Justin L. Gottlieb
Advances in vitreoretinal imaging techniques and success in surgical repair have stimulated great interest in the pathophysiology and natural history of macular holes. In particular, optical coherence tomography (OCT) provides unique imaging of the vitreomacular interface that has refined the understanding of macular hole formation. In the 25 years since Kelly and Wendel's landmark publication describing the successful repair of macular holes with vitrectomy surgery,[1] the surgical technique continues to be refined with improved anatomic and visual outcomes.
EPIDEMIOLOGY AND RISK FACTORS
Macular holes have been reported in association with many causes, including trauma,[2] laser treatment,[3] retinal vascular disease,[4,5] retinal detachment repair,[6,7] lightening,[8] and electrocution,[9] but the vast majority of cases are age-related and idiopathic, unrelated to other antecedent events or other ocular disease. The Eye Disease Case-Control Study Group reported that 72% of idiopathic holes occurred in women and more than 50% in patients 65-74 years of age[10] The observed increased risk in females is poorly understood and explanations only speculative. Investigating the increased incidence of macular hole in females, the case study report found that estrogen use was protective but did not find an association with prior hysterectomy. The observation of macular holes among siblings within four different families has also suggested a possible genetic component in the formation of macular holes.[11]
The risk of full-thickness macular hole formation in the fellow eye is estimated to be ~10-15%.[12-15] Normal fellow eyes with posterior vitreous detachment appear to be at a very low risk of macular hole development.[14,16] However, in fellow eyes with persistent vitreofoveal attachments (as evidenced by optical coherence tomography) 11% of fellow eyes developed a full-thickness macular hole over a 2 year period of observation.[17]
PATHOGENESIS
Theories from the early nineteenth century of the pathogenesis of macular hole focused on trauma,[18] although contemporary reports find that greater than 80% are idiopathic.[19] Early histological description of full-thickness hole noted cystic intraretinal changes.[20,21] These changes were usually assumed to be due to ocular trauma, supporting the prevailing theories of the era.
Other early theories of macular hole formation suggested that macular cysts may form atraumatically and degenerate into macular holes.[22,23] Kuhnt implicated a degenerated fovea as the cause of macular hole and termed this disorder retinitis atrophicans sive rarificans centralis.[22] The implication of cystoid degeneration, coalescence of cystic spaces, and the development of a full-thickness hole was an important development in the understanding of macular hole development, as it emphasized that trauma was not a necessary precedent event.[24]
Current concepts of macular hole formation focus on the role of the vitreomacular interface. As early as 1924, Lister stated the importance of the vitreous in the pathogenesis of macular hole,[25] noting traction of fibrous bands in the vitreous. However, he was puzzled by his own clinical observations of a lack of visible tractional vitreous bands in cases of macular holes.[26] Several series from the 1960s described signs of vitreomacular traction contributing to macular hole formation.[27-30]
Avila and Jalkh concluded that persistent vitreous-to-macula traction was important in the formation of macular holes, as 53% of their cases of macular holes did not have a posterior vitreous detachment demonstrable on biomicroscopic examination.[31] Similarly, Akiba et al described the progression of premacular hole lesions to fully developed holes without the occurrence of a posterior vitreous detachment.[32] In contrast, McDonnell et al noted a complete vitreous separation in all macular hole cases and in all cases observed to progress from premacular hole lesions to full-thickness macular hole,[33] concluding that the act of vitreous separation from the macula was critical to the formation of a full-thickness hole. It is interesting that each group concluded that vitreous traction on the macula was important in the pathogenesis of macular holes, but arriving at this conclusion from seemingly contradicting evidence.
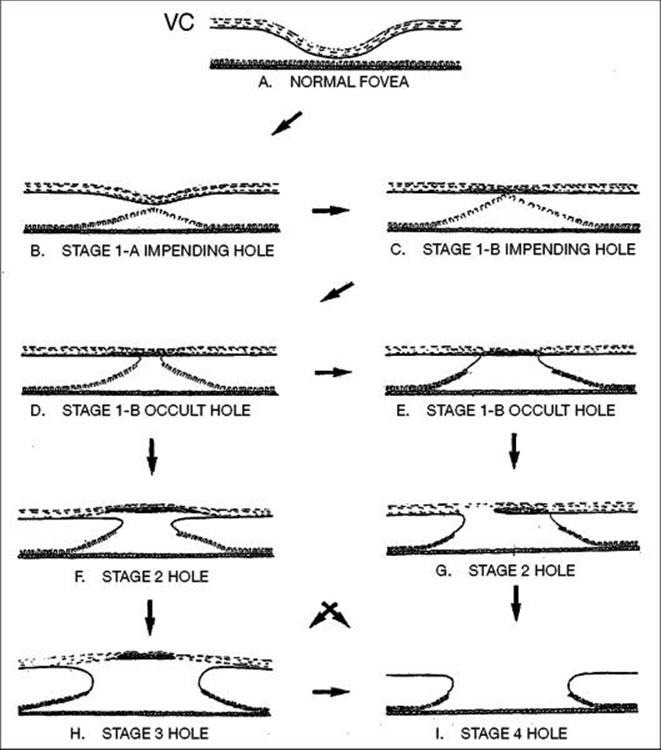
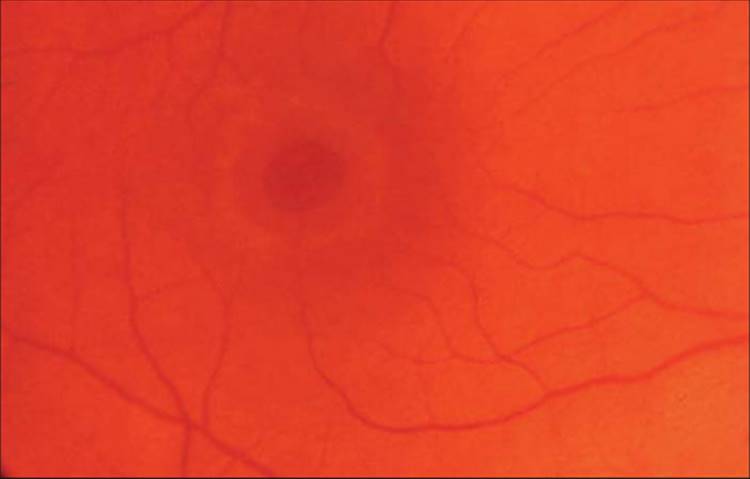
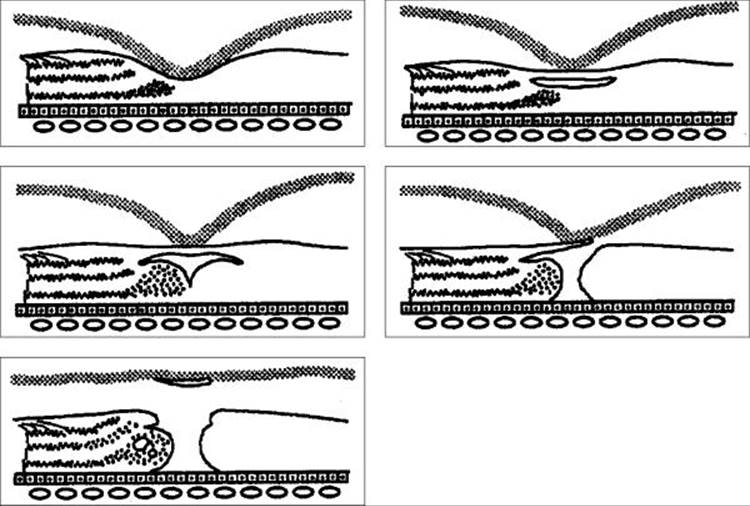
The current concept of macular hole pathogenesis has grown from the understanding that vitreofoveal traction is central to the development of and progression to a full-thickness macular hole. In 1988, Gass[31] and Johnson and Gass[35] proposed a new hypothesis of macular hole formation, including a classification scheme for idiopathic holes and precursor lesions. This classification scheme has guided the description of macular hole development and theories of pathogenesis since that time. Gass proposed that contraction of prefoveolar cortical vitreous resulted in tangential traction. This traction resulted in a predictable progression through multiple stages of development (Fig. 155.1). Stage 1 is the earliest biomicroscopic sign of an impending macular hole and results from a foveolar or foveal detachment. Ophthalmoscopically, it appears as a yellow dot (stage 1a) or yellow ring (stage 1b), respectively (Fig. 155.2). Progressive tangential traction may result in a small full-thickness break in the neurosensory retina. These holes were described as eccentric can-opener shaped tears or small central defects (stage 2) (Fig. 155.3). These small holes usually progressed to larger 400-500 ?m holes with or without operculum (stage 3) (Fig. 155.4) and finally may involve the separation of the posterior vitreous (stage 4) (Fig. 155.5).
|
|
|
|
FIGURE 155.1 Schematic diagram of stages of development of idiopathic macular hole based on biomicroscopic observations as proposed by Gass. See text for detail. |
|
|
|
|
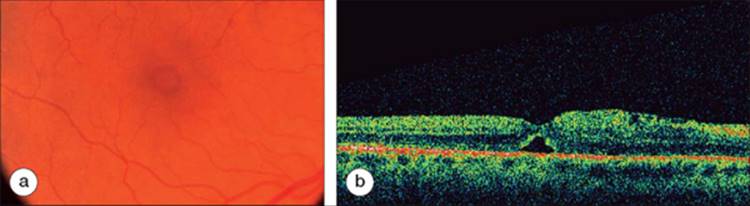
FIGURE 155.2 (a) Color fundus photograph of stage 1b hole. Note the central yellow ring. (b) Optical coherence tomography of stage 1 hole. Note the foveolar detachment. Visual acuity was 20/25. This eye later developed a full-thickness macular hole. |
|
|
|
|
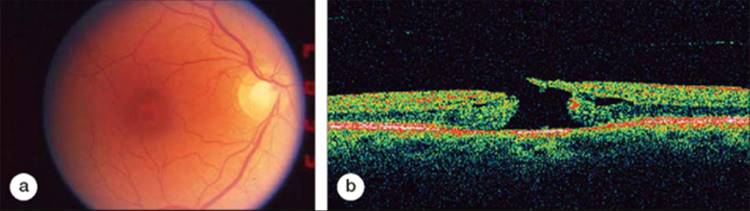
FIGURE 155.3 (a) Color fundus photograph of stage 2 macular hole. The hole is full-thickness but a diameter less than 400 ?m. (b) Optical coherence tomograph of stage 2 macular hole. Note the vitreous traction on the operculum which is not yet detached from the retina. |
|
|
|
|
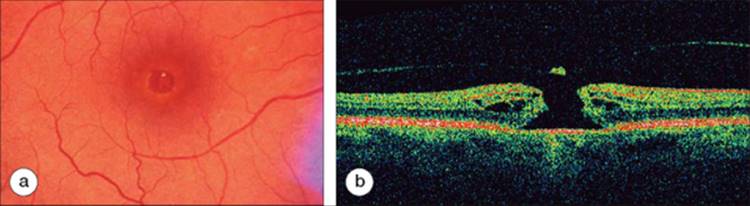
FIGURE 155.4 (a) Color fundus photograph of a stage 3 hole. This hole is at least 400 ?m in diameter and has an overlying pseudo-operculum. (b) Optical coherence tomography of stage 3 hole. In comparison to Figure 155.3b, the operculum is clearly detached form the retina surface and attached to the posterior vitreous. |
|
|
|
|
FIGURE 155.5 Color fundus photograph of stage 4 hole. This hole was present for at least 1 year and the visual acuity had decreased to 20/200. |
Dr Gass later provided a revision and update of the biomicroscopic classification.[36] In this reappraisal, Gass proposed that the yellow ring of a stage 1b hole is due to centrifugal displacement of retinal receptors after a dehiscence at the umbo. The occult hole may be hidden by the semiopaque prefoveolar condensed vitreous cortex bridging the hole. The occult hole may then become visible after an early separation or an eccentric can-open-like tear in the condensed prefoveolar vitreous cortex. The prefoveolar cortex may then form a prehole pseudo-operculum. This scheme helped to unify surgical observations of restoration of foveal architecture and sometimes near normal function, which seemed at odds with the earlier scheme of pathogenesis in which foveal opercula containing photoreceptors were thought to develop (Fig. 155.1).
MACULAR HOLE IMAGING AND PATHOGENESIS
The classification scheme and description of pathogenesis provided by Dr Gass was based primarily on biomicroscopic observations. Other diagnostic studies may be used to help establish the diagnosis of macula hole, although the biomicroscopic appearance remains the primary means of diagnosis. Fluorescein angiography may show focal hyperfluorescence in stage 1 and stage 2 holes.[34] However, a similar pattern may be present in lesions mimicking macular holes, such as epiretinal membrane with pseudohole. B-scan ultrasonography is an excellent means of imaging the posterior vitreous hyaloid and may help determine the presence of persistent vitreous attachment to the macula.[14,37,38] It is rarely utilized to determine the presence of macular hole in clinical practice and except for the determination of posterior vitreous detachment, is not useful for staging macular holes.
Ocular coherence tomography (OCT) is a medical imaging technology that has improved the imaging of both the neurosensory retina and vitreoretinal interface.[39] OCT has especially improved visualization of very shallow detachments of the posterior hyaloid over the macula. Even with contact lens biomicroscopy this shallow detachment over the parafovea and macula is most often imperceptible. Information gained from OCT evaluation of macular hole formation in evolution has provided new understandings of the sequence of events leading from vitreofoveal traction to full-thickness macular hole formation. Gaudric et al[40] utilized OCT to study eyes with macular holes as well at the fellow eyes to detect the initial stages of vitreous separation. They were able to demonstrate initial stages of vitreous separation in the peripheral portions of the macula which then spread throughout the macula with the hyaloid remaining focally adherent to the foveola and the optic disk. A distinct convexity was observed, suggesting antero-posterior traction from the vitreous (Figs 155.2b, 155.3b, 155.4b, and 155.6). Other investigators have confirmed the ability of OCT to detect the perifoveal vitreous detachment.[41,42,43]
|
|
|
|
FIGURE 155.6 Schematic diagram of macular hole formation based on optical coherence tomography observations. |
Johnson and co-workers[44] utilized B-scan ultrasonography and vitreoretinal surgical observations of eyes with stage 1 or stage 2 macular holes. They demonstrated the presence of a shallow, localized detachment of perifoveal vitreous typically extending to the temporal vascular arcades, supporting the findings of Gaudric. The elegant findings of investigators using OCT[40-42] and B-scan ultrasonography[14,44] suggest a modified theory of macular hole pathogenesis implicating age-related posterior vitreous detachment beginning in the perifoveal region with abnormally strong persistent vitreofoveal adherence. This theory implicates anteroposterior traction, not the tangential traction as suggested by Gass.[34,36,45] Smiddy and Flynn[46] present a unifying theory incorporating observations of early cystic degeneration, attempted wound healing by Müller and glial cells creating tangential traction, and later anteroposterior traction as clearly seen in OCT imaging. They suggest that it is possible that the weakened or dehisced central fovea may be a primary event, followed by attempted repair by focal proliferation of Müller and glial cells, and persistent anteroposterior traction at the foveola finally resulting in an irreversible development of full-thickness hole.
Staging systems utilizing the observations from OCT have been developed. These generally retain the Gass biomicroscopic stages 1A/1B through four as a basis.[47]
NATURAL HISTORY
There is a wide range of variation in the stated progression of pre-hole (stage 1 or macular 'cyst') lesions to full-thickness hole formation. The Vitrectomy for Prevention of Macular Hole Study Group[48]reported that 40% of eyes with stage 1 lesions randomized to observation progressed to full-thickness macular hole over 2 years. This occurred in an average time of 4.1 months after diagnosis. Other studies are mostly small and retrospective. Rates of progression from premacular hole lesions to full-thickness holes range from ~10 to 70%.[35,36,48,49]
Generally, spontaneous resolution of stage 1 lesions is associated with a vitreofoveal separation with foveal reattachment and a normal biomicroscopic appearance, or may demonstrate an inner lamellar hole.[36]
Visual symptoms in stage 1 or early stage 2 lesions include metamorphopsia and reduced visual acuity. The visual acuity of eyes with stage 1 macular holes may help to predict the progression to full-thickness hole formation. The visual acuity of most stage 1 lesions ranges from 20/25 to 20/80. In one retrospective series, if the visual acuity was 20/40 or better, 23% progressed to a macular hole within 2 years, whereas, if the visual acuity was 20/50 or worse, 89% progressed to macular hole.[19] The Vitrectomy for Prevention of Macular Hole Study Group similarly found that stage 1 macular holes with best-corrected visual acuity of 20/50 to 20/80 had a 66% rate of progression, while eyes with best-corrected visual acuity of 20/25 to 20/40 had a 30% risk of progression to full-thickness macular hole.[48]
The majority of stage 2 holes continue to progress to stage 3 or stage 4 holes.[50,51] Stage 3 macular holes have central visual acuity loss to the 20/80 to 20/200 level.[51] There is a strong co-relation between macular hole diameter and visual acuity.[51,52] Similarly, the hole diameter (and visual acuity) is closely correlated to duration of symptoms.
DIFFERENTIAL DIAGNOSIS
|
Key Features |
||||||||||||||||||||||||
|
Several lesions may simulate a full-thickness macular hole or a precursor macular hole lesion (stage 1a or 1b). The most common lesion to be mistaken for a full-thickness macular hole is an epiretinal membrane and pseudohole.[53] Also simulating a full-thickness macular hole may be a lamellar macular hole[54] or chronic cystic macular edema.
Premacular hole lesions are often misdiagnosed. Gass and Joondeph[55] reported that only one of 18 patients referred with a diagnosis of stage 1 lesion actually had such a lesion. The other misdiagnosed lesions included aborted macular hole, stage 2 holes, stage 3 holes, and unrelated lesions. Other lesions simulating a 'pre-hole' lesion may include central serous chorioretinopathy with a central yellow spot,[55] the early yellow lesion of solar retinopathy,[55] a central druse in age-related macular degeneration,[55] or a pseudo-operculum.[56]
MANAGEMENT OF MACULAR HOLES
Because of the preservation of peripheral vision and the relative rarity of bilateral central visual loss, some have questioned the necessity for surgical intervention for repair of macular holes.[57] However, the improvements in surgical techniques and results and a concomitant decrease in overall surgical complications of vitreoretinal surgery have led most vitreoretinal surgeons to readily recommend surgical repair for affected eyes. Most retina specialists now recommend surgery for symptomatic stage 2, 3, or 4 macular holes of limited duration with visual acuity of at least 20/50 or worse.
Appreciating the role of vitreomacular traction in macular hole formation led to the first attempts at macular hole repair through pars plana vitrectomy surgery. In 1991, Kelly and Wendel reported on pars plana vitrectomy, removal of the posterior cortical vitreous, and strict facedown positioning after gas-fluid exchange for repair of macular hole.[1] The original technique of Kelly and Wendel remains the basis of surgical technique today.
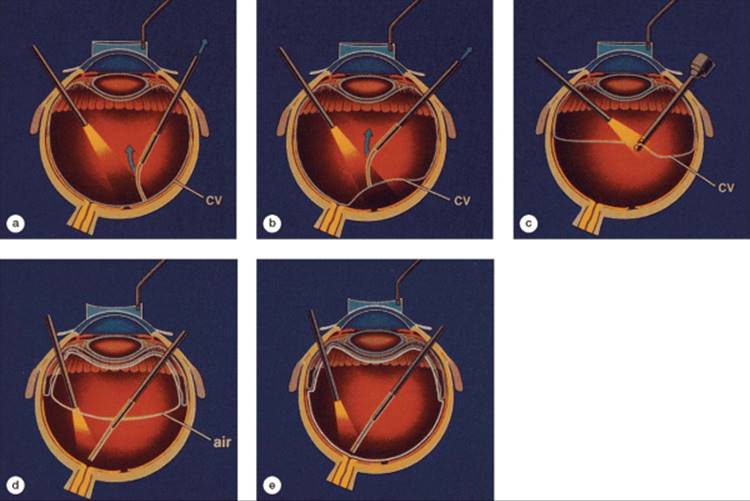
The critical component of the surgical repair macular holes is the induction of a posterior vitreous detachment (Fig. 155.7). This is confirmed intraoperatively by the identification of a Weiss ring and the visualization of the more opaque posterior cortical vitreous face of the vitreous. The posterior cortical vitreous may be identified with the use of a soft silicone extrusion cannula. With gentle aspiration, the silicone tip will engage the posterior cortical vitreous and induce a bend in the tip similar to a 'fish-strike' on a fishing line.[1] Many surgeons simply use the vitrectomy cutting instrument on aspiration mode to engage and elevate the posterior cortical vitreous, prior to carefully completing the vitrectomy to the vitreous base. Epiretinal membranes are then generally excised using a barbed microvitreoretinal blade, diamond-dusted silicone scraper and/or fine intraocular forceps. Indirect ophthalmoscopy of the retina is performed to carefully inspect for iatrogenic retinal tears, most often associated with the process of vitreous separation.[58] A fluid-air exchange is performed, followed by a second fluid aspiration at least 10 min after the initial fluid-air exchange. The second aspiration allows for removal of the preretinal fluid accumulating from the residual vitreous skirt, ciliary body, and anterior-segment structures.[59] The air is then exchanged with a longer acting, nonexpansile concentration of gas. Face-down positioning is required postoperatively to provide maximum tamponade of the gas upon the surface of the macula and to stimulate closure of the macular hole.
|
|
|
|
FIGURE 155.7 Basic steps in vitrectomy surgery for macular hole. (a) Engagement of posterior cortical vitreous (CV) with a soft-tipped extrusion cannula during active aspiration - 'the fish-strike sign'. (b) Stripping of the CV. (c) Completion of the posterior vitrectomy with the vitreous cutter. (d) Fluid-air exchange. (e) Completion of fluid-air exchange with removal of fluid over the optic nerve. |
In the initial report of successful macular hole surgery by Kelly and Wendel, 58% of the holes were successfully closed and visual acuity improvement by two or more lines occurred in 42% (73% of anatomically successful eyes). In a second report, Wendel and co-authors reported improved success with 73% anatomic success and 55% improvement by two or more lines.[60] The authors noted greater success in holes present for less than 6 months. The greater success with holes present for shorter duration has been confirmed by a number of other authors.[61,62]
Most reports of visual and anatomic results are small and uncontrolled. The definitions of anatomic and visual success differ among the many reports. Two multicenter, randomized clinical trials provide information regarding success rates. Kim and colleagues reported the results of surgery for stage 2 macular holes.[63] There was no statistically significant difference in ETDRS chart visual acuity between the surgical and observed groups. However, the Bailey-Love word-reading test did show a significant difference between the two groups (20/78 vs 20/135, P = 0.006).
In a second report from the Vitrectomy for Treatment of Macular Hole Study Group, Freeman and colleagues reported the results of surgery versus observation for stages 3 and 4 macular holes.[64] They report a 69% closure rate, as compared with a 2% spontaneous closure rate in the observation group. The surgically repaired eyes had a statistically significant better visual acuity at 6 months, both by ETDRS chart testing (20/115 versus. 20/166, P ? 0.004) and by Bailey-Love word-reading test (20/155 vs 20/166, P=<0.01).
A 2 year randomized clinical trial from Moorefields Eye Hospital compared surgery to observation for full-thickness macular holes of less than or equal to 9 months duration.[65] They additionally compared whether the addition of autologous serum improved results in the surgical arm. They reported an 11.5% spontaneous closure rate with little or no visual acuity change of those eyes at 24 months. The surgical group had an overall closure rate of 80.6%, with 45% of eyes achieving a visual acuity of 20/40 or greater. Autologous serum did not affect the anatomic or visual results.
CONTROVERSIES IN MACULAR HOLE REPAIR SURGERY
SURGICAL ADJUVANTS
Most surgeons do not currently use adjuvant agents in the surgical repair of macular holes. Such adjuvants are generally applied to the surface of the macular hole at the conclusion of vitrectomy surgery and fluid-air exchange and still require face-down positioning after an initial period of prone positioning. Glaser et al reported initial success with intravitreal transforming growth factor beta (TGF-?) derived from bovine bone with higher anatomic closure rate compared with placebo.[66] However TGF-? derived from recombinant DNA did not result in similar success.[67]
Other blood-derived adjuvants, such as autologous serum,[65,68] autologous concentrated platelets,[69] and whole blood[70] have also been utilized. Randomized clinical trials using autologous serum have not demonstrated improved closure rates or visual results.[65,68] Similarly, platelet concentrates and whole blood have not proven effective in clinical trials.
INTERNAL LIMITING MEMBRANE PEEL
Currently, the greatest controversy in surgical technique for macular hole is the role of internal limiting membrane (ILM) peeling. The necessity, preferred technique, and potential complications, including toxicity of adjuvant agents are far from definitively established.
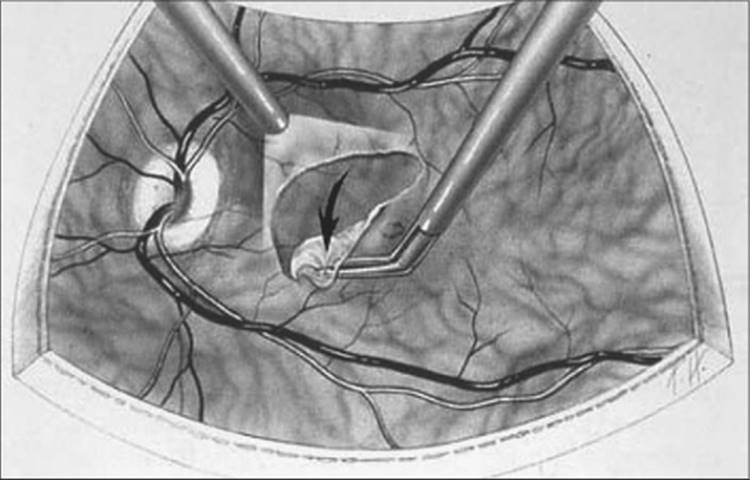
Techniques for removal of the ILM involve establishing an elevated edge of the ILM and then peeling the ILM from around the macular hole. Establishing an initial edge may be accomplished with the use of a barbed microvitreoretinal blade[71] or with the use of fine intraocular end-grasping forceps to 'pinch' and elevate the ILM.[72] The ILM peel is most often performed in a circular motion around the hole ('maculorhexis') (Fig. 155.8).[73]
|
|
|
|
FIGURE 155.8 Peeling the internal limiting membrane with forceps in a circular fashion around the macular hole - 'macculorhexis'. |
Removal of the ILM appears to increase the rate of macular hole closure and perhaps improve the final visual acuity. Closure rates as high as 88-100% have been reported.[71-75] However, no prospective, randomized trials have been performed to compare standard procedures with and without ILM peeling. A retrospective comparative study of hole closure rate and postoperative visual acuities did not demonstrate a statistical difference in outcomes.[76]
The identification and peeling of the ILM is technically challenging. Adjuvants to improve visualization of the ILM include indocyanine green dye (ICG), trypan blue dye, and triamcinolone acetonide.
Indocyanine green dye is instilled onto the surface of the retina in an air-or fluid-filled eye. The ICG selectively stains the ILM, and the ILM may be more easily identified and elevated with the use of diamond-dusted silicone cannula or with fine end-grasping forceps (Fig. 155.9). Retinal and retinal pigment epithelial toxicity[77-79] have been reported and questions have arisen about potentially diminished visual acuity in eyes exposed to intravitreal ICG dye.[80] Others report excellent results with the use of adjunctive-ICG without evidence of toxicity.[81] No randomized, prospective trials have been performed.
|
|
|
|
FIGURE 155.9 Intraoperative photograph of peeling of the internal limiting membrane after staining with indocyanine green dye. |
Trypan blue stains both the ILM and epiretinal membranes. The staining of the ILM is less intense than the staining achieved with ICG.[82,83] There have been no reports of toxicity associated with trypan blue.
Triamcinolone acetonide can be injected intraoperatively onto the surface of the macula. While it does not stain the internal membrane, it adheres to the surface and may facilitate identification of the ILM.[84,85]
DURATION OF FACE-DOWN POSITIONING
Currently most vitreoretinal surgeons recommend strict face-down positioning for at least 1 week postoperatively. Compliance with positioning seems to increase the success rates of hole closure.[60] Studies of decreased duration suggest that successful closure of holes can occur with 0-4 days of positioning.[86,87] The shorter duration of positioning depends on a very complete vitreous removal in a pseudophakic eye and successful ILM peeling.[87]
The use of silicone oil for postoperative tamponade has been advocated for patients unable to position. The visual acuity and closure rates are better among eyes undergoing surgery with gas tamponade compared with silicone oil.[88,89]
COMPLICATIONS OF MACULAR HOLE SURGERY
|
Key Features |
|||||||||||||||||||||
|
The most common complication of macular hole surgery is cataract formation.[90,91,92] Phakic patients undergoing macular hole surgery should be advised that cataract extraction surgery will likely be required within 1-2 years after macular hole surgery. Other surgical complications include intraoperative iatrogenic retinal tears (3-17%),[74,93,94] postoperative retinal detachment (1-5% in most reports, but up to 14% reported).[74-76,87,93,95] Postoperative retinal detachments are most typically inferiorly located and associated with small retinal tears at the vitreous base. Visual-field loss (up to 20%),[96,97] may be due to excessive infusion pressures and retinal dehydration during fluid-air exchange.[98,99] Elevated intraocular pressures are common after vitrectomy surgery with intraocular gas infusions[100] and angle closure in the unoperated eye during face-down positioning has been reported.[101]
SUMMARY
Full-thickness macular holes are most often unilateral, age-related, and idiopathic. Visual symptoms include central metamorphopsia and reduced visual acuity. Improved understanding of the pathophysiology of macular holes has occurred through careful biomicroscopic observations and through the improved visualization of the vitreoretinal interface provided by OCT. Vitreoretinal surgical techniques continue to evolve, and there remain questions as to the best surgical approach to macular holes. However, surgery most often results in successful closure of the macular hole and improvement of visual function. Vision-targeted health status questionnaires demonstrate that successful macular hole closure is associated with significant improvement in patients' vision-related quality of life, even when there is only modest improvement in visual acuity.[102]
REFERENCES
1. Kelly NE, Wendel RT: Vitreous surgery for idiopathic macular holes: results of a pilot trial. Arch Ophthalmol 1991; 109:654-659.
2. Knapp H: Ueber isolerte zerreissungen der aderhaut in folge von traumen auf dem augapfel. Arch Augenklinik 1869; 1:6-29.
3. Vendantham V: Optical coherence tomography findings in macular hole due to argon laser burn. Arch Ophthalmol 2006; 124(2):287-288.
4. Cohen SM, Gass JDM: Macular hole formation following severe hypertensive retinopathy. Arch Ophthalmol 1994; 112:878-879.
5. Amemiya T, Yoshida H: Macular hole in diabetic maculopathy. Ophthalmologica 1978; 177:188-191.
6. Brown GC: Macular hole following rhegmatogenous retinal detachment repair. Arch Ophthalmol 1988; 106:765-766.
7. Runge PE, Wyhinny GJ: Macular hole secondary to pneumatic retinopexy: case report. Arch Ophthalmol 1988; 106:586-587.
8. Campo RV, Lewis RS: Lightening-induced macular hole. Am J Ophthlamol 1984; 97:792-794.
9. Chavanne H: Pseudo-trou maculaire par electrocution. Bull Soc Ophthalmol Fr 1958.271-275.
10. Risk factors for idiopathic macular holes : The Eye Disease Case-Control Study Group. Am J Ophthalmol 1994; 118:754-761.
11. Lalin SC, Chang S, Flynn H, et al: Familial idiopathic macular holes. Am J Ophthalmol 2004; 138:608-611.
12. Ezra E, Wells JA, Gray RH, et al: Incidence of idiopathic full-thickness macular holes in fellow eyes. A 5-year prospective natural history study. Ophthalmology 1998; 105:353-359.
13. Lewis ML, Cohen SM, Smiddy WE, Gass JD: Bilaterality of idiopathic macular holes. Graefes Arch Clin Exp Ophthalmol 1996; 234:241-245.
14. Fisher YL, Slakter JS, Yannuzzi LA, Guyer DR: A prospective natural history study and kinetic ultrasound evaluation of idiopathic macular holes. Ophthalmology 1994; 101:5-11.
15. Guyer DR, de Bustros S, Diener-West M, Fine SL: Observations on patients with idiopathic macular holes and cysts. Arch Ophthalmol 1992; 110:1264-1268.
16. Akiba J, Quiroz MA, Trempe L: Role of posterior vitreous detachment in idiopathic macular holes. Ophthalmology 1990; 97:1610-1613.
17. Niwa H, Tersasaki H, Ito Y, Mikake Y: Macular hole development in fellow eyes with unilateral macular hole. Am J Ophthalmol 2005; 140:370-375.
18. Kipp CJ: Macular holes: a clinical contribution. Tran Am Ophthalmol Soc 1908; 11:518-528.
19. McDonnell PJ, Fine SL, Hillis AI: Clinical features of idiopathic macular cysts and holes. Am J Ophthalmol 1982; 93:777-786.
20. Fuchs E: Zur veranderung der macula lutea nach contusion. Ztschr Augenheilk 1901; 6:181-186.
21. Coats G: The pathology of macular holes. Roy London Hosp Report 1907; 17:69-96.
22. Kuhnt H: Ueber eine eigenthumliche Veranderung der Netzhaut as maculam (retinitis atrophicans sive rare-cans centralis). Z Augneheilk 1900; 3:105-112.
23. Tower P: Observations on hole in the macula. Ophthalmologica 1954; 40(suppl):1-60.
24. Aaberg TM, Blair CJ, Gass JDM: Macular holes. Amer J Ophthalmol 1970; 69:640-650.
25. Lister W: Holes in the retina and their clinical signi-cance. Br J Ophthalmol 1924; 8:1-20.
26. Aaberg TM: Macular holes: A review. Surv Ophthalmol 1970; 15:139-162.
27. Reese AB, Jones IS, Cooper WC: Macular changes secondary to vitreous traction. Am J Ophthalmol 1967; 64:544-549.
28. Aaberg TM, Blair CJ, Gass JDM: Macular holes. Am J Ophthalmol 1970; 69:555-562.
29. Yoshioka H: Clinical studies on macular holes. III. On the pathogenesis of the senile macular hole. Acta Soc Ophthalmol Jpn 1968; 72:575-584.
30. Jaffe NS: Vitreous traction at the posterior pole of the fundus due to alterations in the vitreous posterior. Tran Am Acad Ophthalmol Otolaryngol 1967; 71:642-652.
31. Avila MP, Jalkh AE, Murakami K, et al: Biomicroscopic study of the vitreous in macular breaks. Ophthalmol 1983; 90:1277-1283.
32. Akiba J, Quiroz MA, Trempe CL: Role of the posterior vitreous detachment in idiopathic macular holes. Ophthalmology 1990; 97:1610-1613.
33. McDonnell PJ, Fine SL, Hillis AI: Clinical features of idiopathic macular cysts and holes. Am J Ophthalmol 1982; 93:777-786.
34. Gass JDM: Idiopathic senile macular hole. Its early stages and pathogenesis. Arch Ophthalmol 1988; 106:629-639.
35. Johnson RN, Gass JDM: Idiopathic macular holes. Observations, stages of formation, and implications for surgical intervention. Ophthalmology 1988; 95:917-924.
36. Gass JDM: Reappraisal of biomicroscopic classi-cation of stages of development of a macular hole. Am J Ophthalmol 1995; 119:752-759.
37. Dagel PU, Smiddy WE, Byrnes SF, et al: Macular hole syndromes: echographic findings with clinical correlation. Ophthalmology 1994; 101:815-821.
38. Glacet-Bernard A, Zourdani A, Perrenoud F, et al: Stage 3 macular hole: role of optical coherence tomography and B-scan ultrasonography. Am J Ophthalmol 2005; 139:814-819.
39. Hee MR, Pulia-to CA, Wong C, et al: Optical coherence tomography of macular holes. Ophthalmology 1995; 102:748-756.
40. Gaudric A, Haouchine B, Massin P, et al: Macular hole formation. New data provided by optical coherent tomography. Arch Ophthalmol 1999; 117:744-751.
41. Chauhan DS, Antcliff RJ, Rai PA, et al: Papillofoveal traction in macular hole formation: the role of optical coherence tomography. Arch Ophthalmol 2000; 118:32-38.
42. Mori K, Abe T, Yoneya S: Dome shaped detachment pf premacular vitreous cortex in macular hole development. Ophthalmic Surg Lasers 2000; 31:203-209.
43. Chan A, Duker JS, Schuman JS, Fujimoto JG: Stage 0 macular holes. Observations by optical coherence tomography. Ophthalmology 2004; 111:2027-2032.
44. Johnson MW, Van Newkirk MR, Meyer KA: Perifoveal vitreous detachment is the primary pathogenic event in idiopathic macular hole formation. Arch Ophthalmol 2001; 119:215-222.
45. Gass JDM: Müller cell cone, an overlooked part of the anatomy of the fovea centralis: hypotheses concerning its role in the pathogenesis of macular hole and foveomacular retinoschisis. Arch Ophthalmol 1999; 117:821-823.
46. Smiddy WE, Flynn Jr HW: Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol 2004; 137:525-537.
47. Altaweel M, Ip M: Macular hole: improved understanding of pathogenesis, staging, and management based on optical coherence tomography. Sem Ophthalmol 2003; 18:58-66.
48. De Bustros S: Vitrectomy for prevention of macular holes. Results of a randomized multicenter clinical trial. Vitrectomy for prevention of macular hole study group. Ophthalmology 1994; 101:105-1059.
49. Guyer DR, de Bustros S, Diener-West M, Fine SL: The natural history of idiopathic holes and cysts. Arch Ophthalmol 1992; 110:1264-1268.
50. Hickichi T, Toshida A, Akiba J, et al: Prognosis of stage 2 macular holes. Am J Ophthalmol 1995; 119:571-575.
51. Kim JW, Freeman WR, Azen SP, et al: Prospective randomized trial of vitrectomy or observation for stage 2 macular holes. Am J Ophthalmol 1996; 121:605-614.
52. Sjaarda RN, Frank DA, Glaser BM, et al: Assessment of vision in idiopathic macular hole with macular microperimetry using the scanning laser ophthalmoscope. Ophthalmology 1993; 100:1513-1518.
53. Allen AW, Gass JDM: Contraction of a perifoveal epiretinal membrane simulating a macular hole. Am J Ophthalmol 1976; 82:684-691.
54. Smiddy WE, Gass JDM: Masquerades of macular holes. Ophthalmic Surg 1995; 26:16-24.
55. Gass JDM, Joondeph BC: Observations concerning patients with suspected impending macular holes. Am J Ophthalmol 1990; 109:638-646.
56. Gass JDM, VanNewkirk M: Xanthic scotoma and yellow foveolar shadow caused by a pseudo-operculum after vitreofoveal separation. Retina 1992; 12:242-244.
57. Fine SL: Vitreous surgery for macular hole in perspective. Is there an indication? (Editorial). Arch Ophthalmol 1991; 109:635-636.
58. Sjaarda RN, Glaser BM, Thompson JT, et al: Distribution of iatrogenic retinal breaks in macular hole surgery. Ophthalmology 1995; 102:1387-1392.
59. Rubin JS, Thompson JT, Sjaarda RN, et al: Ef-cacy of fluid-air exchange during pars plana vitrectomy. Retina 1995; 15:291-294.
60. Wendel RT, Patel AC, Kelly NA, et al: Vitreous surgery for macular holes. Ophthalmology 1993; 100:1671-1676.
61. Thompson JT, Sjaarda RN, Lansing MB: The results of vitreous surgery for chronic macular holes. Retina 1997; 17:493-501.
62. Willis AW, Garcia-Cosio JF: Macular hole surgery. Comparison of longstanding versus recent macular holes. Ophthalmology 1996; 103:1811-1814.
63. Kim JW, Freeman WR, Azen SP, et al: Prospective randomized trial of vitrectomy or observation for stage 2 macular holes. Vitrectomy for Macular Hole Study Group. Am J Ophthalmol 1996; 121:605-614.
64. Freeman WR, Azen SP, Kim JW, et al: Vitrectomy for treatment of full-thickness stage 3 or 4 macular holes. Results of a multicenter randomized clinical trial. The Vitrectomy for Treatment of Macular Hole Study Group. Arch Ophthalmol 1997; 115:11-21.
65. Ezra E, Gregor ZJ for the Moore-elds Macular Hole Surgery Group : Surgery for idiopathic full-thickness macular hole. Two-year results of a randomized clinical trial comparing natural history, vitrectomy, and vitrectomy plus autologous serum: Moore-elds Macular Hole Study Group Report No. 1. Arch Ophthalmol 2004; 122:224-236.
66. Smiddy WE, Glaser BM, Thompson JT, et al: Transforming growth factor-beta 2 signi-cantly enhances the ability to flatten the rim of subretinal fluid surrounding macular holes: preliminary results of a multicenter prospective randomized study. Retina 1993; 13:296-301.
67. Thompson JT, Smiddy WS, William GA, et al: Comparison of recombinant transforming growth factor beta-2 and placebo as an adjuvant for macular hole surgery. Ophthalmology 1998; 105:700-706.
68. Banker AS, Freeman WR, Azen SP, et al: A multicentered clinical study of serum as adjuvant therapy for surgical treatment of macular holes. Vitrectomy for Macular Hole Study Group. Arch Ophthalmol 1999; 117:1499-1502.
69. Paques M, Chastang C, Mathis A, et al: Effect of autologous platelet concentrate in surgery for idiopathic macular hole: results of a multicenter, double-masked, randomized trial. Platelets in macular hole surgery group. Ophthalmology 1999; 106:932-938.
70. Hoerauf H, Kluter H, Joachimmeyer E, et al: Results of vitrectomy and the no-touch-technique using autologous adjuvants in macular hole treatment. Int Ophthalmol 2001; 24:151-159.
71. Brooks Jr HL: Macular hole surgery with and without internal limiting membrane peeling. Ophthalmology 2000; 107:1939-1949.
72. Smiddy WE, Feuer W, Cordahi G: Internal limiting membrane peeling in macular hole surgery. Ophthalmology 2001; 108:1471-1478.
73. Mester V, Kuhn F: Internal limiting membrane removal in the management of full-thickness macular holes. Am J Ophthalmol 2000; 129:769-777.
74. Park DW, Sipperly JO, Sneed SR, et al: Macular hole surgery with internal-limiting membrane peeling and intravitreous air. Ophthalmology 1999; 106:1392-1397.
75. Olsen TW, Sternberg Jr P, Capone Jr A, et al: Macular hole surgery using thrombin-activated fibrinogen and selective removal of the internal limiting membrane. Retina 1998; 18:322-329.
76. Margherio RR, Margherio AR, Williams GA, et al: Effect of perifoveal tissue dissection in the management of acute idiopathic full-thickness macular holes. Arch Ophthalmol 2000; 118:495-498.
77. Sippy BD, Englebrecht NE, Hubbard GB, et al: Indocyanine green effect on cultured human retinal pigment epithelial cells : implications for macular hole surgery. Am J Ophthalmol 2001; 132:433-435.
78. Gandorfer A, Haritoglou C, Kampic A: Retinal damage from indocyanine green in experimental macular surgery. Invest Ophthalmol Vis Sci 2003; 44:316-323.
79. Haritoglou C, Gandorfer A, Gass CA, et al: Indocyanine green-assisted peeling of the internal limiting membrane in macular hole surgery affects visual outcome: a clinicopathologic correlation. Am J Ophthalmol 2002; 134:836-841.
80. Gass CA, Haritoglou C, Schaumberger M, Kampic A: Functional outcomes of macular hole surgery with and without indocyanine green-assisted peeling of the internal limiting membranes. Graefes Arch Clin Exp Ophthalmol 2003; 241:716-720.
81. Da Mata AP, Burk SE, Foster RE, et al: Long-term follow-up of indocyanine green assisted peeling of the retinal internal limiting membrane during vitrectomy surgery for idiopathic macular hole repair. Ophthalmology 2004; 111:2246-2253.
82. Li K, Wong D, Hiscott P, et al: Trypan blue staining of internal limiting membrane and epiretinal membrane during vitrectomy: visual results and histopathological findings. Br J Ophthalmol 2003; 87:216-219.
83. Azad RV, Pal N, Vashisht N, et al: Ef-cacy of 0.15% trypan blue for staining and removal of the internal limiting membrane, epiretinal membranes, and the posterior hyaloid during pars plana vitrectomy. Retina 2005; 25:676.
84. Horio N, Horiguchi M, Yamamoto N: Triamcinolone-assisted internal limiting membrane peeling during idiopathic macular hole surgery. Arch Ophthalmol 2005; 123:96-99.
85. Shah GV, Rosenblatt BJ, Blinder KJ, et al: Triamcinolone-assisted internal membrane peeling. Retina 2005; 25:972-975.
86. Krohn J: Duration of face-down positioning after macular hole surgery; a comparison between 1 week and 3 days. Acta Ophthalmol Scan 2005; 83:289-292.
87. Tornambe PE, Poliner L, Grote K: Macular hole surgery without face-down positioning: a pilot study. Retina 1997; 17:179-185.
88. Lai JC, Stinnett SS, McCuen BW: Comparison of silicone oil versus gas tamponade in the treatment of idiopathic full-thickness macular holes. Ophthalmology 2003; 110:1170-1174.
89. Couvillion SS, Smiddy WE, Flynn Jr HW, et al: Outcomes of surgery for idiopathic macular hole: a case-control study comparing silicone oil with gas tamponade. Ophthalmic Surg Lasers Imaging 2005; 36:365-371.
90. Leonard II RE, Smiddy WE, Flynn Jr HW, Feuer W: Long-term visual outcomes in patients with successful macular hole surgery. Ophthalmology 1997; 104:1648-1652.
91. Cheng L, Azen SP, El-Bradley MH, et al: Duration of vitrectomy and post-operative cataract in the vitrectomy for macular hole study. Am J Ophthalmol 2001; 132:881-887.
92. Thompson JT: The role of patient age and intraocular gas use in cataract progression after vitrectomy for macular holes and epiretinal membranes. Am J Ophthalmol 2004; 137:250-257.
93. Banker AS, Freeman WR, Kim JW, et al: Vision-threatening complications of surgery for full-thickness macular holes. Vitrectomy for macular hole study group. Ophthalmology 1997; 104:1442-1452.
94. Sjaarda RN, Glaser BM, Thompson JT, et al: Distribution of iatrogenic retinal breaks in macular hole surgery. Ophthalmology 1995; 102:1387-1392.
95. Park SS, Marcus DM, Duker JS, et al: Posterior segment complications after vitrectomy for macular hole. Ophthalmology 1995; 102:775-781.
96. Pendergast SD, McCuen II BW: Visual field loss after macular hole surgery. Ophthalmology 1996; 103:1069-1077.
97. Boldt HC, Munden PM, Folk JC, Mehaffey MG: Visual field defects after macular hole surgery. Am J Ophthalmol 1996; 122:371-381.
98. Welch JC: Dehydration injury as a possible cause of visual defect after pars plana vitrectomy for macular hole. Am J Ophthalmol 1997; 124:698-699.
99. Hirata A, Yonemura N, Hasamura T, et al: Effect of infusion pressure on visual field defects after macular hole surgery. Am J Ophthalmol 2000; 130:611-616.
100. Anderson NG, Fineman MS, Brown GC: Incidence of intraocular pressure spike and other adverse events after vitreoretinal surgery. Ophthalmology 2006; 113:42-47.
101. Bansal A, Salmon JF, Malhotra R, et al: Delayed acute angle closure after macular hole surgery. Eye 2003; 17:779-781.
102. Tranos PG, Ghazi-Nouri SMS, Rubin GS, et al: Visual function and subjective perception of visual ability after macular hole surgery. Am J Ophthalmol 2004; 138:995-1002.