Perhaps surprisingly, nighttime feedings are a frequent, if easy to miss, cause of major sleep disturbances. Once your baby is about three months old, she should not require more than one feeding during the night (in addition to a feeding at bedtime), and that last nighttime feeding will probably be given up at some point over the next month or two. You certainly should not have to continue getting up repeatedly during the night to feed her. If you do, the sleep disturbance associated with these excessive nighttime feedings can be dramatic, and if you allow the night feedings to continue, the problem may go on for a very long time—years, even. On the other hand, when you begin to eliminate the extra feedings, the improvement in sleep is usually very rapid.
You may find that having your child fall asleep as you feed her in your arms is rewarding for you and satisfying for her. There is nothing wrong with continuing to nurse your child to sleep during her first year, as long as you enjoy it, as long as you can easily transfer her to her crib or bed as soon as she is done, and as long as she begins to sleep through the night. But if it’s difficult to put her down after feedings, or if she wakes repeatedly and has to be fed each time before she can go back to sleep, then she is developing a sleep problem, and the feedings are almost certainly the cause.
A baby with this problem has learned to associate nursing with falling asleep, as described in Chapter 4. In addition, if your child drinks large amounts of milk or juice at night, her sleep may be disturbed for other reasons as well: for instance, if her diaper is soaked, the discomfort can certainly wake her. Furthermore, extra nutrients ingested at night will stimulate your child’s digestive system, which should ordinarily be relatively inactive during the night. The process of metabolizing those nutrients will alter patterns of functioning in other body systems; it will trigger or inhibit the release of many different hormones, and it will raise the body temperature, which is normally low at night. The overall result is that many important biological rhythms that are closely tied to the ability to sleep are disrupted.
Even the timing of a child’s feelings of hunger can be affected. We all get hungry at the times of the day or night when we are accustomed to eating. This timing is learned—it is not simply determined by the number of hours since our last meal. If, for example, you change your dinnertime from 5:00 to 7:00 P.M., then—after a period of gradual adaptation—you will find that you don’t get hungry in the evening until two hours later than you used to, even if your breakfast time and lunchtime remain unchanged. Similarly, if your child is used to being fed often during the night, she is likely to wake up hungry. She will eagerly nurse or take her bottle, but she has simply learned to eat on this schedule and does not actually need food at these times. This learned hunger then becomes a trigger for extra wakings. Her sleep at night won’t consolidate into long periods, but—like the sleep that occurs in the daytime—it will remain as mere naps between wakings and feedings.
Sleep disruptions caused by too much feeding at night occur most often in children under two years old who are still breast-feeding or using a bottle. Kayla, for example, was eight months old when I first saw her. Her parents told me that she fell asleep easily at bedtime while nursing at the breast, and once asleep, she could be moved into the crib without difficulty. She would sleep for two and a half hours, but then wake crying. Her father was unable to comfort her; only her mother seemed to be able to put her back to sleep. When she picked Kayla up and nursed her again, Kayla would stop crying and go back to sleep within ten minutes. But she would continue to wake up every hour or two, and each time the same process had to be repeated. On most nights Kayla woke five or six times for feedings, and her soaked diapers had to be changed at least once. Since Kayla’s mother was always the one to take care of Kayla at night, she was exhausted and frustrated. Occasionally she was so tired that she wanted to let Kayla cry, but her husband insisted that she respond. That made her angry with him as well as with Kayla, and there was a great deal of tension in the family.
You will probably recognize by now that Kayla associated falling asleep with being held and nursed. That was true, but it was not the whole story. When such associations are the only problem, there will usually be only a few apparent nighttime wakings, times when the child wakes fully and needs help returning to sleep. Kayla’s wakings, however, occurred too frequently—up to once an hour—to be explained by sleep associations alone. Something was either waking her more frequently or causing her to wake fully almost every time she stirred.
Allison, another child I saw with this problem, was two years old and had never once slept through the night. She was no longer held or rocked to sleep, but her parents handed her a bottle when she was placed in her crib. She always finished all eight ounces—sometimes twelve—then she turned over and fell asleep. After about three hours, she would wake crying and wouldn’t stop until she was given another bottle, after which she would fall asleep quickly again. She woke four to six times a night, and each time she needed another bottle to go back to sleep.
Often, when Allison woke, she was soaking wet even though she was in double or triple diapers. At each waking her mother or father would go in, change her if necessary, hand her another bottle, and leave. When Allison’s parents went to bed they would prepare four or five bottles and leave them in the refrigerator or on Allison’s window ledge. The entire burden did not fall on Allison’s mother as it had on Kayla’s, and since Allison did not need to be held, her parents could go right back to sleep themselves. Still, after two years, they too were tired and frustrated, and they usually went to bed early in the evening just to be sure they could get enough sleep.
Allison, like Kayla, had associations that interfered with falling asleep—in this case, sucking on a bottle. However, she did not need the bottle to actually fall asleep; that was evident because she usually finished the bottle, tossed it aside, rolled over, and then went to sleep without having the bottle in her mouth. Her sleep disturbances evidently had to do with the large amount of milk she drank during the night.
Both Kayla’s and Allison’s wakings had probably begun as the normal arousals of an infant who is just beginning to develop good sleep habits. But when their parents tried to “treat” these wakings with extra feedings, the wakings became excessive. The “cure” for normal wakings had become the cause of abnormal ones.
Is Your Child’s Sleep Problem
Caused by Nighttime Feedings?
Although your baby may give up regular nighttime feedings on her own by the end of her first three months, it is not reasonable to expect or insist that such a young infant give them up altogether. But if your child is at least three months old, still nurses or requires a bottle at bedtime, and needs to eat again several more times during the night, then the extra feedings may well be causing the extra wakings. If that is the case, you may be able to help her sleep better by decreasing the number of these feedings.
If your child nurses only for a minute or so at the nighttime wakings, or takes just a few sips from the bottle, she is not taking in much food. Rather, she is behaving like a child who is dependent on a pacifier: it is the breast or bottle itself that she needs before she can go to sleep, not the food. This pattern can be stopped immediately, as discussed in Chapter 4. On the other hand, if she takes in a substantial amount of food—from extended feedings at the breast, or from bottles adding up to more than eight ounces over the course of the night—then she has learned that certain times of night are mealtimes. To eliminate these feedings suddenly would be neither wise nor kind.
Frequent diaper changes are another clue that your child’s feedings at night may be excessive. Most babies three months or older do not need to be changed at night at all. If your baby’s diapers are often soaked when she wakes during the night, then it is likely that she is drinking too much. She certainly cannot be thirsty or getting too little to drink if she is wetting that much. Medical causes such as diabetes are extremely unlikely, certainly if the same problems (of excessive feeding and wetting) do not occur in the daytime. If you are at all concerned, consult your doctor. But in all likelihood your child probably simply has a habit of taking in too much fluid at night.
The amount of milk or juice your child drinks during the night may be considerable. If she finishes four full eight-ounce bottles, she is drinking an entire quart! That is a large amount for even an adult to consume overnight, and an adult who drinks that much at night will not sleep well, if only because it will mean extra trips to the bathroom. It should not be so surprising to find that your child, like Allison or Kayla, does not sleep well either.
How to Solve the Problem
If you have concluded that excessive and unnecessary feedings at night are disrupting your child’s sleep, you will be relieved to learn that although such feedings can produce especially severe sleep disturbances, this problem is also one of the easiest to treat. There are two tasks you need to carry out. One is to reduce or eliminate the nighttime feedings, thus avoiding their various sleep-disrupting effects and also helping your child learn to get hungry only at reasonable times during the day. The other task is to teach your child new sleep associations so that she can fall asleep without being held, without eating, and without sucking on the breast, bottle, or pacifier. You can take these jobs on simultaneously or one at a time.
To address the problems caused by the feedings, begin by gradually decreasing the number of nighttime feedings or their size, or both (see below for more about these options). Don’t stop the feedings suddenly: although your child would not suffer from lack of nourishment, she has become accustomed to being fed during the night and she will probably be hungry. A program designed to allow new patterns to develop gradually will be easier for her, and also for you.
Your goal is to gradually move your child’s feelings of hunger out of the nighttime and into the daytime by eliminating the feedings at night—or, if you have a young infant, at least to move some of the feedings to the daytime by spacing them farther apart at night. If your child feeds substantially at only one or two of the feedings, then the other “feedings” are not a response to hunger and can be eliminated immediately, like a pacifier. The real feedings can then be reduced gradually. Once there is only a single remaining nighttime feeding left, you can choose to stop that feeding right away (instead of gradually) if you prefer, since the total amount ingested during the night is now fairly small.
It is not always necessary to eliminate nighttime feedings altogether; in fact, for a young infant that would be inappropriate. Still, it is unpleasant and usually unnecessary to nurse or feed a baby hourly throughout the night; if your child is an infant, you may simply want to decrease the number of feedings. It’s entirely reasonable to cut back to two nighttime feedings by the time your child is two or three months of age, one feeding by three or four months, and none at all at five months. Many children give up nighttime feedings altogether around the age of three or four months; basically no normal, healthy full-term babies still require a nighttime feeding when they are five months old, and you can certainly insist on stopping them altogether at that point if you want to.
(There is nothing wrong with continuing a single nighttime feeding for some months beyond that point, if you enjoy it, but be aware that this is a choice, not a response to your baby’s biological needs. However, if you have to feed her several times during the night, it may not be so nice for your child, even if you don’t mind. Instead of allowing her an uninterrupted night’s sleep, you’re making it necessary for her to wake up repeatedly, call for you or go and find you, and perhaps wait for you to get up and prepare a bottle, before she can go back to sleep. After all, if she weren’t hungry at these times, she could just stir and go right back to sleep. Furthermore, if she relies on the breast or bottle to go back to sleep, she has another problem as well: if she happens to wake too soon after a feeding and is not yet hungry, or has completed a feeding but is still awake, then what is she to do? She is accustomed to nurse to go back to sleep, but now she doesn’t want to feed, or cannot, because she is not hungry. This is unpleasant for her, and it should be unnecessary.)
Use the chart in Figure 8 as a guide. Whether you are nursing or feeding by bottle, the key is to increase the minimum time between feedings. Note how close together your child’s nighttime feedings are currently, and use that interval as the point from which to begin adjusting the feeding schedule. (If there is a range—perhaps one to three hours—start with the shortest interval.) For example, if you are starting with an interval of two hours on the first night, don’t allow your child to feed until at least two hours have passed since the previous feeding. If your child wakes before two hours have passed, she will have to wait for her next feeding; if she wakes later, she can be fed immediately. Increase the minimum time between feedings by thirty minutes each night.
If you are bottle-feeding, you may find it helpful to decrease the amount offered at each feeding as well. Note how many ounces your child drinks at each waking. (If there is a range, start with the largest amount she takes most nights.) Each night, in addition to spacing out the feedings, decrease the amount in each bottle by one ounce. If you’re aiming to eliminate nighttime feedings altogether, keep this up until you reach one ounce per bottle. Because you also have been spacing out the feedings, there should now be only one or two nighttime feedings left, totaling one to two ounces for the entire night. On the next night, eliminate nighttime feedings completely.
(Many parents find that the nighttime wakings decrease markedly even before the feedings are completely eliminated, and that the remaining very small feedings—one to three ounces—sometimes seem more upsetting to a child than comforting. For this reason, parents sometimes decide to stop the feedings a day or two earlier than originally planned.)
FIGURE 8. ELIMINATING EXTRA FEEDINGS AT SLEEP TIMES
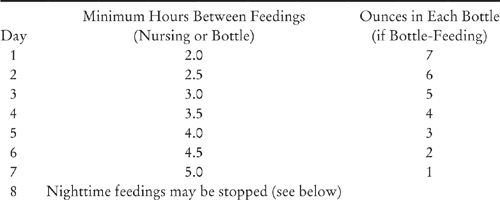
The ounces and times in this chart are general guidelines. You can alter them to fit your own desires and your child’s current feeding schedule.
1. If your child takes less than eight ounces in each bottle, start with one ounce less than she usually takes and continue reducing from there.
2. If the minimum time between your child’s nighttime feedings is already more than two hours, then begin with the line in the chart one half hour longer than the current minimum and continue increasing the times from there.
3. If you are breast-feeding, just increase the minimum time between feedings according to the first two columns on the chart. Don’t worry about the exact amounts consumed at each feeding.
4. By day seven, you will probably be feeding only once during the night, five hours or more after your child first falls asleep. If your child is young and you want to continue one feeding at night, you can stop here. Otherwise you can stop all nighttime feedings the next night. If you are nursing, and the remaining feeding seems to be a substantial one, or if you are bottle-feeding and have not made the feedings smaller, you can also choose to continue moving that last feeding further away from bedtime, an extra thirty minutes a night, until it moves out of the nighttime altogether.
5. If you prefer, you can decrease the size and number of feedings every other day instead of every day. It will just take a little longer.
If you are trying to reduce the number of nighttime feedings to one or two, rather than eliminating them altogether, then you may not need to decrease their size at all, unless any are more than eight ounces. (Most nighttime feedings should be in the range of four to eight ounces. Giving more than eight ounces is unnecessary, if the goal of the feeding is only to satisfy hunger, and feedings of less than four ounces usually reflect a habit of sucking more than they do true sensations of hunger.) Apart from that, all you need to do is to progressively increase the time between feedings (perhaps to somewhere between three and six hours, depending upon your child’s age and your goal) until you are down to the number of nighttime feedings you want.
If you are working on sleep associations and hunger patterns simultaneously, put your child in bed as soon as each feeding is over, even if she wakes and begins to cry. If you nurse her and she sleeps next to you, move her off of you when the feeding is done so that she can learn to fall asleep without using your breast as a pacifier. You’ve just fed her, so she is not hungry; now you are only changing her expectation of what happens while she falls asleep. (Remember, if she is asleep or almost asleep in your arms and never knows that she is being moved away from you, then when she wakes during the night she may be surprised to find she is no longer where she was when she went to sleep.) If she protests, follow the progressive waiting program described in Chapter 4, responding to her briefly at increasing intervals until either she goes back to sleep or it’s time for her next feeding. Within a week, if all goes well, you will have finished cutting down on or eliminating the nighttime feedings. After that, continue applying the technique of progressive waiting at any wakings at night (except for feeding times) until the wakings stop. It should not take more than another few days.
If you hand your child a bottle in the crib and she takes it by herself without being held, then you don’t need to work on her sleep associations directly. Since she already falls asleep by herself without being held, she does not have that association. As you eliminate feedings from the nighttime, the association of falling asleep with sucking will also disappear (as long as you do not introduce a pacifier to replace the bottle).
But if you are keeping some of the nighttime feedings, it is particularly important to dissociate feeding from the act of falling asleep. Your goal in feeding her is to take away the hunger, not to get her to sleep. If she keeps falling asleep in your arms, or even just with the bottle in her mouth, it may be difficult to make the progress you would like.
If you are nursing and your nursing child sleeps in your bed, you may have to be firm when she tries to get at your breast before it is time to nurse. You may even have to get up temporarily and sit by the bed, or even leave the room (if there is another parent staying behind for safety), until your child goes back to sleep or it’s time for the next feeding. Once the nighttime feedings stop, that will no longer be necessary.
If you have chosen to work on the nighttime hunger problem first and change sleep associations second, then don’t change the bedtime ritual yet. Let your child fall asleep in your arms during or after feeding, if that is what she has been doing. If she wakes and cries before it’s time for her next feeding, you can try to comfort her, if it helps. Do whatever seems to comfort her most: hold her, soothe her, rock her, or talk to her. The purpose is only to calm her down and help her fall asleep while she learns not to expect a feeding. Sometimes it’s best not even to try to help: if she sleeps in her own room, she may become more upset if you go in but refuse to feed her, and she may calm down more quickly without you there.
If you are a nursing mother, it may be difficult to hold your child without nursing her. You may have a letdown response, and your child will smell the milk and expect to nurse. In a two-parent family, it is often easier for the non-nursing parent to settle the child at times when she is not being fed. Your child may still seem a bit frustrated, but in this way she will learn not to expect you and to nurse so often during the night.
Once you have eliminated nighttime feedings or cut them down to the number you want, and your child is falling asleep without nursing or taking a bottle (at least after nighttime wakings), you have solved the problem of excessive fluids and broken the association of falling asleep with having the bottle or sucking at the breast. If she still needs you to hold her, rub her back, or rock her before she can go to sleep, you can now begin to correct those associations, as described in Chapter 4. Once excessive feedings are no longer complicating the picture, the rest of the relearning process usually happens quickly.
Even if you continue to nurse your child to sleep at bedtime and nap time, you may find that if you just eliminate the middle-of-the-night feedings, she will still be able to put herself back to sleep after waking during the night. That is fine, as long as it’s working well. But if she isn’t adjusting to this pattern—if it still takes a long time to transfer her from your arms to the crib or mattress, or if she wants to be nursed whenever she wakes during the night—then you must take more care to clearly separate the bedtime feeding from the act of falling asleep. Note carefully when she is getting close to falling asleep. Stop feeding her at that point, and put her to bed; wake her a little if necessary, so that she will be aware of being moved. Or move the final feeding a little earlier, so that she will definitely still be awake when you put her to bed.
A schedule with one or two nighttime feedings is a little more unstable than one with no feedings, because it means that sometimes your child gets fed before she goes back to sleep during the night and sometimes she doesn’t. If she has been waking once a night for a feeding, she may begin waking twice a night, and if you feed her at that second waking, she may begin waking three times a night. You can prevent this regression by sticking to a maximum number of feedings and a minimum time between feedings and, if necessary, by making certain that after she feeds she is always put to bed awake.
Some families find a slightly different approach helpful in cutting out unnecessary bottle feedings. Rather than spacing out the feedings and making them smaller, they progressively dilute the contents of each nighttime bottle until their baby is just getting water. For instance, on the first night, instead of full-strength milk (or formula or juice), use a three-quarter-strength mixture—three parts milk (or formula or juice) to one part water. Dilute the bottle further every night or two, to half-strength, one-quarter-strength, and then one-eighth-strength. Now, assuming your child is drinking the same number of ounces of fluid as before, she is getting only an eighth of the amount of milk she started with. The next night, give her just water. Now she is not being fed at all during the night. Since she is taking only water, the nutritionaleffects are no longer important. She may still be wetting at night, but she probably won’t feel hungry. Now the bottle is only being used as a pacifier, so you can stop using it the next night altogether. Help her learn to fall asleep without sucking, along with any other remaining inappropriate associations, by following the methods described above and in Chapter 4.
If you use this approach, stick to the concentration you offer each night, even if your child complains, and don’t give in to demands for larger or more frequent feedings. Some children take the diluted milk without complaint; others complain considerably or refuse to take it at all. If she won’t take the bottle, she probably isn’t very hungry, and she will give up the extra feeding that much quicker. You can simply look in on her at increasing intervals; if she decides she wants the bottle after all, she can still have it. If you find this approach too difficult for your child, use the other approach of spacing out the feedings and making them smaller instead.
We used the methods described in this section with Kayla and Allison, and both girls soon started sleeping soundly through the night. Allison gave up the bottle within a week after the treatment began. Her mother followed the program of progressively spacing out feedings and decreasing the amount of milk in each bottle, and she was surprised how quickly Allison’s nighttime behavior improved. Allison did cry a little when her nighttime bottle was taken away altogether, but only for two nights and only for five minutes each time. Her parents can now enjoy their time together in the evenings, and they can sleep through the night again.
Kayla’s mother continued to nurse her twice a day, but never at night. She occasionally nursed Kayla to sleep at nap time, because she found that it did not seem to affect the good nighttime habits they had established, and because she still found it rewarding and pleasurable. Kayla’s father came to understand that he had been wrong to insist that his wife get up to nurse throughout the night, and the tension between the parents eased.
Other Points to Keep in Mind
Eliminating feedings at night may or may not lead to weaning. If your child always drinks from a cup except at bedtime, at nap time, and during the night, you will be weaning her altogether if you discontinue all the sleep-time feedings. On the other hand, if she is not ready to be weaned, or if you do not want to wean her yet, you can still eliminate feedings during the night. Simply continue nursing or bottle-feeding her at other times as you always have.
Decreasing nighttime feedings generally won’t affect your child’s daytime feedings much, unless she has been getting a significant part of her nourishment at night. In that case, you will probably notice that over several weeks she gradually feeds more during the day as her patterns of hunger and satiation change.
Feeding your child at appropriate intervals during the day will not interfere with her sleep at night or during naps. After about the age of two months, though, your baby’s nighttime sleep may be affected if she is given a bottle or put to the breast whenever she seems the least bit upset, fussy, or demanding, even though it is clear to you at these times that she is not hungry and eats very little. Learning to associate the breast or bottle with a feeling of comfort is important, but it will become a problem if your child never learns to be comforted any other way. If you find that you are using the breast or bottle as a pacifier too frequently during the day, consider offering them less often and less quickly. (Of course, you should not withhold feedings during the day when she actually is hungry, needs to be fed, and takes more than an ounce or two before being satisfied.) Your goal is to help your child learn other ways to calm herself, so that she will begin to associate the breast or bottle mainly with hunger and feedings. Once you have seen that your child can accept these changes without lasting frustration—on the contrary, she will probably be happier in the daytime—you should be able to work on the nighttime changes more easily and with new confidence.
Feedings in relation to naps can be handled in any of several different ways. You can leave them unchanged, as long as your child falls asleep easily while feeding, can be transferred out of your arms easily and without waking, and finishes her nap without needing to feed again. If you are trying to separate feeding from falling asleep, you can (if you choose) make the separation clear at nap times as well as at night. But if you put her to bed awake at nap time, it is reasonable to have a time limit: if she has not fallen asleep after thirty minutes of checking, pick her up and end the nap for that day. She may later fall asleep on her own in another room; that’s fine as long as she does so without being fed. Alternatively, you can make the separation (between feeding and falling asleep) only at night to begin with, and once your child has learned how to fall asleep at night without feeding, you can start to do the same thing at nap time, asking her to do during the day what she has already learned to do at night.
Medical Considerations
You should always avoid feeding your child when she is lying in her bed or crib, even if sleep disruptions aren’t a problem. Simply handing a bottle to a child lying supine is a way to cause ear and dental problems. Because the eustachian tube (a small passageway to the throat that vents or drains the middle-ear cavity) is short and horizontal in young children, liquid—and bacteria—can easily pass from the throat to the middle-ear space if a child sucks on a bottle while lying on her back. The result can be a middle-ear infection, otitis media. Also, once your child’s teeth erupt, she is at risk for tooth decay if she goes to sleep with milk or juice in her mouth, and this is just what happens when she falls asleep with a bottle in her mouth.