The middle mediastinum (a term not frequently used) contains the pericardium and heart, the adjoining parts of the great vessels, the lung roots, the phrenic nerves, and the deep part of the cardiac plexus.
Pericardium
Fibrous pericardium
Unlike the pleura and peritoneum, the pericardium has an outer single-layered fibrous sac that encloses the heart and the roots of the great vessels, fusing with the adventitia of these vessels. Its broad base overlies the central tendon of the diaphragm, with which it is inseparably blended, both being derived from the septum transversum (see p. 187). The phrenic nerves lie on the surface of the fibrous pericardium and the mediastinal pleura is adherent to it, wherever the two membranes are in contact with each other. The fibrous pericardium is connected to the back of the sternum by weak sternopericardial ligaments. It is supplied with blood by the internal thoracic arteries.
Serous pericardium
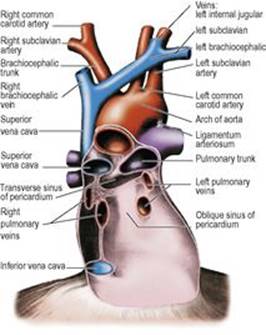
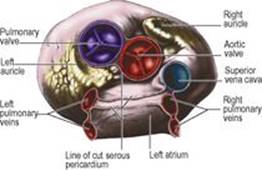
A serous layer lines the inside of the fibrous pericardium, whence it is reflected around the roots of the great vessels to cover the entire surface of the heart, where it forms the epicardium. Between these parietal and visceral layers there are two sinuses: the transverse sinus and the oblique sinus of the pericardium. The transverse sinus is a passage above the heart, between the ascending aorta and pulmonary trunk in front and the superior vena cava, left atrium and pulmonary veins behind. The oblique sinus is a space behind the heart, between the left atrium in front and the fibrous pericardium behind, posterior to which lies the oesophagus. A hand passed from below easily enters the oblique sinus, but the fingertips can only pass up as far as a double fold of serous pericardium that separates the oblique and transverse sinuses from each other (Fig. 4.16). It is through the transverse sinus that a temporary ligature is passed to occlude pulmonary trunk and aorta during pulmonary embolectomy and cardiac operations.
|
|
|
Fig 4.16 Posterior wall of serous pericardial sac: viewed from in front after removal of the heart. |
Nerve supply
The fibrous pericardium is supplied by the phrenic nerve. The parietal layer of serous pericardium that lines it is similarly innervated, but the visceral layer on the heart surface is insensitive. Pain from the heart (angina) originates in the muscle or the vessels and is transmitted by sympathetic nerves (see p. 194). The pain of pericarditis originates in the parietal layer only, and is transmitted by the phrenic nerve.
Blood supply
Pericardial blood supply is derived from the internal thoracic artery, its pericardiophrenic and musculophrenic branches, bronchial arteries and the thoracic aorta. The veins drain into the azygos system.
Pericardial drainage
A needle inserted in the angle between the xiphoid process and the left seventh costal cartilage and directed upwards at an angle of 45°, towards the left shoulder, passes through the central tendon of the diaphragm into the pericardial cavity. The creation of a small pericardial window surgically through the same route, or through the anterior end of the fourth intercostal space, provides more effective drainage.
Heart
The heart is the muscular pump responsible for blood circulation. It is an organ with four chambers: right and left atria, and right and left ventricles. The two atria receive blood, the left from the lungs and the right from the rest of the body. The right ventricle propels blood to the lungs and the left ventricle propels blood around the rest of the body (the systemic circulation).
Position
As the heart lies obliquely in the thorax, with its long axis passing downwards and to the left to the apex, and as the heart has undergone a degree of rotation during development, the chambers are not located strictly in the positions that their names suggest. The right-sided chambers are mainly anterior to their left-sided counterparts and the atria are mainly to the right of their respective ventricles (Figs 4.17 and 4.18). The interatrial and interventricular septa thus lie at about 45° to the sagittal plane, while the plane of the atrioventricular valve orifices lies almost vertically at about 90° to the septal plane. As seen from the front, the heart is described as having right, inferior (acute) and left (obtuse) borders, an anterior or sternocostal surface, an inferior or diaphragmatic surface, a base or posterior surface, and an apex at its left inferior corner.
|
|
|
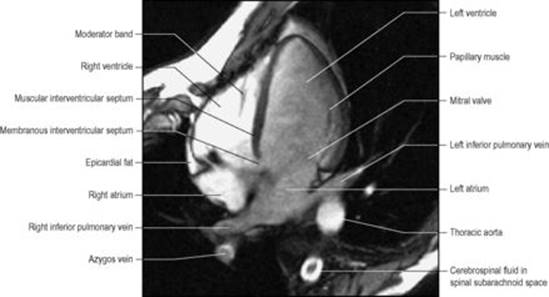
Figure 4.17 Oblique axial magnetic resonance image (MRI) showing a four-chamber view of the heart, viewed from below. (Provided by Dr R.A. Coulden, Papworth Hospital, Cambridge.) |
|
|
|
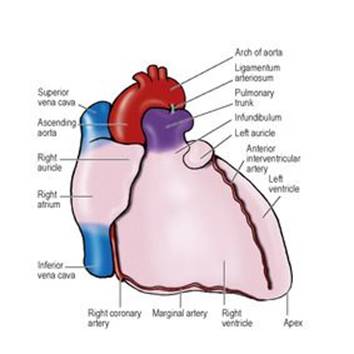
Figure 4.18 Anterior (sternocostal) surface of the heart. The left auricle is shown somewhat enlarged. |
The right border consists entirely of the right atrium (Fig. 4.18). The inferior border is made up mostly of right ventricle with a small portion of left ventricle, which forms the apex, at the junction of the inferior and left borders. The left border is mostly left ventricle, with the auricle of the left atrium forming the uppermost part of this border. The anterior or sternocostal surface consists mainly of the right ventricle, with the right atrium on its right side and a narrow strip of the left ventricle on the left border. The tip of the left auricular appendage peeps over the top of this border. The inferior or diaphragmatic surface is made up of one-third right ventricle and two-thirds left ventricle, separated by the posterior interventricular branch of the right coronary artery. The posterior surface (or base) of the heart (Fig. 4.19) consists almost entirely of the left atrium, receiving the four pulmonary veins. From it the left ventricle converges to the left towards the apex. A narrow strip of right atrium forms the horizon on the right.
|
|
|
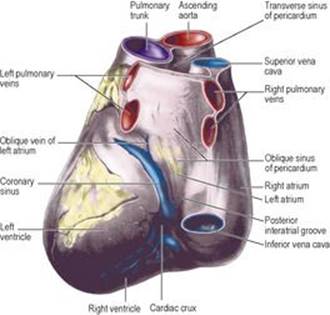
Figure 4.19 Posterior and inferior (diaphragmatic) surfaces of the heart. The cardiac crux is the junction of the posterior interatrial, atrioventricular and interventricular grooves. |
Surface markings
About one-third of the heart lies to the right of the midline. The right border of the heart extends from the lower border of the right third costal cartilage to the lower border of the right sixth costal cartilage, just beyond the right margin of the sternum and describing a slight convex curve between these points. The inferior border passes from the right sixth costal cartilage to the apex, which is normally in the left fifth intercostal space in the midclavicular line. From the apex the left border extends upwards to the lower border of the left second costal cartilage about 2cm from the sternal margin. These are the borders as seen in a typical radiograph of the normal heart, although the area of cardiac dullness as determined by percussion will be smaller.
Fibrous skeleton
The two atria and the two ventricles are attached to a pair of conjoined fibrous rings which, in the form of a figure 8, bound the atrioventricular orifices. The muscle of the heart is attached to this fibrous skeleton and the muscle fibres encircle the chambers of the heart in a series of whorls and spirals. The atria lie to the right and the ventricles to the left of the fibrous skeleton and there is no muscular continuity between the two. The atrioventricular conducting bundle is the only physiological connection between atria and ventricles across the fibrous ring. The membranous part of the interventricular septum is attached to the fibrous skeleton, and so are the bases of the cusps of the tricuspid, mitral and aortic valves; the region where they meet is termed the central fibrous body.
Right atrium
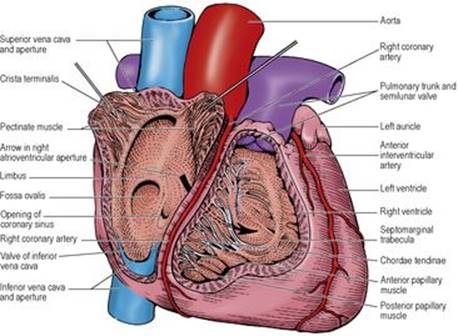
This elongated chamber lies between the superior and inferior venae cavae, and forms the right border of the heart (Fig. 4.18). Its lower end is almost completely occupied by the orifice for the inferior vena cava. Above this the medial part of the right atrium is prolonged to the left of the superior vena cava as the right auricle. This large, triangular appendage overlies the commencement of the aorta and the upper part of the right atrioventricular groove and, with the left auricle, it clasps the infundibulum of the right ventricle. The left atrium lies behind the right atrium. From the angle between the superior vena cava and the right auricle a shallow groove sometimes descends; this is the sulcus terminalis. It is produced, when present, by the projection into the cavity of the right atrium of a vertical ridge of heart muscle, the crista terminalis. The interior of the right atrium is smooth to the right of the crista terminalis, but between the crista and the blind extremity of the auricle the myocardium is projected into a series of horizontal ridges like the teeth of a comb: the pectinate muscles (Fig. 4.20). This rough area represents the true auricular chamber of the embryonic heart. The smooth-walled remainder of the atrial cavity is produced by incorporation of the right horn of the sinus venosus (see p. 30).
|
|
|
Figure 4.20 Interior of right atrium and right ventricle. |
The opening of the inferior vena cava is partly bounded by a small, crescentic ridge, the remains of the valve of the inferior vena cava, that is continued upwards towards the opening of the coronary sinus. This opening lies above the septal cusp of the tricuspid valve, and to the left of the inferior vena caval orifice.
The interatrial septum forms the posterior wall of the right atrium above the opening of the coronary sinus. Towards its lower part is a shallow saucer-shaped depression, the fossa ovalis. This is the primary septum of the fetal heart. The crescentic upper margin of the fossa ovalis is called the limbus, and indicates the lower edge of the secondary septum. Failure of fusion of the two septa gives rise to a persistent foramen ovale (see p. 206). In the fetal circulation the valve of the inferior vena cava directed caval blood towards the foramen ovale (see p. 206).
Right ventricle
This chamber projects to the left of the right atrium (Figs 4.18 and 4.20). The atrioventricular groove between the two is almost vertical over the front of the heart and anteroposterior on the diaphragmatic surface. It lodges the right coronary artery and is usually filled with fat. The right ventricle narrows as it passes upwards towards the commencement of the pulmonary trunk.
The walls are thrown into a series of muscular ridges, the trabeculae carneae, which project into the cavity of the ventricle. One of these ridges has broken free and lies in the cavity attached by its two ends to the interventricular septum and the anterior papillary muscle. This is the septomarginal trabecula (also called the moderator band); it contains part of the right branch of the conducting bundle. Other projections into the lumen from the ventricular walls form the papillary muscles.
The tricuspid valve guards the right atrioventricular orifice. It has three cusps and admits the tips of three fingers. The three cusps, called anterior, posterior and septal, are attached by their bases to the fibrous atrioventricular ring and in the open position lie against the sternocostal, diaphragmatic and septal walls of the ventricle. The cusps of both the tricuspid and mitral valves often appear to be subdivided but without forming complete additional leaflets. The edges and ventricular surfaces of the cusps receive the attachments of the chordae tendineae, collagenous cords which diverge from the papillary muscles and prevent the cusps from being everted when the ventricle contracts. The main papillary muscles are anterior, inferior (posterior) and septal in location and each is connected to more than one cusp.
The cavity of the ventricle continues upwards into a narrowing funnel-shaped approach to the pulmonary orifice. The walls of this part, the infundibulum or conus, are thin and smooth.
The three semilunar cusps of the pulmonary valve are attached at the junction of the infundibulum and the commencement of the pulmonary trunk. In the adult heart there are two anterior (right and left) and one posterior cusp (Fig. 4.21). The official anatomical nomenclature (Terminologia Anatomica, 1998) refers to them as anterior, posterior and septal cusps in accordance with their position in the fetus. The pulmonary orifice lies almost in the horizontal plane and is at a higher level than the aortic orifice.
|
|
|
Figure 4.21 Superior aspect of the heart; the aorta and pulmonary trunk have been removed, exposing their valves. |
Left atrium
The left atrium forms the posterior surface (base) of the heart, and lies behind the right atrium (Fig. 4.19). The inferior margin of the left atrium lies a little above that of the right atrium, whose posterior wall here receives the coronary sinus; this runs to the right between the left atrium and the left ventricle. From the left atrium the left ventricle slopes away to the apex. A small, bent left auricle projects from its upper border and curves round to the front on the left side of the infundibulum (Fig. 4.18). The four pulmonary veins enter the left atrium symmetrically, one above the other on each side.
The cavity of the left atrium is smooth-walled except in the auricle; here muscular ridges indicate that the appendage was the original auricular chamber of the embryonic heart. All the smooth-walled portion is derived by incorporation of the embryonic pulmonary veins into the atrial cavity.
The bicuspid mitral valve admits the tips of two fingers. The cusps are named anterior and posterior. The base of the anterior cusp is attached to one-third, and that of the posterior cusp to two-thirds of the margin of the fibrous atrioventricular ring; but sometimes they fail to meet and a small accessory cusp fills the gap between them. The anterior cusp of the mitral valve is thicker and more rigid than the posterior cusp. The anterior cusp lies between the mitral and aortic orifices and thus lies between the inflow and outflow tracts of the left ventricle (Fig. 4.22).
|
|
|
Figure 4.22 Interior of the left ventricle, in a sagittal section viewed from the left, to show the cusps of the mitral valve. The arrow indicates the path of blood, entering from the left atrium behind the anterior cusp and leaving the ventricle in front of the anterior cusp to pass through the aortic valve. |
Left ventricle
The walls of this cavity are three times as thick as those of the right ventricle. The trabeculae carneae are well developed. There are two papillary muscles, anterior and posterior, the anterior being the larger. Both are connected by chordae tendineae to each valve cusp (Fig. 4.22). The posterior cusp receives the chordae on both its margin and its ventricular surface, but since blood is squirted across both surfaces of the anterior cusp the chordae are attached to it only along its margins.
The interventricular septum bulges forwards into the cavity of the right ventricle, so that in cross-section the lumen of the left ventricle is circular and that of the right crescentic. The upper and right end of the septal wall is smooth, thinner and more fibrous; this is the membranous part of the septum. As the left ventricle is larger than the right ventricle and the right atrium is larger than the left atrium, the membranous part of the septum lies between the left ventricle and the right atrium. Between the membranous part and the anterior cusp of the mitral valve is the aortic vestibule, which leads up to the aortic orifice.
The aortic orifice is guarded by the aortic valve, at the entrance to the ascending aorta. It lies at a lower level than the pulmonary orifice, to its right side (Fig. 4.21), and is more obliquely placed. It has three semilunar cusps. In the adult heart these cusps are in anterior, left posterior and right posterior positions. In the Terminologia Anatomica (1998) the corresponding cusps are named right, left and posterior in keeping with their fetal positions. Cardiac surgeons refer to the same cusps as right coronary, left coronary and non-coronary in accordance with the origins of the coronary arteries. Fibrous continuity between the left coronary and non-coronary aortic cusps and the anterior mitral cusp is termed the subaortic curtain.
Structure of heart valves
The cusps of the tricuspid and mitral valves are flat and their free edges are serrated. On closure of the valves during ventricular systole the cusps do not meet edge to edge, but come into mutual contact on their auricular surfaces near the serrated margins. This contact and the pull of the marginal chordae prevent eversion of the free edges into the cavity of the atrium, while the centrally attached chordae limit the amount of ballooning of the cusps towards the atrium. The tricuspid and mitral valves are kept competent by active contraction of the papillary muscles, which pull on the chordae during ventricular systole.
The cusps of the pulmonary and aortic valves are cup shaped. The free edge of each cusp contains a central fibrous nodule from each side of which straight edges slope at 120° from each other to the attached base of the cusp. Three cusps lying edge to edge thus close the circular orifice (Fig. 4.21). During ventricular systole the bulge of the aortic sinuses (see below) above the cusps prevents the cusps from becoming flattened against the walls of the sinuses; the residual blood in the sinuses forms vortices which help the elastic recoil of the cusps at the end of systole. During ventricular diastole pressure of blood above the valves distends the cusps, so that their free edges are forced together. Competence of the pulmonary and aortic valves is thus a passive phenomenon, the result of mutual pressure between the distended cusps, and is dependent on the integrity of their straight edges.
Microscopically the valves of the heart are composed of a core of collagenous fibrous tissue covered on each surface by vascular endothelium (endocardium).
Surface markings of valves
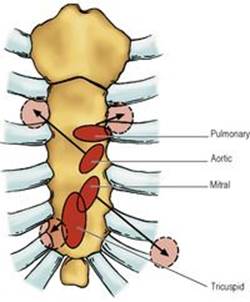
All the valves of the heart lie behind the sternum, making a line with each other that is nearly vertical (Fig. 4.23). The bases of tricuspid and mitral valves, attached to the atrioventicular ring, are indicated by vertical lines over the lower part of the sternum. The tricuspid valve lies behind the midline of the lower sternum, the mitral valve, overlapping it, lies higher and somewhat to the left opposite the fourth left intercostal space and costal cartilage. The aortic and pulmonary orifices lie behind the left border of the sternum at the level of the third intercostal space and the third costal cartilage, respectively.
|
|
|
Figure 4.23 Surface markings of the heart valves. The arrows indicate the directions in which the sounds of the closing valves are propagated, and the circles indicate the generally preferred sites for auscultation. Mitral valve sounds are best heard over the apex of the heart at the fifth left intercostal space in the midclavicular line. |
The normal heart sounds are produced by closure of heart valves, and the opening snap of the mitral valve may also be audible. They are heard best (Fig. 4.23) where the corresponding chambers or channels lie nearest to the chest wall. For the tricuspid valve this is over its surface, but for the mitral valve it is at the apex beat. For the aortic valve it is where the ascending aorta lies nearest the surface, at the right sternal margin in the second intercostal space, and for the pulmonary valve at the left sternal margin at the same level, over the pulmonary trunk.
Great vessels
In their course through the pericardial cavity the great vessels are invested with a reflexion of serous pericardium. The ascending aorta and pulmonary trunk share a common sleeve of serous pericardium in which they lie in front of the transverse sinus (Fig. 4.19). The whole of the ascending aorta and the entire pulmonary trunk, each about 5cm in length, are inside the fibrous pericardium.
The six veins share another common sleeve of serous pericardium (Fig. 4.19). The four pulmonary veins and the inferior vena cava are all 1cm or less in length within the pericardium, but the superior vena cava courses for about three times that distance through the pericardial cavity before entering the right atrium.
Ascending aorta
Immediately above the aortic orifice the wall of the ascending aorta bulges to form the aortic sinuses (of Valsalva), one above each cusp and similarly named. From the sinus that lies anteriorly in the adult heart the right coronary artery emerges, and from the left posterior sinus, the left coronary artery. Above the sinuses the aorta runs to the right behind the infundibulum of the right ventricle (Fig. 4.18) and as it passes upwards it slants a little forward towards the manubrium, before curving backwards at the commencement of the arch. Here the fibrous pericardium is blended with its wall.
Pulmonary trunk
Commencing at the summit of the infundibulum at a slightly higher level than the aortic orifice (Fig. 4.23), the wide pulmonary trunk arches backwards initially in front of and then to the left of the ascending aorta. The two vessels make a gentle spiral enclosed in the common sleeve of serous pericardium in front of the transverse sinus. The fibrous pericardium blends with the wall of the pulmonary trunk as it divides—to the left of the midline (Fig. 4.29), under the concavity of the aortic arch and in front of the left main bronchus—into the right and left pulmonary arteries.
Catheterization. Various aspects of cardiorespiratory function can be monitored by pulmonary artery catheterization. The catheters are introduced into the right atrium, usually via the internal jugular or subclavian veins (see pp. 344and 348) and carried on through the tricuspid valve into the right ventricle and pulmonary trunk, and then into the right pulmonary artery, under radiological vision.
Conducting (conduction) system
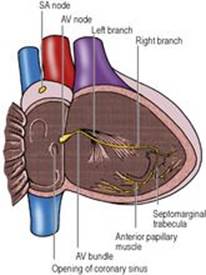
The conducting system of the heart consists of the sinuatrial node (SA node), the atrioventricular node (AV node), the atrioventricular bundle (of His), the right and left limbs or branches of the bundle, and the subendocardial Purkinje fibres. From the SA node, which, like the AV node and its extensions, is composed of a specialized type of cardiac muscle fibres (not nervous tissue), impulses are conducted to the AV node by atrial cardiac muscle fibres. The AV node, bundle, branches and subendocardial fibres form one continuous mass of conduction tissue.
The sinuatrial node, or pacemaker of the heart, is a small mass of histologically distinctive myocardial cells. It is subepicardially situated in the wall of the right atrium, just below the superior vena cava, at the top of the sulcus terminalis. It has no macroscopic or palpable features that indicate its location. The atrioventricular node is also a small mass of specialized myocardial cells. It is subendocardially situated in the right atrium on the interatrial septum, above the attachment of the septal cusp of the tricuspid valve, to the left of the opening of the coronary sinus (Fig. 4.24).
|
|
|
Figure 4.24 Conducting system of the heart, from the front after removal of parts of the right atrium and the ventricles. This diagrammatic representation illustrates that the left and right branches of the AV bundle, which pass down their respective sides of the interventricular septum, are very different. The left branch rapidly breaks up into a sheaf of subendocardial fibres, but the right continues towards the septomarginal trabecula; part of the branch enters it to reach the anterior papillary muscle. Only the more proximal parts of the subendocardial fibres are shown. |
From the AV node, the AV bundle runs along the inferior border of the membranous part of the interventricular septum, where it divides into right and left branches. Since the fibrous framework of the heart separates the muscles of the atria from those of the ventricles, the bundle is the only means of conducting the contractile impulse from atria to ventricles. The right branch runs at first within the muscle of the septum and then becomes subendocardial on the right side of the septum. Much of it continues into the septomarginal trabecula (moderator band) to reach the anterior papillary muscle and the anterior wall of the ventricle, and its Purkinje fibres then spread out beneath the endocardium. The left branch reaches the septal endocardium of the left ventricle and rapidly breaks up into a sheaf of branches which spread out subendocardially over the septum and the rest of the ventricular wall.
Blood supply of the heart
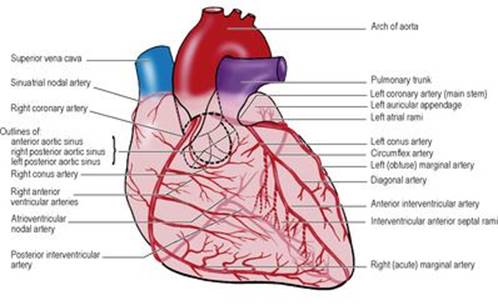
The heart is supplied by the two coronary arteries and their branches (Fig. 4.25). Variations occur occasionally in their origins and patterns of distribution; the account that follows describes the usual arrangement. The right and left coronary arteries arise from aortic sinuses at the beginning of the ascending aorta. Each coronary artery is the main source of supply to its same side atrium and ventricle, but also supplies the opposite side chambers to some extent. The veins that drain the myocardium do not have names that correspond to the arteries; in this respect the heart resembles the brain.
|
|
|
Figure 4.25 Coronary arteries and their main branches. The ascending aorta and pulmonary trunk are depicted in the same pink colour as the heart to enable the visualization of the origins and early branches of the coronary arteries. The right conus artery is seen arising directly from the anterior aortic sinus as it may do in one third of individuals. |
Right coronary artery. Arising from the anterior aortic sinus the artery passes between the right auricle and the infundibulum of the right ventricle (Fig. 4.20). Running downwards in the atrioventricular groove the artery turns backwards at the inferior border of the heart and runs posteriorly. It gives off branches to both atrium and ventricle. One of the highest branches is the conus artery which passes upwards and medially on the front of the conus (infundibulum) of the right ventricle. It frequently anastomoses with a similar branch from the left coronary artery to form an anastomosis around the origin of the pulmonary trunk. Another high atrial branch is usually the SA nodal artery which passes back between right auricle and the aorta and forms a vascular ring around the termination of the superior vena cava. It supplies the SA node in about 60% of hearts. At the sharp (acute) inferior border the right marginal artery passes to the left along the right ventricle, although it often has a much higher origin and passes obliquely down over the front of the ventricle. On the diaphragmatic surface of the heart the posterior interventricularbranch—also called the posterior descending artery—is given off. This large vessel passes along the interventricular groove towards the apex of the heart. The right coronary artery has a characteristic loop where the posterior interventricular artery is given off and the AV nodal artery arises here. Having given off one or more left ventricular (right posterolateral) branches, the remaining and much smaller right coronary artery anastomoses with the termination of the circumflex branch of the left coronary artery to a varying extent.
Left coronary artery. Arising from the left posterior aortic sinus the artery runs to the left behind the pulmonary trunk and emerges between the left auricle and the infundibulum of the right ventricle. After this short course it divides into its two terminal (circumflex and anterior interventricular) branches (Fig. 4.25). The circumflex branch continues round the left margin to the back of the heart in the atrioventricular groove, giving off various ventricular and atrial branches and anastomosing variably with the end of the right coronary. One large left marginal artery frequently runs down the rounded (obtuse) left border of the heart. In about 40% of hearts the circumflex artery gives off the SA nodal artery which passes to the right behind the ascending aorta. The anterior interventricular artery, also called the left anterior descending artery, is the cardiac vessel most often affected by disease. It runs down in the interventricular groove to anastomose under the apex with the posterior interventricular branch of the right coronary. Near its origin it gives a conus branch and further towards the left several ventricular branches. One is often large; this diagonal artery may arise separately from the left coronary trunk, which then ends by trifurcation.
In about 10% of hearts the right coronary is shorter than usual and the posterior interventricular artery is replaced by a continuation of the circumflex artery, which also supplies the AV node; in this case the heart is said to show ‘left dominance’. In the more common ‘right dominance’ the posterior interventricular comes from the right coronary; the artery giving off the posterior interventricular branch is defined as the dominant artery. In a ‘balanced’ circulation, branches of both arteries run in or near the posterior interventricular groove.
Anastomoses of the coronary arteries. Anastomoses exist at the arteriolar level between the terminations of the right and left coronary arteries in the atrioventricular groove and between their interventricular and conus branches. The time factor in occlusion is all important; in slow occlusion there is time for healthy arterioles to open up, in abrupt occlusion there is not. Potential anastomoses exist between the coronary arteries and pericardial arteries around the roots of the great vessels.
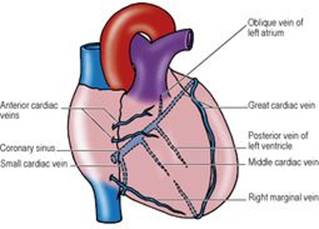
Veins of the heart. The veins of the heart (Fig. 4.26) are the coronary sinus with its five normal tributaries (the great, middle and small cardiac veins, the posterior vein of the left ventricle and the oblique vein of the left atrium), the anterior cardiac veins and the venae cordis minimae. The coronary sinus receives most of the heart's blood.
|
|
|
Figure 4.26 Cardiac veins, seen from the front. The vessels not on the anterior surface are shown in interrupted line. The middle cardiac vein usually opens into the coronary sinus nearer its termination. |
The coronary sinus is a wide vessel that lies in the posterior part of the atrioventricular groove (Fig. 4.19), covered by a thin layer of myocardium, and opens at its right end into the posterior wall of the right atrium to the left of the inferior vena caval opening (Fig. 4.20). The great cardiac vein accompanies the anterior interventricular and circumflex arteries to enter the left end of the sinus, receiving in its course a number of left ventricular tributaries. The middle cardiac vein accompanies the posterior interventricular artery and opens near the termination of the coronary sinus. The small cardiac vein opens into the coronary sinus near its atrial end. The posterior vein of the left ventricle joins the sinus to the left of the middle cardiac vein, and the small oblique vein of the left atrium runs downwards into the sinus near its left end.
The anterior cardiac veins are a series of parallel veins that run across the surface of the right ventricle to open into the right atrium. The right marginal vein passes to the right along the inferior cardiac margin and joins the small cardiac vein, or drains directly into the right atrium in the manner of an anterior cardiac vein.
The venae cordis minimae are very small veins in the walls of all four chambers of the heart that open directly into the respective chambers. They are most frequent in the right atrium.
Lymph drainage
The lymphatics of the heart drain back along the coronary arteries, emerge from the fibrous pericardium along with the aorta and pulmonary trunk, and empty into the tracheobronchial and brachiocephalic lymph nodes.
Nerve supply
The heart is innervated by the cardiac plexus, which has been described on page 193 together with the pathways for cardiac pain.
Development
The earliest stages of cardiac development have been mentioned on page 30.
The original single atrium becomes partitioned by the formation of two septa. The primary septum (septum primum) grows down towards the endocardial cushions (see below) at the atrioventricular orifice but does not immediately fuse with them; the gap remaining above the cushions is the primary foramen (ostium primum). Before this foramen becomes obliterated by further downgrowth of the septum, a new foramen (secondary foramen, ostium secundum) appears as a result of breakdown of the upper part of the primary septum. The right and left parts of the atrium thus still remain in communication. Now a further septum appears (secondary septum, septum secundum), on the right of the primary septum, overlapping the secondary foramen and the upper part of the primary septum. It does not grow down as far as the cushions but ends at a curved posteroinferior border. The gap under the secondary septum, through which fetal blood from the right side can flow up between the septa and to the left side, is the foramen ovale, allowing fetal blood to flow from the right to the left side. At birth when the lungs begin to function, the pressure in the left atrium increases, forcing the primary septum against the left side of the secondary septum so that they fuse, making a complete interatrial septum. The lower edge of the secondary septum remains as the limbus of the fossa ovalis; the floor of the fossa is the part of the primary septum not overlapped by the secondary septum. Sometimes, although the septa overlap, fusion is incomplete and a small cleft remains; this has no functional significance, but a catheter introduced into the right atrium may be manipulated between the septa into the left atrium-a condition known as probe-patent foramen ovale. The right horn of the sinus venosus becomes incorporated into the wall of the right atrium, forming its smooth part and accounting for the drainage of the superior and inferior venae cavae into this chamber; the auricle with the pectinate muscles represents the original atrium. The rest of the sinus venosus persists as the coronary sinus, with the left horn being represented by the oblique vein of the left atrium (vein of Marshall).
The left atrium incorporates the ends of the pulmonary veins to such an extent that only the auricle represents the original atrium.
The channel between the original atrium and ventricle (atrioventricular canal) becomes constricted by internal dorsal and ventral swellings, the endocardial cushions, and these converge to convert what was a single passage into the two atrioventricular orifices. Subendocardial tissue at these sites produces the mitral and tricuspid valves.
In the floor of the original ventricle, a partition grows upwards to become the muscular part of the interventricular septum. It does not grow as far as the endocardial cushions, but leaves a gap which becomes filled in by the membranous part of the septum. The muscular part of the septum arises from the junction of the ventricle and the bulb (see p. 30), so that the original ventricle becomes the left ventricle and the adjacent part of the bulb becomes the rough (trabecular) part of the right ventricle. The lower part of the bulb forms the smooth (outflow) part of the right ventricle, which continues upwards into the part of the bulb called the truncus arteriosus. This becomes divided into two by internal swellings, the right and left bulbar ridges, which meet to form the aorticopulmonary septum, so that from the single tube both the ascending aorta and pulmonary trunk are formed. The bulbar ridges are not vertical but assume a spiral form, hence the way the aorta and pulmonary trunk curl round one another. It is the fusion of the lower ends of the bulbar ridges with the posterior endocardial cushion which creates the membranous part of the interventricular septum.
The junction of the truncus arterious and the definitive ventricles is the site where the aortic and pulmonary valves develop from the bulbar ridges and the aortic and pulmonary trunk walls.
The SA node develops from sinus venosus tissue but the AV node and bundle are derived from the original atrium.
Congenital defects. Among the more common congenital defects of cardiac development are malformations of the interatrial and interventricular septa, and Fallot's tetralogy. Most atrial septal defects are due to maldevelopment of the primary or secondary septa. Most ventricular septal defects are in the membranous part. Fallot's tetralogy is due to the unequal division of the truncus arteriosus, giving a small pulmonary trunk and a large ascending aorta, and hence the tetrad of (1) pulmonary stenosis, (2) right ventricular hypertrophy, (3) a defect of the membranous part of the interventricular septum, and (4) an over-riding aorta (sitting astride both ventricles because of the septal defect).
Other anomalies, such as patent ductus arteriosus and coarctation of the aorta, although commonly classified as ‘cardiac’ defects, are strictly speaking anomalies of the great vessels, and are considered on page 27.
Surgical approach
Many operations on the heart are carried out through a median sternotomy, although some require a left thoracotomy. In the former, after splitting the sternum and dividing the thymus into its two lobes, the pericardium is incised in the lines of an inverted T, with the vertical incision extending as high as the pericardial reflexion from the aorta and the transverse incisions along the reflexions from the diaphragm. For cardiopulmonary bypass (to keep the circulation going during open heart surgery), the superior and inferior venae cavae are cannulated through the wall of the right atrium, in order to deliver blood to the oxygenating machine. The oxygenated blood is delivered to the aorta through a cannula in the aortic arch proximal to the brachiocephalic trunk. Some of this blood will pass downwards into the ascending aorta and so perfuse the coronary vessels whose openings are just above the aortic valves (kept closed by the pressure of the incoming blood).
In earlier coronary artery bypass operations, a suitable length of great saphenous vein was anastomosed at one end to the ascending aorta and at the other to the appropriate coronary vessel distal to the site of blockage. The vein, of course, must be turned upside down so that any valves in the chosen segment do not obstruct the arterial flow. Current opinion now often favours the use of the internal thoracic artery, particularly for the left anterior descending artery; the proximal end remains intact at its subclavian origin and the cut lower end is anastomosed to the coronary vessel. Three or four coronary arteries may be bypassed in the same patient utilizing both internal thoracic arteries and vein grafts or free arterial segments (such as from the radial artery).
A minimally invasive approach is used for coronary artery bypass grafting in suitable cases. A mini-thoracotomy through the fourth left intercostal space provides access to the anterior interventricular artery.
In percutaneous transluminal coronary angioplasty, following vascular access through the femoral artery in the groin, a catheter is passed retrograde to the site of coronary arterial obstruction and a balloon at the tip of the catheter inflated; patency may be maintained by the placement of a stent.
For the repair of atrial septal defects, the right atrium is incised along its right border, avoiding the region of the SA node. For ventricular septal defects the front of the right ventricle can be incised vertically or transversely avoiding any obvious arteries or veins. For operations on the mitral valve, the left atrium is entered from the right through an incision behind the interatrial groove and in front of the two pulmonary veins.
Transplantation. The patient's heart is removed by incisions through the aorta, pulmonary trunk and both atria. The incision line through the right atrium leaves the two venae cavae, the posterior wall of the atrium and the region of the SA node in situ. The posterior part of the left atrium with the four pulmonary vein orifices is also left intact. The donor heart is trimmed through the atria to match up with the remains of the patient's atria, although the lower end of the donor superior vena cava remains attached to the right atrium so that the donor heart retains its own SA node. For combined heart–lung transplantation, the donor block is removed through the trachea, right atrium and aorta, and sutured to the recipient in that order.