better to err by identifying an airway as potentially difficult, only to subsequently find this not to be the case, than the other way around.
Evidence
1. What is the incidence of difficult and failed airway? In anesthesia practice, the incidence of the failed airway has been identified as 1:2,230 (0.05%) in surgical patients (1) and in approximately 1:280 (0.36%) of parturients for cesarian section under general anesthesia (2). The largest single-center series in the emergency medicine literature has demonstrated a failure rate for RSI of approximately 1% (3). Emerging numbers from the multicenter NEAR project show cricothyrotomy rates of approximately 0.5% in medical cases and 2.3% in trauma (4).
2. How reliable are the factors we evaluate in predicting difficult intubation? Many studies have attempted not only to define the features that may predict difficulty, but also to precisely define those airways where failure will occur. The goal has been to attempt to precisely divide the population into those who can be safely anesthetized and paralyzed and those who ought to be intubated while awake. The landmark publication in 1956 by Cass et al. (5) identified those anatomical features that may predict difficult intubation. This work coincided with the introduction of paralytic agents into anesthetic practice in the late 1940s and early 1950s. Many subsequent investigators attempted to deliver tools that could accurately predict failure (6,7,8,9,10,11,12,13). Although all failed to craft a formula or identify a specific predictor for failure, Mallampati had a measure of success in that he identified oral access as a crucial feature of the assessment for difficulty (13). Langeron, in particular, contributed greatly to the scientific validation of those features, predicting difficult BMV with his study published in 2000 (14,15).
3. Is there any evidence that positioning the airway prior to intubation improves the view of the glottis? Cormack and Lehane (16) devised the most widely accepted system of categorizing the view of the larynx achieved with an orally placed laryngoscope. The sniffing position has been widely accepted as the optimum position for orotracheal intubation (17), although Adnet et al. (18) more recently challenged this dogma, suggesting that simple extension may be sufficient or possibly even superior. In attempting to provide a framework or an approach to answering the question of optimum positioning of the head and neck, Levitan et al. (19) devised a scoring system to quantify the percentage of glottic opening visible during a best laryngoscopy, although this scale has yet to gain widespread acceptance.
4. What is the evidence that stridor indicates a critically narrowed airway? Stridor is of particular significance in the setting of an acute airway problem, where progression of the pathophysiological process may precipitate total airway obstruction that cannot be rescued. Stridor is a characteristic sign in disorders such as croup. Its significance in this condition is attenuated by the fact that we know children with croup seldom progress in an unpredictable manner to total airway obstruction. Stridor is also seen in many chronic ear, nose, and throat disorders, but again is much less significant in this setting due to the nonprogressive or slowly progressive nature of the disorder. The presence of stridor in the setting of an acute upper airway disorder is generally considered to indicate that the circumference of the airway has been reduced to less than 50% of its normal calibre (20), or to a diameter of 4.5 mm or less (21).
5. Is there any evidence to support the use of RODS to predict difficulty in placing an extraglottic device? The first three letters are as much a matter of common sense as evidence. However, there is good evidence that ventilation with an EGD may be difficult or impossible in the face of substantial increases in airway resistance (e.g., deadly asthma) or decreases in pulmonary compliance (e.g., pulmonary edema) (22). Furthermore, there are reports of difficult LMA insertion in patients with limited neck movement (23,24).
References
1. Samsoon GLT, Young JRB. Difficult tracheal intubation: a retrospective study. Anaesthesia 1987;14:17–27.
2. Rocke DA, Murray WB, Rout CC, et al. Relative risk analysis of factors associated with difficult intubation in obstetric anesthesia. Anaesthesiology 1992;77:67.
3. Sakles JC, Laurin EG, Rantapaa AA, et al. Airway management in the emergency department: a one-year study of 610 tracheal intubations. Ann Emerg Med 1998;31:325–332.
4. Bair AE, Filbin MR, Kulkarni RG, et al. The failed intubation attempt in the emergency department: analysis of prevalence, rescue techniques, and personnel. J Emerg Med 2002;23:131–140.
5. Cass NM, James NR, Lines V. Difficult direct laryngoscopy complicating intubation in anaesthesia. BMJ 1956;1:488–490.
6. Bellhouse CP, Dore C. Criteria for estimating likelihood of difficulty of endotracheal intubation with the MacIntosh laryngoscope. Anaesth Intensive Care 1988;16:329.
7. Savva D. Prediction of difficult tracheal intubation. Br J Anaesth 1994;73:149.
8. Tse JC, Rimm EB, Hussain A. Predicting difficult endotracheal intubation in surgical patients scheduled for general anesthesia: a prospective blind study. Anesth Analg 1995;81:254.
9. El-Ganzouri AR, McCarthy RJ, Tuman KJ, et al. Preoperative airway assessment: predictive value of a multivariate risk index. Anesth Analg 1996;82:1197–204.
10. Oates JD, MacLeod AD, Oates PD, et al. Comparison of two methods for predicting difficult intubation. Br J Anaesth 1991;66:305.
11. Rose DK, Cohen MM. The airway: problems and predictions in 18,500 patients. Can J Anesth 1994;41:372–383.
12. Mallampati SR. Clinical sign to predict difficult tracheal intubation (hypothesis). Can Anesth Soc J 1983;30:316.
13. Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult intubation: a prospective study. Can Anesth Soc J 1985;32:429.
14. Langeron O, Masso E, Hurax C, et al. Prediction of difficult mask ventilation. Anaesthesiology 2000;92:1229.
15. Wilson ME, Spiegelhalter D, Robertson JA, et al. Predicting difficult intubation. Br J Anaesth 1988;61:211.
16. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984;39:1105.
17. Benumof JL. The ASA difficult airway algorithm: new thoughts and considerations. In: Hagberg CA. Handbook of difficult airway management. Philadelphia: Churchill Livingstone; 2000;31–48.
18. Adnet F, Baillard C, Borron SW, et al. Randomized study comparing the “sniffing position” with simple head extension for laryngoscopic view in elective surgery patients. Anesthesiology 2001;95:836–841.
19. Levitan RM, Ochroch AE, Hollander J, et al. Assessment of airway visualization: validation of the percent of glottic opening (POGO) scale. Acad Emerg Med 1998;5:919–923.
20. Mason RA, Fielder CP. The obstructed airway in head and neck surgery. Anaesthesia 1999;54:625–628.
21. Donlon J Jr. Anesthetic and airway management of laryngoscopy and bronchoscopy. St. Louis, MO: Mosby; 1996.
22. Buckham M, Brooker M, Brimacombe J, et al. A comparison of the reinforced and standard laryngeal mask airway: ease of insertion and the influence of head and neck position on oropharyngeal leak pressure and intracuff pressure. Anaesth Intensive Care 1999;27:628–631.
23. Ishimura H, Minami K, Sata T, et al. Impossible insertion of the laryngeal mask airway and oropharyngeal axes. Anesthesiology 1995;83:867–869.
24. Olmez G, Nazaroglu H, Arslan SG, et al. Difficulties and failure of laryngeal mask insertion in a patient with ankylosing spondylitis. Turk J Med Sci 2004;34:369–352.