Giuseppe De Luca
Salvatore Cassese
Paolo Marino
This chapter deals with the clinical presentation and evaluation of chest pain in the intensive care unit (ICU). Please see Chapters 119 and 120 for a full discussion of non–ST-segment elevation myocardial infarction and ST-segment elevation myocardial infarction.
Evaluation of Chest Pain
Immediate Concerns
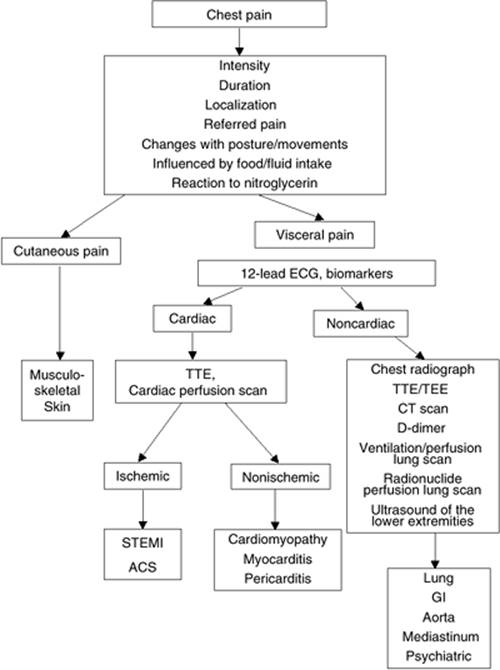
Despite insights and innovations over the last decades, acute nontraumatic chest pain still represents one of the most difficult diagnostic challenges in medicine. In fact, it is commonly observed in several life-threatening illnesses, including cardiovascular, pulmonary, and gastrointestinal diseases and, when symptoms are atypical, it may be difficult to interpret (Table 118.1) (1). Algorithms have been proposed to improve the accuracy of diagnosis and the patient's risk stratification via the integrated use of clinical data, biomarkers, and noninvasive diagnostic tests (2,3) (Fig. 118.1).
Main Tips
When confronted with a patient suffering from acute chest pain:
1. First, exclude major life-threatening processes, such as myocardial infarction, pulmonary embolism (PE), or aortic dissection.
2. Obtain a careful history and perform a meticulous physical examination, particularly in patients with atypical chest pain, which is commonly seen in the emergency department (Table 118.2).
3. Use this information to select the most appropriate tests or procedures needed to confirm or reject the suspected diagnosis.
Clinical Evaluation
The evaluation of patients with acute chest pain should include the following.
History
1. Symptoms and description of the current illness: The patient should be allowed to describe the character (pressure, sharp, burning, pleuritic), duration (minutes, hours, days), intensity (scale of 0–10), location, radiation, and onset (sudden, gradual) of the pain. Associated symptoms and signs such as nausea, vomiting, diaphoresis, dyspnea, presyncope, and syncope should be noted. Factors that worsen or relieve the symptoms should be obtained (Table 118.2).
2. Past medical history: A thorough investigation on history of cardiopulmonary and gastrointestinal disease is mandatory (Table 118.1).
3. Family history: A family history of glucose intolerance, coronary artery disease, and sudden or premature death should be investigated.
4. Social history: A history of alcohol, cigarette, cocaine, or other drug use should be sought.
Physical Examination
1. Vital signs: Changes in heart rate, blood pressure, pulse pressure, pulmonary artery waveforms and pressure, ventilatory parameters, temperature, and urine output should be noted.
2. Inspection and palpation: Examination of the head, neck, chest, and abdomen may reveal significant disease. Disrobe the patient and visually inspect for obvious deformities and asymmetry. Significant point tenderness and crepitation should be sought by applying firm pressure to the anterior, lateral, and posterior chest wall. Cardiac impulses may reveal significant underlying disease. Palpate and note the symmetry of all upper and lower extremity pulses. Palpation of the abdomen for tenderness and pulsatile masses is vital in making the diagnosis of thoracic and intra-abdominal disease.
3. Auscultation: The neck should be auscultated to evaluate for the presence of significant upper airway obstruction (stridor). Careful auscultation of the chest should assess symmetry of breath sounds. Abnormal sounds (i.e., rales, wheezing, rhonchi, friction rubs) and their location should be noted. Heart sounds should be carefully studied. The cardiac rate and rhythm should be noted. Close attention to findings suggestive of valvular heart disease is important. The abdomen should be auscultated, and the presence and quality of bowel sounds should be noted.
|
Table 118.1 Differential diagnosis of chest pain |
|
|
Diagnostic Tests for Acute Chest Pain
1. Electrocardiogram (ECG): An electrocardiogram should be obtained as soon as possible, particularly in patients with persistent chest discomfort at the time of evaluation. Nondiagnostic ECG changes (i.e., old left bundle branch block) or a normal ECG may neither prove nor disprove significant cardiac ischemia. Right axis deviation, right bundle branch block, and inversion of T waves in chest (V-) leads may be observed in acute pulmonary embolism. Diffusely concave ST-segment elevation or inversion of T waves may be observed in patients with pericarditis.
2. Biomarkers
A. Markers of myocardial injury: Several markers are currently available that allow accurate identification of patients with myocardial injury. Cardiac troponin I and T represent a more accurate and sensitive marker of myocardial injury (3,4). It is imperative to consider that a single negative troponin assay at the time of a patient's admission cannot always be relied upon to exclude myocardial infarction. In this setting, it is recommended to repeat the test 6 to 12 hours after admission and after any further episode of chest pain. Myoglobin might be considered between 2 and 6 hours from symptom onset, as compared to creatine kinase (CK)-MB mass and troponin, but the maximal negative predictive value of myoglobin reaches only 89% during this time frame (5). Elevation of troponin may be observed also in patients with acute pulmonary embolism, where it correlates well with the extent of right ventricular dysfunction and prognosis (6,7,8), and in patients with myocarditis, pericarditis, or acute heart failure (4).
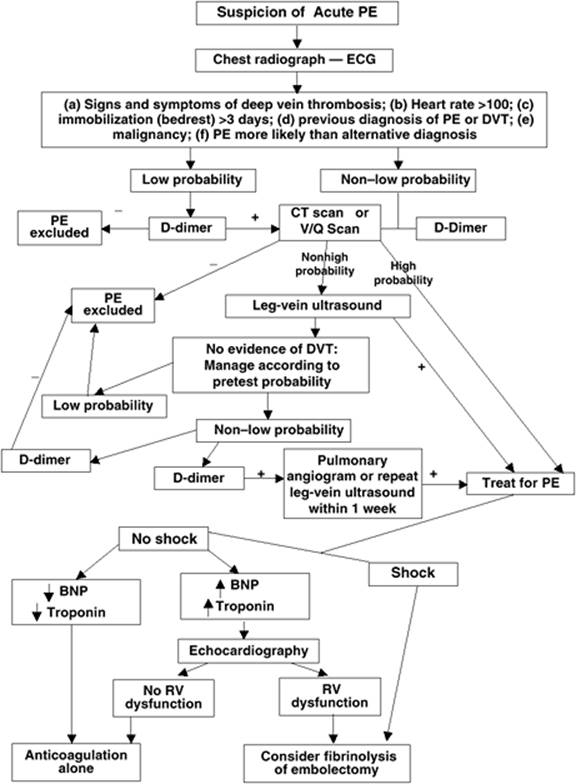
B. Natriuretic peptides: Cardiac natriuretic peptides are useful diagnostic and prognostic markers for patients with heart failure (8,9). Similar to cardiac troponin, elevations in brain natriuretic peptide (BNP) and in N-terminal proBNP (the prohormone) are associated with right ventricular dysfunction in acute pulmonary embolism, and may help to identify a subgroup of hemodynamically stable patients at especially high risk for adverse clinical events (8) (Fig. 118.2).
C. D-dimer: Fibrin d-dimer (DD) has been proposed as a diagnostic tool in patients with suspected pulmonary thromboembolism (Fig. 118.2) (10). In fact, the dimeric d-domain serves as an indicator of in vivo fibrin formation. However, many conditions are associated with fibrin formation:
· Nonpathologic: Cigarette smoking, aging, functional impairment, pregnancy, and postoperative state
· Pathologic: Trauma, pre-eclampsia, malignancy, infection, disseminated intravascular coagulation, arterial or venous thromboembolism, atrial fibrillation, acute coronary syndromes, stroke, and acute upper gastrointestinal hemorrhage
Because of this low specificity, DD testing may not be helpful in hospitalized patients in whom comorbidities are common. In addition, DD assays (especially qualitative latex agglutination assays) are not 100% sensitive, limiting their utility as a single screening test.
3. Imaging techniques:
A. Echocardiography: The echocardiogram plays an important role in evaluating chest pain and is frequently used to diagnose regional wall motion abnormalities, aortic stenosis, dissecting aortic aneurysm, pericardial effusion, and cardiac tamponade. Preserved regional wall motion occasionally occurs early in the process of significant cardiac ischemia. Contrast echocardiography may further improve diagnostic accuracy in the evaluation of acute chest pain (11). Transesophageal echocardiography (TEE) has a sensitivity approaching 100% for aortic dissection (12).
B. Radionuclide myocardial perfusion imaging: Tc-99m–based tracers have been shown to be highly sensitive in the detection of myocardial infarction, although somewhat less specific. However, data acquisition in a gated mode for additional wall motion score information results in a significant increase in specificity (13). The most suitable population for this method are patients judged at low to intermediate probability of having myocardial ischemia, with an atypical chest pain and a normal or nondiagnostic ECG (14,15).
|
|
|
Figure 118.1. Diagnostic flow chart in patients with chest pain. ECG, electrocardiogram; TTE, transthoracic echocardiography; TEE, transesophageal echocardiography; CT, computed tomography; STEMI, ST-segment elevation myocardial infarction; ACS, acute coronary syndrome; GI, gastrointestinal. |
C. Chest radiography: The chest radiograph may provide important clues regarding the cause of chest pain. The presence or absence of the following radiographic abnormalities should be determined: subcutaneous air, rib fractures, pneumothorax, pulmonary infiltrates, widened mediastinum, pleural effusions, and intraperitoneal free air.
|
Table 118.2 Clinical features of chest pain according to the etiology |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
D.
|
|
|
Figure 118.2. Algorithm on diagnosis and management of patients with acute pulmonary embolism (PE). ECG, electrocardiogram; DVT, deep vein thrombosis; CT, computed tomography; V/Q, ventilation/perfusion; BNP, brain natriuretic peptide; RV, right ventricle. |
E. Radionuclide perfusion lung scan: Intubated patients or patients too ill for transport who are believed to have PE may undergo bedside perfusion lung scanning. Whereas this test is often nondiagnostic, a normal scan result is a sensitive negative predictor for the presence of pulmonary emboli. This test is no longer a principal diagnostic test in PE, being supplanted by computed tomography (CT) scan, unless patients are too unstable for transportation.
F. Radionuclide ventilation/perfusion ([V with dot above]/[Q with dot above]) lung scan: Normal- and high-probability findings on [V with dot above]/[Q with dot above] scan often are sensitive enough to dictate therapy without further evaluation. Patients with low- and intermediate-probability [V with dot above]/[Q with dot above] scan results, depending on the level of clinical suspicion, frequently require additional examinations (see Chapter 144). This is no longer a principal diagnostic test in PE, being supplanted by CT scan. It is usually reserved for patients with renal insufficiency, contrast allergy, or pregnancy (because of lower radiation exposure as compared to CT scan).
G. Duplex ultrasound of the lower extremities: Venous ultrasonography is useful if it demonstrates deep venous thrombosis (DVT) in patients with suspected PE. However, the majority of patients with PE have no imaging evidence of DVT. Therefore, if clinical suspicion of PE is high, patients without evidence of DVT should still be investigated for PE.
H. CT scan: It is readily available in most emergency departments, and performed rapidly. It may help in challenging cases when the chest radiograph is not conclusive (e.g., pneumothorax). Furthermore, CT angiography scan may evaluate coronary, aortic, and pulmonary anatomy with great clarity. Several studies have shown that 64-slice computed tomography coronary angiography is very accurate in the diagnosis of coronary artery disease (16). The multidetector CT seems at least as good as stress nuclear imaging for the detection and exclusion of an acute coronary syndrome in low-risk chest pain patients (17). A recent large study has shown that CT scan is effective in the evaluation and management of patients with clinically suspected pulmonary embolism (18). In cases of acute aortic syndromes, in addition to making the initial diagnosis, CT angiography can assess the extent of aortic involvement and depict involvement of visceral and iliac arteries. The average sensitivity exceeds 95%, with specificities of 87% to 100%, and may be more accurate than magnetic resonance imaging (MRI) or TEE in the detection of aortic arch vessel involvement (19).
I. Gadolinium-enhanced magnetic resonance angiography (MRA): Despite the high accuracy for the detection of coronary artery disease, acute aortic dissection, and PE (16,20) and the clear advantages due to the fact that this examination does not require ionizing radiation or use of iodinated contrast agents, MRA is currently used as a second-line diagnostic study when a first imaging study is not adequate or the true diagnosis remains uncertain. The reasons include the limited availability of MRI, especially on an emergency basis, and the issues surrounding patient inconvenience and limited applicability (MRI cannot be performed on patients with claustrophobia, pacemakers, aneurysm clips, or other metal devices).
Chest Pain Syndromes
Pinpointing the origin of chest pain is often problematic because nociceptors from within the myocardium, aorta, pleura, lungs, and esophagus traverse a common neuronal pathway to the cortex (21). Structures within the thorax that are relatively insensitive to pain include the lung parenchyma and visceral pleura. The parietal pleura, upper airways, musculoskeletal structures of the upper torso, diaphragm, and mediastinal structures respond to trauma and inflammation with pain impulses. Diabetic neuropathy, differing pain thresholds, medications, and varying levels of consciousness all may greatly influence a patient's description of the chest pain.
Classic Chest Pain
Certain disease processes are associated with characteristic pain patterns (Table 118.2). For example, an inflammatory process involving the pleural surfaces of the lungs or heart may produce pleuritic chest pain. This type of pain is described as a sharp, scratchy, or catch-like discomfort. Pneumonia, PE, and pericarditis produce inflammatory processes with this type of pain. Patients who describe their chest discomfort as retrosternal, squeezing, pressure-like, or heavy in nature often are diagnosed with myocardial ischemia (22,23). One of the most dramatic presentations of chest pain is that of acute aortic dissection. Patients frequently describe an excruciating, sharp, knifelike retrosternal pain radiating to the back. The evaluation of patients presenting with classic chest pain syndromes should be directed to specifically confirm or exclude the suspected diagnosis.
Atypical Chest Pain
As shown in Figure 118.1, the approach to patients with chest pain can be systematic and organized. Musculoskeletal or cutaneous causes of atypical chest pain should be excluded. An ECG and cardiac enzymes should thus be obtained. If the index of suspicion for cardiac ischemia is high, irrespective of the ECG and cardiac enzymes, one should proceed with further studies to either confirm or negate the suspected diagnosis. If the index of suspicion for cardiac ischemia is low, causes of chest pain such as PE, aortic dissection, pleural inflammation, pneumothorax, and gastroesophageal disease should be considered. If the ECG reveals new ischemic changes, one may assume that this is the primary cause of the patient's discomfort. Many patients in the adult ICU have significant undiagnosed coronary artery disease. An echocardiogram, unless the result is totally normal, usually is not sensitive enough to exclude acute and significant cardiac ischemia. Stress echocardiography, nuclear medicine studies, angio-CT, and, finally, cardiac catheterization may be necessary under these circumstances. The urgency with which to pursue these tests depends on the acuity of illness.
Life-threatening Causes of Chest Pain
Differential Diagnosis: Pulmonary Causes of Chest Pain
Pulmonary Embolism
Approximately 200,000 patients die yearly from PE. The mortality of untreated PE is five times greater than treated cases (24). The multiple factors that appear to predispose to pulmonary thromboembolism are detailed in Table 118.3. The signs and symptoms of PE have been well described (25). The clinical presentation of acute PE includes the following:
· Abrupt onset of dyspnea
· Chest pain unrelieved with nitroglycerin
· Apprehension
· Tachypnea
· Diaphoresis
· Fever
· Tachycardia
· Increased P2
· Dyspnea at rest
· Thrombophlebitis of the lower extremity
· Decreasing PaO2
The most common complaint is the sudden onset of pleuritic chest pain; nonpleuritic discomfort occurs less frequently. Approximately 84% of patients complain of dyspnea, and apprehension, cough, and hemoptysis are noted in 50% of patients. Syncope may also be a presenting sign.
On physical examination, most patients have tachycardia and tachypnea. Fever is seen in nearly half of affected patients. Patients with large or multiple emboli often have evidence of hypoperfusion. A narrowed pulse pressure, poor peripheral perfusion, hypotension, low urine output, and mental status changes are common signs of hypoperfusion. Once a suspicion of PE is entertained, one should proceed with further diagnostic studies (Fig. 118.2) (26,27,28) (see Chapter 144).
|
Table 118.3 Predisposing factors to acute aortic syndrome, pulmonary embolism, and acute coronary syndrome |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Pneumothorax
Pneumothorax, a common entity in the ICU setting, is an abnormal collection of air between the parietal and visceral pleurae, which may be, if undiagnosed, rapidly fatal. Pneumothoraces are either spontaneous, traumatic, or iatrogenic. Irrespective of the etiology, a pneumothorax can have a significant impact on oxygenation and hemodynamics. The array of clinical presentations ranges from mild pleuritic chest pain with the sensation of shortness of breath to cardiac arrest. The clinician should look for the following signs and symptoms when pneumothorax is suspected:
· Tachypnea
· Dyspnea at rest
· Dyspnea with exertion
· Localized decrease in breath sounds
· Unilateral hyperresonance to chest percussion
· Dyspnea of abrupt onset
· Increased peak airway pressure
· Sudden hemodynamic instability
· Arterial desaturation
Patients are often apprehensive and demonstrate tachypnea and tachycardia. Auscultation and percussion of the chest often reveal decreased breath sounds and hyperresonance of the affected side. Tracheal deviation, jugular venous distention, hypotension, and shock are indicators of an immediate life-threatening process (tension pneumothorax). A chest radiograph should be obtained in the relatively stable patient believed to have a pneumothorax. Expiratory radiographs increase the likelihood of visualizing a small pneumothorax. Chest radiographs are usually diagnostic when the lung parenchyma is normal. The diagnosis of tension pneumothorax should ideally be made clinically, and the pneumothorax evacuated without waiting for results of a chest radiograph.
Patients who are critically ill and undergoing mechanical ventilation are at risk for a pneumothorax. Such patients may have increased peak airway pressures, arterial desaturation, and increased oxygen extraction. Despite sedation, some patients may become agitated and diaphoretic. Compression of the mediastinal structures with a subsequent decrease in preload may result in a significant decrease in the cardiac output and hemodynamic instability. If a ball-valve mechanism occurs during positive-pressure ventilation, a life-threatening tension pneumothorax may rapidly develop.
A pneumothorax in a patient with severe underlying pulmonary disease may be extremely difficult to diagnose (29,30). Loculated pneumothoraces are frequently missed on portable radiographs of critically ill patients. Once suspected, this diagnosis must be confirmed or negated, as nearly half of all untreated pneumothoraces progress to tension pneumothorax. In these circumstances, a CT scan of the chest often is necessary to make the diagnosis.
Differential Diagnosis: Cardiovascular Causes of Chest Pain
Acute Aortic Syndrome
Acute aortic syndrome is the modern term that includes aortic dissection, intramural hematoma (IMH), and symptomatic aortic ulcer (12). Clinical manifestations, etiology, and treatment can be readily differentiated by using the Stanford or DeBakey classification of aortic dissection. Due to new studies demonstrating that intramural hemorrhage, intramural hematoma, and aortic ulcers may be signs of evolving dissections or dissection subtypes, a new system of differentiation has been proposed (Table 118.4).
|
Table 118.4 Proposed classifications of aortic dissection |
|||||||||||||
|
Among several factors (Table 118.3), the most common risk condition for acute aortic syndromes is hypertension, with chronic exposure of the aorta to high pressures leading to intimal thickening, fibrosis, calcification, and extracellular fatty acid deposition.
Patients complain of the sudden onset of excruciating chest discomfort. This discomfort is sharp and tearing in nature, radiating to the back, abdomen, and extremities. Syncope, diaphoresis, and generalized weakness may occur. Patients may have evidence of shock with mental status changes, cool clammy skin, low urine output, hypertension or hypotension, and lactic acidosis. The clinical presentation of acute aortic syndromes may include the following signs and symptoms:
· Abrupt onset
· Maximal severity at onset
· Knifelike or tearing substernal chest pain
· Severe back pain
· Chest pain unrelieved by nitroglycerin
· Fever
· Tachycardia
· Elevated diastolic blood pressure
· Diaphoresis
Untreated acute aortic dissection is associated with a 50% mortality within the first 48 hours.
Classic Aortic Dissection
Acute aortic dissection is characterized by the rapid development of an intimal flap separating the true and false lumens (12,31). The dissection can spread from the intimal tear in an antegrade or retrograde fashion, often involving side branches and causing malperfusion syndromes, tamponade, or aortic insufficiency (12,32). Once a patient survives to hospital discharge, further prognostic stratification based on clinical and imaging parameters is challenging. Spontaneous false lumen thrombosis (better prognosis), evidence of persistent communication, and/or a patent false channel (worse prognosis) may be used to estimate late risk of expansion (12,33,34).
Type A dissections are most often seen in young patients with Marfan syndrome or cystic medial necrosis. Upper extremity weakness, diminished or loss of upper extremity pulses, asymmetric upper extremity blood pressure, hemiplegia, Horner syndrome, recurrent laryngeal nerve damage, hemopericardium, and cardiac tamponade all are associated with type A dissections. Acute aortic valvular insufficiency and dissection of the coronary artery ostium resulting in an acute myocardial infarction may occur. A prominent diastolic murmur of aortic insufficiency and congestive heart failure may be present. Type B aortic dissections are usually seen in older patients with a history of hypertension and atherosclerosis. Paresthesias, weakness, and pain of the lower extremities may result from compromised blood flow to the spinal arteries, iliac arteries, or both. Diminished or unequal lower extremity pulses and pressures relative to the upper extremities also are suggestive of distal dissection of the aorta. Manifestations of mesenteric and renal ischemia may occur (35).
The radiographic data suggestive of a type A dissection include a widened superior mediastinum and left pleural effusion. Chest radiographs of type B dissections are usually unrevealing. One may, however, see a widened descending aorta relative to the ascending aorta. When a dissection is suspected, immediate surgical consultation is required and a rapid diagnosis is warranted. The CT scan, MRI, and TEE are sensitive and specific (36,37,38).
Surgery is the preferred approach in case of proximal dissection, whereas medical therapies, including sodium nitroprusside, β-blockers or labetalol, and morphine, may be preferred in distal dissection. However, it is important to monitor the patient vigilantly for any evidence of branch arterial compromise, with the most lethal consequence being mesenteric ischemia.
Intramural Hematoma
Aortic IMH is considered a precursor of dissection, originating from ruptured vasa vasorum in medial wall layers and resulting in an aortic wall infarct that may provoke a secondary tear, causing a classic aortic dissection. It is similar to classic dissection in its natural history in that IMH may extend, progress, regress, or reabsorb. Whereas IMH resorption has been reported in about 10% of cases, resorption of aortic dissection has rarely been so reported (12,39,40). Most IMHs (50%–85%) are located in the descending aorta and are typically associated with hypertension (41,42). Although clinical manifestations of IMH are similar to acute aortic dissection, IMH tends to be a segmental process; therefore, radiation of pain to the head or legs is less common. Chest pain is more common with ascending (type A) IMH; upper or lower back pain is more common with descending (type B) lesions. Nonetheless, the diagnosis of IMH versus acute aortic dissection cannot be made clinically. IMH is a tomographic imaging diagnosis in the appropriate clinical setting. These patients should be managed as those with classic aortic dissection.
Plaque Rupture/Penetrating Atherosclerotic Ulcer
Deep ulceration of atherosclerotic aortic plaques can lead to IMH, aortic dissection, or perforation (43,44,45,46). Noninvasive imaging has further elucidated this disease process that often further complicates IMH and appears as an ulcer-like projection into the hematoma. In association with IMH, limited series have reported penetrating atherosclerotic ulcers almost exclusively in patients with type B IMH (46). Symptomatic ulcers with signs of deep erosion are more prone to rupture than others. In these patients, endovascular stent grafting is emerging as an attractive therapeutic modality.
Acute Pericarditis
Acute pericarditis is an inflammatory process of the pericardium caused by a variety of disorders. It is the most common disease of the pericardium. Pericarditis is commonly caused by infection, trauma, autoimmune disease, or neoplasm (see Chapter 127).
The diagnosis of acute pericarditis is established by the presence of chest pain, pericardial friction rub, and ECG abnormalities. A more complete list of the clinical features of acute pericarditis is as follows:
· Chest pain at rest
· Exacerbation of chest pain with breathing
· Chest pain lasting longer than 20 minutes
· Chest pain unrelieved with nitroglycerin
· Fever; sinus tachycardia
· ST-segment elevation without reciprocal depression
· Inverted T waves
· Pericardial friction rub
· Leukocytosis
Pericardial effusions of various sizes are seen by echocardiography (47). The pain of acute pericarditis is pleuritic in nature and often is described as a sharp, retrosternal discomfort radiating to the back and shoulders. This pain is relieved by leaning forward and worsened by recumbency, inspiration, and cough. The chest pain of acute pericarditis may be bandlike with radiation to the arms, similar to that of a myocardial infarction.
Pathognomonic for acute pericarditis is a three-component friction rub that is heard best over the left sternal border with the patient sitting upright and leaning forward. It is high pitched and scratching in nature. The rub is often transitory and may be confused with aortic stenosis or mitral regurgitation; careful auscultation of the early diastolic component makes the distinction. In the absence of a large pericardial effusion, subepicardial inflammation often yields a classic triphasic ECG. In the acute stages, one may see diffuse ST-segment elevation with concurrent PR depression in the limb and precordial leads. At 24 to 48 hours, ST and PR segments normalize; however, diffuse T-wave inversion occurs. The T-wave abnormalities subsequently resolve with time. Because there may be elevation of cardiac enzymes, the distinction between myocardial infarction and pericarditis may be difficult initially. Sequential ECGs demonstrating concave morphologic features of the ST segments and absence of Q waves are suggestive of pericarditis. With the development of a large pericardial effusion, reduced QRS voltage, oscillatory voltage pattern, and atrial arrhythmias are sometimes present (48,49).
|
Table 118.5 Diagnostic tests for acute pericarditis |
||||||||||||||||||||
|
Most patients who are diagnosed with acute pericarditis have an uneventful recovery with bedrest and anti-inflammatory drug therapy. However, a substantial number of individuals have persistent chest discomfort, fever, leukocytosis, generalized illness, or hemodynamically significant pericardial effusions. In these patients, aggressive diagnostic strategies including pericardiocentesis are warranted (Table 118.5). Despite an aggressive search, a diagnosis is obtained in only approximately 20% of cases (50,51).
Cardiac Ischemia
An imbalance between myocardial oxygen supply and demand is the basic pathophysiologic process for a variety of disease entities. Myocardial infarction, myocardial ischemia, aortic stenosis, hypertrophic cardiomyopathy, right ventricular hypertension, and severe anemia all are associated with the development of such an imbalance. The distinction between these disease processes is made by medical history, symptoms, physical examination, ECG, cardiac enzymes, chest radiographs, and other related studies.
Acute Coronary Syndrome (see below and Chapters 121 and 122)
ST-segment Elevation Myocardial Infarction (see Chapter 122)
Aortic Stenosis
Aortic stenosis is a narrowing of the aortic valve orifice secondary to congenital abnormality, valvular degeneration (calcific), or rheumatic heart disease (see Chapter 125). Discomfort associated with aortic stenosis mimics typical angina pectoris. The clinical presentation of aortic stenosis includes the following:
· Exertional dyspnea
· Chest pain at rest
· Heart gallop
· Forceful localized apical impulse
· Murmur of aortic stenosis
· Decreased aortic component of S2 or presence of S4
· Left-axis deviation on ECG
· Left ventricular hypertrophy on ECG
Although the syndrome of chest pain in patients with aortic stenosis is anginal, only 40% of such patients have coronary artery disease. The remaining patients develop ischemia secondary to altered perfusion pressures within a hypertrophied ventricle (52). The diagnosis of aortic stenosis is based on symptoms, with confirmation by echocardiography, coronary angiography, or both; heart catheterization with left ventricular and aortic pressure gradient is also a diagnostic tool. Patients with severe aortic stenosis—less than 1.0 cm3 valve area—who develop chest pain and hypotension are at a high risk of immediate death and require aggressive management.
Differential Diagnosis: Gastrointestinal Causes of Chest Pain
Unless chest pain is related to obvious life-threatening gastrointestinal disease, many patients initially undergo an evaluation for myocardial ischemia. Most patients with severe gastrointestinal disease have a prior history of gastroesophageal reflux, peptic ulcer disease, caustic ingestion, forceful vomiting, or recent instrumentation.
Esophageal Injury and Rupture
Most causes of esophageal injury are suggested by history. Patients who attempt suicide by ingesting lye or other caustic agents may have obvious injury to the oropharynx. In this circumstance, emergency endoscopy may be warranted. Less obvious causes of chest pain related to esophageal injury include mucosal damage by ingested pills or the presence of pill fragments lodged in the distal esophagus. Occasionally, nasogastric tubes have been found to be the culprit of significant esophageal trauma with resultant chest pain.
Acute increases in intra-abdominal pressure secondary to vomiting, heavy lifting, trauma, or straining during defecation have been associated with esophageal wall tear and rupture. Without a preceding event, making the diagnosis is extremely difficult because this process may easily mimic myocardial infarction, pneumothorax, or esophageal spasm. Undiagnosed esophageal rupture may result in life-threatening mediastinitis. The diagnosis of a nonperforating esophageal injury is frequently obtained by upper endoscopy. The presence of subcutaneous emphysema, pleural effusion, or mediastinal air on chest radiograph is suggestive of esophageal perforation. This may be confirmed by barium or water-soluble contrast studies of the entire esophagus (see Chapter 160).
Esophageal Spasm
Esophageal spasm is a motility disorder characterized by abnormal lower esophageal sphincter tone. Phasic propulsive contractions cause diffuse spasm of the esophagus. These spasms are associated with substernal chest pain that is squeezing in nature and may occur with exercise, thus making this disorder difficult to distinguish from angina pectoris. Unlike angina pectoris, the discomfort is often induced by very hot or cold liquids. Dysphagia with liquid and solid food may accompany the discomfort.
Once this disease entity is considered, a variety of tests can aid the clinician in establishing the diagnosis. Esophageal scintigraphy, esophageal manometry, and provocative tests all have been used.
Nonlife-threatening Causes of Chest Pain
Costochondritis
Inflammation of the costochondral joints frequently results in chest wall pain. This pain is exacerbated by applying pressure over the affected area, by deep breathing, or by coughing. Often, patients can point to the exact area of inflammation.
Herpes Zoster
Reactivation of latent varicella-zoster virus with subsequent posterior root neuronal viral replication and inflammation can result in severe chest pain. This process can be triggered by trauma, surgery, immunosuppression, and a multitude of other immunologic stresses. The distribution of pain is usually along a particular dermatome, with eventual eruption of vesiculopustules on an erythematous base. The Tzanck test demonstrating multinucleated giant epidermal cells is diagnostic.
Asthma and Chronic Obstructive Lung Disease
A well-known association exists between atypical chest pain and obstructive lung disease. Patients describe a variety of symptoms ranging from sharp stabbing discomfort to pressure-like sensations. Bronchodilators may provide relief in some patients.
Psychosomatic Chest Pain
Psychosomatic chest pain is a diagnosis of exclusion. Patients may present with either classic or atypical symptoms. Significant coronary artery disease is frequently excluded by coronary angiography. Many of these patients have clinical depression and need aggressive intervention.
Summary
The evaluation of patients with chest pain should be organized and proceed rapidly in logical sequence. The evaluation should include a review of the patient's past medical history, history of present illness, risk factors, and a detailed physical examination. This initial evaluation should narrow the differential diagnosis and direct the clinician so that appropriate tests or procedures are performed.
Evaluation of Acute Coronary Syndromes
Immediate Concerns
Acute coronary syndrome (ACS) is a broad term that encompasses a range of acute manifestations of coronary atherosclerosis, including ST-segment elevation myocardial infarction (see Chapter 122), non–ST-segment elevation myocardial infarction (N-STEMI), and unstable angina (UA) (see Chapter 123). The diagnosis and the optimal treatment of these patients may be associated with significant improvement in outcome and survival. We focus on patients with UA/N-STEMI, although, as noted above, there are separate chapters within this textbook that will deal with these topics in detail.
Main Tips
When confronted with a patient suffering from acute coronary syndrome (UA/N-STEMI):
1. Obtain a careful history and perform a meticulous physical examination (Table 118.1), particularly in patients with atypical chest pain, which is commonly seen in the ICU, to exclude:
· Noncardiac causes of chest pain
· Nonischemic cardiac disorders (pericarditis, valvular disease)
· Precipitating extracardiac causes (anemia)
· Signs of potential hemodynamic instability
2. Monitor ECG and repeat marker of myonecrosis if initially negative (at least 6 hours after initial measurement).
3. Perform echocardiography to identify regional dysfunction and/or nonischemic disorders.
4. After confirmation of the diagnosis, start medical therapy as soon as possible.
5. Risk stratification: high-risk patients may benefit from aggressive antiplatelet therapy and early angiography and revascularization.
Clinical Evaluation
Patients with acute coronary syndromes should undergo rapid and accurate evaluation (see Chapters 120, 121 and 122). Obtaining a careful history and a meticulous physical examination are mandatory as a guide toward a definite diagnosis, which may influence therapeutic strategies.
Unstable angina is defined as angina pectoris (or equivalent type of ischemic discomfort) with at least one of the three features:
1. Occurrence at rest (or with minimal exertion) and lasting more than 20 minutes (if not interrupted by nitroglycerin)
2. Severe new-onset chest pain (i.e., within 1 month)
3. Occurrence with a crescendo pattern (i.e., more severe, prolonged, or frequent than previously) (53,54)
These symptoms may be associated with ECG changes, such as inversion of T waves or ST-segment depression, and elevation of cardiac biomarkers of necrosis (such as CK-MB or troponin T or I, or both); when this is the case, the condition is defined as non–ST-segment elevation myocardial infarction (53,54). Asymptomatic patients with ECG changes and/or elevation of cardiac enzymes are also included in these categories. ST-segment elevation myocardial infarction is defined as prolonged chest pain at rest (greater than 30 minutes), the presence of ST-segment elevation in the 12-lead ECG (more than 0.1 mV in at least two contiguous peripheral leads or more than 0.2 mV in at least two contiguous chest leads), or new-onset left bundle branch block (see Chapter 122).
The discomfort associated with acute coronary syndromes typically radiates to the left shoulder and the left arm, and may be associated with diaphoresis, nausea, and vomiting. Left ventricular failure—manifested by pulmonary edema and shock—may occur. During attacks, increased heart rate, distant heart sounds, and a diffuse apical impulse may develop. Localized papillary muscle dysfunction may cause the late systolic murmur of mitral regurgitation. The tools for diagnosing the problem include ECG changes during attacks, biomarkers, echocardiography, nuclear medicine scan, exercise stress testing, CT scan, and cardiac catheterization.
Risk Stratification
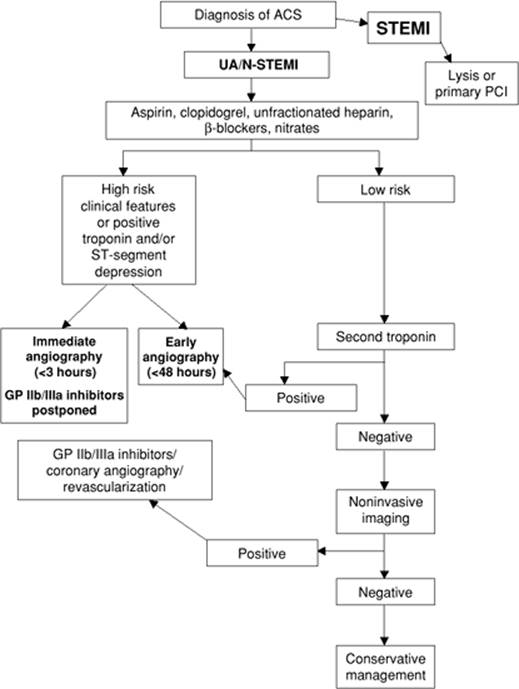
Due to differences in the extent and severity of underlying coronary artery disease, and the different degree of thrombotic risk, identification of high-risk patients is of high clinical relevance in order to prevent, by adequate pharmacologic therapies and mechanical revascularization, the progression and the extent of myocardial infarction and the risk of death (53,54,55). As previously noted, medical history, clinical examination, ECG, and biomarkers provide key elements for risk assessment (Fig. 118.3).
The characteristics of patients with non–ST-segment elevation ACS at high risk for rapid progression to myocardial infarction or death who should undergo coronary angiography within 48 hours include:
· Recurrent rest pain
· Dynamic ST-segment changes: ST-segment depression of more than or equal to 0.1 mV or transient (less than 30 minutes) ST-segment elevation more than or equal to 0.1 mV
· Elevated troponin-I, troponin-T, or CK-MB levels
· Hemodynamic instability within the observation period
· Major dysrhythmias (ventricular tachycardia, ventricular fibrillation)
· Early postinfarction unstable angina (56,57,58,59,60)
Furthermore, the following markers of severe underlying disease (i.e., a high long-term risk) might also be helpful for risk assessment in non–ST-segment elevation ACS:
· Age older than 65 to 70 years
· History of known coronary artery disease, previous MI, prior percutaneous coronary intervention (PCI), or coronary artery bypass grafting (CABG)
· Congestive heart failure, pulmonary edema, and new mitral regurgitant murmur
· Elevated inflammatory markers (i.e., C-reactive protein [CRP], fibrinogen, interleukin (IL)-6)
· BNP or NT-proBNP in upper quartiles
· Renal insufficiency
|
|
|
Figure 118.3. Algorithm on management of patients with acute coronary syndrome (ACS). STEMI, ST-segment elevation myocardial infarction; UA, unstable angina; N-STEMI, non–ST-segment elevation myocardial infarction; GP, glycoprotein. |
The Thrombolysis in Myocardial Infarction (TIMI) risk score has been shown to be an accurate tool for risk stratification that can be easily applied at the bedside of a patient with N-STEMI (61).
Perioperative Management
Cardiac Surgery
Despite improvements in intraoperative myocardial protection, between 5% and 15% of patients undergoing cardiac surgery actually experience a perioperative myocardial infarction due to diffuse atherosclerotic disease of the distal coronary arteries, spasm, embolism, thrombosis of native coronary vessels or bypass graft, technical problems with graft anastomoses, or increased myocardial oxygen need (as in left ventricular hypertrophy).
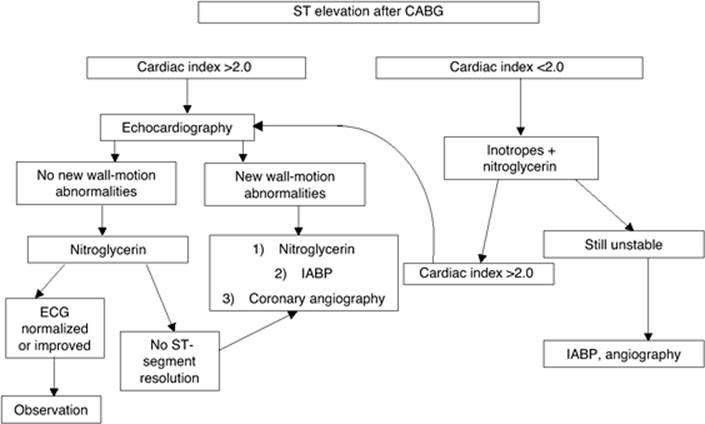
The diagnosis of postoperative MI is difficult because of the nonspecific ST–T-wave abnormalities frequently present in those patients. In addition, troponins are elevated in almost all patients who undergo CABG. A 12-lead ECG should be obtained upon arrival in the ICU after surgery and every 24 hours, since it represents the most reliable tool to diagnose perioperative MI. CK and CK-MB should be evaluated every 8 hours for the first 36 hours, if postprocedural MI is suspected. Bedside echocardiography, by detecting new regional wall motion abnormalities, represents a major diagnostic tool, particularly when ECG and serum marker measurements are unclear. The appropriate management strategy should be defined according to an integrated evaluation of clinical findings and diagnostic tests (Fig. 118.4).
Major Noncardiac Surgery
Myocardial infarction and ischemia occurring during or after major noncardiac surgery are difficult to diagnose, since they are often silent and because of the confounding effects of analgesics and postoperative surgical pain. The diagnosis is often based on evaluation of cardiac troponins, since CK and CK-MB are less specific and may be elevated during aortic surgery or mesenteric ischemia. Furthermore, most perioperative MIs are non–Q wave, and nonspecific ST changes are common after surgery with or without MI. Echocardiography may certainly help by identifying new wall motion abnormalities.
|
|
|
Figure 118.4. Algorithm on management of patients with ST-segment elevation myocardial infarction after coronary artery bypass grafting (CABG). IABP, intra-aortic balloon pump; ECG, electrocardiogram. |
The management of these patients should be based on the extension and severity of ischemia, weighing the risk of bleeding complications and the benefits from an aggressive therapy. Patients in stable hemodynamic condition, without severe ischemia, may be managed conservatively with administration of acetylsalicylic acid (ASA), β-blockers (if not contraindicated), nitroglycerin, and low-molecular-weight heparin (LMWH). In patients with large STEMI or who are hemodynamically unstable, immediate coronary angiography and PCI should be the preferred strategy.
Drug Therapy
The main objectives of medical therapy in patients with ACS are to stabilize and “cool” the culprit lesion, treat residual ischemia, and prevent long-term complications.
Antiplatelet and Anticoagulation Therapies
Aspirin and clopidogrel, as shown by several large randomized trials (62,63), improve the outcome, and thus represent a cornerstone in the initial treatment of ACS. Glycoprotein IIb/IIIa inhibitors have been shown to reduce mortality. However, the benefits were restricted to patients with positive troponin. A strategy of upstream administration—starting 48 hours before angiography—is currently recommended with eptifibatide or tirofiban. Abciximab may be considered for downstream administration in the cardiac catheterization laboratory in patients with positive troponin undergoing percutaneous revascularization due to the significant benefits shown in a recent randomized trial (64).
Intravenous heparin or LMWH are considered a fundamental therapy for treating ACS and are a class IA therapy when given in conjunction with antiplatelet agents (53,54,55). However, it seems that LMWH further improves the outcome as compared to intravenous unfractionated heparin (65).
Anti-ischemic Drugs
Relief of the symptoms of acute myocardial ischemia requires the use of drugs that correct the imbalance that exists between myocardial oxygen supply and demand. In the absence of contraindications, β-adrenergic blockers should be first-line anti-ischemic therapy and should be given intravenously in high-risk patients, particularly if ischemia is ongoing. A meta-analysis of three randomized clinical trials comparing β-blockers with placebo in unstable angina showed a significant reduction in rates of progression to acute myocardial infarction, but not death, by active treatment (66).
There are no randomized, placebo-controlled trials investigating the effect of nitrates on symptoms or prognosis in ACS. A number of small, uncontrolled datasets have been published (67,68), but the routine use of this group of drugs is almost entirely based on anecdotal experience of their efficacy in relieving symptoms. It is recommended that sublingual glyceryl trinitrate should be given in all cases where ischemic chest discomfort is present at the time of initial clinical assessment. If symptoms are not relieved rapidly thereafter and after administration of intravenous β-blockers, an intravenous nitrate infusion should be started.
Randomized studies of calcium channel blockers in ACS have shown their efficacy in relieving symptoms (69,70). In addition, diltiazem may have a protective effect (71,72), whereas there is strong evidence that immediate-release nifedipine (a dihydropyridine) increases mortality rate, particularly if given without β-blockers (73,74). Current guidelines recommend reserving the dihydropyridine calcium antagonists for use as second- or third-line therapy after β-blockers and nitrates, whereas the rate-limiting, nondihydropyridine agents (diltiazem and verapamil) may be reasonable alternatives when β-blockers are contraindicated.
Statins represent the main agents for treatment of hypercholesterolemia today. Recent studies have shown that their effects on progression of atherosclerosis may be explained by additional properties beyond lowering cholesterol (75,76,77). In particular, their antithrombotic and anti-inflammatory properties make statins a therapeutically attractive option in ACS patients. In fact, early statin therapy has been shown to be associated with a significant improvement in clinical outcome (78), and is strongly recommended after ACS (53,54).
Summary
The evaluation of patients with ACS should be organized and proceed rapidly in logical sequence. The evaluation should include a review of the patient's past medical history, history of present illness, risk factors, and a detailed physical examination, to exclude noncardiac or nonischemic disorders and precipitating extracardiac causes. After confirmation of the diagnosis, all patients should be treated with optimal medical therapy. Risk stratification is mandatory, since high-risk patients may benefit from aggressive antiplatelet therapy and early angiography and revascularization, whereas patients at lower risk should undergo early, noninvasive testing for inducible myocardial ischemia, followed by coronary angiography when such testing is positive.
References
1. Lee T, Goldmann L. Evaluation of the patients with acute chest pain. N Eng J Med. 2006;342:1187–1195.
2. Puleo PR, Meyer D, Wathen C, et al. Use of a rapid assay of subforms of creatine kinase-MB to diagnose or rule out acute myocardial infarction. N Engl J Med. 1994;331:561–566.
3. Newby LK, Goldmann BU, Ohman EM. Troponin: an important prognostic marker and risk-stratification tool in non-ST-segment elevation acute coronary syndromes. J Am Coll Cardiol. 2003;41(4 Suppl S):31S–36S.
4. Korff S, Katus HA, Giannitsis E. Differential diagnosis of elevated troponin. Heart. 2006;92:987–993.
5. de Winter RJ, Koster RW, Sturk A, et al. Value of myoglobin, troponin T, and CK-MBmass in ruling out an acute myocardial infarction in the emergency room. Circulation. 1995;92:3401–3407.
6. Konstantinides S, Geibel A, Olschewski M, et al. Importance of cardiac troponins I and T in risk stratification of patients with acute pulmonary embolism. Circulation. 2002;106:1263–1268.
7. Giannitsis E, Muller-Bardorff M, Kurowski V, et al. Independent prognostic value of cardiac troponin T in patients with confirmed pulmonary embolism. Circulation. 2000;102:211–217.
8. Kucher N, Goldhaber SZ. Cardiac biomarkers for risk stratification of patients with acute pulmonary embolism. Circulation. 2003;108:2191–2194.
9. Panteghini M. Role and importance of biochemical markers in clinical cardiology. Eur Heat J. 2004;25:1187–1196.
10. Wakai A, Gleeson A, Winter D. Role of fibrin D-dimer testing in emergency medicine. Emerg Med J. 2003;20:319–325.
11. Kang DH, Kang SJ, Song JM, et al. Efficacy of myocardial contrast echocardiography in the diagnosis and risk stratification of acute coronary syndrome. Am J Cardiol. 2005;96:1498–1502.
12. Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation. 2005;112:3802–3813.
13. Conti A, Zanobetti M, Grifoni S, et al. Implementation of myocardial perfusion imaging in the early triage of patients with suspected acute coronary syndromes. Nucl Med Commun. 2003;24:1055–1060.
14. Wackers FJ, Brown KA, Heller GV, et al. American Society of Nuclear Cardiology position statement on radionuclide imaging in patients with suspected acute ischemic syndromes in the emergency department or chest pain center. J Nucl Cardiol. 2002;9:246–250.
15. Bulow H, Schwaiger M. Nuclear cardiology in acute coronary syndromes. Q J Nucl Med Mol Imaging. 2005;49:59–71.
16. Schuijf JD, Bax JJ, Shaw LJ, et al. Meta-analysis of comparative diagnostic performance of magnetic resonance imaging and multislice computed tomography for noninvasive coronary angiography. Am Heart J. 2006;151:404–411.
17. Gallagher MJ, Ross MA, Raff GL, et al. The diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patients. Ann Emerg Med. 2007;49(2):125–136.
18. van Belle A, Buller HR, Huisman MV, et al. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295:172–179.
19. Erbel R, Alfonso F, Boileau C, et al. Task Force on Aortic Dissection, European Society of Cardiology. Diagnosis and management of aortic dissection. Eur Heart J. 2001;22:1642–1681.
20. Ohno Y, Higashino T, Takenaka D, et al. MR angiography with sensitivity encoding (SENSE) for suspected pulmonary embolism: comparison with MDCT and ventilation-perfusion scintigraphy. AJR Am J Roentgenol. 2004;183:91–98.
21. Richter JE. Overview of diagnostic testing for chest pain of unknown origin. Am J Med. 1992;92:41S.
22. Levine HJ. Difficult problems in the diagnosis of chest pain. Am Heart J. 1980;100:108.
23. Christie LG Jr, Conti CR. Systematic approach to evaluation of angina-like chest pain: pathophysiology and clinical testing with emphasis on objective documentation of myocardial ischemia. Am Heart J. 1981;102:897.
24. Rude RE, Poole VVK, Muller JE, et al. Electrocardiographic and clinical criteria for recognition of acute myocardial infarction based on analysis of 3,697 patients. Am J Cardiol. 1983;52:936.
25. Bell WR, Simon TL, DeMets DL. The clinical features of submassive and massive pulmonary emboli. Am J Med. 1977;62:355.
26. Piazza G, Goldhaber SZ. Acute pulmonary embolism. Part I: epidemiology and diagnosis. Circulation. 2006;114:e28–e32.
27. PIOPED Investigators. Value of ventilation/perfusion scan in acute pulmonary embolism: results of the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED). JAMA. 1990;263:2753.
28. Goldhaber SZ, Norpurgo M. Diagnosis, treatment and prevention of pulmonary embolism. JAMA. 1972;268:1727.
29. Tocino IM, Miller MH, Fairfax WR. Distribution of pneumothorax in the supine and semirecumbent critically ill adult. AJR Am J Roentgenol. 1981;137:699.
30. Ziter FMH, Westcott JL. Supine subpulmonic pneumothorax. AJR Am J Roentgenol. 1981;137:699.
31. DeSanctis RW, Doroghazi RM, Austen WG, et al. Aortic dissection. N Engl J Med. 1987;317:1060–1067.
32. Suzuki T, Mehta RH, Ince H, et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the International Registry of Aortic Dissection (IRAD). Circulation. 2003;108(suppl II):II-312–II-317.
33. Erbel R, Oelert H, Meyer J, et al. Effect of medical and surgical therapy on aortic dissection evaluated by transesophageal echocardiography: implications for prognosis and therapy: the European Cooperative Study Group on Echocardiography. Circulation. 1993;87:1604–1615.
34. Glower DD, Speier RH, White WD, et al. Management and long-term outcome of aortic dissection. Ann Surg. 1991;214:31–41.
35. Cambria RP, Brewster DC, Gertler J, et al. Vascular complications associated with spontaneous aortic dissection. J Vasc Surg. 1988;7:199.
36. Chan K. Impact of transesophageal echocardiography on the treatment of patients with aortic dissection. Chest. 1992;101:406.
37. Cigarroa JE, Isselbacher EM, DeSanctis RW, et al. Diagnostic imaging in the evaluation of suspected aortic dissection: old standards and new directions. N Engl J Med. 1993;328:35.
38. Nienaber CA, Spielmann RP, von Kodolitsch Y, et al. Diagnosis of thoracic aortic dissection: magnetic resonance imaging versus transesophageal echocardiography. Circulation. 1991;85:434.
39. Nienaber CA, von Kodolitsch Y, Petersen B, et al. Intramural hemorrhage of the thoracic aorta: diagnostic and therapeutic implications. Circulation. 1995;92:1465–1472.
40. Vilacosta I, San Roman JA, Ferreiros J, et al. Natural history and serial morphology of aortic intramural hematoma: a novel variant of aortic dissection. Am Heart J. 1997;134:495–507.
41. Yacoub MH, Gehle P, Chandrasekaran V, et al. Late results of a valve-preserving operation in patients with aneurysms of the ascending aorta and root. J Thorac Cardiovasc Surg. 1998;115:1080–1090.
42. Maraj R, Rerkpattanapipat P, Jacobs LE, et al. Meta-analysis of 143 reported cases of aortic intramural hematoma. Am J Cardiol. 2000;86:664–668.
43. von Kodolitsch Y, Nienaber CA. Ulcer of the thoracic aorta: diagnosis, therapy and prognosis [in German]. Z Kardiol. 1998;87:917–927.
44. Stanson AW, Kazmier FJ, Hollier LH, et al. Penetrating atherosclerotic ulcers of the thoracic aorta: natural history and clinicopathologic correlations. Ann Vasc Surg. 1986;1:15–23.
45. Movsowitz HD, Lampert C, Jacobs LE, et al. Penetrating atherosclerotic aortic ulcers. Am Heart J. 1994;128:1210–1217.
46. Ganaha F, Miller DC, Sugimoto K, et al. Prognosis of aortic intramural hematoma with and without penetrating atherosclerotic ulcer: a clinical and radiological analysis. Circulation. 2002;106:342–348.
47. Horowitz MS, Schults CS, Stinson EB, et al. Sensitivity and specificity of echocardiographic diagnosis of pericardial effusion. Circulation. 1974;50:239.
48. Spodick DH. Arrhythmias during acute pericarditis (100) cases. JAMA. 1976;235:39.
49. Spodick DH. Diagnostic electrocardiographic sequences in acute pericarditis. Circulation. 1973;48:575.
50. Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378.
51. Permanyer-Miralda G, Sagrista-Sauleda J, Soler-Soler J. Primary acute pericardial disease: a prospective series of 231 consecutive patients. Am J Cardiol. 1985;56:623.
52. Marcus ML, Doty DB, Hiratzka LF, et al. Decreased coronary reserve: a mechanism for angina pectoris in patients with aortic stenosis and normal coronary arteries. N Engl J Med. 1982;307:1362.
53. Bertrand ME, Simoons ML, Fox KA, et al. Task Force on the Management of Acute Coronary Syndromes of the European Society of Cardiology. Management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2002;23(23):1809–1840.
54. Gibler WB, Cannon CP, Blomkalns AL, et al. American Heart Association Council on Clinical Cardiology (Subcommittee on Acute Cardiac Care); Council on Cardiovascular Nursing, and Quality of Care and Outcomes Research Interdisciplinary Working Group; Society of Chest Pain Centers. Practical implementation of the guidelines for unstable angina/non-ST-segment elevation myocardial infarction in the emergency department: a scientific statement from the American Heart Association Council on Clinical Cardiology (Subcommittee on Acute Cardiac Care), Council on Cardiovascular Nursing, and Quality of Care and Outcomes Research Interdisciplinary Working Group, in collaboration with the Society of Chest Pain Centers. Circulation. 2005;111:2699–2710.
55. Silber S, Albertsson P, Aviles FF, et al. Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Eur Heart J. 2005;26:804–847.
56. McKay RG. “Ischemia-guided” versus “early invasive” strategies in the management of acute coronary syndrome/non-ST-segment elevation myocardial infarction: the interventionalist's perspective. J Am Coll Cardiol. 2003;41:96S–102S.
57. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842.
58. Garcia S, Canoniero M, Peter A, et al. Correlation of TIMI risk score with angiographic severity and extent of coronary artery disease in patients with non-ST-elevation acute coronary syndromes. Am J Cardiol. 2004;93:813–816.
59. Boersma E, Pieper KS, Steyerberg EW, et al. Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation. Results from an international trial of 9461 patients. The PURSUIT Investigators. Circulation. 2000;101:2557–2567.
60. Cannon CP. Evidence-based risk stratification to target therapies in acute coronary syndromes. Circulation. 2002;106:1588–1591.
61. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842.
62. Risk of myocardial infarction and death during treatment with low dose aspirin and intravenous heparin in men with unstable coronary artery disease. The RISC Group. Lancet. 1990;336:827–830.
63. Yusuf S, Zhao F, Mehta SR, et al., Clopidogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001;345:494–502.
64. Kastrati A, Mehilli J, Neumann FJ, et al. Intracoronary Stenting and Antithrombotic: Regimen Rapid Early Action for Coronary Treatment 2 (ISAR-REACT 2) Trial Investigators. Abciximab in patients with acute coronary syndromes undergoing percutaneous coronary intervention after clopidogrel pretreatment: the ISAR-REACT 2 randomized trial. JAMA. 2006;295:1531–1538.
65. Petersen JL, Mahaffey KW, Hasselblad V, et al. Efficacy and bleeding complications among patients randomized to enoxaparin or unfractionated heparin for antithrombin therapy in non-ST-segment elevation acute coronary syndromes: a systematic overview. JAMA. 2004;292:89–96.
66. Yusuf S, Wittes J, Friedman L. Overview of results of randomized clinical trials in heart disease. II. Unstable angina, heart failure, primary prevention with aspirin, and risk factor modification. JAMA. 1988;260:2259–2263.
67. Kaplan K, Davison R, Parker M, et al. Intravenous nitroglycerin for the treatment of angina at rest unresponsive to standard nitrate therapy. Am J Cardiol. 1983;51:694–698.
68. Roubin GS, Harris PJ, Eckhardt I, et al. Intravenous nitroglycerine in refractory unstable angina pectoris. Aust N Z J Med. 1982;12:598–602.
69. Theroux P, Taeymans Y, Morissette D, et al. A randomized study comparing propranolol and diltiazem in the treatment of unstable angina. J Am Coll Cardiol. 1985;5:717–722.
70. Parodi O, Simonetti I, Michelassi C, et al. Comparison of verapamil and propranolol therapy for angina pectoris at rest: a randomized, multiplecrossover, controlled trial in the coronary care unit. Am Cardiol. 1986;57:899–906.
71. Gibson RS, Hansen JF, Messerli F, et al. Long-term effects of diltiazem and verapamil on mortality and cardiac events in non-Q-wave acute myocardial infarction without pulmonary congestion: post hoc subset analysis of the multicenter diltiazem postinfarction trial and the second Danish verapamil infarction trial studies. Am J Cardiol. 2000;86:275–279.
72. Gibson RS, Young PM, Boden WE, et al. Prognostic significance and beneficial effect of diltiazem on the incidence of early recurrent ischemia after non-Q-wave myocardial infarction: results from the multicenter diltiazem reinfarction study. Am J Cardiol. 1987;60:203–209.
73. Yusuf S, Held P, Furberg C. Update of effects of calcium antagonists in myocardial infarction or angina in light of the second Danish verapamil infarction trial (DAVIT-II) and other recent studies. Am J Cardiol. 1991;67:1295–1297.
74. Psaty BM, Heckbert SR, Koepsell TD, et al. The risk of myocardial infarction associated with antihypertensive drug therapies. JAMA. 1995;274:620–625.
75. Undas A, Brozek J, Musial J. Anti-inflammatory and antithrombotic effects of statins in the management of coronary artery disease. Clin Lab. 2002;48:287–296.
76. Thompson PD, Moyna NM, White CM, et al. The effects of hydroxy-methyl-glutaryl co-enzyme A reductase inhibitors on platelet thrombus formation. Atherosclerosis. 2002;161:301–306.
77. Dangas G, Badimon JJ, Smith DA, et al. Pravastatin therapy in hyperlipidemia: effects on thrombus formation and the systemic hemostatic profile. J Am Coll Cardiol. 1999;33:1294–1304.
78. Schwartz GG, Olsson AG, Ezekowitz MD, et al. Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering (MIRACL) Study Investigators. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA. 2001;285:1711–1718.