Psoriasis is a chronic, recurrent disease marked by epidermal proliferation and characterized by remissions and exacerbations. Flare-ups are commonly related to specific systemic and environmental factors but may be unpredictable. Widespread involvement is called exfoliative or erythrodermic psoriasis.
Although this disorder commonly affects young adults, it may strike at any age, including infancy. Genetic factors predetermine the incidence of psoriasis; affected families have a significantly greater incidence of human leukocyte antigens (HLA) B13, B17, and CW6.
Flare-ups can usually be controlled with therapy. Appropriate treatment depends on the type of psoriasis, the extent of the disease, the patient's response, and the effect of the disease on the patient's lifestyle. No permanent cure exists, and all methods of treatment are palliative.
Causes
· Genetically determined tendency to develop psoriasis
· Possible immune disorder, as suggested by HLA type in families
· Flare-up of guttate (drop-shaped) lesions from infections, especially beta-hemolytic streptococci
Other contributing factors
· Pregnancy
· Endocrine changes
· Climate (cold weather tends to exacerbate psoriasis)
· Emotional stress or physical illness
· Infection
· Certain medications, such as systemic glucocorticoids and lithium
Pathophysiology
A skin cell normally takes 14 days to move from the basal layer to the stratum corneum, where it's sloughed off after 14 days of normal wear and tear. Thus, the life cycle of a normal skin cell is 28 days.
In psoriasis, the immune system sends signals that speed up the normal process from 28 days to just 4 days. This markedly shortened cycle doesn't allow time for the cell to mature. Consequently, the stratum corneum becomes thick with extra skin cells. On the surface, the skin cells pile up and the dead cells create a white, flaky layer, the cardinal manifestation of psoriasis.
Signs and symptoms
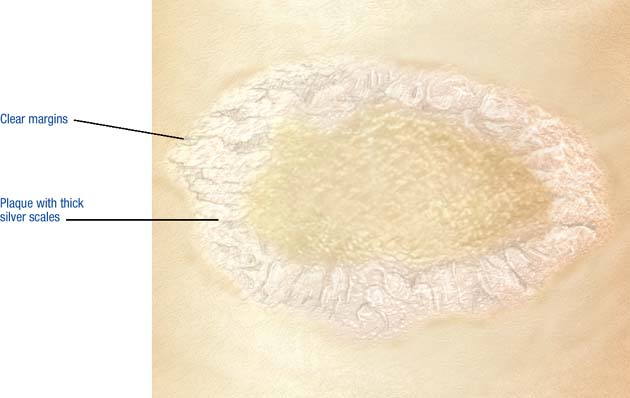
· Erythematous papules and plaques with thick silver scales, most commonly on the scalp, chest, elbows, knees, back, buttocks
· Plaques with characteristic silver scales that either flake off easily or thicken, covering the lesion (scale removal can produce fine bleeding [Auspitz's sign])
· Itching and occasional pain from dry, cracked, encrusted lesions
· Occasional small guttate lesions (usually thin and erythematous, with few scales), either alone or with plaques
Diagnostic test results
Diagnosis is based on patient history, appearance of the lesions and, if needed, the results of skin biopsy. Blood chemistry reveals elevated serum uric acid level.
Treatment
· Topical fluorinated glucocorticoids
· Low-dose antihistamines, oatmeal baths, emollients, and open wet dressings to help relieve pruritus
· Aspirin and local heat to help alleviate the pain of psoriatic arthritis; nonsteroidal anti-inflammatory drugs in severe cases
· Ultraviolet B (UVB) or natural sunlight exposure to retard rapid cell production to the point of minimal erythema
· Tar preparations or crude coal tar applications to the affected areas about 15 minutes before exposure to UVB or at bedtime and wiped off the next morning
· Intralesional steroid injection for small, stubborn plaques
· Anthralin ointment or paste mixture for well-defined plaques (because anthralin injures and stains normal skin, apply petroleum jelly around the affected skin before applying it)
· Calcipotriene ointment, a vitamin D analogue; best when alternated with a topical steroid
· Tazarotene, a topical retinoid
· Topical administration of psoralens (plant extracts that accelerate exfoliation) followed by exposure to high-intensity UVA
· Extensive psoriasis: acitretin, a retinoid compound
· Resistant disease: cyclosporine
· Last-resort treatment for refractory psoriasis: cytotoxin, usually methotrexate
· Psoriasis of scalp: tar shampoo followed by a steroid lotion
P.389
PSORIATIC LESION
|
|
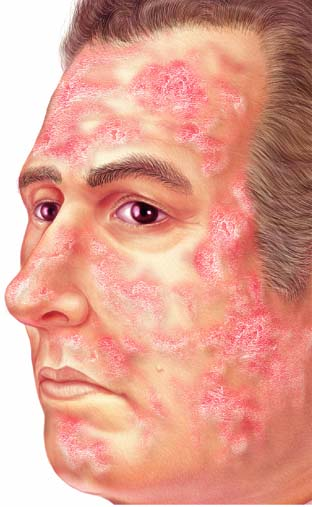
DIFFUSE PSORIATIC PLAQUES
|
|