An 86-year-old patient with a prior history of hypertension, hyperlipidemia, and atrial fibrillation presents with difficulty speaking and right-sided numbness. On examination, she has apraxia of speech and right hemiparesis. An MRI shows a left internal carotid occlusion with acute ischemic change in the left cerebral hemisphere. Systolic blood pressure is fluctuating and at times 130 mmHg. It appears that her speech problems also fluctuate, and a possible link between worsening aphasia and relative hypotension is assumed. The decision is made to discontinue atenolol to maintain a higher blood pressure. Within 12 hours, the patient develops a rapid ventricular response to her atrial fibrillation with a pulse up to 140 beats per minute. Serum troponin has increased to 0.16 ng/ml. The electrocardiogram (EKG) shows rate-related repolarization changes (Figure 22.1). The patient is transferred to the Neurosciences Intensive Care Unit for acute management.
What do you do now?
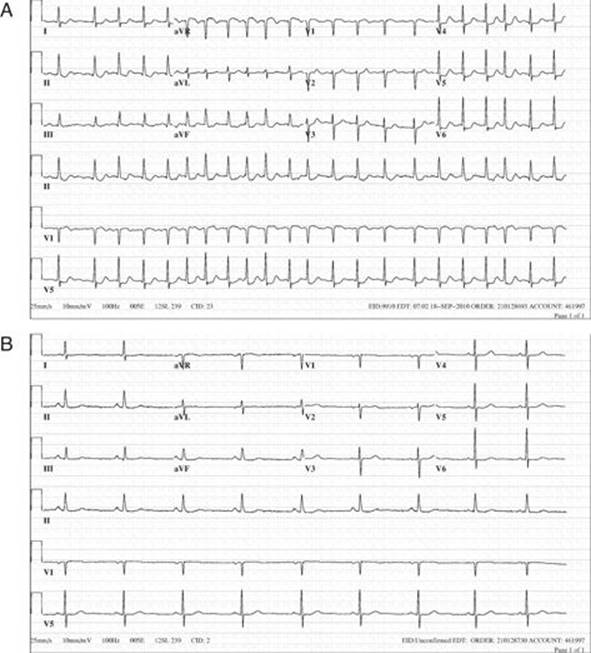
FIGURE 22.1 EKG: Atrial fibrillation and rapid ventricular response (A) with resolution (B).
Cardiac arrhythmias and EKG changes are quite common in patients with critical neurologic illness, often need more than cursory attention and management may become complex. Cardiac arrhythmias are often brief periods of premature beats, sinus bradycardia, or, as it is in our case, atrial fibrillation with rapid ventricular response. Conversely, an intracerebral hematoma may coincide with long-standing atrial fibrillation. An intracranial hemorrhage can be an unintended consequence of warfarin therapy to protect the patient from an ischemic stroke. In patients with an ischemic stroke, atrial fibrillation may not have been treated with warfarin or may have been recently discontinued for a surgical procedure leading to mobilization of an atrial thrombus to a major cerebral artery. In other patients there may be no direct correlation, and a carotid or basilar artery occludes from progressive atherosclerotic disease, such as in our patient example.
After an acute ischemic stroke patients may have a relatively low to normal blood pressure, and that is partly due to sudden bed rest and relative dehydration. “Low” systolic blood pressure (less than 155 mmHg) has been associated with increased mortality after a stroke, but the nature of the relationship remains unexplained. This all provides a motivation to increase the blood pressure in the acute stage. Not infrequently, beta-blockers are first discontinued to allow for higher blood-pressures. This may provide better perfusion in collaterals and could reduce the ischemic area.
However, the risks of such an intervention are not known. Stopping rate control medication in patients with atrial fibrillation may result in tachycardia that could lead to demand ischemia, which may be more severe in patients with coronary artery disease. This occurred in our case example with an increase in serum troponin.
The treatment for atrial fibrillation with rapid ventricular rate is either calcium channel blockers (for example intravenous diltiazem) beta-blockers, or amiodarone. These drugs control ventricular rate successfully, but amiodarone induces less hypotension and has higher frequency of converting patients with new onset atrial fibrillation into normal sinus rhythm. Cardioversion is rarely attempted in acute stroke because 1) patients often would need at least two days of anticoagulation, 2) hypotension might be deleterious to the patient, and 3) atrial fibrillation is often long-standing and patients are unlikely to stay in sinus rhythm. After control of the ventricular response is achieved, oral doses of beta-blockers (i.e. metoprolol) are administered to maintain rate control.
It is true that cardiac arrhythmias are prevalent in the NICU, but they may just be transient and without any consequence. Drug induced arrhythmias should be excluded. However, any new cardiac arrhythmia could point toward new onset sepsis, pulmonary emboli, or sudden blood loss. Acute myocardial ischemia with new cardiac arrhythmias may occur in any patient with a recent neurosurgical procedure. There are far more details that need to be known, but a general guideline for treatment of cardiac arrhythmias is shown in Table 22.1.
Another commonly asked question is whether the EKG changes are a result of the acute neurologic injury (a favorite cardiologist explanation). Morphological EKG changes are common in traumatic brain injury and subarachnoid hemorrhage (typically S-T segment sagging, prolonged QT interval, and symmetrically peaked T-waves often referred to as cerebral T-waves), and patients with ischemic strokes affecting the insula appear to be more prone to cardiac arrhythmias. However, most often it is not prudent to solely attribute cardiac rhythm changes to the acute brain injury. Further cardiac evaluation is necessary in the vast majority of patients.
TABLE 22.1 Guidance for the Treatment of Common Cardiac Arrhythmias
|
Arrhythmia |
Therapy |
|
Sinus tachycardia |
Fluids, esmolol |
|
Sinus bradycardia |
Atropine, cardiac pacing |
|
Atrial fibrillation |
Diltiazem, esmolol, amiodarone |
|
Multifocal atrial tachycardia |
Verapamil or metoprolol |
|
Atrioventricular block |
Cardiac pacing |
|
Ventricular tachycardia |
Cardioversion |
|
Torsades de pointes |
Magnesium sulfate |
Adapted from Wijdicks EFM, The Practice of Emergency and Critical Care Neurology, Oxford University Press, New York, 2010.
KEY POINTS TO REMEMBER REGARDING CARDIAC ARRHYTHMIA AFTER ACUTE BRAIN INJURY
· Sudden discontinuation of anti-arrhythmic drugs can lead to rapid ventricular response (RVR) in patients with known atrial fibrillation.
· Treat cardiac arrhythmias when symptomatic or at risk of becoming symptomatic. Correct serum potassium and magnesium.
· Amiodarone or diltiazem infusion will control RVR in atrial fibrillation.
· S-T segment sagging, prolonged QT interval and peaked T-waves may be due to acute brain injury, but a comprehensive cardiac evaluation remains necessary.
· New EKG changes in critically ill neurologic patients could indicate acute myocardial ischemia or pulmonary emboli.
Further Reading
Barnes BJ, Hollands JM. Drug-induced arrhythmias. Crit Care Med 2010; 38: S188–197.
Bossone E, DiGiovine B, Watts S et al. Range and prevalence of cardiac abnormalities in patients hospitalized in a Medical ICU. Chest 2002; 122:1370–1376.
Goodman S, Weiss Y, Weissman C. Update on cardiac arrhythmias in the ICU. Curr Opin Crit Care 2008; 14:549–554.
Oppenheimer S. Cerebrogenic cardiac arrhythmias: Cortical lateralization and clinical significance. Clin Auton Res 2006; 16:6–11.
Samuels MA. The brain-heart connection. Circulation 2007; 116:77–84.