Marian Rewers, MD, PhD
H. Peter Chase, MD
 ESSENTIALS OF DIAGNOSIS & TYPICAL FEATURES
ESSENTIALS OF DIAGNOSIS & TYPICAL FEATURES
![]() Polyuria, polydipsia, and weight loss.
Polyuria, polydipsia, and weight loss.
![]() Hyperglycemia and glucosuria often with ketonemia/ketonuria.
Hyperglycemia and glucosuria often with ketonemia/ketonuria.
GENERAL CONSIDERATIONS
Type 1 diabetes (T1D) is the most common type of diabetes mellitus in people younger than 20 years, but can develop at any age and most cases are diagnosed after age 20. The classical presentation includes increased thirst (polydipsia), urination (polyuria), and weight loss; however, the patient may be overweight or even obese. T1D is further divided into T1a (autoimmune) (~95% of the cases) and T1b (idiopathic) diabetes. T1a diabetes is marked by presence of autoantibodies to islet cell autoantigens (insulin, GAD65, IA-2, and ZnT8) and high-risk HLA (human leucocyte antigen) haplotypes (DR4, DQ8, and DR3/DQ2). Insulin production, measured by fasting or stimulated C-peptide levels, is usually low. In the United States, T1D affects an estimated 1.5 million people, including 160,000–200,000 patients younger than age 20 (~25,000 diagnosed annually).
Type 2 diabetes (T2D) is a heterogeneous phenotype diagnosed most often in persons older than age 40 who are usually obese and initially not insulin-dependent. T2D is rare before age 10, but has increased in frequency in older children as a consequence of the epidemic of obesity. The vast majority of the 26 million patients with diabetes in the United States have T2D, but only approximately 16,000 patients are younger than age 20 (~5000 diagnosed annually).
Monogenic forms of diabetes can be diagnosed at any age. They account for less than 1% of childhood diabetes, but form the majority of cases diagnosed before the ninth month of life. Neonatal diabetes is transient in about half of the cases; if persistent, it presents a significant clinical challenge. Some infants respond better to sulfonylurea than insulin. Maturity-onset diabetes of the young (MODY) presents as a nonketotic and usually non–insulin-dependent diabetes in the absence of obesity or islet autoantibodies. A strong family history of early-onset diabetes is common. The most frequent forms are due to mutations in glucokinase or hepatic nuclear factor 1 or 2 genes. Glucokinase mutations rarely require therapy; other forms respond to oral hypoglycemic agents or insulin. Commercial and research-oriented genotyping services are available to aid correct diagnosis.
![]() Pathogenesis
Pathogenesis
A. Type 1 Diabetes
Type 1 diabetes results from autoimmune destruction of the insulin-producing β cells of the pancreatic islets. This destruction occurs over months or years and symptoms do not appear until most of the pancreatic islets have been destroyed.
The incidence is the highest in children of European ancestry, followed by African Americans and Hispanics; the rates are low in Asians and Native Americans.
About 6% of siblings or offspring of persons with T1D also develop diabetes (compared with prevalence in the general population of 0.2%–0.3%). However, fewer than 10% of children newly diagnosed with T1D have a parent or sibling with the disease. More than 90% of children with T1D carry at least one of the two high-risk HLA haplotypes—DR4/DQ8 or DR3/DQ2—and 40% of US children diagnosed before age of 10 years have both (one from each parent), compared with only 2.5% of the general population. Over 30 non-HLA genetic variants have also been implicated.
Since the 1950s, the incidence of T1D has increased dramatically worldwide, doubling approximately every 20 years. Despite much research of early childhood infections and diet, the environmental factor(s) responsible for this epidemic are poorly defined. There is no effective prevention as of 2013; however, screening of high-risk groups for islet autoantibodies and intensive follow-up reduces the severity of the presentation.
B. Type 2 Diabetes
Type 2 diabetes has a strong genetic component, although the inherited defects vary in different families. Obesity, particularly central, and lack of exercise are major causes, but rarely sufficient alone to cause diabetes in youth. Most pediatric patients come from low socioeconomic strata and dysfunctional families; some present with psychiatric disorders. Obesity, T2D, and associated insulin resistance adversely affect cardiovascular health. Acanthosis nigricans, a thickening and darkening of the skin over the posterior neck, armpits, or elbows, is present in many obese children and has occasionally contributed to the diagnosis of T2D.
![]() Prevention
Prevention
A. Type 1 Diabetes
Islet autoantibodies are present for months to years prior to diagnosis in the serum of patients who develop T1a diabetes. Free antibody screening is now available for families having a relative with type 1 diabetes (1-800-425-8361). These antibodies, which do not mediate β-cell destruction, offer a useful screening tool. The β-cell damage is mediated by T lymphocytes. Immunosuppression at different checkpoints of the autoimmune process can slow down the damage, but has no durable effect when stopped. Immunomodulation, including induction of tolerance to islet autoantigens, with or without immunosuppression, is an area of intensive research.
B. Type 2 Diabetes
The Diabetes Prevention Program in adults with impaired glucose tolerance found that 30 minutes of exercise per day (5 d/wk) and a low-fat diet reduced the risk of diabetes by 58%. Taking metformin also reduced the risk of T2D by 31%.
![]() Clinical Findings
Clinical Findings
A combination of polyuria, polydipsia, and weight loss in a child is unique to diabetes. Unfortunately, these symptoms are often missed by primary care providers or even emergency department staff. The frequency of diabetic ketoacidosis (DKA) in US children has not decreased in the past 20 years and is approaching 40%, a sign of poor provider and poor community awareness. More than half of DKA patients were seen by a provider in days preceding diagnosis and obvious symptoms and signs were missed. In contrast, only 10%–20% of newly diagnosed children in Scandinavia or Canada present with DKA. This embarrassing statistic could be greatly improved with better history taking and point-of-care urine analysis. Initial diagnosis can be easily confirmed by blood glucose and ketones measurement using widely available and inexpensive meters.
The clinical presentation of DKA includes abdominal pain, nausea, and vomiting that can mimic an acute abdomen. The patients are mildly to moderately dehydrated (5%–10%), may have Kussmaul respiration, and become progressively somnolent and obtunded. The distribution of diagnosis has shifted to younger age; infants, toddlers, and preschool age children are at particular risk. They often have symptoms of minor infection or gastrointestinal upset. A heavy diaper in a dehydrated child without diarrhea should always flash an alarm. Blood or urine glucose levels could be lifesaving. Blood glucose higher than 200 mg/dL in a child is always abnormal and must be promptly and meticulously followed in consultation with a pediatric endocrinology service. If the presentation is mild and an outpatient diabetes education service is available, hospitalization is usually not necessary.
Transient, “stress-” or steroid-induced hyperglycemia can occur with illness. In a well child, the diagnosis must not be based on a single plasma glucose test or a borderline result obtained using a glucose meter. Our center routinely tests such children for islet autoantibodies to rule out ongoing islet autoimmunity. Absence of the three most available autoantibodies (to insulin, GAD, and IA-2) provides 80% negative predictive value. If HbA1c is normal, we recommend home monitoring of blood glucose for several days. In children progressing to overt diabetes, hyperglycemia after dinner is usually the initial abnormality, which is detectable by self–blood glucose monitoring at home.
In the presence of typical symptoms, a random blood glucose level above 200 mg/dL (11 mmol/L) (confirmed on a CLIA [Clinical Laboratory Improvement Amendments]-certified instrument) is sufficient to make the diagnosis of diabetes. An oral glucose tolerance test is rarely necessary in children. In borderline or asymptomatic cases, a fasting plasma glucose level over 126 mg/dL (7 mmol/L) or a plasma glucose level above 200 mg/dL (11.1 mmol/L) 2 hours after an oral glucose load (1.75 g glucose/kg up to a maximum of 75 g) on 2 separate days confirms the diagnosis. Impaired (not yet diabetic) fasting glucose values are 100–125 mg/dL (5.5–6.9 mmol/L) and impaired 2-hour values are 140–200 mg/dL(7.8–11.1 mmol/L). Children with impaired fasting glucose or impaired glucose tolerance are at high risk of T2D and require careful follow-up and lifestyle modification with weight loss, if obese.
![]() Treatment
Treatment
Major variables in T1D treatment are insulin therapy, diet, exercise, and psychosocial support. All must be addressed to achieve safe and effective metabolic control. At present, the safest recommendation for glycemic control in children is to achieve an HbA1c < 7.5% or the lowest that can be sustained without severe hypoglycemia or frequent moderate hypoglycemia. The HbA1c level reflects the average blood glucose levels over the previous 3 months. Each child should have targets individually determined.
Intensive diabetes management includes: (1) three or more insulin injections per day, or insulin pump therapy based on carbohydrate counting; (2) at least four blood glucose determinations per day; (3) ketone monitoring during hyperglycemia; and (4) frequent contact with a diabetes healthcare provider. The Diabetes Control and Complications Trial (DCCT) showed that this approach improved HbA1c to approximately 7% and significantly reduced the risk for retinal, renal, cardiovascular, and neurologic complications of diabetes.
A. Patient and Family Education
Education about diabetes for all family members is essential for the home management of diabetes. The use of an educational book (see Understanding Diabetes and Understanding Insulin Pumps and Continuous Glucose Monitors) can be very helpful to the family. All caregivers need to learn about diabetes, how to give insulin injections, perform home blood glucose monitoring, and handle acute complications. Although teenagers can be taught to perform many of the tasks of diabetes management, they do better when supportive, not overbearing, parents continue to be involved in management of their disease. Children younger than age 12 years cannot reliably administer insulin without adult supervision because they may lack fine motor control and/or may not understand the importance of accurate dosage.
B. Insulin
Insulin has three key functions: (1) it allows glucose to pass into the cell for oxidative utilization; (2) it decreases the physiologic production of glucose, particularly in the liver; and (3) it turns off lipolysis and ketone production.
1. Treatment of new-onset diabetes—Children presenting in DKA (pH < 7.30 or bicarbonate < 15 mEq/L in presence of hyperglycemia and ketosis/ketonemia) require intravenous insulin in addition to replacement of fluids and electrolytes. Regular insulin is given as a continuous drip at a rate of 0.05–0.1 U/kg/h to achieve drop in blood glucose of approximately 100 mg/dL per hour. Giving an IV insulin bolus of insulin before the completion of the initial fluid bolus has been associated with brain edema. Fast-acting insulin analogs have no advantage over regular insulin when given intravenously.
In children who present without DKA and have adequate oral intake, the initial insulin dose can be administered subcutaneously as 0.2 U/kg of short-acting insulin (regular) or, preferentially, rapid-acting analog: lispro (Humalog), aspart (NovoLog), or glulisine (Apidra). At the same time, 0.2–0.3 U/kg of long-acting insulin analog—glargine (Lantus) or detemir (Levemir)—can be administered subcutaneously to limit the need for multiple insulin injections. This usually suffices for the initial 12–24 hours preceding systematic diabetes education.
The dose is adjusted with each injection during the first week. The rule of thumb is to start insulin at the low end of the estimated daily requirement and titrate it up based on frequent (q2–4h) blood-glucose monitoring. The initial daily dose of insulin is higher in the presence of ketosis, infection, obesity, or steroid treatment. It also varies with age and severity of onset. A total subcutaneous daily dose of 0.3–0.7 U/kg/day may suffice in prepubertal children, while pubertal or overweight children and those with initial HbA1c > 12% commonly require 1.0–1.5 U/kg/day of insulin during the initial week of treatment.
The insulin dose peaks about 1 week after diagnosis and decreases slightly with the waning of glucotoxicity and voracious appetite. Approximately 3–6 weeks after diagnosis, most school-children and adolescents experience a partial remission or “honeymoon period.” Temporary decrease in the insulin dose during this period is necessary to avoid severe hypoglycemia. The remission tends to last longer in older children, but is rarely complete and never permanent. Other types of diabetes should be considered in patients with unusually low insulin requirements.
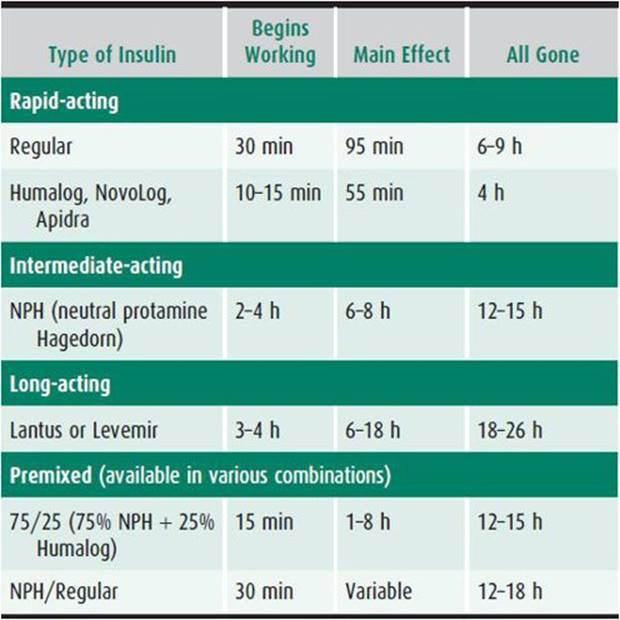
2. Long-term insulin dosage—Children usually receive a rapid-acting insulin to cover food intake or correct high blood glucose and a long-acting insulin to suppress endogenous hepatic glucose production. This is achieved by combining insulins with the desired properties. Understanding the onset, peak, and duration of insulin activity is essential (Table 35–1).
Table 35–1. Kinetics of insulin action.
Nearly all children diagnosed with T1D at our center receive a basal-bolus multiple daily injection (MDI) treatment. This usually consists of 3–4 injections (boluses) of rapid-acting analog before meals and 1–2 injections of long-acting analog insulin. The dose of premeal rapid-acting insulin is calculated based on anticipated carbohydrate content of the meal and additional insulin to correct for high blood glucose, if needed. Sliding scales for dosing of rapid-acting insulin are helpful initially, while families learn carbohydrate counting. This shortcut assumes that the content of carbohydrates does not vary, for example in dinner, from day to day, this may lead to significant under- and overdosing.
Children younger than 4 years usually need 1 or 2 units of rapid-acting insulin to cover carbohydrate intake. Children aged 4–10 years may require up to 4 units of rapid-acting insulin to cover breakfast and dinner, whereas 4–10 units of rapid-acting insulin are used in older children. These estimates do not include correction for high blood glucose.
Families gradually learn to make small weekly adjustments in insulin dosage based on home blood glucose testing. Rapid-acting analog insulin is given 10–20 minutes before eating to account for delay in insulin action. If slower human regular insulin is used, the injections should be given 30–60 minutes before meals—rarely a practical option. In young children who eat unpredictably, it is often necessary to wait until after the meal to decide on the appropriate dose of rapid-acting insulin, which is a compromise between avoiding hypoglycemia and tolerating hyperglycemia after meals.
A long-acting analog insulin glargine (Lantus) or detemir (Levemir) is given once or twice a day to maintain basal insulin levels between meals. Daily adjustments in long-acting insulin dose usually are not needed. However, decreases should be made for heavy activity (eg, sports, hikes, or overnight events).
In the past, most children would receive 2 injections per day of a rapid-acting insulin and an intermediate-acting insulin (NPH), often mixed just before injection. About two-thirds of the total dosage would be given before breakfast and the remainder before dinner. This regiment has been shown to be inferior in achieving recommended HbA1c levels and avoiding hypoglycemia, compared with the basal-bolus regiment described above. Analog insulin (glargine, detemir) works more efficiently than NPH. When changing a patient from NPH insulin to an analog, initially only 50% of the daily units of long-acting insulin is recommended.
3. Insulin pump treatment—Continuous subcutaneous insulin (insulin pump) therapy is the best way to restore the body’s physiologic insulin profile. The pump delivers a variable programmed basal rate that corresponds to the diurnal variation in insulin needs. Prepubertal children require higher basal rate in the early part of night, while postpubertal patients who experience the “dawn phenomenon” require higher rates in the morning. The user initiates bolus doses before meals and to correct hyperglycemia. Most pumps can receive wireless transmission of test results from glucose meters, but the patient or caregiver must still manually enter the amount of carbohydrate being consumed. The pump calculates the amount of insulin needed for a meal or correction based on previously entered parameters which include: insulin-to-carbohydrate ratios, insulin sensitivity factor, glycemic target, and duration of insulin action (set at 3–4 hours to protect from accumulating too much insulin). The user may override the suggestion or press a button to initiate the bolus.
Most clinical trials have demonstrated better HbA1c and less severe hypoglycemia with pump therapy, compared to MDI. Pump therapy can improve the quality of life in children who have trouble with or fear of injections or who desire greater flexibility in their lifestyle; for example, with sleeping in, sports, or irregular eating. Insulin pumps can be particularly helpful in young children or infants who have multiple meals and snacks and require multiple small doses of rapid-acting insulin. The newer generation of insulin pumps can deliver as little as 0.025 U/h, but higher rates using diluted insulin may be needed for uninterrupted flow.
Compliance problems include infrequent blood glucose testing, not reacting to elevated blood glucose, incorrect carbohydrate counting, or missing the boluses altogether. Side effects of insulin pump treatment include failures of insulin delivery because of a displaced or obstructed infusion set. Insulin pump treatment is significantly more expensive than regimens based on injections. For some patients, pumps may be too difficult to operate, or they cannot comply with the multiple testing and carbohydrate counting requirements, or the pump is unacceptable because of body image issues or extreme physical activity (swimming, contact sports). Disposable pumps are already available and much smaller “patch” pumps are in development.
4. “Closed-loop” systems—In the near future, insulin pumps will be directed automatically by a continuous glucose sensor (see section Home Blood Glucose Measurements) with minimal human input. Simple systems are already available that feature, for instance, sensor-initiated automatic suspension of insulin delivery at a predetermined low-glucose level and automatic resumption of the delivery at a safe level. Others, controlling postprandial glycemia are in clinical trials. A number of issues remain to be solved, for example, the accuracy and biocompatibility of the sensors and infusion sets, limitations (lag time) of the systemic versus intraportal administration of insulin, lack of counterbalancing delivery of glucagon, and optimal delivery algorithms for various meals and activities.
5. Treatment of type 2 diabetes—Treatment of type 2 diabetes in children varies with the severity of the disease. If the HbA1c is still near normal, modification of lifestyle (preferably for the entire family) is the first line of therapy. This must include reducing caloric intake and increasing exercise. With mildly elevated HbA1c (6.2%–8.0%) and no ketosis, metformin is usually started at a dose of 500 mg twice daily along with modification of lifestyle. If needed, and if gastrointestinal adaptation has occurred, the dose can be gradually increased to 1 g twice daily. If the presentation is more severe, with ketosis, the initial treatment is similar to that of T1D, including IV or subcutaneous insulin. Of note, 10% of children with T2D present in DKA. Oral hypoglycemic agents may be tried at a later date, particularly if weight loss has been successful.
C. Diet
A thorough dietary history should be obtained including the family’s dietary habits and traditions, the child’s typical meal times, and patterns of food intake. Nutritional management in children with diabetes does not require a restrictive diet, just a healthy dietary regimen that the children and their families can benefit from. Insulin pump and MDI therapy utilize carbohydrate counting in which the grams of carbohydrate to be eaten are counted and a matching dose of insulin is administered. This plan allows for the most freedom and flexibility in food choices, but it requires expert education and commitment and may not be suitable for many families or situations, such as for school lunches and teenagers. Alternatively to a precise carb counting, “exchanges” are taught to estimate 10- or 15-g servings of carbohydrate.
A constant carbohydrate meal plan was used often in the past with insulin regimens based on NPH and regular insulin, where carbohydrate intake and the amount of insulin were kept relatively constant from day to day. This is now perceived as too restrictive and a potential source of conflict that will lead to poor control.
D. Exercise
Regular aerobic exercise is important for children with diabetes. Exercise fosters a sense of well-being; helps increase insulin sensitivity (a drop in glycemia in response to insulin); and helps maintain proper weight, blood pressure, and HDL-cholesterol levels.
Hypoglycemia during exercise or in the 2–12 hours after exercise can be prevented by careful monitoring of blood glucose before, during, and after exercise; reducing the dosage of the insulin active at the time of (or after) the exercise; and by providing extra snacks. Fifteen grams of glucose usually covers about 30 minutes of exercise. The use of drinks containing 5%–10% dextrose, such as Gatorade, during the period of exercise is often beneficial. Insulin dose for meals as well as the basal insulin pump rate should be reduced before, during, and sometimes after the exercise; the longer and more vigorous the activity, the greater the reduction in insulin dose.
E. Psychological Care
The diagnosis of T1D changes lives of the affected families and brings on relentless challenges. It is impossible to take “vacation” from diabetes without some unpleasant consequences. The stress imposed on the family around the time of initial diagnosis may lead to feelings of shock, denial, sadness, anger, fear, and guilt. Meeting with a counselor to express these feelings at the time of diagnosis helps with long-term adaptation. Children with T1D and their parents often experience difficult adjustment. Persisting adjustment problems may indicate underlying dysfunction of the family or psychopathology of the child or caregiver. Young people with T1D are more frequently diagnosed with and treated for psychiatric disorders, disordered eating, neurocognitive, learning problems, and poor coping skills than the general population.
Routine assessment should be made of developmental adjustment to and understanding of diabetes management, including diabetes-related knowledge, insulin adjustment skills, goal setting, problem-solving abilities, regimen adherence, and self-care autonomy and competence. This is especially important during late childhood and prior to adolescence. General and diabetes-related family functioning such as communication, parental involvement and support, and roles and responsibilities for self-care behaviors need to be assessed. Teaching parents effective behavior management skills, especially at diagnosis and prior to adolescence, emphasizes involvement and support, effective problem-solving, self-management skills, and realistic expectations. Adolescents should be encouraged to assume increased responsibility for diabetes management, but with continued, mutually agreed parental involvement and support. The transition to adult diabetes care should be negotiated and planned between adolescents, their parents, and the diabetes team well in advance of the actual transfer.
F. Home Blood Glucose Measurements
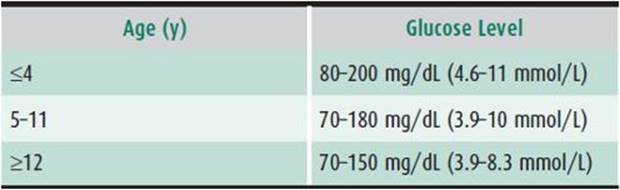
All families must be able to monitor blood glucose levels at least four times daily—and more frequently in patients who have glucose-control problems or intercurrent illnesses. Blood glucose levels can be monitored using any downloadable meter. Target levels when no food has been eaten for 2 or more hours vary according to age (Table 35–2). At least half of the values must be below the upper limit to have a good HbA1c.
Table 35–2. Ideal glucose levels after 2 or more hours of fasting.
The frequency of self-monitoring of blood glucose correlates with improved HbA1c. Patient acceptance may be enhanced by testing on the forearm, in addition to the fingertips; however, that site may be slower to reflect falling blood glucose.
Blood glucose results, insulin dosage, and events, for example, illness, parties, exercise, menses, and episodes of hypoglycemia or ketonuria/ketosis should be recorded in a logbook or downloaded. Regular evaluation by the family helps to see patterns, adjust insulin dosage and, if needed, communicate with healthcare providers. If more than 50% of the values are above the desired range for age or more than 14% below the desired range, the insulin dosage usually needs to be adjusted.
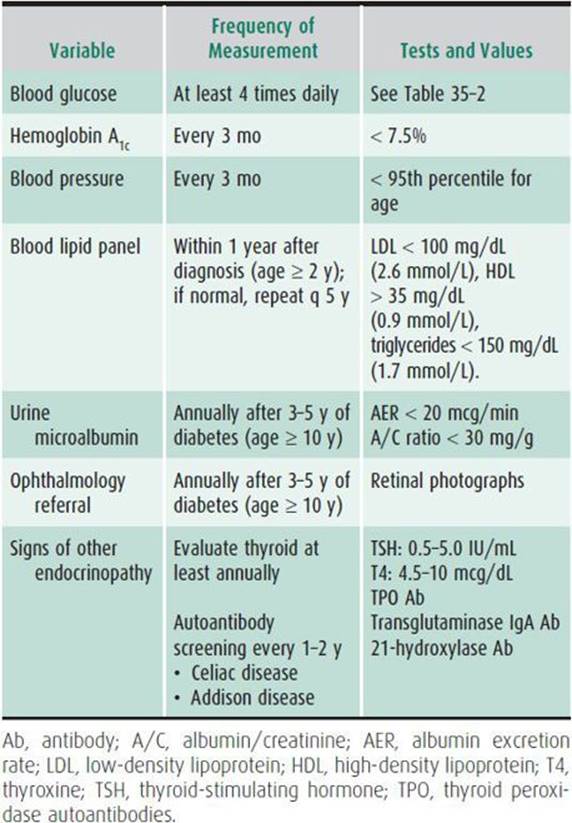
Some families are able to make these changes independently, whereas others need help from the healthcare provider by telephone, fax or email to optimize insulin dose between visits. Children with diabetes should be evaluated by a diabetes provider every 3 months to check compliance, adjust insulin dose according to growth, measure HbA1c, and review blood glucose patterns, as well as for routine review of systems, physical examination, and laboratory tests (Table 35–3).
Table 35–3. Checklist of good diabetes management in children and adolescents.
Home continuous glucose monitoring (CGM) is now routinely available and can tremendously improve diabetes management if used most of the time. Subcutaneous glucose levels are obtained every 1–5 minutes from a sensor placed under the skin. The sensor must be replaced every 7–10 days. The sensor has to be calibrated a couple of times a day using a conventional glucose meter. A transmitter sends glucose levels via radio waves from the sensor to a receiver that can be inside an insulin pump. As with insulin pump therapy, intensive education and follow-up is required, usually at a specialty diabetes center. The user is trained on how to keep the real-time displayed blood glucose “between the lines,” that is, in the personalized range. Low- and high blood glucose alarms can be set and in some systems they may change insulin pump delivery rate. At the time of consultation, data from CGM devices and pumps are routinely downloaded for analysis of patterns. CGM systems produced by DexCom and Medtronic are currently available by prescription in the United States.
G. Prevention of Chronic Complications
1. Maintaining low HbA1c levels—Elevated HbA1c predicts long-term microvascular and macrovascular complications. HbA1c values approximately 7% compared to values approximately 9% result in greater than 50% reductions in the eye, kidney, cardiovascular, and neurologic complications of diabetes. Normal values vary among laboratories but are usually below 6.2%. In diabetes, the desired ranges are less than 7.5% in children and less than 7% in adults. Higher levels may be acceptable in younger children at risk of severe hypoglycemia. Low HbA1c values are generally associated with a greater risk for hypoglycemia.
The HbA1c level reflects the average blood glucose levels over the previous 3 months and should be measured every 3 months. However, in the DCCT study, HbA1c 7% (53 mmol/mol) corresponded to a higher average blood glucose concentration (measured seven times a day) of 192 mg/dL in the conventionally treated patients compared with 163 mg/dL in the intensively treated patients. HbA1c is only one measure of optimal glycemic control, along with preventing hypoglycemia and maximizing quality of life.
The long-term prognosis of children diagnosed with T1D has improved tremendously over the past 20 years, primarily due to better control of blood glucose and blood pressure. While life expectancy is now only 3 years shorter in these patients, compared to the general population, the risk of cardiovascular disease is still four to ten times higher, especially in diabetic women. A checklist of routine tests is presented in Table 35–3.
2. Hypertension—Elevated blood pressure is one of the strongest predictors of both micro- and macrovascular diseases. Treatment of blood pressure is critical in reducing these complications in adults with diabetes and presumably in children and adolescents as well. Blood pressure should be checked and reviewed at each clinic visit. Hypertension is defined as systolic or diastolic blood pressure (measured on at least 3 separate days) above the 95th percentile for the child’s age, sex, and height. Care should be taken to ensure use of the appropriate size cuff in children to avoid inaccurate readings. If elevated blood pressure is confirmed, nondiabetic causes of hypertension should first be excluded. Angiotensin-converting enzyme inhibitors are the first-line agents; if not tolerated well, angiotensin II receptor blockers can be used.
3. Lipid abnormalities—Lipid profiles are generally favorable in children with T1D. The screening for dyslipidemia should commence after the age of 2 years and should be repeated every 5 years thereafter if normal. Good glycemic control should be established in newly diagnosed patients prior to screening, but screening should not be delayed more than 1 year after diagnosis. Children with LDL levels of 130–159 mg/dL (3.4–4.1 mmol/L) should receive dietary and exercise counseling for 6 months, with consideration of pharmacologic therapy if this fails. Statin therapy in addition to diet and lifestyle changes are recommended if LDL is more than 160 mg/dL (4.1 mmol/L). The treatment goals are LDL less than 100 mg/dL (2.6 mmol/L), HDL more than 35 mg/dL (0.9 mmol/L), and triglycerides less than 150 mg/dL (1.7 mmol/L). The use of lipid-lowering drugs in children has been the subject of much discussion. The American Heart Association recommends initiating therapy with statins at the lowest dose at age > 10 years in boys, Tanner stage II or higher, and preferably after menarche in girls.
4. Nephropathy—Microalbuminuria is the first clinical manifestation of diabetic kidney disease and may be reversible with diligent glycemic and blood pressure control. Microalbuminuria is defined as: urinary albumin excretion rate between 20 and 200 μg/min or urinary albumin/creatinine ratio 2.5–25 mg/mmol or 30–300 mg/g (spot urine) in males and 3.5–25 mg/mmol in females. Screening for microalbuminuria with a random spot urine sample should occur annually in children once they are 10 years of age and have had diabetes for more than 3–5 years. If values are abnormal, borderline, or increasing, two timed overnight collections should occur and abnormal results should be repeated. The diagnosis of microalbuminuria requires documentation of two out of three abnormal samples over a period of 3–6 months. Once persistent microalbuminuria is confirmed, nondiabetic-related causes of renal disease should be excluded. Following this evaluation, treatment with an ACE inhibitor should be started, even if the blood pressure is normal. Patients should be counseled about the importance of glycemic control and smoking cessation, if applicable. Patients with T2D should have microalbuminuria assessed soon after diagnosis and then annually.
5. Retinopathy—The first dilated ophthalmologic examination should be obtained by an ophthalmologist or optometrist trained in diabetes-specific retinal examination once the child is ≥ 10 year old and has had diabetes for 3–5 years. The frequency of subsequent examination is generally every 1–2 years, depending on the patient risk profile and advice of the eye care provider. While rare in children, proliferative retinopathy does occur in adolescents with long duration and poor control of diabetes. Laser treatment to coagulate proliferating capillaries prevents bleeding and leakage of blood into the vitreous fluid or behind the retina. This treatment preserves useful vision.
6. Associated autoimmune diseases—Thyroid-stimulating hormone (TSH) level should be measured yearly in all patients. Thyroid peroxidase autoantibody (TPO) is usually the first test to become abnormal in the autoimmune thyroiditis affecting up to 20% of children with T1D. If TPO is positive, we recommend screening with TSH and free T4 every 6–12 months.
Transglutaminase autoantibodies offer a sensitive and specific screening test for celiac disease affecting up to 10% of children with T1D. Risk of celiac disease is most strongly associated with the HLA-DR3/DQ2 haplotype. We recommend routine screening at diagnosis of diabetes and, if negative, retesting every 1–2 year. About half of celiac disease cases develop several years after diagnosis of T1D. Most of the biopsy-confirmed children are “asymptomatic,” but report improved health status upon initiation of gluten-free diet. Untreated celiac disease may lead to severe hypoglycemia, increased bone turnover, and decreased bone mineralization, among many other long-term complications (see Chapter 21).
The 21-hydroxylase autoantibody, a marker of increased risk of Addison disease, is present in approximately 1.3% of patients with type 1 diabetes, although Addison disease develops (usually slowly) in only about one-third of these antibody-positive individuals.
![]() Acute Complications
Acute Complications
A. Hypoglycemia
Hypoglycemia (or insulin reaction) is defined as a blood glucose level below 60 mg/dL (3.3 mmol/L). For preschool children, values below 70 mg/dL (3.9 mmol/L) should be cause for concern. The common symptoms of hypoglycemia are hunger, weakness, shakiness, sweating, drowsiness (at an unusual time), headache, and behavioral changes. In the DCCT study, 10% of patients with standard management and 25% of those with intensive insulin management had one or more severe hypoglycemic reactions each year. Children learn to recognize hypoglycemia at different ages but can often report “feeling funny” as young as age 4–5 years. School personnel, sports coaches, and babysitters must be trained to recognize and treat hypoglycemia. If low blood glucose is not treated immediately with simple sugar, the hypoglycemia may result in loss of consciousness and seizures; brain damage or death can occur with prolonged hypoglycemia.
Consistency in daily routine, correct insulin dosage, regular blood glucose monitoring, controlled snacking, compliance of patients and parents, and good education are all important in preventing severe hypoglycemia. In addition, insulin should not be injected prior to getting into a hot tub, bath, or shower as the heat may cause more rapid insulin uptake. The use of insulin analogs has helped to reduce the occurrence of hypoglycemia.
The treatment of mild hypoglycemia involves giving 4 oz of juice, a sugar-containing soda drink, or milk, and waiting 10 minutes. If the blood glucose level is still below 60 mg/dL (3.3 mmol/L), the liquids are repeated. If the glucose level is above 60 mg/dL, solid foods are given. Moderate hypoglycemia, in which the person is conscious but incoherent, can be treated by squeezing one-half tube of concentrated glucose (eg, Insta-Glucose or cake frosting) between the gums and lips and stroking the throat to encourage swallowing.
Families are advised to have glucagon in the home and in their travel pack to treat severe hypoglycemia by giving subcutaneous or intramuscular injections of 0.3 mL (30 units in an insulin syringe) for children younger than age 5 years; 0.5 mL (50 units) to those older than age 5 years; and 1 mL (100 units) to those heavier than 100 lb. Smaller doses of glucagon (2 units + number of units equal to the age of the child, eg, 2 + 10 = 12 units in a 10-year-old) up to a maximum of 15 units can be used to prevent severe hypoglycemia during nondiabetic illness (gastroenteritis, respiratory infections).
Some patients, usually those who have had diabetes for more than 10 years or those tolerating routinely blood glucose 50–80 mg/dL, fail to recognize the symptoms of low blood glucose (hypoglycemic unawareness). For these individuals, glucose control must be liberalized to prevent severe hypoglycemia and CGM should be considered.
B. Sick Day and Diabetic Ketoacidosis
Families must be educated to check blood or urine ketone levels during any illness (including vomiting even once) or any time a fasting blood glucose level is above 240 mg/dL (13.3 mmol/L), or a randomly measured glucose level is above 300 mg/dL (16.6 mmol/L). If moderate or significant ketonuria is detected, or the blood ketone (β-hydroxybutyrate—using the Precision Xtra meter) is above 1.0 mmol/L, the healthcare provider should be called. Usually 10%–20% of the total daily insulin dosage is given subcutaneously as rapid-acting analog or regular insulin every 3–4 hours until blood glucose normalizes. This prevents ketonuria and ketonemia from progressing to ketoacidosis and allows most patients to receive treatment at home by telephone management. Water is the oral fluid of choice if blood glucose is more than 250 mg/dL; at lower levels of glycemia, one should switch to Gatorade/Poweraid or other glucose-containing beverages.
Mild ketonuria/ketonemia secondary to fasting or acute gastrointestinal upset and associated with normal or low blood glucose does not require supplemental insulin treatment. Of note, the brain uses β-hydroxybutyrate as the alternate fuel to glucose in the setting of hypoglycemia. Overtreatment with insulin during a sick day that begins with hyperglycemia and ketosis may lead to loss of consciousness and/or seizures due to severe hypoglycemia.
Acidosis (venous blood pH < 7.30 or bicarbonate <15 mEq/L) is unfortunately still a frequent acute complication in patients with established T1D. Acidosis may occur in those who miss insulin injections, do not check blood or urine ketone levels, or fail to seek help when ketones are elevated. Repeated episodes of ketoacidosis signify that counseling may be indicated, and that a responsible adult must take over the diabetes management. If for any reason this is not possible, a change in the child’s living situation may be necessary.
Treatment of DKA is based on four physiologic principles: (1) restoration of fluid volume; (2) intravenous insulin to inhibit lipolysis and return to glucose utilization; (3) replacement of electrolytes; and (4) correction of acidosis. Mild DKA is defined as a venous blood pH of 7.2–7.3; moderate DKA, a pH of 7.10–7.19; and severe DKA, a pH below 7.10. Patients with severe DKA should be hospitalized in a pediatric intensive care unit, if available. Laboratory tests at the start of treatment should include venous blood pH, glucose, and an electrolyte panel. More severe cases may benefit from determination of blood osmolality, calcium, phosphorus, and urea nitrogen levels. Severe and moderate episodes of DKA generally require hourly determinations of serum glucose, electrolytes, and venous pH levels, whereas these parameters can be measured every 2 hours if the pH level is 7.20–7.30.
1. Restoration of Fluid Volume—Dehydration is judged by estimated loss of body weight, dryness of oral mucous membranes, low blood pressure, and tachycardia. Initial treatment is with normal saline (0.9%), 10–20 mL/kg during the first hour (can be repeated in severely dehydrated patients during the second hour). The total volume of fluid in the first 4 hours of treatment should not exceed 20–40 mL/kg because of the danger of cerebral edema. After initial expansion, 0.45%–0.9% saline is given at 1.5 times maintenance to replace losses over 24–36 hours. When blood glucose level falls below 250 mg/dL (13.9 mmol/L), 5% dextrose is added to the intravenous fluids. If blood glucose level falls below 120 mg/dL (6.6 mmol/L), 10% dextrose can be added.
2. Inhibition of Lipolysis and Return to Glucose Utilization— Insulin turns off fat breakdown and ketone formation. Regular insulin is given intravenously at a rate of 0.05–0.1 U/kg/h. The insulin solution should be administered by pump and can be made by diluting 30 units of regular insulin in 150 mL of 0.9% saline (1 U/5 mL). If necessary, the insulin dosage can be reduced, but it should not be discontinued before the venous blood pH reaches 7.30 and there is sufficient level of insulin from subcutaneous injections. The half-life of intravenous insulin is 6 minutes, whereas subcutaneous rapid-acting analog insulins take 10–15 minutes, and regular insulin takes 30–60 minutes, to begin activity. We recommend continuing intravenous insulin for at least 30 minutes after the initial subcutaneous insulin injection.
3. Replacement of Electrolytes—In patients with DKA, both sodium and potassium pass into the urine and are depleted. In addition, serum sodium concentrations may be falsely lowered by hyperglycemia, causing water to be drawn into the intravenous space, and by hyperlipidemia if fat replaces some of the water in the serum used for electrolyte analysis. Sodium is usually replaced adequately by the use of 0.45%–0.9% saline in the rehydration fluids.
Serum potassium levels may be elevated initially because of inability of potassium to stay in the cell in the presence of acidosis (even though total body potassium is low). Potassium should not be given until the serum potassium level is known to be < 5.0 mEq/L and urine output is confirmed. It is then usually given in replacement fluid at a concentration of 40 mEq/L, with half of the potassium (20 mEq/L) either as potassium acetate or potassium chloride and the other half as potassium phosphate (20 mEq/L). Hypocalcemia can occur if all of the potassium is given as the phosphate salt; hypophosphatemia occurs if none of the potassium is of the phosphate salt.
4. Correction of Acidosis—Acidosis corrects spontaneously as the fluid volume is restored and insulin facilitates aerobic glycolysis and inhibits ketogenesis. Bicarbonate is generally not recommended.
5. Management of Cerebral Edema—Some degree of cerebral edema has been shown by computed tomography scan to occur commonly in DKA. Associated clinical symptoms are rare, unpredictable, and may be associated with demise. Cerebral edema may be related to the degree of dehydration, cerebral hypoperfusion, acidosis, and hyperventilation at the time of presentation. In general, it is recommended that no more than 40 mL/kg of fluids be given in the first 4 hours of treatment and that subsequent fluid replacement not exceed 1.5 times maintenance. Cerebral edema is more common when the serum sodium is noted to be falling rather than rising. Early neurologic signs may include headache, excessive drowsiness, and dilated pupils. Prompt initiation of therapy should include elevation of the head of the bed, mannitol (1 g/kg over 30 minutes), and fluid restriction. If the cerebral edema is not recognized and treated early, over 50% of patients will die or have permanent brain damage.
In summary, modern diabetes care can lead to excellent health outcomes. Tremendous progress in biotechnology (insulin analogs), insulin pumps, and continuous glucose sensing has made the prevention of acute and long-term complications achievable. However, comprehensive and continuing education of patients and their families remains the foundation of healthy and quality life with diabetes.
REFERENCES
American Diabetes Association: Clinical practice recommendations. Diabetes Care 2013;32(Suppl 1).
CGM devices approved by the FDA. www.fda.gov/MedicalDevices/default.htm or call 1-888-INFO-FDA (463-6332).
Chan C, Rewers M: Diabetes in childhood. In Holt RIG, Cockram C, Flyvbjerg A, Goldstein BJ (eds): Textbook of Diabetes, 4th ed. Wiley-Blackwell; 2010:859–874.
Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Research Group: Modern-day clinical course of type 1 diabetes mellitus after 30 years’ duration. Arch Intern Med 2009;169:1307 [PMID: 19636033].
Eisenbarth GS (ed): Type 1 Diabetes: Cellular, Molecular, & Clinical Immunology. http://www.barbaradaviscenter.org.
ISPAD: Clinical Practice Consensus Guidelines 2009 Compendium. Pediatric Diabetes 2009;10(Suppl 12):1–210 [PMID: 19754612].
Monogenic Forms of Diabetes: Neonatal Diabetes Mellitus and Maturity-onset Diabetes of the Young. http://diabetes.niddk.nih.gov/pubs/mody.
Rewers M, Gottlieb P: Immunotherapy for the prevention and treatment of type 1 diabetes: human trials and a look into the future. Diabetes Care 2009;32:1769–1782 [PMID: 19794002].
Understanding Diabetes and Understanding Insulin Pumps and Continuous Glucose Monitors by H. Peter Chase. http://www.barbaradaviscenter.org.