CASE 79: A 17-YEAR-OLD WITH KNEE PAIN![]()
A 17-year-old female high school soccer player is brought to a pediatric emergency department with a chief complaint of left knee pain. The onset of symptoms occurred during a soccer game the previous day. The athlete states that as she went to kick the ball with her right foot, she planted her left foot, felt her left knee buckle, and heard a “pop.” She then fell to the ground and had to be helped off the field. She experienced immediate swelling in the knee as well as some difficulty straightening the knee. She denied any tingling or numbness in the leg. She is using crutches because walking is painful. She denies any history of previous knee injuries and has played soccer for 7 years.
SELECT THE ONE BEST ANSWER
1. The best initial management for this athlete on the soccer field should include
(A) ice applied to the knee joint for approximately 20 minutes
(B) application of a knee immobilizer after attempting to straighten the leg to full extension
(C) ambulation on the sidelines to improve the range of motion and decrease the swelling
(D) an immediate dose of oral (PO) ibuprofen 600-800 mg to prevent inflammation
(E) immediate transport by ambulance to the nearest emergency department for evaluation
2. Based on the history alone, the most likely diagnosis of this girl’s injury is
(A) meniscal tear
(B) medial collateral ligament (MCL) tear
(C) anterior cruciate ligament (ACL) tear
(D) distal femur fracture
(E) patellar dislocation
3. On physical examination, a moderate knee joint effusion and a 5-degree flexion contracture are noted. Valgus and varus testing performed at 30 degrees of knee flexion reveal no instability. An anterior drawer test performed with the knee at 90 degrees of flexion reveals increased laxity. A posterior drawer test is negative. McMurray test is negative. There is no pain with patellar compression, nor is patellar instability noted. Based on the physical examination just described, which of the following tests performed is most helpful in confirming your suspected diagnosis?
(A) valgus test
(B) varus test
(C) anterior drawer test at 90 degrees of flexion
(D) Lachman test at 30 degrees of flexion
(E) McMurray test
4. You tell the patient that the swelling in her knee indicates inflammation is present. Which of the following statements is most accurate regarding inflammation?
(A) inflammation is primarily an acute response to trauma, infection, and autoimmune diseases
(B) nonsteroidal anti-inflammatory drugs (NSAIDs) work on joint inflammation by inhibiting prostaglandin synthesis in the arachidonic acid cascade at the cyclo-oxygenase pathway
(C) corticosteroids work most effectively on joint inflammation by inhibiting leukotriene production
(D) inflammation is characterized by erythema, edema, warmth, and pain and has a protective effect on synovium, tendons, bursae, and cartilage
(E) none of the above
5. The patient now tells you she is in pain after you have examined her and asks what she should do. Your next step in treatment should be which of the following?
(A) apply an ACE wrap
(B) knee joint aspiration
(C) corticosteroid injection
(D) knee joint aspiration followed by a corticosteroid injection
(E) knee brace
6. You speak with the orthopedic surgeon regarding follow-up as an outpatient. What radiographic study will best aid her in follow-up management?
(A) anteroposterior (AP) and lateral plain radiograph
(B) AP, lateral, sunrise, and notch plain radiographs
(C) computed tomography (CT) scan
(D) magnetic resonance imaging (MRI) scan
(E) no imaging study is needed
7. Which of the following treatment recommendations is likely to result in complete recovery from the above injury including eventual return to soccer?
(A) custom hinged knee brace for 3-6 months
(B) 6-12 weeks of physical therapy in a sports rehabilitation center
(C) arthroscopic surgery and repair
(D) arthroscopic surgery and reconstruction
(E) complete rest and crutch-assisted ambulation for 6-12 weeks
8. The same patient returns to the emergency department 2 weeks later. She is now complaining of severe sharp stabbing sensations of pain when she attempts to straighten her leg completely. Your physical examination reveals a 10-degree flexion contracture, a small joint effusion, and medial joint line tenderness. Attempts to straighten the knee into neutral (full extension at 0 degrees) reproduce the sharp pain. Laxity is again noted with a Lachman test. McMurray testing reveals a painful “click.” You are now most concerned about the following diagnosis
(A) ACL injury
(B) MCL injury
(C) meniscal injury
(D) A and C
(E) A, B, and C
9. The patient now tells you she has been unable to go for an MRI because of her insurance and lack of transportation; however, she is planning to go in 10 days. She asks what you want her to do in the meantime. The most appropriate recommendation to make at this point is
(A) continue the brace and follow up after the MRI
(B) continue the brace and physical therapy and follow up after the MRI
(C) resume crutch use, stop physical therapy, and await the MRI
(D) referral to an orthopedic surgeon after the MRI
(E) referral to an orthopedic surgeon within 1 week, regardless of the MRI being done
10. An 11-year-old boy presents to the pediatric emergency department complaining of pain in his right knee. He has played soccer everyday for the past 4 months on a traveling soccer team. He has noted that the pain has worsened over the past week. You are concerned about
(A) osteochondritis dissecans
(B) physeal injury
(C) meniscal tear
(D) cruciate ligament injury
(E) tibial tubercle avulsion
11. A 12-year-old girl comes to the emergency department after falling while playing basketball. Her knee is painful and swollen and she is unable to bear weight. Which study below would be the least helpful in initial diagnosis of a physeal injury?
(A) plain radiographs including AP, lateral, notch, and sunrise view
(B) CT scan
(C) MRI scan
(D) bone scan
(E) all are equally sensitive and specific to clarify the cause of a physeal injury
12. Which of the following conditions is the least common cause of knee pain in adolescent females?
(A) patellar dislocation
(B) osteochondritis dissecans
(C) patellofemoral pain
(D) ACL injury
(E) meniscal injury
13. An 11-year-old boy presents to the emergency department complaining of 4 weeks of localized pain below the knee. On examination the child is noted to have proximal tibial tuberosity tenderness. What is this child’s most likely diagnosis?
(A) patellofemoral pain
(B) Osgood-Schlatter disease
(C) plica band syndrome
(D) chronic MCL sprain
(E) iliotibial band syndrome
14. Which of the following physical examination findings is not associated with an increased risk of patellofemoral pain?
(A) genu valgum
(B) pes planovalgus foot deformity
(C) Q angle of 15 degrees
(D) weak quadriceps muscles
(E) patellar hypermobility
15. Which of the following activities is least associated with increased stress on the patellofemoral joint?
(A) jumping
(B) squatting
(C) prolonged sitting
(D) stair climbing
(E) straight leg raises
16. A 15-year-old obese boy presents to the pediatric emergency department complaining of right hip pain during ambulation for 1 week. He denies trauma. On examination, he is noted to have a shortened right leg that is externally rotated and adducted. Before getting X-rays on her child, the mother wants to know her child’s most likely diagnosis
(A) femur fracture
(B) Legg-Calvé-Perthes disease
(C) toxic synovitis
(D) slipped capital femoral epiphysis
(E) congenital hip dislocation
17. A 7-year-old is brought to the emergency department for a limp of 1 month duration and right hip pain. The mother states that the child fell off his bike 2 months ago. He had an evaluation at the time of the initial injury including X-rays of his hips that were normal. On examination, the child has a limited range of motion of the right hip due to pain at the joint. What do you expect to see when you repeat the hip radiographs?
(A) distal femur fracture
(B) femoral head fracture
(C) dislocation of the femoral head
(D) displacement of the epiphysis downward and posterior
(E) widened joint space between the femoral head and the acetabulum
ANSWERS
1. (A) The best initial treatment for an injured knee is ice applied to the swollen and painful area for approximately 20 minutes. It is appropriate to follow the general RICE (rest, ice, compression, elevation) principles for acute injury treatment. However, in the provided choices for an acute knee injury, one should not attempt to “force” the knee into extension because there may be mechanical limitations, such as torn tissue or extreme swelling that prevent the knee from reaching full extension. The knee joint has maximal space to accommodate swelling at approximately 30 degrees of flexion. Weight bearing should be as tolerated and, in this setting, keeping the athlete non-weight-bearing until a full examination is performed is appropriate. Although immediate use of ibuprofen or another NSAID may be helpful for pain, it is unlikely to have any immediate effect on the posttraumatic inflammatory response. Urgent treatment is prudent in the setting of sports-related knee injuries. In the absence of gross deformity or neurovascular compromise, emergent transport is unnecessary.
2. (C) A noncontact deceleration injury to the knee joint resulting in a painful “pop,” immediate swelling, and an inability to fully bear weight following the injury is an ACL tear approximately 85% of the time in a skeletally mature patient.
3. (D) The maneuver most helpful to confirm your diagnosis is the Lachman test performed at 30 degrees of flexion. The Lachman test is performed by using one hand to stabilize the femur while the examiner’s opposite hand is placed around the leg at the level of the tibial tubercle and an attempt is made to anteriorly translocate the tibia forward. The Lachman test is more clinically sensitive at diagnosing ACL tears than an anterior drawer test performed at 90 degrees of knee flexion (see Figure 79-1). In that instance, it is more common to find patients guarding or reflexively tightening their hamstring muscles; this results in a false-negative drawer test with decreased anterior translation. The McMurray test is performed with the patient lying supine. The examiner places one hand anteriorly on the joint lines and then proceeds to cup the heel with the opposite hand and begins to flex and extend the knee while simultaneously internally and externally rotating the tibia on the femur. The test is positive, indicating a torn meniscus, if a painful click is felt.

FIGURE 79-1. Anterior drawer test. (Reproduced, with permission, from Imboden J, Hellmann DB, Stone JH. Current Rheumatology Diagnosis & Treatment, 2nd ed. New York: McGraw-Hill; Fig. 12-3.)
4. (B) Inflammation is both an acute and chronic response to trauma, infection, and systemic autoimmune disease. In the acute phase, inflammation may be a healthy, self-limiting response; however, in the chronic phase it is often destructive, such as in the setting of arthritis and articular cartilage destruction. Corticosteroids affect inflammation by inhibiting leukotriene production but also by inhibiting prostaglandin synthesis via the phospholipase A2 pathway.
5. (E) In the setting of traumatic knee injuries there is no role for acute corticosteroid injections and no significant therapeutic role for knee joint aspiration. If a joint aspiration is performed, the hemarthrosis tends to reaccumulate quickly, thus limiting the effectiveness of the therapeutic aspiration. An ACE wrap is a relatively ineffective way to provide support and compression if a more supportive knee brace is available. Knee immobilizers that do not allow for motion of the joint are acceptable alternatives initially, but their use should be limited to a few days, and active range of motion should be encouraged within the limits of pain.
6. (D) Although plain radiographs of the knee are an appropriate initial study, a noninfused MRI of the left knee is helpful in diagnosing ligamentous injuries of the knee, as well as diagnosing other associated intra-articular injuries, such as meniscal tears. Some might argue that no imaging study is needed in the case described because the diagnosis is clinically apparent; however MRIs are helpful to look for associated injuries such as collateral ligament, meniscal, and articular cartilage injuries. MRIs are generally recommended as part of the evaluation for an internal derangement of the knee. An MRI can be done as an outpatient in preparation for orthopedic follow-up care.
7. (D) ACL injuries usually result in complete ligament tears either midsubstance or from the proximal attachment on the posterior femur. The injured ligament usually retracts and loses proper anatomic positioning, thereby preventing any reasonable chance of healing with conservative management. Although bracing and physical therapy are important adjunctive treatments to decrease pain and improve strength and function, both pre- and post-surgery, the definitive treatment is an ACL reconstruction using a graft. Attempts to repair torn ACLs surgically have resulted in high failure rates and complications; therefore, in general, a surgical reconstruction is the preferred treatment of choice.
8. (D) Given the above information, your examination suggests ACL and meniscus injury resulting in signs of internal derangement. Bucket handle meniscal tears are most likely to result in a mechanical block in knee joint range of motion (see Figure 79-2). An MCL injury should be associated with pain to palpation over this extra-articular structure and increased laxity with valgus testing.
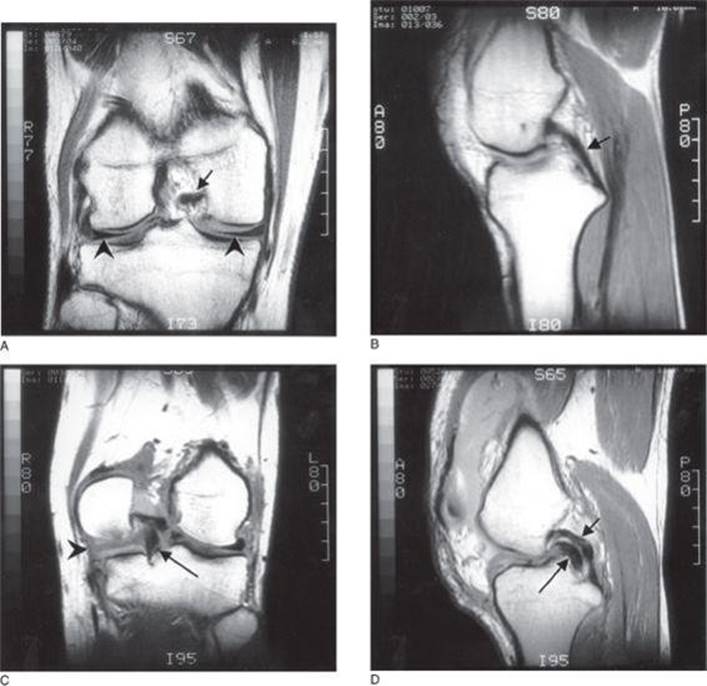
FIGURE 79-2. Bucket-handle meniscal tear. A. Normal medial and lateral menisci and B. normal posterior cruciate ligament in the intercondylar notch as demonstrated on magnetic resonance proton-density (partial T2 weighting) coronal and sagittal images. The menisci are the dark triangular structures in A marked with arrowheads. The normal posterior cruciate ligament is shown as a small black arrow in A and B. C. Proton-density coronal scan showing a large complex tear involving the posterior horn of the medial meniscus (black arrowhead) with most of the fragment displaced into the intercondylar notch (the “bucket-handle,” long black arrow) inferior to the normal posterior cruciate ligament. D. Sagittal proton-density image showing the meniscal fragment (long black arrow) displaced under the posterior cruciate ligament (short black arrow) and having a similar appearance (“double PCL sign”). Not shown is the “bucket” part of the meniscus, which stays attached to the medial tibia. (Reproduced, with permission, from Tintinalli, JE, Kelen GD, Stapczynski JS. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 6th ed. New York: McGraw-Hill; 2004: Fig. 305-3A-D.)
9. (E) A flexion contracture as a sign of internal derangement of the knee at 10-14 days postinjury is an indication for an immediate surgical evaluation. Mechanical blocks of the joint are associated with higher complication rates such as permanent loss of normal range of motion and damage to articular cartilage from pinching and compression with knee joint movement. Therefore, although it would be helpful to expedite the MRI, if that seems unlikely to happen, it is appropriate to refer for an orthopedic consultation 10-21 days postinjury in the setting of a presumed mechanical block. The surgeon may recommend immediate arthroscopy to address the “locked” knee.
10. (A) Osteochondritis dissecans injuries are much more common in the skeletally immature athlete; however, they are more frequently associated with overuse (see Figure 79-3). Boys in the second decade of life are most affected. The etiology is multifactorial and thought to result from cumulative microtrauma to the subchondral bone leading to stress fracture and, ultimately, collapse. The child often presents with mild to moderate chronic pain that is associated with activity. Treatment of this lesion depends on whether the cartilage is intact, partially attached, or completely detached.
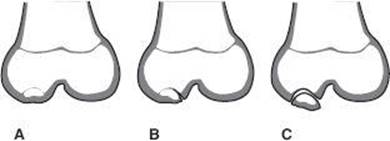
FIGURE 79-3. Various forms of the osteochondritis dissecans lesion found in children. A. Defect in ossification center without cartilage defect. B. Lesion with a hinged flap. C. Complete separation of bone and cartilage, which can lead to loose body in the knee joint. (Reproduced, with permission, from Skinner HB. Current Diagnosis & Treatment in Orthopedics, 4th ed. New York: McGraw-Hill; 2006: Fig. 11-27.)
11. (A) It is reasonable to assume that a 12-year-old girl is not yet skeletally mature. Therefore, the highest risk of injury associated with knee trauma is a physeal injury to the distal femur or proximal tibia. Physeal, or growth plate injuries are best treated with casting and crutches and merit a referral to a pediatric orthopedist because there is increased risk of growth arrest. Tibial tubercle avulsion injuries can best be diagnosed on a lateral radiograph of the knee and also merit an orthopedic evaluation. ACL injuries do occur in skeletally immature athletes. The management of ACL injuries at this age is controversial. In the setting of physeal injuries, a number of nondisplaced Salter-Harris 1-2 fractures can be difficult to see on plain radiographs. Often a follow-up radiograph obtained 24-48 hours postinjury or 10-14 days postinjury will demonstrate the fracture line or a periosteal reaction. MRI, CT, and bone scan are all sensitive and specific for identifying physeal fractures. Clinically, pain at the end of long bones is a physeal injury until proven otherwise.
12. (B) Osteochondritis dissecans lesions are most common in boys 9-18 years old. Patellofemoral pain and patellar dislocations are associated with underlying patellar instability and malalignment, a clinical finding more common in females. Females tend to have valgus knee alignment that is often associated with flat feet. These cause overpronation and abnormal patellar tracking on the femur. Females often have “looser” ligaments and relatively weaker supporting muscles such as the quadriceps and hamstring muscles. ACL injuries are more common in females because of the above factors and the frequent presence of a smaller bony notch on the femur for the ligament to pass through. Hormonal influences are also thought to play a role in increasing a female’s risk of ACL injury.
13. (B) Osgood-Schlatter disease is inflammation and pain at the tibial tubercle seen in growing prepubescents (see Figure 79-4). It results from repetitive microscopic injuries that produce inflammation of the apophysis of the tibial tuberosity and partial avulsion of the tibial tubercle. Patellofemoral pain syndrome is the most common cause of adolescent knee pain, particularly in females. It is often referred to as anterior knee pain. There are many contributing factors (see next question). Plica syndrome is a painful band of synovial tissue that snaps on the undersurface of the patella causing pain. Iliotibial band syndrome is tendonitis causing lateral knee pain—most common in runners.

FIGURE 79-4. Osgood-Schlatter disease. The radiographs would show characteristic fragmentation of the tibial tubercle apophysis, similar to that shown in the diagram. (Reproduced, with permission, from Skinner HB. Current Diagnosis & Treatment in Orthopedics, 4th ed. New York: McGraw-Hill; 2006: Fig. 11-29.)
14. (C) Anterior or patellofemoral pain is associated with a variety of physical findings including flat feet, knock knees (valgus knees), and increased internal hip rotation (femoral anteversion). Obesity also contributes to the presence of anterior knee pain. Functionally, weak quadriceps muscles, tight hamstrings, and patellar instability contribute to the development of patellofemoral pain. The Q angle refers to the relationship of the quadriceps and patella vectors. One line is drawn from the anterior superior iliac spine and bisects the mid-superior pole of the patella. A second line is drawn from the mid-patella to the mid-patellar tendon. An angle more than 20 degrees is associated with lateral patellar tracking and increased stress on the patellofemoral joint.
15. (E) Patellofemoral pain has often been referred to as “theater knee” because weight-bearing activities and prolonged sitting tend to increase anterior knee pain. Sitting with the knee extended or performing exercises with a straight leg do not require stress to be placed across the patellofemoral joint, therefore usually do not hurt, and are often used as early exercises to start strengthening the leg without aggravating the patella and its surrounding structures.
16. (D) Obese and rapidly growing adolescent boys are at highest risk for slipped capital femoral epiphysis (SCFE). There is often no associated trauma. Symptoms are often gradual but can be acute in onset. Pain is noted as well as limited range of motion. The typical “ice cream falling off the cone” is noted on AP and frog leg films of the hip. An irregular widening of the epiphyseal line is seen and the epiphysis is displaced downward and posterior. Emergent referral to an orthopedic surgeon is needed.
17. (E) The most likely diagnosis for this child is Legg-Calvé-Perthes disease, an avascular necrosis of the femoral head. This is most commonly seen in elementary school age children, more often boys. Often an injury precedes the symptoms and the initial radiographs are normal.
![]()
SUGGESTED READING![]()
Bernstein J. Musculoskeletal Medicine. Rosemont, IL: AAOS Publications; 2003.
Fleisher GR. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott; 2010.
Harris SS, Anderson SJ. Care of the Young Athlete. 2nd ed. Rosemont, IL: AAOS and AAP Publications; 2009.
CASE 80: A 15-YEAR-OLD AND A 17-YEAR-OLD WHO COLLAPSE DURING A MARATHON![]()
You are working in the emergency department on a Saturday afternoon watching the local marathon race on television. The announcer has just stated that the outside temperature is 95°F (35°C) and the humidity is 80%.
A 15-year-old female marathon runner is brought into the emergency department complaining of spasms in her calf muscles, mild lower abdominal pain, and thirst. She states she is competing in her first marathon, softball is her usual sport, and she didn’t train much for this race. She did drink some water every 3 miles at the fluid stations then collapsed at mile 16. Her weight is 85 kg. Her vital signs are: pulse 96 bpm, blood pressure (BP) 110/70 mm Hg, respiratory rate 28, temperature 99.9°F (37.7°C). She is wearing a tight-fitting, dark long-sleeve shirt over a tank top and matching shorts. Upon removal of her garments she was noted to have sunburned skin without blistering on her face, back, chest, and upper and lower extremities. She appears profusely sweaty and has tight gastrocnemius muscles with spasms.
SELECT THE ONE BEST ANSWER
1. Which diagnosis most likely explains this athlete’s symptoms?
(A) sunburn
(B) dehydration
(C) heat exhaustion
(D) heat cramps
(E) heat stroke
2. Which of these factors contributed the most to this girl’s illness?
(A) obesity
(B) dehydration
(C) clothing
(D) sunburn
(E) excessive exercise
3. What is the best initial treatment for this 15-year-old?
(A) intravenous (IV) fluid replacement with normal saline
(B) salt tablets
(C) unlimited oral intake of a standard electrolyte solution
(D) unlimited oral intake of water
(E) massage and gentle calf stretching
4. After 2 hours, the girl feels much better and is ready to go home. You advise her that in the future she should try to prevent heat cramps during competition in strenuous and endurance sports lasting longer than 1 hour. Which of the following recommendations is most effective in the prevention of heat cramps?
(A) salt tablets
(B) water only before and during intense endurance exercise
(C) water and an electrolyte drink before and during intense exercise
(D) increased warm-up time and stretching of calf muscles before exercise
(E) weight loss
5. A second marathon runner is brought in by ambulance. He is a 17-year-old male cross-country runner who collapsed at mile 23 complaining of dizziness, lightheadedness, headache, nausea. He had vomited twice in the field. His weight is 80 kg. His vital signs are BP 100/60 mm Hg, pulse 110 bpm, respiratory rate 36, tympanic temperature 101°F (38.5°C). On examination he appears confused and disoriented, and his skin is sweaty and hot to the touch. Further examination is unremarkable.
Based on the initial presentation, what is the most likely diagnosis accounting for the second athlete’s symptoms?
(A) dehydration
(B) heat stroke
(C) heat exhaustion
(D) heat syncope
(E) rhabdomyolysis
6. You are called to the bedside of the 17-year-old male runner and you observe generalized tonicclonic seizure activity and posturing. The patient feels hot and dry to the touch. You are concerned now that the second athlete is suffering from heat stroke. Which of the following would be least likely to be found in a patient with heat stroke?
(A) a temperature of 101°F (38.5°C)
(B) an increased creatine phosphokinase level
(C) urine specific gravity higher than 1.030
(D) lactic acidosis
(E) BP of 100/60 mm Hg
7. The nurse reports to you that the current vital signs for the boy are as follows: BP 90/50 mm Hg, pulse 120, oxygen saturation 95% on room air, temperature 106.7°F (41.5°C). What is the most important initial emergency department treatment for the athlete in Question 6?
(A) prepare the patient for emergent placement of a Swan-Ganz catheter for central venous pressure monitoring
(B) begin rapid cooling procedures
(C) administer supplemental oxygen
(D) administer room temperature IV fluids using a 1L bolus of 0.9% normal saline over 30-60 minutes
(E) administer an antipyretic medication emergently
8. The most practical initial method to achieve rapid cooling is which of the following?
(A) whole body immersion in ice water
(B) wrapping the body in cold towels
(C) packing the body in ice
(D) spraying with water and place in front of fans
(E) ice packs in the groin and axilla
9. You have now initiated rapid cooling and the patient is more lucid, the skin is feeling cooler and clammy to the touch. At what temperature do you want to stop rapid cooling?
(A) 37°C (98.6°F)
(B) 37.3°C (99°F)
(C) 37.7°C (100°F)
(D) 38.3°C (101°F)
(E) 39.6°C (103°F)
10. Which of the following is the most serious form of heat illness?
(A) fever
(B) heat syncope
(C) heat stroke
(D) heat exhaustion
(E) rhabdomyolysis
11. What environmental conditions predispose an athlete to heat illness?
(A) high ambient temperature
(B) high winds
(C) high humidity
(D) A and C
(E) A, B, and C
12. What is the most important mechanism the body uses for heat dissipation?
(A) conduction
(B) convection
(C) radiation
(D) evaporation
(E) respiration
13. Which of the following statements regarding heat dissipation is false?
(A) conduction occurs via indirect contact of the body with the environment
(B) convection is heat transferred from a solid surface to surrounding gas molecules
(C) radiation is the transfer of heat between the body and its environment via electromagnetic waves
(D) evaporation is the conversion of liquid to gas
(E) all of the above are true
14. Heat cramps are most likely related to the loss of which electrolyte?
(A) Mg++
(B) Na+
(C) K+
(D) Cl−
(E) Ca++
15. When caring for a preadolescent athlete, all of the following statements accurately describe heat illness except
(A) children are at increased risk for heat illness because of a higher surface area to mass ratio
(B) younger athletes have slower rates of acclimatization
(C) children are at decreased risk for heat illness because the circulating blood volume is less
(D) children are less efficient at sweating
(E) children’s motor movements are less efficient than those of adults during exercise
16. Which of the following statements is true regarding heat exhaustion and heat stroke?
(A) heat exhaustion and heat stroke are separate clinical conditions that do not occur in the same patient suffering from heat illness
(B) hemoconcentration, urinary concentration, and hypertension are common occurrences in both conditions
(C) both conditions can result in hyperpyrexia at 105°F (40.5°C) or higher
(D) both conditions may cause an athlete to experience weakness, fatigue, dizziness, disorientation, myalgias, tachycardia, nausea, vomiting, or hypotension
(E) both conditions result in reversible tissue damage if an accurate diagnosis and prompt initiation of treatment occurs
17. Which of the following are complications of heat stroke?
(A) permanent neurologic deficits
(B) hepatic failure
(C) uremia
(D) disseminated intravascular coagulation
(E) all of the above
18. Which of the following statements is true regarding measurement of core body temperature in a patient with heat illness?
(A) rectal thermometers are used only in patients who feel “hot” to the touch.
(B) rectal thermometers are preferred but need only to be able to measure up to 106°F (41.1°C)
(C) oral temperatures are notoriously unreliable in exertional heat illness because of tachypnea and compliance
(D) tympanic membrane temperature measurement has been proven to reflect true core temperature because the tympanic membrane is adjacent to the hypothalamic temperature regulation center
(E) all of the above
19. After successfully taking care of the marathon runners, you are asked by the medical student what type of preparatory advice you can give future runners. You would include all of the statements below except
(A) the sweat rate for the average endurance athlete in a temperate climate averages 1.0-1.2 L per hour and can exceed 2 L per hour in conditions of high heat and humidity
(B) sweat is hypotonic and is more hypotonic in those athletes who sweat greater volumes
(C) athletes should voluntarily drink fluids before, during, and after activities
(D) if an athlete is participating in endurance events, she or he should start taking salt tablets 2-3 days before competition
(E) proper nutrition, adequate sleep, gradual acclimatization, and avoidance of drugs/substances like alcohol, ephedra, and caffeine are important preventive measures
ANSWERS
1. (D) Heat cramps are a common mild form of heat illness that tend to occur after exercise and are associated with a large production of sweat during exercise. Heat cramps also occur in unconditioned athletes.
2. (B) All of the listed factors contribute to an increased risk of heat illness. However, dehydration and volume depletion as a result from sweating without adequate fluid replacement is the most important risk factor for heat-related illness.
3. (C) The best initial treatment for heat cramps is drinking an electrolyte solution (or administering 1 tsp of table salt dissolved in 500 mL of water). The underlying cause of heat cramps is total-body salt depletion. Cramping is often made worse by excessive intake of hypotonic fluids such as water. Gentle massage and stretching may be a helpful adjunct to treatment of the underlying problem. IV fluid use is generally reserved for the more severe cases.
4. (C) The best prevention of heat cramps is adequate hydration before and during athletic activities. Appropriate clothing, conditioning, and, in rare cases, modest increases in dietary salt are helpful interventions. Excessive water intake often worsens heat cramps because it causes further total body sodium loss.
5. (C)
6. (A) Heat stroke is associated with temperatures of 105°F (40.5°C) or higher.
7. (B) In the setting of suspected heat stroke, it is vital that you initiate treatment before firmly establishing the diagnosis. In fever, the set point for temperature regulation is increased and often responds to the use of antipyretics. In the setting of heat illness, the set point for temperature regulation is maintained yet hyperthermia results because more heat is gained than lost. In hyperthermia, antipyretics are likely to be ineffective and alternative methods of body cooling are necessary.
8. (D) Whether in the medical tent or in the emergency department it is critical to initiate treatment immediately. The most important initial treatment is the institution of rapid cooling. The treating physician must also follow the general principles of ABC, monitor the vital signs, obtain appropriate laboratory tests, and start IV rehydration. The most effective way to achieve rapid cooling is whole body immersion in ice water. Unfortunately this method is usually not practical. The most common way to initiate rapid cooling is through the use of water sprays and fans (maximizes convection). One may also pack the athlete in ice or cold wet towels. It is important to expose as much skin as possible. One should avoid placing ice packs over the major vessels in the groin and axilla because this may result in peripheral vasoconstriction and less efficient cooling. See Table 80-1 for summary of heat exhaustion versus heat stroke.
9. (D) One of the most common complications of rapid cooling is overcooling, and temperatures as low as 88°F (31°C) have been reported (Boston Marathon). Therefore, the ideal temperature at which to stop rapid cooling is 101°F (38.3°C), subsequently allowing the body to further cool on its own. Shivering is a sign of overcooling and actually causes increased heat production and may cause a rebound increase in core temperature.
10. (C) Heat stroke is the most severe form because it is associated with irreversible tissue damage.
11. (D) Heat and humidity are most important. Once ambient temperature equals or exceeds skin temperature, conduction, convection, and radiation cease to be effective methods of heat loss. Once ambient humidity exceeds 75%, the effectiveness of evaporation decreases. Low winds are associated with decreased heat dissipation.
TABLE 80-1 Heat Exhaustion Versus Heat Stroke
|
FACTOR |
HEAT EXHAUSTION |
HEAT STROKE |
|
|
||
|
Signs and symptoms |
Vague malaise, fatigue, headache, nausea, dizziness |
Central nervous system dysfunction (coma, seizures, delirium) |
|
Core temperature |
Normal or elevated <40.0C |
Elevated >40.5C |
|
Sweating |
Common |
Present in some cases but dry, hot skin is more concerning |
|
Treatment |
Slow cooling |
Rapid cooling |
|
Slow volume repletion |
Vigorous volume repletion if orthostatic and hypotensive <90/60 mm Hg |
|
|
Antipyretic benefit |
Ineffective |
Ineffective |
|
End organ injury |
Reversible |
Often irreversible |
|
|
||
12. (D) Evaporation (via sweating) is the dominant mode of heat dissipation or heat loss in the body.
13. (A) Conduction requires direct contact of the body with surrounding objects and air.
14. (B) Heat cramps are thought to be caused by a total body loss of sodium and are exacerbated by excessive sweating.
15. (C) Children are at increased risk for heat illness because circulating blood volume is less and the ability to circulate blood volume increases blood flow to the periphery, resulting in a greater ability to dissipate heat.
16. (D) Both conditions have similar initial signs and symptoms; however, they represent a continuum of disease process. If left untreated or unrecognized, heat exhaustion can quickly become heat stroke at which time extreme hyperpyrexia (>40.5°C [105°F]—not seen in heat exhaustion), coma, seizures, and irreversible tissue damage can occur.
17. (E) All of the above are potential complications of heat stroke. Rhabdomyolysis, dysrhythmias, acidosis, adynamic ileus, electrolyte imbalances, and seizures are also seen.
18. (C) Rectal temperature measurement is the gold standard, and it is recommended that probes be accurate to at least 112°F. Tympanic membrane measurement has not correlated well with 10-cm rectal probe temperature measurements in research studies, despite the hypothesis described in answer D.
19. (D) Salt tablets are generally not recommended because the high solute load causes gastrointestinal irritation. However, adding extra table salt to food is recommended.
![]()
SUGGESTED READING![]()
Barkin RM. Pediatric Emergency Medicine: Concepts and Clinical Practice. St. Louis, MO: Mosby; 1997:430-433.
Barr SI, Costill DL, Fink WJ. Fluid replacement during prolonged exercise: effects of water, saline or no fluid. Med Sci Sports Exerc. 1995;27:2002-2010.
Fleisher GR. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott; 2010.
Lugo-Amador N, Rothenhaus T, Moyer P. Heat-related illness. Emerg Med Clin North Am. 2004;22:315-327.
Marx J, Hockberger R, Walls R. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. St. Louis, MO: Mosby; 2009.
CASE 81: A 5-YEAR-OLD BOY WITH ABDOMINAL PAIN![]()
A 5-year-old African American boy presents to a pediatric emergency department with a chief complaint of abdominal pain. His pain is periumbilical and is described as diffuse and nonradiating, worsening with no relationship to meals or bowel movements. His pain began after lunch yesterday and he developed vomiting overnight. He has had three nonbilious and nonbloody episodes of emesis, two loose nonbloody stools today, and a tactile temperature. He states he is thirsty but has refused to eat for the last several hours. The patient denies headache, sore throat, dysuria, frequency, or urgency. His past medical history is unremarkable.
His vital signs reveal a BP of 100/60 mm Hg, pulse of 100, respiratory rate of 36, and a temperature of 100.4°F (38°C). Upon examination he is found to have dry mucous membranes, hypoactive bowel sounds with reproducible periumbilical tenderness, mild right lower quadrant (RLQ) tenderness, and rebound tenderness. His rectal examination is unremarkable except for a small amount of soft stool in the rectal vault.
SELECT THE ONE BEST ANSWER
1. What is the most likely diagnosis in this patient?
(A) gastroenteritis
(B) acute pancreatitis
(C) peritonitis
(D) acute appendicitis
(E) cholecystitis
2. Initial management steps for this patient in the emergency department should include all of the following except
(A) make the patient NPO (nothing by mouth)
(B) administer IV fluids
(C) place a nasogastric tube to low intermittent wall suction
(D) obtain prompt surgical consultation
(E) draw appropriate laboratory studies
3. Which of the following laboratory studies is least helpful in confirming the etiology of this patient’s abdominal pain?
(A) serum electrolytes, blood urea nitrogen (BUN), and creatinine
(B) urinalysis
(C) C-reactive protein (CRP)
(D) white blood cell count with differential
(E) amylase and lipase
4. All of the following are common causes of acute abdominal pain in children that do not require surgical treatment except
(A) mesenteric adenitis
(B) gastroenteritis
(C) psoas abscess
(D) pyelonephritis
(E) constipation
5. Which of the following is/are considered common extra-abdominal cause(s) of abdominal pain in children?
(A) ingestion of drugs such as acetaminophen or salicylates
(B) diabetic ketoacidosis
(C) pneumonia
(D) group A streptococcal pharyngitis
(E) all of the above
6. Which of the following statements describing acute appendicitis in a school-age child is false?
(A) diarrhea is rarely associated with appendicitis
(B) the onset of abdominal pain frequently precedes the appearance of any other symptoms
(C) tenderness upon rectal examination is a nonspecific finding in appendicitis
(D) anorexia and low-grade fever may be associated symptoms
(E) pain may be either constant or colicky but almost always worsens with movement
7. Which of the following physical examination findings is least likely to correlate with a diagnosis of acute appendicitis?
(A) referred tenderness from the left lower quadrant (LLQ) to the RLQ during palpation
(B) bluish discoloration around the umbilicus
(C) tenderness at a point between the umbilicus and the anterior superior iliac spine two-thirds the distance from the umbilicus
(D) extension of the hip posteriorly with the patient lying prone elicits pain
(E) abduction of the right hip with the patient lying supine elicits pain
8. Which of the following statements is true regarding the management of acute appendicitis in children?
(A) all patients should receive immediate IV antibiotics
(B) all patients should have at least one imaging study
(C) all patients should have a prompt surgical consultation
(D) all pain medicine should be held until a surgeon evaluates the patient
(E) all of the above
9. Which of the following statements is true regarding imaging studies in children with acute appendicitis?
(A) CT offers the advantages of better contrast sensitivity, the capability of viewing all tissue layers, reduced operator dependence, and is the safest imaging modality
(B) ultrasonography offers the advantage of low cost, no radiation exposure, and little variation among operators
(C) abdominal radiographs are most helpful in diagnosing other causes of abdominal pain, such as constipation, bowel obstruction, or free air
(D) ultrasonography offers 100% sensitivity and specificity to accurately exclude the possibility of appendicitis as a cause of acute abdominal pain in children as long as either a normal appendix is visualized or the appendix is not visualized at all
(E) all of the above statements are true
10. Which of the following statements is false?
(A) appendicitis is the most common surgical abdominal emergency in children
(B) missed appendicitis is one of the top reasons for malpractice claims in the emergency department
(C) in cases involving appendicitis in children, a well-documented chart will not prevent a lawsuit
(D) all children with acute onset of abdominal pain should have an imaging study regardless of the clinical diagnosis
(E) males have a higher lifetime risk of suffering from appendicitis than females
11. A delay in diagnosing acute appendicitis in children can have serious consequences. Which of the following is least likely to occur as a direct result of a delayed diagnosis?
(A) death
(B) bowel obstruction
(C) perforation
(D) peritonitis
(E) pancreatitis
12. A 5-year-old boy presents to the pediatric emergency department early in the morning. You find him lying on his side with his knees curled up. His mother tells you he fell off his bike last night. He is now complaining of worsening periumbilical abdominal pain and also midback pain. On examination, the child has hypoactive bowel sounds, guarding, and right upper quadrant tenderness. All of the following statements are true regarding your suspected diagnosis except
(A) a complete blood count might demonstrate a leukocytosis with a bandemia
(B) abnormal liver function tests as well as an elevated lipase and amylase might be present
(C) a sentinel loop of small bowel seen best on a plain radiograph is often diagnostic
(D) ultrasonography is the cornerstone of diagnosis for the suspected condition
(E) blunt abdominal trauma is a relatively rare cause of this condition
13. Which of the following is least likely to be a potential cause of acute pancreatitis in a 5-year-old?
(A) trauma
(B) cholelithiasis
(C) viral infection
(D) cystic fibrosis
(E) urolithiasis
14. You are asked to evaluate a 2-year-old African American girl who presents with a history of sudden, intermittent, crampy abdominal pain for 1 day and decreased oral intake. Your physical examination reveals no reproducible abdominal tenderness; however, a guaiac-positive soft mucous-like stool on rectal examination is noted. Which of the following abdominal imaging studies would diagnose and treat your suspected diagnosis?
(A) a plain radiograph
(B) ultrasonography
(C) CT
(D) barium enema
(E) MRI
15. A 1-year-old presents with bilious vomiting, abdominal distention, tenderness, and guarding. Which of the following diagnoses would be most likely?
(A) midgut volvulus
(B) mesenteric adenitis
(C) peritonitis
(D) gastroenteritis
(E) Meckel diverticulum
16. In any infant or toddler who presents with acute abdominal pain, bilious emesis, and guarding, which of the following imaging studies is the initial study of choice most likely to confirm your suspicions?
(A) MRI
(B) ultrasonography
(C) CT
(D) barium enema
(E) upper gastrointestinal (GI) series
17. A 6-week-old infant with postprandial emesis worsening over the past 4 days presents to the emergency department. The mother describes the vomit as projectile and nonbilious. On examination, the child appears hungry and slightly dehydrated. In preparation for your discussion with the surgeons, you order some basic laboratory tests. You suspect the child will have
(A) normal laboratory values
(B) hyperkalemia, hyperchloremia metabolic alkalosis
(C) hypokalemia, hypochloremia metabolic alkalosis
(D) hyperkalemia, hyperchloremia metabolic acidosis
(E) hypokalemia, hypochloremia metabolic acidosis
ANSWERS
1. (D) Acute appendicitis is the most likely etiology of this patient’s illness. Although the presentation could initially be confused with gastroenteritis, the presence of hypoactive bowel sounds, anorexia, pain preceding the onset of any other symptoms, and reproducible tenderness have a higher likelihood of appendicitis than any of the other diseases listed.
2. (C) The placement of a nasogastric tube should be reserved for patients who need gastric decompression. This would include patients with suspected pancreatitis, some forms of bowel obstruction such as a volvulus, or a patient with bilious emesis.
3. (A) Serum electrolytes, BUN, and creatinine may be helpful for assessing a patient’s renal and hydration status but otherwise add little to the diagnostic evaluation of abdominal pain. The urinalysis is useful to exclude the diagnosis of a urinary tract infection; amylase and lipase are useful in differentiating pancreatitis from other causes of abdominal pain such as appendicitis. Lastly, the combination of an increased leukocyte count with an increased blood CRP level can be suggestive of appendicitis in the setting of acute abdominal pain.
4. (C) A psoas abscess usually requires surgical drainage.
5. (E) All of the conditions can present with abdominal pain in children and must be included in the differential diagnosis.
6. (A) In children, diarrhea can be associated with the presence of appendicitis up to 30% of the time. Many of the clinical features of acute appendicitis are nonspecific; however, pain as the initial symptom and pain associated with movement—that is, jumping up and down, riding in a bumpy car, or tapping on the patient’s heel—raise clinical suspicion.
7. (B) Bluish discoloration around the umbilicus describes Cullen sign that, when coupled with Grey Turner sign (bluish discoloration around the flank), is suggestive of acute hemorrhagic pancreatitis (see Figure 81-1). Rovsing sign refers to referred pain from the LLQ to RLQ. McBurney point is the classic RLQ appendiceal location for pain. Choices “D” and “E” refer to the classic psoas and obturator signs, respectively, that if present, nonspecifically support the diagnosis of acute appendicitis.

FIGURE 81-1. Grey Turner and Cullen Signs. This patient has both flank and periumbilical ecchymoses characteristic of Grey Turner and Cullen signs. (Reproduced, with permission, from Knoop KJ, Stack LB, Storrow AS, et al. Atlas of Emergency Medicine, 3rd ed. New York: McGraw-Hill; 2010:166. Photo contributor: Michael Ritter, MD.)
8. (C) All suspected cases of acute appendicitis should have early surgical evaluation because some children will be spared further diagnostic evaluations once the decision for surgical treatment has been made. In the absence of a perforation or peritonitis, antibiotics are not always necessary, although most experts recommend them. Often the diagnosis of appendicitis can be made clinically and imaging is not necessary. Pain medication should not be withheld. The examination of a surgical abdomen will not be masked by giving adequate pain control to a child.
9. (C) Abdominal radiographs are traditionally not useful in the diagnostic evaluation of appendicitis except in the presence of a fecalith (calcified appendix). The disadvantage of CT is radiation exposure compared with ultrasound imaging associated with a high degree of operator dependency and variation. The presence of a normal appendix on an ultrasound effectively excludes appendicitis as a diagnosis; however, the inability to visualize the appendix renders the study inconclusive.
10. (D) Not all patients with acute abdominal pain need an imaging study, but a prompt surgical consultation is recommended.
11. (E) Pancreatitis is not a complication of acute appendicitis. Rather, it must be differentiated from appendicitis in the setting of acute abdominal pain.
12. (E) All of the choices are true in the setting of suspected acute pancreatitis except that blunt abdominal trauma is actually a common cause. In fact, it is the most common cause of acute pancreatitis and accounts for 13-33% of cases.
13. (E) Blunt trauma to the midepigastric area of the abdomen such as being struck with bicycle handlebars is the most common cause of acute pancreatitis in children. Viruses such as coxsackie B, cytomegalovirus, varicella, hepatitis A and B, influenza A and B, and Epstein-Barr virus have also been implicated in addition to bacterial and parasitic causes. Gallstones can cause pancreatitis but are usually only seen in this age range in the presence of a hereditary hemolytic anemia such as hereditary spherocytosis or sickle cell disease. Cystic fibrosis can cause acute pancreatitis, but the incidence is relatively low among African Americans. Renal stones should not cause pancreatitis.
14. (D) A barium enema continues to be the gold standard for the diagnosis (100% sensitivity and specificity) and has a 70% successful reduction rate of intussusception. However, recent practice reflects increasing use of ultrasonography with pneumatic reduction by an air enema. Success rates approach 90% with fewer complications than barium enemas.
15. (A) The presence of bilious emesis should prompt a thorough evaluation for bowel obstruction. Malrotation with intermittent volvulus is one cause in the toddler to preschool-age child (see Figure 81-2).

FIGURE 81-2. Abdominal radiograph of a 10-day-old infant with bilious emesis. Note the dilated proximal bowel and the paucity of distal bowel gas, characteristic of a volvulus. (Reproduced, with permission, from Brunicardi FC, Andersen DK, Billiar TR, et al. Schwartz’s Principles of Surgery, 9th ed. New York: McGraw-Hill; 2010: Fig. 39-16.)
16. (E) An upper GI series with a contrast enema is still the gold standard for the diagnosis of volvulus. If the duodenal C-loop crosses to the left of the midline at a level higher than or equal to the pylorus, then malrotation is effectively ruled out. Conversely, a corkscrew column that ends abruptly is highly suspicious for volvulus.
17. (C) Pyloric stenosis is the most common disorder requiring abdominal surgery in infancy. Vomiting is the initial complaint and can begin around 3 weeks of age. Parents note that the child has a voracious appetite and then forceful emesis at the end of the feeding or just after. A hypokalemic, hypochloremic metabolic alkalosis may be found in these infants.
![]()
SUGGESTED READING![]()
Barkin RM. Pediatric Emergency Medicine: Concepts and Clinical Practice. St. Louis, MO: Mosby; 1997:726-795.
Fleisher GR. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott; 2010.
Guzman D. Pediatric surgical emergencies. Clin Pediatr Emerg Med. 2002;3(1):1–2.
Halter J, Basel T, Nicolette L, et al. Common gastrointestinal problems and emergencies in neonates and children. Clin Fam Pract. 2004;6(3):731-754.
Reynolds S. Missed appendicitis and medical liability. Clin Pediatr Emerg Med. 2003;4(4):231.
CASE 82: A 3-YEAR-OLD GIRL WHO DRINKS A BOTTLE OF ACETAMINOPHEN![]()
You are called to evaluate a 3-year-old, 15-kg girl brought in by ambulance. The aunt who arrived with the patient states she was sick last week with a “cold” and had fever up to 101°F (38°C), a cough, and 2-3 episodes of vomiting. Currently, the girl is complaining of “stomach pain.” The aunt states that she left the girl alone for 10 minutes while she took a shower. The aunt found her with an empty bottle of berry-flavored acetaminophen next to her and some drops of it on her shirt.
According to the aunt, the ingestion occurred no more than 30 minutes ago. On physical examination, the BP is 90/50 mm Hg, the pulse is 110, the respiratory rate is 40, and she is afebrile. The child appears uncomfortable. The examination is significant for mild midepigastric tenderness without rebound or guarding. Bowel sounds are normal and a rectal examination is unremarkable. You note that the child has a acetaminophen “mustache” and a berry-like odor to her breath. Mom arrives with the empty acetaminophen bottle. You examine the bottle and see it originally contained 4 oz of acetaminophen suspension (160 mg/5 mL). Mom states the bottle was new because she ran out when her child was sick and restocked her medicine cabinet yesterday.
SELECT THE ONE BEST ANSWER
1. Which of the following laboratory studies is most likely to be helpful in the management of this 3-year-old patient?
(A) standard urine drug screen
(B) liver function tests
(C) 1 hour serum acetaminophen level
(D) electrolytes, BUN, creatinine, blood glucose
(E) 4-hour serum acetaminophen level
2. The patient is complaining of nausea. Which of the following statements best describes your initial management steps?
(A) activated charcoal alone
(B) activated charcoal plus gastric lavage
(C) N-acetylcysteine (NAC) alone
(D) activated charcoal and NAC
(E) gastric lavage, activated charcoal, and NAC
3. Which of the following statements regarding childhood poisonings is false?
(A) the ingestion of a potentially poisonous substance by a young child is a common event
(B) death attributable to unintentional poisoning is uncommon in children younger than 6 years
(C) data such as signs and symptoms of toxicity, management strategies in the home, and indications for seeking emergency care are available from local and national poison control centers
(D) the American Academy of Pediatrics (AAP) currently recommends that syrup of ipecac be kept at home for emergency use
(E) the storage of poisonous substances in the home should be discussed at the 6-month wellchild visit
4. All of the following statements correctly describe reasons for the decrease in the death rate attributable to unintentional poisoning among young children in the last 50 years except
(A) the advent of child-resistant closures for products
(B) an increase in the over-the-counter (OTC) drug products available for parents to purchase for routine household use
(C) improved public education and anticipatory guidance
(D) the establishment of multiple poison control centers
(E) all of the above are true (no exception)
5. Which of the following statements regarding syrup of ipecac is true?
(A) the only recommended method of inducing emesis is administration of ipecac
(B) syrup of ipecac is a safe emetic
(C) the amount of substance removed from the stomach is solely related to the duration of time from its ingestion to emesis
(D) the induction of emesis using ipecac is the first line of treatment in the pediatric emergency department
(E) the use of home ipecac therapy has the potential to decrease the efficacy of other poison treatments, such as activated charcoal or NAC
6. Which of the following statements best describes gastrointestinal decontamination in the emergency department setting?
(A) the initial management steps should always include gastric lavage or administration of an antiemetic
(B) the use of activated charcoal alone without gastric emptying is the recommended procedure of choice
(C) a cathartic, such as sorbitol, is used with each dose of activated charcoal to improve its efficacy
(D) the risk of aspiration is decreased when a gastric emptying technique is performed in conjunction with the administration of activated charcoal
(E) all of the above
7. A 15-year-old girl is brought to the pediatric emergency department and is unresponsive with no gag reflex. Her friends called 911 when they found her passed out at a party. Which of the following should be your initial step in the management of this patient?
(A) intubate the patient
(B) administer naloxone
(C) obtain a bedside glucose measurement
(D) administer 20 mL/kg of 0.9% normal saline as an IV bolus over 30 minutes
(E) call the poison control center for assistance
8. Which of the following ingested substances is least likely to adsorb activated charcoal?
(A) acetaminophen
(B) salicylates
(C) iron
(D) beta-blockers
(E) tricyclic antidepressants (TCAs)
9. Acetaminophen overdose is most frequently associated with toxicity to which of the following?
(A) central nervous system
(B) liver
(C) kidneys
(D) pancreas
(E) bone
10. Which of the following statements describing acetaminophen toxicity is false?
(A) most cases involve unintentional overdosing
(B) delays in the diagnosis and treatment of acetaminophen intoxication do not adversely affect outcome
(C) the risk of toxicity is increased in patients taking drugs such as carbamazepine that are metabolized via the cytochrome P450 pathway
(D) acetaminophen toxicity includes four phases progressing from mild nonspecific symptoms to onset of organ injury, peaking with maximum organ injury and ending with either recovery or irreversible injury
(E) conditions such as diabetes mellitus, obesity, malnutrition, and/or a family history of hepatotoxic reactions may increase the risk of acetaminophen toxicity
11. A 3-year-old boy presents to the pediatric emergency department after ingesting half a bottle of ibuprofen. Which of the following statements is true regarding acute NSAID toxicity?
(A) most ibuprofen overdoses follow a benign, rapidly reversible course
(B) plasma NSAID concentrations are useful and should always be obtained
(C) as a result of high protein binding and rapid metabolism, gastric decontamination with activated charcoal is never indicated
(D) GI toxicity is rarely associated with NSAID use or overdose
(E) all of the above
12. Which of the following household items is least likely to be harmful to a child if swallowed in large quantities?
(A) antidiarrheal medication
(B) ibuprofen
(C) mouthwash
(D) multivitamins
(E) household bleach
13. Which of the following statements is false regarding caustic ingestions?
(A) the vast majority of all reported cases of caustic ingestion occur in children
(B) caustic substances have the potential to cause tissue burns on contact with the eyes, skin, airway/ lungs, and/or the GI tract
(C) alkalis, acids, and antiseptics are all agents capable of causing chemical injury
(D) the transfer and storage of cleaners and caustic substances to alternative household containers has been associated with a decreased risk of ingestion in children
(E) button battery ingestion may cause esophageal obstruction and pressure necrosis and/or caustic injury because of leakage of alkaline material
14. The presentation of a comatose patient with marked miosis, respiratory depression, hypotension, bradycardia, and hyporeflexia would make you most concerned about the possible overdose of which of the following?
(A) opioids
(B) organophosphates
(C) cocaine
(D) diphenhydramine
(E) pseudoephedrine
15. The presentation of a confused, diaphoretic patient with miosis, abdominal cramping, fecal and urinary incontinence, profuse sweating, and drooling would cause you to be most concerned about which of the following toxic ingestions?
(A) opioids
(B) organophosphates
(C) cocaine
(D) ethanol
(E) ephedra
16. Which of the following signs and symptoms is not consistent with an anticholinergic toxic syndrome?
(A) tachycardia
(B) dry, flushed skin
(C) urinary retention
(D) miosis
(E) slightly elevated temperature
17. Which of the following pair of toxins and antidotes does not match?
(A) opiates and naloxone
(B) benzodiazepines and flumazenil
(C) methanol and ethanol
(D) salicylates and NAC
(E) iron and deferoxamine
ANSWERS
1. (E) Simply detecting the presence of the drug ingested is not as helpful as the actual measurement of the serum drug level. Drug screens are helpful in detecting the presence of other ingested substances. Acetaminophen levels are important. However, a 4-hour level is needed to determine the relative risk of hepatic damage and the need to administer NAC. The Rumack-Matthew Nomogram helps to determine the need for NAC.
2. (A) The need for gastric lavage for patients with an acetaminophen overdose is rare because of the rapid GI absorption of acetaminophen. Activated charcoal will effectively adsorb acetaminophen and is ideally given in the first 30 minutes to 1 hour postingestion. NAC is an effective antidote that should be given up to 8 hours postingestion. However, NAC should be given after the 4-hour acetaminophen level is back and the Rumack-Matthew nomogram should be used.
3. (D) The AAP no longer recommends syrup of ipecac be stored in a household for emergency use.
4. (B) Decreases in the death rate are attributable to safer medications and product formulations, not the OTC availability.
5. (E) Syrup of ipecac is no longer recommended for toxic ingestions. It can delay emergency department care of the child and limit more effective interventions due to repetitive emesis.
6. (B) The current recommendation to use activated charcoal (AC) alone for GI decontamination without the use of a gastric emptying technique such as gastric lavage or syrup of ipecac has improved outcomes. Sorbitol speeds AC clearance but does not improve efficacy. Multiple doses of sorbitol can lead to profuse diarrhea and electrolyte imbalance in small children. The risks of aspiration are largely avoided when AC is used alone.
7. (A) The highest priority in the management of any acutely ill patient is the evaluation and support of airway, breathing, and circulation (ABCs).
8. (C) Ions, hydrocarbons, metals such as iron, and ethanol do not adsorb. Whole bowel irrigation may be considered.
9. (B) Hepatotoxicity is of greatest concern because hepatic metabolism accounts for up to 90% of acetaminophen elimination. It is important to note that in acute toxicity, liver injury usually presents 24-48 hours postingestion. Acetaminophen ingestions of more than 150 mg/kg are associated with highest risk of hepatotoxicity.
10. (B) Delay in diagnosis and failure to institute treatment measures are associated with poorer outcomes. Because the early symptoms seen in stage 1 are nonspecific, a heightened awareness of the potential for toxicity and the recognition of patients at risk for toxicity are vital.
11. (A) Unlike acetaminophen toxicity, NSAID overdoses do follow fairly benign courses. Children who ingest more than 300 mg/kg should have GI decontamination, evaluation, and observation. Highprotein binding causes urinary alkalinization, hemoperfusion, and hemodialysis to be ineffective in enhancing elimination (dialysis is used in salicylate intoxication). GI side effects are the most common side effects associated with the use of NSAIDs.
12. (E) Household bleach is nontoxic. Antidiarrheal products tend to contain salicylates. Both salicylates and ibuprofen can cause significant renal impairment. Many mouthwash products contain ethanol that can cause hypoglycemia. A multivitamin overdose can lead to multiple organ system impairment.
13. (D) The transfer of caustic substances to unlabeled or erroneously labeled containers is an associated risk factor for potential ingestion by a child.
14. (A) An opioid overdose results in global depression with depressed sensorium as the hallmark.
15. (B) This scenario describes the cholinergic syndrome seen in organophosphate poisoning. A useful mnemonic to remember is “SLUDGE”: salivation, lacrimation, urination, defecation, GI cramping, and emesis. Exposure sometimes occurs through unsuspected dermal exposure. Organophosphates are found in many pesticides and insecticides as well as drugs such as neostigmine and physostigmine.
16. (D) The anticholinergic effects include all the following except miosis. Dilated pupils, or mydriasis are seen. Remember “mad as a hatter,” “red as a beet,” “dry as a bone,” and “hot as a hare.” Anticholinergics are found in drugs such as atropine as well as hallucinogenic mushrooms and plants such as jimson weed.
17. (D) NAC is the antidote used in acetaminophen toxicity.
![]()
SUGGESTED READING![]()
AAP Committee on Drugs. Acetaminophen toxicity in children. Pediatrics. 2001;108(4):1020-1024.
AAP Policy Statement. Poison treatment in the home. Pediatrics. 2003;112(5):1182-1185.
Abbruzzi G. Pediatric toxicologic concerns. Emerg Med Clin North Am. 2002;20(1):223-247.
Barkin RM. Pediatric Emergency Medicine: Concepts and Clinical Practice. St. Louis, MO: Mosby; 1997:463-513.
Fleisher GR. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott; 2010.
Goldfrank LR. Goldfrank’s Toxicologic Emergencies. 9th ed. New York, NY: McGraw-Hill; 2010.
Marx J, Hockberger R, Walls R. Rosen’s Emergency Medicine. 7th ed. St. Louis, MO: Mosby; 2009.