Achille Gaspardone
Leonardo De Luca
Overview of ST Elevation Myocardial Infarction
Definition of Terms
The definition of acute myocardial infarction (MI) may refer to different perspectives related to clinical, electrocardiographic (ECG), biochemical, and pathologic characteristics, all reflecting death of cardiac myocytes caused by prolonged ischemia (1,2). A definition for acute evolving myocardial infarction in the presence of clinically appropriate symptoms has been established as:
1. Patients with ST-segment elevation (ST elevation MI [STEMI])—that is, new ST-segment elevation at the J-point with the cutoff points greater than or equal to 0.2 mV in V1 through V3 and greater than or equal to 0.1 mV in other leads, or
2. Patients without ST-segment elevation (non–ST elevation MI [N-STEMI])—that is, ST-segment depression or T-wave abnormalities with elevated biomarkers of myocardial damage. ST-segment elevation is usually indicative of transmural MI, while ST-segment depression—whether associated or not with T-wave abnormalities—is more likely indicative of subendocardial MI.
Clinically established myocardial infarction may be defined by any Q wave in leads V1 through V3, or a Q wave greater than or equal to 0.03 s in leads I, II, aVL, aVF, V4, V5, or V6. In the setting of acute MI, ECG changes are associated with elevation of the biomarkers of myocardial damage. The standard biomarker for myocardial damage is cardiac troponin (I or T), which has an elevated myocardial tissue specificity as well as high sensitivity, and creatine kinin (CK)-MB mass, which is less tissue specific than cardiac troponin but more specific for irreversible injury (1,2). Recently, a Global Task Force composed by several worldwide scientific working groups redefined the ESC/ACC criteria for the diagnosis of MI from various perspectives (2A) (Table 120.1). Clinically, the various types of MI, according to this new definition, can be classified as shown in Table 120.2.
Epidemiology
Acute MI represents a significant public and social health problem in industrialized countries, and is becoming an increasingly significant issue in developing countries (3). Although the exact incidence is difficult to ascertain, using primary listed and secondary hospital discharge data, the incidence has been estimated at 500,000 STEMI events per year in the United States (3). Several registries have reported significant declines in the incidence of STEMI such that ST-elevation MIs are becoming less frequent (4). Accompanying these trends, the overall proportion of admissions for chest pain caused by STEMI is also declining, while several sources have indicated that the incidence of unstable angina and N-STEMI is increasing (4).
Pathogenesis of ST Elevation Myocardial Infarction and Its Complications
ST elevation is conventionally thought of as representing transmural ischemia in response to fissuring or rupture of an atheromatous plaque with total and prolonged occlusion of a major coronary artery. Less frequently vessel occlusion may be caused by a prolonged coronary artery spasm.
After an acute MI, mechanical problems that result from dysfunction or disruption of critical myocardial structures (e.g., loss of contracting muscle causing left ventricular dysfunction, mitral regurgitation, rupture of the interventricular septum or of the free wall, or ventricular aneurysm formation) may occur and require an immediate combination of pharmacologic, catheter-based, and surgical treatments. This may lead to ventricular remodeling, a term that refers to changes in size, shape, and thickness of the left ventricle involving both the infarcted and noninfarcted segments of the left ventricle (1,2,5,6). An extra load is placed on the residual functioning myocardium, which results in compensatory hypertrophy. Additionally, cardiac dysrhythmias may result from electrical instability, pump failure/excessive sympathetic stimulation, and conduction disturbances (1,2,5,6).
|
Table 120.1 New definition of myocardial infarction (from ref 2A) |
|||||||
|
|||||||
|
Table 120.2 Clinical classification of different types of myocardial infarction (from ref 2A) |
|||||||
|
|
Table 120.3 Aims of acute management of ST elevation myocardial infarction |
|
|
Early Evaluation
Immediate Concerns and Questions to Be Addressed at the Initial Evaluation
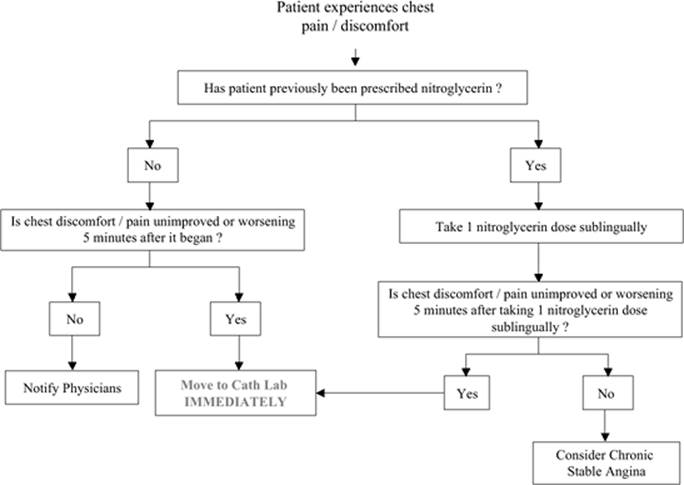
Rapid diagnosis and early risk stratification are essential to identify patients with acute chest pain in whom early revascularization can improve outcomes (Table 120.3). A working diagnosis of acute MI is usually based on the history of severe chest pain lasting for 20 minutes or more, not responding to nitroglycerin (Fig. 120.1). Important clues are a previous history of coronary artery disease (CAD) and radiation of the pain to the neck, lower jaw, or left arm. The pain may not be severe and, particularly in the elderly, other presentations such as fatigue, dyspnea, feeling faint or simply feeling “poorly,” or syncope are common. There are no individual physical signs diagnostic of myocardial infarction, but most patients have evidence of autonomic nervous system activation (e.g., pallor and/or sweating) and either hypotension or a narrow pulse pressure. Features may also include irregularities of the pulse, bradycardia or tachycardia, and a third heart sound (7,8). The presence and severity of basal pulmonary rales is an easy, immediate, and pivotal tool for an early risk stratification of STEMI patients (Table 120.4).
An ECG should be obtained as soon as possible. In case of ST-segment elevations, or new or presumed new left bundle branch block, reperfusion therapy should be initiated as soon as possible. However, the ECG is often equivocal in the early hours and, even in proven infarction, it may never demonstrate the classic features of ST-segment elevation and new Q waves. During the early evolution of infarction, the ECG may be abnormal without significant ST elevation. Typical changes may evolve over minutes or hours, and it is critically important to institute continuous ST monitoring or perform repeat ECGs to ensure that such evolution is detected promptly (7,8).
|
|
|
Figure 120.1. Patient (advance) instructions for nitroglycerin use and emergency medical service (EMS) contact in the setting of non–trauma-related chest discomfort/pain. (Modified from Antman EM, Anbe DT, Armstrong PW, et al. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Canadian Cardiovascular Society. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [committee to revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction]. Circulation. 2004;110[9]:e82–e292.) |
|
Table 120.4 Percent mortality by Killip classa |
||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||
In patients with symptoms suggestive of infarction but without diagnostic ECG changes, alternative diagnoses must be considered, including aortic dissection, gastroesophageal disease, and musculoskeletal and mediastinal conditions (Table 120.5). A normal ECG in the presence of suspected cardiac pain should prompt the search for an alternative diagnosis. Similarly, myocardial perfusion scintigraphy or magnetic resonance imaging (MRI) may be used to detect the presence of ischemia or infarction, and a normal result effectively excludes significant MI. Certain groups of patients, including the elderly and those with diabetes, may present without typical symptoms of MI. They may present with evolving ECG changes of MI or hemodynamic/mechanical complications. Their treatment should be similar to patients with typical painful infarction.
|
Table 120.5 Differential diagnosis of ST elevation myocardial infarction |
|||
|
Blood sampling for serum biomarkers is routinely done in the acute phase. Considering that the first blood sample may be negative for elevated biomarkers, even in the presence of acute MI, it is not reasonable to wait for the next results before initiating a reperfusion regimen when the diagnosis of acute MI is established. The finding of elevated biomarkers may sometimes be helpful in deciding to initiate reperfusion therapy (e.g., in patients with left bundle branch block). When the history, ECG, and serum biomarkers are not diagnostic of acute myocardial infarction, the patient can proceed safely to stress testing for investigation of underlying CAD.
Hemodynamic Compromise and Cardiac Arrest
Resuscitation may be suddenly required for ventricular fibrillation (VF) or for ventricular tachycardia with diminished cardiac output; guidelines for such resuscitation are provided within the framework of Basic and Advanced Life Support. For the patient with extensive myocardial ischemia and/or heart failure (HF), additional circulatory support may be necessary, including the insertion of an intra-aortic balloon pump (IABP), as a bridge to revascularization (see below).
Early In-hospital Care and Management Strategies
Pharmacologic Treatment in the Acute Phase of ST Elevation Myocardial Infarction
Pain Control
Pain relief is a key element in the early management of the patient with STEMI. Pain management should be directed toward acute relief of symptoms of ongoing myocardial ischemia and necrosis, and toward general relief of anxiety and apprehension, the latter of which can heighten pain perception. Morphine sulfate remains the analgesic agent of choice for management of pain associated with STEMI, the exception being documented cases of morphine sensitivity. The dose required for adequate pain relief varies in proportion to age and body size, as well as blood pressure and heart rate. Anxiety reduction secondary to morphine administration reduces the patient's restlessness and the activity of the autonomic nervous system, with a consequent reduction of the heart's metabolic demands. Morphine administration for patients with pulmonary edema is clearly beneficial and may promote peripheral arterial and venous dilation, reducing the work of breathing and slowing the heart rate secondary to a combined decrease in sympathetic tone and augmentation of vagal tone (7,8). Side effects of morphine administration, such as hypotension, can be minimized by keeping the patient supine and elevating the lower extremities if systolic pressure decreases below 100 mm Hg, assuming pulmonary edema is not present.
|
Table 120.6 Contraindications to fibrinolytic therapy |
||
|
Fibrinolysis
Prompt and effective reperfusion by pharmacologic therapy is the cornerstone of treatment for STEMI. It is the only widely applicable acute treatment that can diminish infarct size and major cardiac complications (Table 120.6). In trials of fibrinolysis versus control, more than 150,000 patients were randomized and showed that the treatment benefit was approximately 50 lives saved per 1,000 patients treated with the combination of thrombolytic agent and aspirin (9).
Limitations of Fibrinolysis
The major limitation of fibrinolytic drug treatment is that reperfusion is gradual and, in addition, is incomplete or inadequate in a significant proportion of patients. This proportion may range from about 40% showing failure to achieve Thrombolysis in Myocardial Infarction (TIMI) 3 flow within the first 3 hours of reperfusion therapy when streptokinase is used, to 20% to 30% with tissue plasminogen activator (tPA) or tenecteplase (TNK) (Table 120.7).
The principal hazard of fibrinolytic therapy is stroke and intracranial hemorrhage. Overall, about four extra strokes occur per 1,000 patients treated and, of these, two are fatal. The use of accelerated tPA (alteplase) results in ten fewer deaths per 1,000 patients treated, but at the risk of three additional strokes compared with streptokinase treatment (10). Single-bolus agents provide logistic advantages, and both reteplase-PA or weight-adjusted TNK have equivalent efficacy to accelerated tPA. TNK has a lower rate of noncerebral bleeds and a lesser need for blood transfusion. Bolus agents are particularly advantageous in minimizing time delay in the prehospital and emergency room settings (10).
Prehospital Fibrinolysis
In clinical trials, it has been shown that prehospital thrombolysis (PHT) could be used safely in patients presenting with evidence of acute MI (11).
|
Table 120.7 Comparison of approved fibrinolytic agents |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
The efficacy of PHT has initially been demonstrated in the Grampian Region Early Anistreplase Trial (GREAT) (12) in which administration of thrombolysis by the general practitioners before hospital admission resulted in a 50% reduction in 1-year mortality. Recently, a meta-analysis of six trials comparing PHT and in-hospital thrombolysis confirmed this beneficial effect, showing a 17% reduction in in-hospital mortality with the use of PHT (11). The Comparison of Angioplasty and Prehospital Thrombolysis In acute Myocardial infarction (CAPTIM) trial (13), which compared PHT with primary percutaneous coronary intervention (PCI), showed that 1-month mortality was lower in the group that received PHT. These data are concordant with the observation from the meta-analysis of trials of thrombolytic therapy that showed an exponential decrease in the efficacy of thrombolysis in the patients treated more than 3 hours after the onset of chest pain (14).
In this regard, it is now clear that myocardial salvage is highly dependent on the time from the beginning of symptoms to reperfusion, and that very early administration of thrombolytics are likely to result in superior myocardial salvage compared with in-hospital thrombolysis and possibly also primary PCI, for which the time delay observed in the real-world setting is often 1 hour or more (15,16).
Fibrinolysis Combined with Newer Antithrombotic Agents
To improve the rates of patients achieving TIMI 3 flow by pharmacologic reperfusion therapy, glycoprotein (GP) IIb/IIIa antagonists have been combined with fibrinolytic agents to achieve both platelet disaggregation and fibrinolysis (1,2,17). This pharmacologic combination has been tested in seven studies, including two large trials (ASSENT 3 and GUSTO V) involving more than 30,000 patients. There was no overall advantage noted when combining the thrombolytic agent with a GP IIb/IIIa inhibitor. In patients older than 70 years of age, the combination increased the risk of intracranial hemorrhage and extracranial bleeding (10). Similarly, the combination of streptokinase with a specific antithrombin (bivalirudin) failed to improve survival in the HERO 2 trial (18). Two ongoing randomized trials (CARESS and FINESS) are investigating the impact of a combination therapy in the early treatment of STEMI.
Anti-ischemic Drugs
Oxygen
Although oxygen administration to virtually all patients with suspected STEMI has become universal practice, it is still unknown whether this therapy limits myocardial damage or reduces morbidity or mortality. Experimental results indicate that oxygen administration may limit myocardial injury (19), and may reduce ST-segment elevation (20). The rationale for use of oxygen is based on the observation that even with uncomplicated MI, some patients are modestly hypoxemic initially, presumably because of ventilation/perfusion mismatch and excessive lung water (21). For patients without complications, excess administration of oxygen can lead to systemic vasoconstriction, and high flow rates can be harmful to patients with chronic obstructive airway disease. In the absence of compelling evidence for established benefit in uncomplicated cases, and in view of its expense, there appears to be little justification for continuing its routine use beyond 6 hours.
Nitrates
The rationale for using nitrates in the setting of STEMI is that they reduce preload and afterload through peripheral arterial and venous dilation, improve coronary flow by relaxation of epicardial coronary arteries, and dilate collateral vessels, potentially creating a more favorable subendocardial-to-epicardial flow ratio (22,23). Nitrate-induced vasodilatation may also have particular utility in those rare patients with coronary spasm presenting as STEMI.
Clinical trial results have suggested only a modest benefit from nitroglycerin used acutely in STEMI and continued subsequently. A pooled analysis of more than 80,000 patients treated with nitratelike preparations intravenously or orally in 22 trials yielded a mortality rate of 7.7% in the control group, which was reduced to 7.4% in the nitrate group. These data are consistent with a possible small treatment effect of nitrates on mortality, such that three to four fewer deaths would occur for every 1,000 patients treated (24). Nitrates in all forms should be avoided in patients with initial systolic blood pressures less than 90 mm Hg or greater than or equal to 30 mm Hg below baseline, marked bradycardia or tachycardia, or known or suspected right ventricular (RV) infarction.
β-Adrenergic Blockers
The emergency treatment of suspected STEMI with intravenous (IV) β-blocker therapy has also been studied in more than two dozen randomized trials (25,26,27,28,29). Overall, those trials included more than 27,000 patients, but nearly all were done before fibrinolytic and antiplatelet therapy had become routine, and they mainly involved fairly low-risk patients. Collectively, though not separately, their results indicated that this treatment was safe and moderately effective in such low-risk patients (25). However, in the recently published COMMIT trial, 45,852 patients admitted within 24 hours of suspected STEMI onset were randomly allocated metoprolol—up to 15 mg intravenously, followed by 200 mg oral daily—or matching placebo (29). Allocation to early metoprolol was associated with reduced risk of reinfarction and ventricular fibrillation, but increased risk of cardiogenic shock, especially during the first day or so after admission (29). Consequently, it might generally be prudent to consider starting β-blocker therapy in hospital only when the hemodynamic condition after STEMI has been stabilized.
Antiplatelet Therapy
Aspirin
Aspirin should be given to the patient with suspected STEMI as early as possible and continued indefinitely, regardless of the strategy for reperfusion or whether additional antiplatelet agents are administered. Known true aspirin allergy is the only exception to this recommendation. Maintenance aspirin doses for secondary prevention of cardiovascular events in large trials have varied from 75 to 325 mg/day, but no trial has directly compared the efficacy of different doses after STEMI (1,2).
Thienopyridine
A thienopyridine (e.g., ticlopidine or clopidogrel) should be substituted for aspirin in patients with STEMI for whom aspirin is contraindicated because of hypersensitivity or major gastrointestinal intolerance. Clopidogrel is generally preferred to ticlopidine because of fewer side effects, lack of need for laboratory monitoring, and once-daily dosing. On the basis of several randomized trials (30,31,32,33), clopidogrel, in combination with low-dose aspirin—75 to 162 mg, to minimize the risk of bleeding—is recommended for all patients after stent implantation (1,2,34). Recently, two randomized trials of 7,000 patients with STEMI showed that adding clopidogrel to aspirin improved the patency of the infarct-related coronary artery after fibrinolytic therapy, and suggested some reduction in clinical events (35,36). In addition, these trials demonstrated that adding clopidogrel 75 mg daily to aspirin and other standard treatments, such as fibrinolytic therapy, in STEMI patients safely reduces mortality and major vascular events in hospital (35,36).
Prasugrel is a new thienopyridine derivative that is about ten times more potent than clopidogrel in preclinical studies (37). It has been evaluated both in healthy individuals and in patients undergoing elective or urgent PCI, in which it was shown to result in low and similar rates of bleeding when compared with clopidogrel (38).
Platelet Glycoprotein IIb/IIIa Receptor Antagonists
It is reasonable to start treatment with GP IIb/IIIa (abciximab, tirofiban, and eptifibatide) as early as possible in patients undergoing primary PCI. Several randomized studies have demonstrated that adjunctive antiplatelet therapy with GP IIb/IIIa blockade reduces the incidence of acute ischemic events by as much as 35% to 50% among the broad population of patients undergoing primary PCI (39).
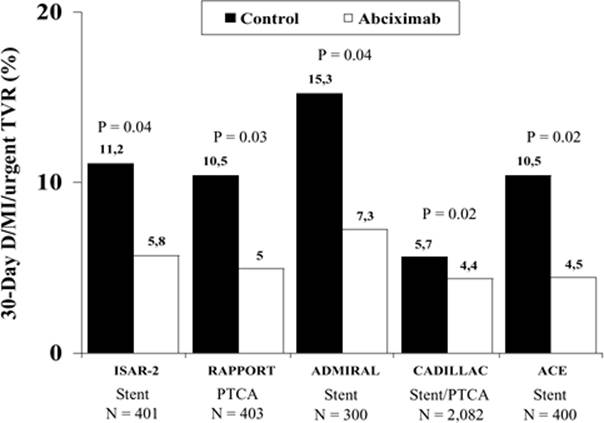
GP IIb/IIIa inhibitors were also shown to decrease coronary thrombus, improve TIMI flow grade, enhance epicardial reperfusion when combined with thrombolysis, improve 30-day clinical outcomes post-MI (Fig. 120.2), speed resolution of ST-segment elevation, and in one study of elective percutaneous coronary intervention, improve coronary artery flow reserve and myocardial blush grade (40). A recent meta-analysis of all completed, published, randomized trials of abciximab in STEMI showed that, when compared with the control group, adjunctive abciximab was associated with a significant reduction in 30-day and long-term mortality in patients treated with primary PCI, but not in those receiving fibrinolysis (41). The 30-day reinfarction rate was significantly reduced in patients treated with either fibrinolysis or primary PCI. A higher risk of major bleeding complications is observed with abciximab in association with fibrinolysis (41).
Antithrombotic Therapy
Unfractionated Heparin
Despite the use of unfractionated heparin (UFH) (42) in STEMI for over 40 years, there is continued controversy regarding its role. In patients who are treated with fibrinolytic therapy, recommendations for UFH therapy depend on the fibrinolytic agent chosen. The nonspecific fibrinolytic agents—streptokinase, anistreplase, and urokinase—that produce a systemic coagulopathy, including depletion of factors V and VIII, and massive production of fibrinogen degradation products are themselves anticoagulants. From this perspective, the need for adjunctive systemic anticoagulation with these agents is conceptually less compelling. When primary PCI is chosen as the route of reperfusion, weight-adjusted boluses of heparin in the range of 70 to 100 U/kg are recommended. This recommendation does not come specifically from empirical data in the setting of STEMI, but from general observations in the setting of angioplasty that an activated clotting time of at least 250 to 350 seconds is associated with a lower rate of complications than lower activated clotting times (43).
When GP IIb/IIIa antagonists are used, the UFH bolus should be reduced to 50 to 70 U/kg to achieve a target activated clotting time of 200 seconds (34). UFH doses used during PCI for failed fibrinolysis should be similarly reduced and further lowered if used with GP IIb/IIIa antagonists.
Low-molecular-weight Heparin
In the setting of STEMI, low-molecular-weight heparin (LMWH) may be an attractive alternative to UFH, as demonstrated by several clinical trials including those with LMWH as ancillary therapy to fibrinolysis and those that randomized patients not receiving fibrinolysis (44,45,46,47,48,49). The two LMWHs studied most extensively in patients with STEMI are enoxaparin and dalteparin.
|
|
|
Figure 120.2. Randomized trials demonstrating the clinical benefits of abciximab in the setting of ST elevation myocardial infarction (STEMI). D, death; MI, myocardial infarction; TVR, target vessel revascularization; PTCA, percutaneous transluminal coronary angioplasty. |
Direct Antithrombin Agents
Selective factor Xa inhibition appears to be a reasonable therapeutic concept in patients presenting with STEMI. A meta-analysis evaluated 11 trials that collectively enrolled more than 35,000 patients, comparing direct thrombin inhibitors with UFH (50). There was an approximate 25% reduction in the incidence of re-MI in patients treated with either hirudin or bivalirudin, but there was less evident efficacy for univalent thrombin inhibitors such as argatroban, efegatran, and inogatran. Other large randomized trials recently completed have confirmed the safety and long-term efficacy of bivalirudin alone compared with heparin or heparin and GP IIb/IIIa in the setting of STEMI (51,52).
Fondaparinux is a synthetic pentasaccharide that is a highly selective inhibitor of factor Xa. It selectively binds antithrombin III, inducing a conformational change that increases the anti-Xa activity of antithrombin III more than 300 times, which results in dose-dependent inhibition of factor Xa (53). In patients with STEMI, particularly those not undergoing primary PCI, fondaparinux seems to reduce mortality and reinfarction without increasing bleeding and strokes (54).
Other Pharmacologic Agents
Angiotensin-converting Enzyme Inhibitors
It is now well established that angiotensin-converting enzyme (ACE) inhibitors should be given to patients who have an impaired left ventricular (LV) ejection fraction or who have experienced congestive heart failure (CHF) in the early phase of an MI. The GISSI-3 (55), ISIS-4 (56), and Chinese study (57) have shown that ACE inhibitors started on the first day after a STEMI reduce mortality in the succeeding 4 to 6 weeks by a small but significant amount. The CONSENSUS II study (58), however, failed to show a benefit of early IV ACE inhibitor administration in STEMI patients. This may have been due to chance, or the fact that treatment was initiated early with an intravenous formulation. However, a systematic overview of trials of ACE inhibition early in acute MI indicated that this therapy is safe, well tolerated, and associated with a small but significant reduction in 30-day mortality, with most of the benefit observed in the first week. Therefore, there is now general agreement on starting ACE inhibitors in the first 24 hours after a STEMI if no contraindications are present (59). Opinions still differ as to whether to give ACE inhibitors to all patients or to high-risk patients only.
Calcium Antagonists
In patients with STEMI, immediate-release nifedipine does not reduce the incidence of reinfarction or mortality when given early (less than 24 hours after STEMI) or late, and may be particularly detrimental in patients with hypotension or tachycardia. Although the overall results of trials with verapamil showed no mortality benefits, subgroup analysis showed that immediate-release verapamil initiated several days after STEMI, in patients who were not candidates for a β-blocking agent, may have been useful in reducing the incidence of the composite end point of reinfarction and death, provided LV function was well preserved with no clinical evidence of CHF. Verapamil is detrimental to patients with CHF or bradyarrhythmias during the first 24 to 48 hours after STEMI (60,61,62,63,64,65).
Data from randomized trials (60,61,62,63,64,65) suggest that patients with non–Q-wave MI or those with Q-wave MI, preserved LV function, and no evidence of CHF may benefit from immediate-release diltiazem.
Inodilators
Administration of inodilator agents may be particularly threatening to patients with acute MI and should be avoided, except when severe hypotension occurs. Positive inotropic agents, especially phosphodiesterase inhibitors and adrenergic agonists such as dobutamine, may be associated with increasing myocardial oxygen demand and the potential to induce malignant dysrhythmias and myocardial ischemia, contributing to further cell death or necrosis (66,67,68,69).
Levosimendan is a calcium sensitizer that, by virtue of its unique mechanism of action and its negligible effect on myocardial oxygen demand, is the only inodilator that has been associated with favorable short-term outcomes in patients with acute MI, but large mortality studies are warranted (70).
Magnesium
Although a meta-analysis of seven randomized trials suggested a significant mortality benefit of magnesium in acute MI (71,72), subsequently a total of 68,684 patients were studied in a series of 15 randomized trials with controversial findings (73,74,75,76,77,78,79,80). On the basis of the totality of available evidence, in current coronary care practice, there is no indication for the routine administration of intravenous magnesium to patients with acute MI at any level of risk. Magnesium can continue to be administered for repletion of documented electrolyte deficits and life-threatening ventricular arrhythmias such as torsades de pointes (81).
Lidocaine
Although it has been demonstrated that lidocaine can reduce the incidence of ventricular fibrillation in the acute phase of MI (82,83), this drug significantly increases the risk of asystole (83). A meta-analysis of 14 trials showed a nonsignificantly higher mortality in lidocaine-treated patients than in controls (84). The routine prophylactic use of this drug is therefore not justified.
Glucose-Insulin-Potassium
There is experimental and limited clinical evidence that routine administration of glucose-insulin-potassium may favorably influence metabolism in the ischemic myocardium and therefore confer a clinical benefit (1,2).
Invasive Strategies
Primary Percutaneous Coronary Intervention
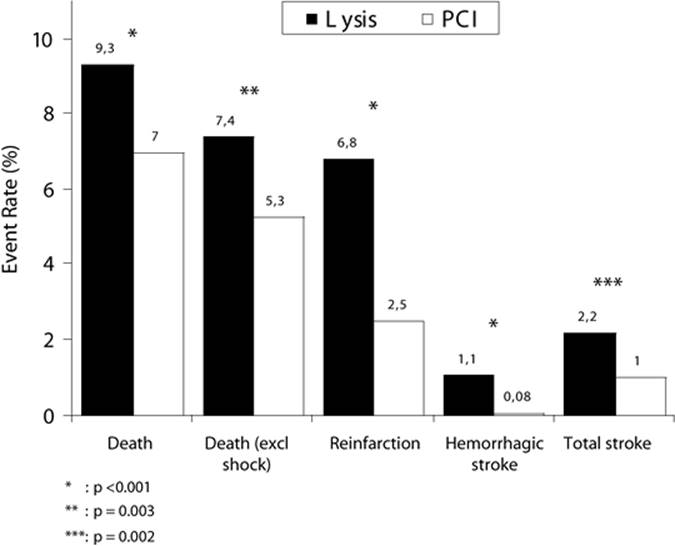
Primary PCI refers to the use of PCI without prior thrombolytic therapy and, as such, is associated with several potential advantages and disadvantages (Fig. 120.3 and Table 120.8). Most significantly, primary PCI results in better acute arterial patency compared to lytics, further improving survival and reducing the hazards of excess cerebral and systemic bleeding and recurrent ischemia, especially in high-risk patients (Fig. 120.4). In addition, several studies have demonstrated improvements in LV function and less reperfusion injury, cardiogenic shock, and myocardial rupture for primary PCI than fibrinolytic therapy (1,2,34,85).
Even lower mortality rates have been reported among patients undergoing primary PCI in centers with a high volume of PCI procedures compared with low-volume centers, demonstrating the need for an experienced team, made up of interventional cardiologists and skilled support staff (1,2,86).
|
|
|
Figure 120.3. A case of successful revascularization of anterior ST elevation myocardial infarction (STEMI) by primary percutaneous coronary intervention (PCI). A: Total occlusion (TIMI 0) in the middle tract of the left anterior descending (LAD) coronary artery. B: Crossing of the guidewire and thrombus removal by a manual thromboaspiration device. C: Restoration of a TIMI 3 flow on the LAD. D: Final angiographic result after stent placement. |
Facilitated Percutaneous Coronary Intervention
Facilitated PCI refers to treatment with low-dose thrombolytic therapy, platelet GP IIb/IIIa inhibitors, or both, before PCI. The rationale is to provide the earliest possible pharmacologic reperfusion before an attempt at definitive mechanical revascularization (87,88). These strategies may offer advantages, but larger-scale trials are still awaited (89).
Recently, the Assessment of the Safety and Efficacy of a New Treatment Strategy for Acute Myocardial Infarction (ASSENT)-4 PCI study was prematurely terminated. The study was intended to be a large, randomized trial in acute MI patients facing very long delays—3 to 4 hours—before receiving therapy, as is typical for patients facing long travel distances or who must be transferred to a hospital with interventional facilities (90). It was an open-label, 1:1 study that randomized patients to either full-dose tenecteplase plus PCI (facilitated PCI) or to primary PCI with unfractionated heparin. GP IIb/IIIa inhibitors were used either in bail-out situations in patients pretreated with fibrinolytic therapy or at the investigator's discretion in the PCI-alone arm. The primary end point—death, cardiogenic shock, or congestive heart failure within 90 days—was significantly lower in the PCI-alone group compared with the facilitated PCI arm (90). The significantly higher rate of stroke at 90 days in the facilitated PCI group was mainly due to a significant increase in the rate of intracranial hemorrhage (90). Additionally, in the recent BRAVE trial examining the impact of PCI with two boluses of 5 U reteplase plus abciximab versus abciximab alone (12 hours), the infarct size was not improved after PCI with reteplase, and bleeding was more frequent (91).
|
Table 120.8 Advantages and disadvantages of primary percutaneous coronary intervention (PCI) versus thrombolysis |
|||
|
On the other hand, the recently published CARESS-in-AMI (Combined Abciximab RE-teplase Stent Study in Acute Myocardial Infarction) suggested that immediate transfer for PCI improves outcomes (composite of death, reinfarction, or refractory ischaemia at 30 days) in high-risk patients with STEMI treated at a non-interventional centre with half-dose reteplase and abciximab compared to standard medical therapy with transfer for rescue angioplasty (91A). Based on these findings and waiting for further trial results, organisation of networks to move patients given a thrombolytic drug to institutions with catheterisation laboratories seems a reasonable option, since primary angioplasty cannot be implemented everywhere.
Rescue Percutaneous Coronary Intervention
Rescue PCI refers to a PCI procedure performed in patients without evidence of a response to thrombolytic treatment within 90 minutes after therapy; that is, there is less than 50% ST-segment resolution and/or symptom regression within 90 minutes after treatment.
|
|
|
Figure 120.4. Meta-analysis of 23 randomized trials of primary percutaneous coronary intervention (PCI) versus thrombolysis. (Modified from Keeley EC, Grines CL. Primary coronary intervention for acute myocardial infarction. JAMA. 2004;291[6]:736–739.) |
Feasibility studies have demonstrated success of PCI in achieving coronary patency and flow, and current guidelines recommend it only for certain high-risk subgroups of patients (1,2,34).
In the recently published Rescue Angioplasty versus Conservative Treatment or Repeat Thrombolysis (REACT) trial, event-free survival after failed thrombolytic therapy was significantly higher with rescue PCI than with repeated thrombolysis or conservative treatment (92). However, available data are still insufficient to demonstrate whether there is improvement in mortality or further MI with this strategy.
Transport for Primary Percutaneous Coronary Intervention
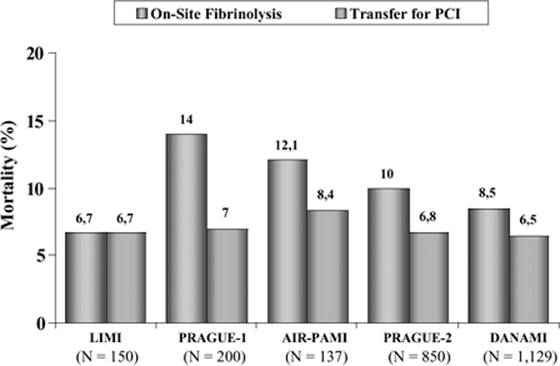
For hospitals without on-site PCI facilities, careful consideration needs to be given to the potential benefits of PCI following transfer to an intervention center versus fibrinolysis (93). For instance, the DANAMI 2 study suggested that for transfer times of 2 hours or less from a community hospital to the start of PCI, there is a significant reduction in death, reinfarction, and stroke compared with thrombolysis (94). After early reports of feasibility (95), five trials (94,96,97,98,99) randomly assigned patients with STEMI in community hospitals without PCI capability to immediate transfer to hospitals that could perform primary PCI or to on-site thrombolytic therapy (Fig. 120.5). Complications were rare during the transfer, with a 0.5% risk for death, a 0.7% to 1.4% risk for ventricular dysrhythmias, and a 2% risk for second- or third-degree heart block (94,96,97,98,99). A meta-analysis of these trials (100), which included a trial comparing primary PCI with prehospital thrombolytic therapy (13), compared outcomes of 1,887 patients randomly assigned to emergency transfer for primary PCI and 1,863 patients randomly assigned to on-site or prehospital thrombolytic therapy. The combined end point of death, reinfarction, and stroke at 30 days was reduced by 42% (p <0.001) in the group transferred for primary PCI as compared with the group receiving thrombolytic therapy (100). However, these findings have a limited application in the daily clinical practice. For instance, most patients randomly assigned to transfer for primary PCI were treated in high-volume PCI centers: in the largest trial 96% of patients were transferred in less than 2 hours and the median interval from symptom onset to first balloon inflation was only 224 minutes (94). Accordingly, these data should not be extrapolated to transfer for primary PCI in low-volume centers or to situations in which transfer delays exceed 2 to 3 hours. More importantly, the time from symptom onset to first balloon inflation must be minimized, requiring that the transferred patient is delivered directly to an experienced “ready and waiting” catheterization laboratory (101).
The Crucial Role of Time in Reperfusion Therapies
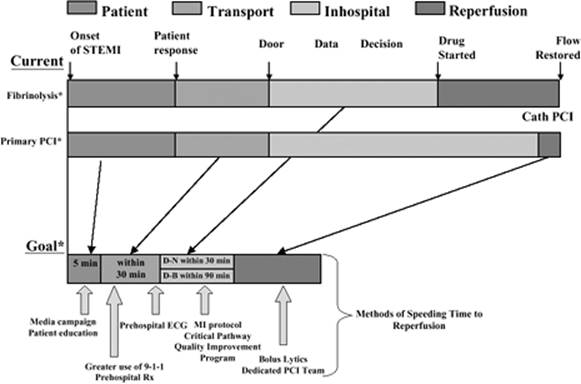
The shorter the time is from symptom onset to treatment, the greater the survival benefit with either reperfusion therapy (102,103,104,105,106,107). The choice between therapies should take into account reperfusion treatment times (1,2) (Figs. 120.6 and 120.7). Time delay is critically important, especially within the first 3 to 4 hours following symptom onset (1,2,108). Overall, there is a progressive decrease of about 1.6 deaths per hour of delay per 1,000 patients treated. However, within the first 2 hours, the reduction in mortality is twice as large as beyond 2 hours (Fig. 120.8). Hence, the European guidelines for the management of acute MI recommend that for those patients with clear-cut changes of acute infarction, no more than 20 minutes should elapse between hospital arrival and the administration of thrombolytic therapy (or prehospital administration) or no more than 60 minutes between hospital arrival and balloon inflation for primary PCI (1,2). A second and critically important reason for minimizing prehospital delay is to treat early ventricular fibrillation. At least as many deaths may be saved by prompt resuscitation therapy in early acute MI as are saved by reperfusion therapy.
While the relationship between mortality and time delay from symptom onset to treatment is stringent in patients with STEMI who are receiving thrombolytic therapy (109,110,111), it is much weaker in patients undergoing primary PCI (108,112,113) (Fig. 120.9). Consequently, favorable results obtained from primary PCI depend less on the time to treatment than does thrombolytic therapy. On the other hand, more recent trials showed that the benefits of primary PCI may diminish with excessive delays in opening the infarct-related artery (106,107,114,115) (Fig. 120.10).
|
|
|
Figure 120.5. Randomized trials comparing on-site fibrinolysis and transfer for primary percutaneous coronary intervention (PCI). |
|
|
|
Figure 120.6. Major components of time delay between onset of symptoms from ST elevation myocardial infarction (STEMI) and restoration of flow in the infarct related artery. PCI, percutaneous coronary intervention. (Modified from Antman EM, Anbe DT, Armstrong PW, et al. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Canadian Cardiovascular Society. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [committee to revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction]. Circulation. 2004;110[9]:e82–e292.) |
Several mechanisms have been proposed to explain this difference in time-to-treatment effect. With thrombolytic therapy, there is an inverse relationship between the rate of achieving normal blood flow and the time-to-treatment interval (116). In addition, patients treated with thrombolytic therapy have an increased risk for mechanical complications, such as myocardial rupture, with progressive increases in time to treatment (116). In patients treated with primary PCI, on the other hand, mechanical complications are rare. Interestingly, thrombolytic therapy is more often complicated by reocclusion of the infarct-related artery, reinfarction, and worse long-term survival as compared with primary PCI (117). Finally, the extent of myocardial salvage is inversely proportional to the time to treatment in patients treated with thrombolytic therapy, but is independent of time to treatment in primary PCI, particularly with adjunctive stenting (118).
Coronary Artery Bypass Surgery
The number of patients who need coronary artery bypass grafting (CABG) in the acute phase of STEMI is quite limited. It may, however, be indicated when PCI has failed, when there has been a sudden occlusion of a coronary artery during catheterization, if PCI is not feasible, in selected patients in cardiogenic shock, or in association with surgery for a ventricular septal defect or mitral regurgitation due to papillary muscle dysfunction and rupture (1,2).
Long-term Post–Myocardial Infarction Pharmacologic Treatment
The results of large randomized clinical trials have formed the basis for the long-term management of acute MI. Evidence from these trials has demonstrated that pharmacologic therapies aimed at limiting risk factors and coronary plaque instability with lipid-lowering therapies, and focused on inhibiting post-MI remodeling with neurohumoral antagonists—namely ACE inhibitors, angiotensin II receptor blockers (ARBs; e.g., valsartan), β-blockers (e.g., carvedilol), and, most recently, aldosterone antagonists (e.g., eplerenone)—can significantly improve long-term outcomes including death, reinfarction, and worsening CHF (1,2) (Table 120.9). Clinical trials have also shown the benefits of antiplatelet and anticoagulant therapies, including aspirin and warfarin, as well as newer platelet inhibitors in limiting recurrent myocardial ischemia and its consequences (1,2) (Table 120.10).
|
|
|
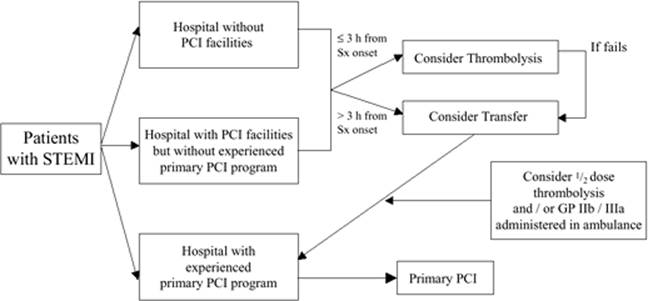
Figure 120.7. Possible strategies for the acute management of ST elevation myocardial infarction (STEMI) patients based on the hospital availability of experienced primary percutaneous coronary intervention (PCI) program. GP, glycoprotein. |
|
|
|
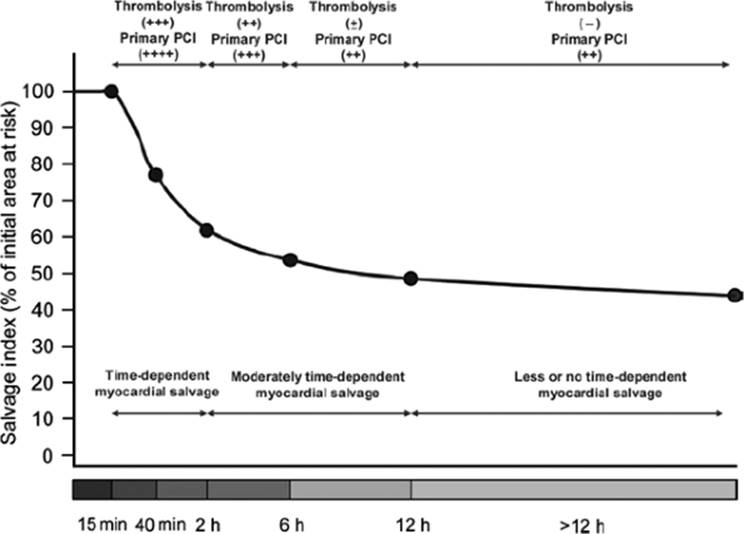
Figure 120.8. Time dependency of myocardial salvage expressed as percentage of initial area at risk. The initial parts of the curve up to 2 hours were reconstructed based on the experimental studies. The other parts of the curve showing myocardial salvage from 2 to 12 hours from the symptom onset are reconstructed according to the data of scintigraphic studies. Efficacy of reperfusion is expressed as follows: ++++, very effective; +++, effective; ++, moderately effective; ±, uncertainly effective; -, not effective. PCI, percutaneous coronary intervention. (From Schomig A, Ndrepepa G, Kastrati A. Late myocardial salvage: time to recognize its reality in the reperfusion therapy of acute myocardial infarction. Eur Heart J. 2006;27:1900–1907.) |
Special Issues
Acute Congestive Heart Failure and Cardiogenic Shock
Acute CHF arises from a sudden injury or structural failure and constitutes approximately 10% of CHF admissions. Etiologies include acute coronary syndromes (ACSs), acute valvular dysfunction (e.g., those due to endocarditis, aortic dissection, or papillary muscle rupture), pericardial disease, new arrhythmia (especially atrial fibrillation), myocarditis, and malignant hypertension (119).
Patients who present with ACS accompanied by CHF have considerable mortality and clearly benefit from emergent revascularization (120,121) (Fig. 120.11). Medical management includes the standard therapies for ACS (antiplatelet therapy and anticoagulation), with the exception that β-blockers are contraindicated in the presence of systolic CHF. β-Blockers are not contraindicated, and are probably helpful, in an ACS with diastolic CHF.
For patients with hypotension or hypoperfusion, serious consideration should be given to placement of a pulmonary artery catheter. An IABP is the most physiologic for improving cardiac output in the setting of ACS as it improves coronary perfusion while increasing blood pressure and decreasing afterload (122) (Fig. 120.12). Notably, all currently available inotropes will worsen ischemia and are proarrhythmic.
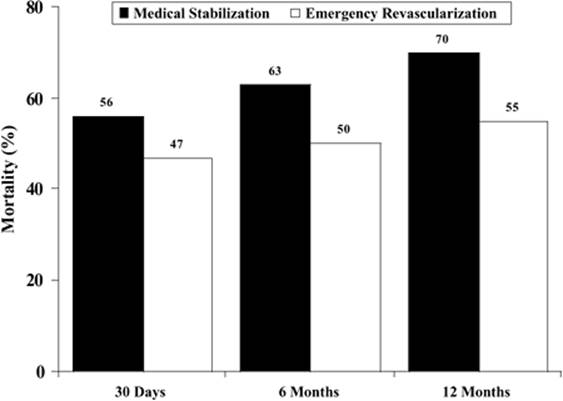
Cardiogenic shock remains the leading cause of death in patients hospitalized with acute MI (123). The SHOCK randomized trial (124,125) demonstrated that in patients with acute MI complicated by cardiogenic shock, early mechanical revascularization reduced 6- and 12-month mortality compared with initial medical stabilization—including IABP counterpulsation and fibrinolytic therapy—followed by late or no revascularization (Fig. 120.13). There was a significant interaction between treatment and age, with apparent lack of benefit of early revascularization for the small subset of patients aged 75 years or older (124,125). Based on these findings, the American College of Cardiology (ACC) and the American Heart Association (AHA) elevated early mechanical revascularization for cardiogenic shock to a class I recommendation for patients younger than 75 years with ST elevation left bundle branch block acute MI in their revised guidelines for the management of acute MI (1).
|
|
||||||
|
Figure 120.9. Time dependence of myocardial salvage according to time-to-treatment interval in patients with ST elevation myocardial infarction (STEMI) treated by percutaneous coronary intervention (PCI) or thrombolysis. A: Myocardial salvage expressed as percentage of the left ventricle (LV). B: Myocardial salvage expressed as proportion of the initial area at risk salvaged by reperfusion therapy. (From Schomig A, Ndrepepa G, Kastrati A. Late myocardial salvage: time to recognize its reality in the reperfusion therapy of acute myocardial infarction. Eur Heart J. 2006;27:1900–1907.) |
||||||
|
Table 120.9 American College of Cardiology/American Heart Association guidelines for management of ST elevation myocardial infarction |
||||||
|
||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
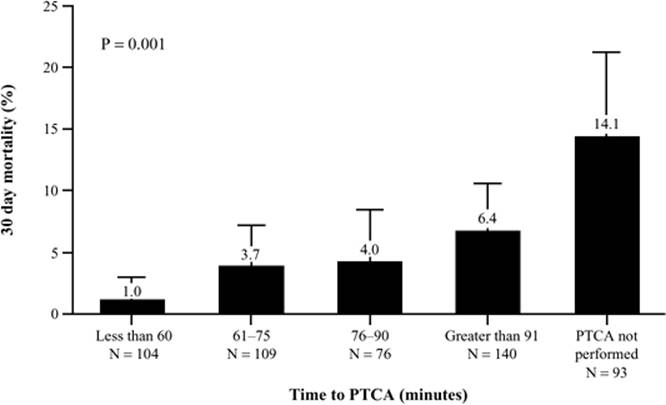
Figure 120.10. Relationship between 30-day mortality and time from study enrollment to first balloon inflation. PTCA, percutaneous transluminal coronary angioplasty. (Modified from Berger PB, Ellis SG, Holmes DR Jr, et al. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction: results from the Global Use of Strategies to Open Occluded Arteries in Acute Coronary Syndromes [GUSTO-IIb] trial. Circulation. 1999;100:14–20.) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Table 120.10 Large-Scale Clinical Trials of Therapy for AMI survivors |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
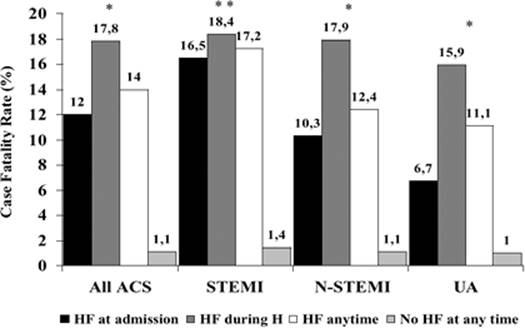
|
Figure 120.11. Impact of presence of heart failure (HF) at admission or development of HF during hospitalization (H) in all patients with acute coronary syndromes (ACSs). STEMI, ST elevation myocardial infarction; N-STEMI, non–ST elevation myocardial infarction; UA, unstable angina. (Modified from Steg PG, Dabbous OH, Feldman LJ, et al.; Global Registry of Acute Coronary Events Investigators. Determinants and prognostic impact of heart failure complicating acute coronary syndromes: observations from the Global Registry of Acute Coronary Events [GRACE]. Circulation. 2004;109:494–499.) |
|
|
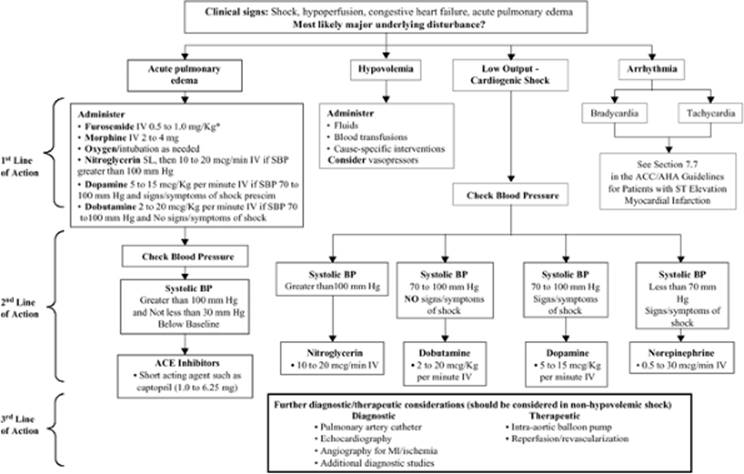
|
Figure 120.12. Emergency management of complicated ST elevation myocardial infarction (STEMI). The emergency management of patients with cardiogenic shock, acute pulmonary edema, or both is outlined. HF, heart failure; IV, intravenous; SL, sublingual; SBP, systolic blood pressure; BP, blood pressure; ACE, angiotensin-converting enzyme; MI, myocardial infarction. (Modified from Antman EM, Anbe DT, Armstrong PW, et al. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Canadian Cardiovascular Society. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [committee to revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction]. Circulation. 2004;110[9]:e82–292.) |
|
|
|
Figure 120.13. Mortality of medical stabilization vs. emergency revascularization by percutaneous coronary intervention (PCI) in ST elevation myocardial infarction (STEMI) patients with shock. (Modified from Hochman JS, Sleeper LA, Webb JG, et al.; SHOCK Investigators. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med. 1999;341:625–634.) |
A large observational study of patients hospitalized with acute MI suggests that over the last 10 years, there has been a relatively stable rate of acute MI complicated by cardiogenic shock, but there has been a decline in the associated in-hospital mortality rate for hospitals with revascularization capability (126). There was a significant increase in total and primary PCI rates. Primary PCI also was independently associated with a reduction in the odds of death during hospitalization even after adjustment with the propensity score. There were low and unchanging rates of IABP use, while fibrinolytic therapy use diminished over time (126,127).
Other Possible In-hospital Complications
Mitral Regurgitation
In a community-based study, mitral regurgitation was present in a remarkable 50% of 773 patients who underwent Doppler echocardiographic examination within 30 days of MI. After a mean follow-up of 4.7 years, a graded positive association was observed between the severity of mitral regurgitation and CHF or death (128). Subsequent echocardiographic and early invasive studies demonstrated the prognostic significance of even mild mitral regurgitation after an acute MI (129).
Deep Vein Thrombosis and Pulmonary Embolism
These complications are now relatively uncommon after MI, except in patients kept in bed for comorbidities or complications of MI. When they occur they should be treated with therapeutic doses of LMWH, followed by oral anticoagulation for 3 to 6 months.
Intraventricular Thrombus and Systemic Emboli
Echocardiography may reveal intraventricular thrombi, especially in patients with a large anterior MI. If the thrombi are mobile or protuberant, they should be treated initially with intravenous UFH or LMWH and subsequently with oral anticoagulants for at least 3 to 6 months.
Pericarditis
Acute pericarditis may complicate MI and is associated with a worse outcome. It gives rise to chest pain that may be misinterpreted as recurrent MI or angina. The pain is, however, distinguished by its sharp nature, and its relationship to posture and respiration. The diagnosis may be confirmed by a pericardial rub. If the pain is troublesome, it may be treated by high-dose oral or intravenous aspirin, nonsteroidal anti-inflammatory agents, or steroids. A hemorrhagic effusion with tamponade is uncommon, is especially associated with anticoagulant treatment, and may usually be recognized echocardiographically. Treatment is by pericardiocentesis if hemodynamic embarrassment occurs.
Late Ventricular Dysrhythmias
Ventricular tachycardia (VT) and ventricular fibrillation (VF) occurring on the first day have a low predictive value for recurring dysrhythmias. Dysrhythmias developing later are liable to recur and are associated with a high risk of death. VT or VF during the first week postinfarction is associated with more extensive myocardial damage; a careful assessment of coronary anatomy and ventricular function should always be undertaken. If it is probable that the arrhythmia is induced by ischemia, revascularization by PCI or surgery should be considered. If this is unlikely, a variety of therapeutic approaches are available, which are, as yet, inadequately researched. These include the use of β-blockers, amiodarone, electrophysiologically guided antidysrhythmic therapy, and/or insertion of an implantable converter defibrillator.
Postinfarction Angina and Ischemia
The routine use of elective PCI following fibrinolytic therapy has been compared with a conservative approach in several randomized trials. It may be concluded that routine PCI in the absence of spontaneous or provocable ischemia does not improve LV function or survival (130,131). In treating angina or recurrent or inducible ischemia, however, whether due to reocclusion or to a residual stenosis, revascularization by PCI or CABG has a definite role (130). It may also be of value in managing dysrhythmias associated with persistent ischemia. CABG surgery may be indicated if symptoms are not controlled by other means or if coronary angiography demonstrates lesions, such as left main stenosis or three-vessel disease with poor LV function, for which surgery improves prognosis.
Right Ventricular Infarction
Right ventricular infarction encompasses a spectrum of disease states ranging from asymptomatic mild RV dysfunction through cardiogenic shock. Most patients demonstrate a return of normal RV function over a period of weeks to months, which suggests that RV stunning, rather than irreversible necrosis, has occurred. In this sense, RV ischemia can be demonstrated in up to half of all inferior STEMIs, although only 10% to 15% of patients show classic hemodynamic abnormalities of clinically significant RV infarction (132,133). Right ventricular infarction with hemodynamic abnormalities accompanying inferior STEMI is associated with a significantly higher mortality (25%–30%) and thus identifies a high-risk subgroup of patients with inferior STEMIs (6%) who should be considered high-priority candidates for reperfusion (132). One group of investigators reported a 31% in-hospital mortality rate in patients with inferior STEMIs complicated by RV infarction compared with 6% in patients who had an inferior STEMI without RV involvement (131). An analysis of patients with predominant RV infarction and cardiogenic shock from the SHOCK trial registry demonstrated an unexpectedly high mortality rate similar to that for patients with LV shock (53.1% vs. 60.8%) (134).
The treatment of patients with RV ischemic dysfunction is different and, in several ways, diametrically opposed to management of LV dysfunction. It includes early maintenance of RV preload, reduction of RV afterload, inotropic support of the dysfunctional RV, and early reperfusion (135). Because of their influence on preload, drugs routinely used in management of LV infarctions, such as nitrates and diuretics, may reduce cardiac output and produce severe hypotension when the RV is ischemic. Indeed, a common clinical presentation is profound hypotension after administration of sublingual nitroglycerin, with the degree of hypotension often out of proportion to the ECG severity of the infarct. Volume loading with normal saline alone often resolves in patients with RV ischemia/infarction (136).
Although volume loading is a critical first step in the management of hypotension associated with RV ischemia/infarction, inotropic support—in particular, with dobutamine—should be initiated promptly if cardiac output fails to improve after 0.5 to 1 L of fluid has been administered. Excessive volume loading may further complicate the right-sided filling pressure increase and RV dilatation, resulting in decreased LV output (136,137) secondary to shift of the interventricular septum toward the LV.
Indications for Hemodynamic Monitoring
It is important to accurately assess the severity of left ventricular dysfunction because maneuvers performed in the coronary care unit may worsen this state. More than half of the patients with a moderate reduction in resting cardiac output and an increase in left ventricular filling pressure have no clinical signs of left ventricular dysfunction. Clinical evaluation frequently does not identify patients with low cardiac output who have normal chest radiographs and physical examinations. However, correlation of the chest radiograph and clinical evaluation with hemodynamic measurements have demonstrated that the presence of cardiomegaly, gallop rhythms, and pulmonary edema may help predict which patients with MI will develop shock (138,139,140).
There is an unfortunate tendency to institute potent therapeutic measures in patients with myocardial infarction before precise hemodynamic indices are known. Intravenous furosemide, for example, may create a decline in pulmonary artery occlusion pressure (PAOP) without compromising the cardiac output if ventricular filling pressures are elevated and there is pulmonary congestion. However, if the clinical diagnosis of CHF is incorrect and the PAOP is normal, diuretic therapy may actually decrease the cardiac output and cause deterioration of an already compromised myocardial flow reserve. This can be particularly detrimental in patients who present with RV infarction.
References
1. Antman EM, Anbe DT, Armstrong PW, et al. American College of Cardiology; American Heart Association Task Force on Practice Guidelines; Canadian Cardiovascular Society. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (committee to revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). Circulation. 2004;110(9):e82–e292.
2. Van de Werf F, Ardissino D, Betriu A, et al. Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2003;24(1):28–66.
2a. Thygesen K, Alpert JS, White HD. Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Circulation. 2007;116:2634–2653.
3. Rogers WJ, Canto JG, Lambrew CT, et al. Temporal trends in the treatment of over 1.5 million patients with myocardial infarction in the US from 1990 through 1999: the National Registry of Myocardial Infarction 1, 2 and 3. J Am Coll Cardiol. 2000;36:2056–2063.
4. Kleiman NS, White HD. The declining prevalence of ST elevation myocardial infarction in patients presenting with acute coronary syndromes. Heart. 2005;91;1121–1123.
5. Braunwald E, Pfeffer MA. Ventricular enlargement and remodeling following acute myocardial infarction: mechanisms and management. Am J Cardiol. 1991;68:1D–6D.
6. Pfeffer MA. Left ventricular remodeling after acute myocardial infarction. Annu Rev Med. 1995;46:455–466.
7. Antman EM, Braunwald E. Acute myocardial infarction. In: Braunwald E, Zipes DP, Libby P, eds. Heart Disease: A Textbook of Cardiovascular Medicine. 6th ed. Philadelphia: WB Saunders Co Ltd; 2001:1114–1251.
8. Hochman JS, Califf RM. Acute myocardial infarction. In: Smith TW, ed. Cardiovascular Therapeutics: A Companion to Braunwald's Heart Disease. 2nd ed. Philadelphia: WB Saunders Co Ltd; 2001:235–291.
9. Collins R, Peto R, Baigent C, et al. Aspirin, heparin, and fibrinolytic therapy in suspected acute myocardial infarction. N Engl J Med. 1997;333:847–860.
10. Boersma E, Mercado N, Poldermans D, et al. Acute myocardial infarction. Lancet. 2003;361:847–858.
11. Morrison LJ, Verbeek PR, McDonald AC, et al. Mortality and prehospital thrombolysis for acute myocardial infarction: a meta-analysis. JAMA. 2000;283:2686–2692.
12. GREAT Group. Feasibility, safety and efficacy of domiciliary thrombolysis by general practitioners. BMJ. 1992;305:548–553.
13. Bonnefoy E, Lapostolle F, Leizorovicz A, et al., on behalf of the CAPTIM Study Group. Primary angioplasty versus prehospital fibrinolysis in acute myocardial infarction: a randomised study. Lancet. 2002;360:825–829.
14. Boersma E, Maas AC, Deckers JW, et al. Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Lancet. 1996;348:771–775.
15. Danchin N, Blanchard D, Steg PG, et al. Impact of prehospital thrombolysis for acute myocardial infarction on 1-year outcome results from the French nationwide USIC 2000 registry. Circulation. 2004;110:1909–1915.
16. Stenestrand U, Lindback J, Wallentin L; RIKS-HIA Registry. Long-term outcome of primary percutaneous coronary intervention vs prehospital and in-hospital thrombolysis for patients with ST-elevation myocardial infarction. JAMA. 2006;296(14):1749–1756.
17. Gibson CM, Cannon CP, Murphy SA, et al. Relationship of TIMI myocardial perfusion grade to mortality after administration of thrombolytic drugs. Circulation. 2000;101:125–130.
18. White H; Hirulog and Early Reperfusion or Occlusion (HERO)-2 Trial Investigators. Thrombin-specific anticoagulation with bivalirudin versus heparin in patients receiving fibrinolytic therapy for acute myocardial infarction: the HERO-2 randomised trial. Lancet. 2001;358(9296):1855–1863.
19. Maroko PR, Radvany P, Braunwald E, et al. Reduction of infarct size by oxygen inhalation following acute coronary occlusion. Circulation. 1975;52:360–368.
20. Madias JE, Hood WB. Reduction of precordial ST-segment elevation in patients with anterior myocardial infarction by oxygen breathing. Circulation. 1976;53:I198–200.
21. Fillmore SJ, Shapiro M, Killip T. Arterial oxygen tension in acute myocardial infarction: serial analysis of clinical state and blood gas changes. Am Heart J. 1970;79:620–629.
22. Abrams J. Hemodynamic effects of nitroglycerin and long-acting nitrates. Am Heart J. 1985;110:216–224.
23. Gorman MW, Sparks HV. Nitroglycerin causes vasodilatation within ischaemic myocardium. Cardiovasc Res. 1980;14:515–521.
24. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. Lancet. 1995;345:669–685.
25. Yusuf S, Peto R, Lewis J, et al. Beta-blockade during and after myocardial infarction: an overview of the randomised trials. Prog Cardiovasc Dis. 1985;27:335–371.
26. The MIAMI Trial Research Group. Metoprolol in acute myocardial infarction (MIAMI). A randomised placebo controlled international trial. Eur Heart J. 1985;6:199–211.
27. Herlitz J, Waagstein F, Lindqvist J, et al. Effect of metoprolol on the prognosis for patients with suspected acute myocardial infarction and indirect signs of congestive heart failure (a subgroup analysis of the Goteborg Metoprolol Trial). Am J Cardiol. 1997;80:40J–44J.
28. ISIS-1 collaborative group. Randomised trial of intravenous atenolol among 16 027 cases of suspected acute myocardial infarction: ISIS-1. Lancet. 1986;2:57–66.
29. COMMIT (ClOpidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Early intravenous then oral metoprolol in 45 852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005;366:1622–1632
30. Mehta SR, Yusuf S, Peters RJ, et al., for the Clopidogrel in Unstable angina to prevent Recurrent Events trial (CURE) Investigators. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358:527–533.
31. Schömig A, Neumann FJ, Kastrati A, et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med. 1996;334:1084–1089.
32. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet. 1996;348:1329–1339.
33. Leon MB, Baim DS, Popma JJ, et al., for the Stent Anticoagulation Restenosis Study Investigators. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. N Engl J Med. 1998;339:1665–1671.
34. Smith SC Jr, Dove JT, Jacobs AK, et al. ACC/AHA guidelines for percutaneous coronary intervention (revision of the 1993 PTCA guidelines): a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (committee to revise the 1993 Guidelines for Percutaneous Transluminal Coronary Angioplasty). Circulation. 2001;103:3019–3041.
35. Sabatine MS, Cannon CP, Gibson CM, et al. Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Engl J Med. 2005;352:1179–1189.
36. Scirica BM, Sabatine MS, Morrow DA, et al. The role of clopidogrel in early and sustained arterial patency after fibrinolysis for ST-segment elevation myocardial infarction. The ECG CLARITY–TIMI 28 Study. J Am Coll Cardiol. 2006;48:37–42.
37. Sugidachi A, Asai F, Ogawa T, et al. The in vivo pharmacological profile of CS-747, a novel antiplatelet agent with platelet ADP receptor antagonist properties. Br J Pharmacol. 2000;129:1439–1446.
38. Wiviott SD, Antman EM, Winters KJ, et al. A randomised comparison of prasugrel (CS-747), a novel thienopyridine P2Y12 antagonist, to clopidogrel in percutaneous coronary intervention; results of the Joint Utilization of Medications to Block Platelets Optimally (JUMBO)-TIMI 26 Trial. Circulation. 2005;111:3366–3373.
39. Lincoff AM, Califf RM, Topol EJ. Platelet glycoprotein IIb/IIIa blockade in coronary artery disease. J Am Coll Cardiol. 2000;35:1103–1115.
40. Kloner RA, Dai W. Glycoprotein IIb/IIIa inhibitors and no-reflow. J Am Coll Cardiol. 2004;43:284–286.
41. De Luca G, Suryapranata H, Stone GW, et al. Abciximab as adjunctive therapy to reperfusion in acute ST-segment elevation myocardial infarction: a meta-analysis of randomized trials. JAMA. 2005;293(14):1759–1765.
42. Antman EM. The search for replacements for unfractionated heparin. Circulation. 2001;103:2310–2314.
43. Ogilby JD, Kopelman HA, Klein LW, et al. Adequate heparinization during PTCA: assessment using activated clotting times. Cathet Cardiovasc Diagn. 1989;18:206–209.
44. Assessment of the Safety and Efficacy of a New Thrombolytic Regimen (ASSENT)-3 Investigators. Efficacy and safety of tenecteplase in combination with enoxaparin, abciximab, or unfractionated heparin: the ASSENT-3 randomised trial in acute myocardial infarction. Lancet. 2001;358:605–613.
45. Wallentin L, Goldstein P, Armstrong PW, et al. Efficacy and safety of tenecteplase in combination with the low-molecular-weight heparin enoxaparin or unfractionated heparin in the prehospital setting: the Assessment of the Safety and Efficacy of a New Thrombolytic Regimen (ASSENT)-3 PLUS randomized trial in acute myocardial infarction. Circulation. 2003;108:135–142.
46. Ross AM, Molhoek P, Lundergan C, et al., for the HART II Investigators. Randomized comparison of enoxaparin, a low-molecular-weight heparin, with unfractionated heparin adjunctive to recombinant tissue plasminogen activator thrombolysis and aspirin: second trial of Heparin and Aspirin Reperfusion Therapy (HART II). Circulation. 2001;104:648–652.
47. Baird SH, Menown IB, Mcbride SJ, et al. Randomized comparison of enoxaparin with unfractionated heparin following fibrinolytic therapy for acute myocardial infarction. Eur Heart J. 2002;23:627–632.
48. Antman EM, Louwerenburg HW, Baars HF, et al. Enoxaparin as adjunctive antithrombin therapy for ST-elevation myocardial infarction: results of the ENTIRE-Thrombolysis in Myocardial Infarction (TIMI) 23 Trial. Circulation. 2002;105:1642–1649.
49. Wallentin L, Bergstrand L, Dellborg M, et al. Low molecular weight heparin (dalteparin) compared to unfractionated heparin as an adjunct to rt-PA (alteplase) for improvement of coronary artery patency in acute myocardial infarction-the ASSENT Plus study. Eur Heart J. 2003;24:897–908.
50. Direct thrombin inhibitors in acute coronary syndromes: principal results of a meta-analysis based on individual patients' data. Lancet. 2002;359:294–302.
51. Stone GW, McLaurin BT, Cox DA, et al.; ACUITY Investigators. Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355(21):2203–2216.
52. Exaire JE, Butman SM, Ebrahimi R, et al.; REPLACE-2 Investigators. Provisional glycoprotein IIb/IIIa blockade in a randomized investigation of bivalirudin versus heparin plus planned glycoprotein IIb/IIIa inhibition during percutaneous coronary intervention: predictors and outcome in the Randomized Evaluation in Percutaneous coronary intervention Linking Angiomax to Reduced Clinical Events (REPLACE)-2 trial. Am Heart J. 2006;152(1):157–163.
53. Coussement PK, Bassand JP, Convens C, et al., for the PENTALYSE investigators. A synthetic factor-Xa inhibitor (ORG31540/SR9017A) as an adjunct to fibrinolysis in acute myocardial infarction. The PENTALYSE study. Eur Heart J. 2001;22:1716–1724.
54. Yusuf S, Mehta SR, Chrolavicius S, et al.; OASIS-6 Trial Group. Effects of fondaparinux on mortality and reinfarction in patients with acute ST-segment elevation myocardial infarction: the OASIS-6 randomized trial. JAMA. 2006;295(13):1519–1530.
55. GISSI-3. Effects of lisinopril and transdermal glyceryl trinitrate singly and together on 6-week mortality and ventricular function after acute myocardial infarction. Gruppo Italiano per lo Studio della Sopravvivenza nell'infarto Miocardico. Lancet. 1994;343:1115–1122.
56. ISIS-4. A randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium in 58,050 patients with suspected acute myocardial infarction. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. Lancet. 1995;345:669–685.
57. Chinese Cardiac Study Collaborative Group. Oral captopril versus placebo among 13,634 patients with suspected myocardial infarction: interim report from the Chinese Cardiac study (CCS-1). Lancet. 1995;345:686–687.
58. Swedberg K, Held P, Kjekshus J, et al. Effects of the early administration of enalapril on mortality in patients with acute myocardial infarction: results of the Cooperative New Scandinavian Enalapril Survival Study II (CONSENSUS II). N Engl J Med. 1992;327:678–684.
59. Pfeffer MA, Hennekens CH. When a question has an answer: rationale for our early termination of the HEART trial. Am J Cardiol. 1995;75:1173–1175.
60. The Danish Study Group on Verapamil in Myocardial Infarction. Verapamil in acute myocardial infarction. Eur Heart J. 1984;5:516–528.
61. Held PH, Yusuf S. Effects of beta-blockers and calcium channel blockers in acute myocardial infarction. Eur Heart J. 1993;14:18–25.
62. Hilton TC, Miller DD, Kern MJ. Rational therapy to reduce mortality and reinfarction following myocardial infarction. Am Heart J. 1991;122:1740–1750.
63. Effect of verapamil on mortality and major events after acute myocardial infarction: the Danish Verapamil Infarction Trial II (DAVIT II). Am J Cardiol. 1990;66:779–785.
64. The Multicenter Diltiazem Postinfarction Trial Research Group. The effect of diltiazem on mortality and reinfarction after myocardial infarction. N Engl J Med. 1988;319:385–392.
65. Gibson RS, Boden WE, Theroux P, et al. Diltiazem and reinfarction in patients with non–Q-wave myocardial infarction: results of a double-blind, randomized, multicenter trial. N Engl J Med. 1986;315:423–429.
66. Caldicott LD, Hawley K, Heppel R, et al. Intravenous enoximone or dobutamine for severe heart failure after acute myocardial infarction: a randomized double-blind trial. Eur Heart J. 1993;14:696–700.
67. Karlsberg RP, DeWood MA, DeMaria AN, et al. The milrinone-dobutamine Study Group. Comparative efficacy of short-term intravenous infusions of milrinone and dobutamine in acute congestive heart failure following acute myocardial infarction. Clin Cardiol. 1996;19:21–30.
68. Gillespie TA, Ambos HD, Sobel BE, et al. Effects of dobutamine in patients with acute myocardial infarction. Am J Cardiol. 1977;39:588–594.
69. Bayram M, De Luca L, Massie BM, et al. Dobutamine, milrinone and dopamine in acute heart failure syndromes: a reassessment. Am J Cardiol. 2005;96(6A):47G–58G.
70. De Luca L, Colucci WS, Nieminen MS, et al. Evidence-based use of levosimendan in different clinical settings. Eur Heart J. 2006;27(16):1908–1920.
71. Teo KK, Yusuf S, Collins R, et al. Effects of intravenous magnesium in suspected acute myocardial infarction: overview of randomised trials. BMJ. 1991;303:1499–1503.
72. Antman EM, Lau J, Kupelnick B, et al. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240–248.
73. Magnesium in Coronaries (MAGIC) Trial Investigators. Early administration of intravenous magnesium to high-risk patients with acute myocardial infarction in the Magnesium in Coronaries (MAGIC) Trial: a randomised controlled trial. Lancet. 2002;360:1189–1196.
74. Rasmussen HS, McNair P, Norregard P, et al. Intravenous magnesium in acute myocardial infarction. Lancet. 1986;1:234–236.
75. Smith LF, Heagerty AM, Bing RF, et al. Intravenous infusion of magnesium sulphate after acute myocardial infarction: effects on arrhythmias and mortality. Int J Cardiol. 1986;12:175–183.
76. Abraham AS, Rosenmann D, Kramer M, et al. Magnesium in the prevention of lethal arrhythmias in acute myocardial infarction. Arch Intern Med. 1987;147:753–755.
77. Ceremuzynski L, Jurgiel R, Kulakowski P, et al. Threatening arrhythmias in acute myocardial infarction are prevented by intravenous magnesium sulfate. Am Heart J. 1989;118:1333–1334.
78. Shechter M, Hod H, Marks N, et al. Beneficial effect of magnesium sulfate in acute myocardial infarction. Am J Cardiol. 1990;66:271–274.
79. Feldstedt M, Boesgaard S, Bouchelouche P, et al. Magnesium substitution in acute ischaemic heart syndromes. Eur Heart J. 1991;12:1215–1218.
80. Woods KL, Fletcher S, Roffe C, et al. Intravenous magnesium sulphate in suspected acute myocardial infarction: results of the second Leicester Intravenous Magnesium Intervention Trial (LIMIT-2). Lancet. 1992;339:1553–1558.
81. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: part 6: advanced cardiovascular life support: section 5: pharmacology I: agents for arrhythmias. The American Heart Association in collaboration with the International Liaison Committee on Resuscitation. Circulation. 2000;102:I112–128.
82. Lie KJ, Wellens HJ, Van Capelle FJ, et al. Lidocaine in the prevention of primary ventricular fibrillation. A double-blind randomized study of 212 consecutive patients. N Engl J Med. 1974;29:1324–1326.
83. Koster RW, Dunning AJ. Intramuscular lidocaine for prevention of lethal arrhythmias in the prehospitalization phase of acute myocardial infarction. N Engl J Med. 1985;313:1105–1110.
84. MacMahon S, Collins R, Peto R, et al. Effects of prophylactic lidocaine in suspected acute myocardial infarction. An overview of results from the randomized, controlled trials. JAMA. 1988;260:1910–1916.
85. Keeley EC, Grines CL. Primary coronary intervention for acute myocardial infarction. JAMA. 2004;291(6):736–739.
86. Magid DJ, Calonge BN, Rumsfeld JS, et al.; National Registry of Myocardial Infarction 2 and 3 Investigators. Relation between hospital primary angioplasty volume and mortality for patients with acute MI treated with primary angioplasty vs thrombolytic therapy. JAMA. 2000;284(24):3131–3138.
87. Collet JP, Montalescot G, Le May M, et al. Percutaneous coronary intervention after fibrinolysis: a multiple meta-analyses approach according to the type of strategy. J Am Coll Cardiol. 2006;48(7):1326–1335.
88. Gersh BJ, Stone GW, White HD, et al. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the shape of the future? JAMA. 2005;293(8):979–986.
89. Borden WB, Faxon DP. Facilitated percutaneous coronary intervention. J Am Coll Cardiol. 2006;48(6):1120–1128.
90. Assessment of the Safety and Efficacy of a New Treatment Strategy with Percutaneous Coronary Intervention (ASSENT-4 PCI) investigators. Primary versus tenecteplase-facilitated percutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction (ASSENT-4 PCI): randomised trial. Lancet. 2006;367(9510):569–578.
91. Kastrati A, Mehilli J, Schlotterbeck K, et al.; Bavarian Reperfusion Alternatives Evaluation (BRAVE) Study Investigators. Early administration of reteplase plus abciximab vs abciximab alone in patients with acute myocardial infarction referred for percutaneous coronary intervention: a randomized controlled trial. JAMA. 2004;291(8):947–954.
91a. Di Mario C, Dudek D, Piscione F, et al. for the CARESS-in-AMI (Combined Abciximab RE-teplase Stent Study in Acute Myocardial Infarction) investigators. Lancet. 2008;371:559–568.
92. Gershlick AH, Stephens-Lloyd A, Hughes S, et al.; REACT Trial Investigators. Rescue angioplasty after failed thrombolytic therapy for acute myocardial infarction. N Engl J Med. 2005;353(26):2758–2768.
93. Ting HH, Yang EH, Rihal CS. Reperfusion strategies for ST-segment elevation myocardial infarction. Ann Intern Med. 2006;145(8):610–617.
94. Andersen HR, Nielsen TT, Rasmussen K, et al.; DANAMI-2 Investigators. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003;349(8):733–742.
95. Zijlstra F, van't Hof AW, Liem AL, et al. Transferring patients for primary angioplasty: a retrospective analysis of 104 selected high risk patients with acute myocardial infarction. Heart. 1997;78:333–336.
96. Widimsky P, Groch L, Zelízko M, et al. Multicentre randomized trial comparing transport to primary angioplasty vs immediate thrombolysis vs combined strategy for patients with acute myocardial infarction presenting to a community hospital without a catheterization laboratory. The PRAGUE study. Eur Heart J. 2000;21:823–831.
97. Widimsky P, Budesinsky T, Vorac D, et al. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial—PRAGUE-2. Eur Heart J. 2003;24:94–104.
98. Vermeer F, Oude Ophuis AJ, vd Berg EJ, et al. Prospective randomised comparison between thrombolysis, rescue PTCA, and primary PTCA in patients with extensive myocardial infarction admitted to a hospital without PTCA facilities: a safety and feasibility study. Heart. 1999;82:426–431.
99. Grines CL, Westerhausen DR Jr, Grines LL, et al. A randomized trial of transfer for primary angioplasty versus on-site thrombolysis in patients with high-risk myocardial infarction: the Air Primary Angioplasty in Myocardial Infarction study. J Am Coll Cardiol. 2002;39:1713–1719.
100. Dalby M, Bouzamondo A, Lechat P, et al. Transfer for primary angioplasty versus immediate thrombolysis in acute myocardial infarction: a meta-analysis. Circulation. 2003;108:1809–1814.
101. Keeley EC, Grines CL. Primary percutaneous coronary intervention for every patient with ST-segment elevation myocardial infarction: what stands in the way? Ann Intern Med. 2004;141:298–304.
102. Goldberg RJ, Mooradd M, Gurwitz JH, et al. Impact of time to treatment with tissue plasminogen activator on morbidity and mortality following acute myocardial infarction (the Second National Registry of Myocardial Infarction). Am J Cardiol. 1998;82:259–264.
103. Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283:2941–2947.
104. Berger AK, Radford MJ, Krumholz HM. Factors associated with delay in reperfusion therapy in elderly patients with acute myocardial infarction: analysis of the Cooperative Cardiovascular Project. Am Heart J. 2000;139:985–992.
105. Berger PB, Ellis SG, Holmes DR Jr, et al. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction: results from the Global Use of Strategies to Open Occluded Arteries in Acute Coronary Syndromes (GUSTO-IIb) trial. Circulation. 1999;100:14–20.
106. De Luca G, Suryapranata H, Ottervanger JP, et al. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation. 2004;109:1223–1225.
107. De Luca G, Suryapranata H, Zijlstra F, et al. Symptom-onset-to-balloon time and mortality in patients with acute myocardial infarction treated by primary angioplasty. J Am Coll Cardiol. 2003;42:991–997.
108. Schomig A, Ndrepepa G, Kastrati A. Late myocardial salvage: time to recognize its reality in the reperfusion therapy of acute myocardial infarction. Eur Heart J. 2006;27:1900–1907.
109. Steg PG, Laperche T, Golmard JL, et al. Efficacy of streptokinase, but not tissue-type plasminogen activator, in achieving 90-minute patency after thrombolysis for acute myocardial infarction decreases with time to treatment. PERM Study Group. Prospective Evaluation of Reperfusion Markers. J Am Coll Cardiol. 1998;31:776–779.
110. Zeymer U, Tebbe U, Essen R, et al. Influence of time to treatment on early infarct-related artery patency after different thrombolytic regimens. ALKK-Study Group. Am Heart J. 1999;137:34–38.
111. Newby LK, Rutsch WR, Califf RM, et al. Time from symptom onset to treatment and outcomes after thrombolytic therapy. GUSTO-1 Investigators. J Am Coll Cardiol. 1996;27:1646–1655.
112. Brodie BR, Stuckey TD, Wall TC, et al. Importance of time to reperfusion for 30-day and late survival and recovery of left ventricular function after primary angioplasty for acute myocardial infarction. J Am Coll Cardiol. 1998;32:1312–1319.
113. Antoniucci D, Valenti R, Migliorini A, et al. Relation of time to treatment and mortality in patients with acute myocardial infarction undergoing primary coronary angioplasty. Am J Cardiol. 2002;89:1248–1252.
114. Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283:2941–2947.
115. Nallamothu BK, Bates ER. Percutaneous coronary intervention versus fibrinolytic therapy in acute myocardial infarction: is timing (almost) everything? Am J Cardiol. 2003;92:824–826.
116. Kahn JK, O'Keefe HJ Jr, Rutherford BD, et al. Timing and mechanism of in-hospital and late death after primary coronary angioplasty during acute myocardial infarction. Am J Cardiol. 1990;66:1045–1048.
117. Gibson CM, Karha J, Murphy SA, et al. Early and long-term clinical outcomes associated with reinfarction following fibrinolytic administration in the Thrombolysis in Myocardial Infarction trials. J Am Coll Cardiol. 2003;42:7–16.
118. Schomig A, Ndrepepa G, Mehilli J, et al. Therapy-dependent influence of time-to-treatment interval on myocardial salvage in patients with acute myocardial infarction treated with coronary artery stenting or thrombolysis. Circulation. 2003;108:1084–1088.
119. Gheorghiade M, Zannad F, Sopko G, et al., for the International Working Group on Acute Heart Failure Syndromes. Acute heart failure syndromes: current state and framework for future research. Circulation. 2005;112:3958–3968.
120. Gheorghiade M, Sopko G, De Luca L, et al. Navigating the crossroads of coronary artery disease and heart failure Circulation. 2006;114:1202–1213.
121. Steg PG, Dabbous OH, Feldman LJ, et al.; Global Registry of Acute Coronary Events Investigators. Determinants and prognostic impact of heart failure complicating acute coronary syndromes: observations from the Global Registry of Acute Coronary Events (GRACE). Circulation. 2004;109:494–499.
122. Trost JC, Hillis LD. Intra-aortic balloon counterpulsation. Am J Cardiol. 2006;97(9):1391–1398.
123. Becker RC, Gore JM, Lambrew C, et al. A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction. J Am Coll Cardiol. 1996;27:1321–1326.
124. Hochman JS, Sleeper LA, Webb JG, et al.; SHOCK Investigators. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med. 1999;341:625–634.
125. Hochman JS, Sleeper LA, White HD, et al.; SHOCK Investigators. One-year survival following early revascularization for cardiogenic shock. JAMA. 2001;285:190–192.
126. Babaev A, Frederick PD, Pasta DJ, et al.; NRMI Investigators. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2005;294(4):448–454.
127. Rogers WJ, Bowlby LJ, Chandra NC, et al.; for the participants in the National Registry of Myocardial Infarction. Treatment of myocardial infarction in the United States (1990 to 1993). Circulation. 1994;90:2103–2114.
128. Bursi F, Enriquez-Sarano M, Nkomo VT, et al. Heart failure and death after myocardial infarction in the community: the emerging role of mitral regurgitation. Circulation. 2005;111:295–301.
129. Salukhe TV, Henein MY, Sutton R. Ischemic mitral regurgitation and its related risk after myocardial infarction. Circulation. 2005;111:254–256.
130. Hochman JS, Lamas GA, Buller CE, et al. Coronary intervention for persistent occlusion after myocardial infarction. N Engl J Med. 2006;355:2395–2407.
131. Dzavik V, Buller CE, Lamas GA, et al.; TOSCA-2 Investigators. Randomized trial of percutaneous coronary intervention for subacute infarct-related coronary artery occlusion to achieve long-term patency and improve ventricular function: the Total Occlusion Study of Canada (TOSCA)-2 trial. Circulation. 2006;114(23):2449–2457.
132. Zehender M, Kasper W, Kauder E, et al. Right ventricular infarction as an independent predictor of prognosis after acute inferior myocardial infarction. N Engl J Med. 1993;328:981–988.
133. Berger PB, Ryan TJ. Inferior myocardial infarction: high-risk subgroups. Circulation. 1990;81:401–411.
134. Jacobs AK, Leopold JA, Bates E, et al. Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry. J Am Coll Cardiol. 2003;41:1273–1279.
135. Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med. 1994;330:1211–1217.
136. Dell'Italia LJ, Starling MR, Blumhardt R, et al. Comparative effects of volume loading, dobutamine, and nitroprusside in patients with predominant right ventricular infarction. Circulation. 1985;72:1327–1335.
137. Love JC, Haffajee CI, Gore JM, et al. Reversibility of hypotension and shock by atrial or atrioventricular sequential pacing in patients with right ventricular infarction. Am Heart J. 1984;108:5–13.
138. Cotter G, Berger PB. Cardiogenic shock–beyond the large infarction. Crit Care Med. 2006;34(8):2234–2235.
139. Bromet DS, Klein LW. Cardiogenic shock: art and science. Crit Care Med. 2004;32(1):293–294.
140. Puri VK. Cardiogenic shock: what has changed? Chest. 2003;124(5):1634–1636.