PERSPECTIVE AND PATTERNS OF SPREAD
The study of the patterns of tumor spread and their invasive behavior provides a unique spyglass through which one can view and understand this regional anatomy three dimensionally.
PERSPECTIVE AND PATTERNS OF SPREAD
The head and neck area is a very complex region consisting of a series of mazes and channels that constitute the upper aerodigestive passages. A large variety of tumors arise from the different tissues that constitute the various structures of the head and neck sites. This section focuses on malignancies arising from the surface epithelium, which are the most frequently encountered cancers. They are very destructive if allowed to progress, and because of the resultant functional disabilities, their impact on social presentation, particularly with regard to self-image, speech, and communication, can be extremely detrimental. The challenge is not only to be able to control these cancers, but also to maintain normal anatomic relationships and structure. The TNM staging reflects the patterns of spread and the oncologic anatomy (Fig. 1.1). The common cancers arising in the upper aerodigestive passages are mainly in the pharyngeal and laryngeal tubes (Table 1.1).
Although head and neck cancers are clustered together, they comprise a very diverse group of tumors. If facial and scalp skin cancers and melanomas were included with extracranial head and neck tumors, this would be the most common anatomic site for malignancy. When typically limited to mucosal cancers of the upper aerodigestive tract, it accounts for 3% of all cancers and ranks 6th worldwide—7th for men and 11th for women. The classic patient population presenting with head and neck cancers consists of those with excessive smoking and alcohol habits. Essential to success are programs designed for posttreatment abstinence to avoid a recurrence of malignant tumors.
Cancers in the head and neck region are similar in terms of their biologic behavior; it is the differences in primary site anatomy that define the uniqueness of their clinical manifestations. The conceptualization of three-dimensional anatomy of the head and neck region is therefore appreciated through cancer spread (Fig. 1.1). The cancer crab can spread in six basic directions: superiorly–inferiorly, medially–laterally, and anteriorly–posteriorly (SIMLAP). There are an infinite number of possible patterns around these six basic vectors; however, these are predetermined by the arrangement of muscle and fascial planes. Cancers of the head and neck tend to follow the path of least resistance, invading fatty areolar spaces, which are particularly vulnerable; along nerves through perineural invasion; and entering bony ostia and foramina. Lymphatics and vessels also provide low-pressure flow channels of minimal resistance.
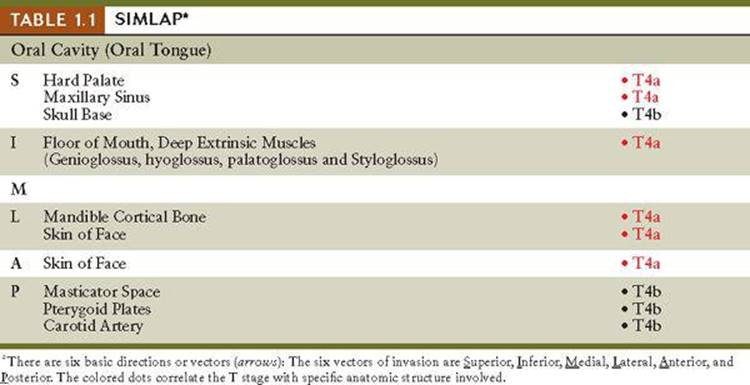
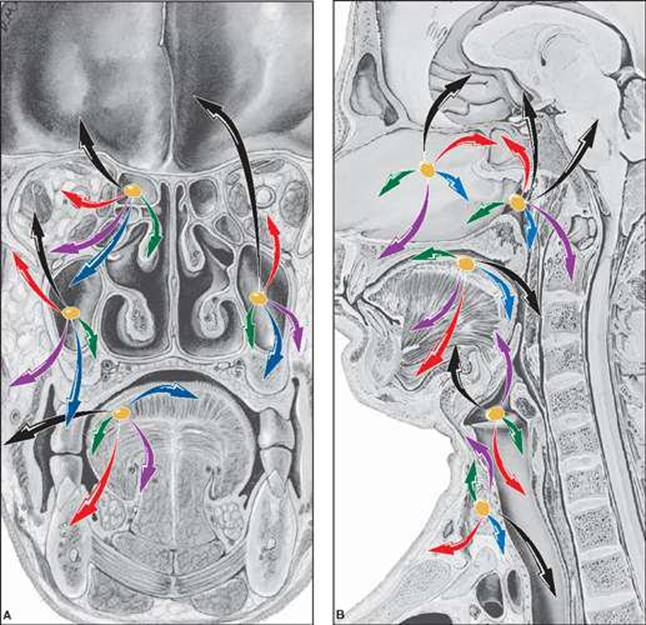
Figure 1.1 | Collage of patterns of spread. The different head and neck primary cancer sites are presented cephalad to caudad. A. Coronal: Ethmoid, maxillary antrum, and oral cavity. B. Sagittal: maxillary antral, nasopharynx, oral cavity, larynx, and thyroid. There are six basic directions or vectors (arrows): anterior–posterior, medial–lateral, superior–inferior. The arrows are color-coded for T stage category: T is yellow, T1 green, T2 blue, T3 purple, T4a red, T4b black. The concept of visualizing patterns of spread to appreciate the surrounding anatomy is well demonstrated by the six directional pattern i.e. SIMLAP Table 1.1.
OVERVIEW OF HISTOGENESIS
The mucosal surfaces of the two major sectors differ (Fig. 1.2; Table 1.2). The respiratory passage is a ciliated columnar or pseudostratified columnar epithelium (Fig. 1.2B–D), and the digestive passage is a stratified squamous epithelium (Fig. 1.2E,F). Both give rise mainly to squamous cell cancers. Most cancers are epithelial in origin, arising from the surface and evolving into four general patterns of invasion; shallow, mucosal, premalignant leukoplakia-like warty lesions often become submucosal (Fig. 1.3A).
• Verrucous growths: Wartlike, spreading on the surface rather than in depth;
• Exophytic and exuberant growth: An polyploid mushroom in appearance that undergoes;
• Fungation, necrosis of growth: This type of tumor usually, but not always, undergoes ulceration; and
• Endophytic invasive growth: Infiltration into muscle or erosion of bone and cartilage, and invasion perineurally of the cranial nerves and their branches.
Adenocarcinomas arise from the endocrine thyroid gland and the exocrine salivary glands (Figs. 1.2C–G and 1.3B).
Because most of the sites consist of different tissue layers (an epithelial surface, underlying muscle, and/or bone with an air-containing cavity), the study of primary tumor sites, where neoplasms commonly arise, requires an appreciation of the surrounding structures. Fat collections in specific pockets in and about the face, pharynx and larynx, and the areolar spaces, which are normally collapsed, are preestablished planes for cancer spread and infection. These spaces allow for mobility and the sliding of muscles during deglutition and speech. The various foramina are particularly vulnerable to spread. Because nerves pass through these openings in their course, perineural infiltration is often a problem.
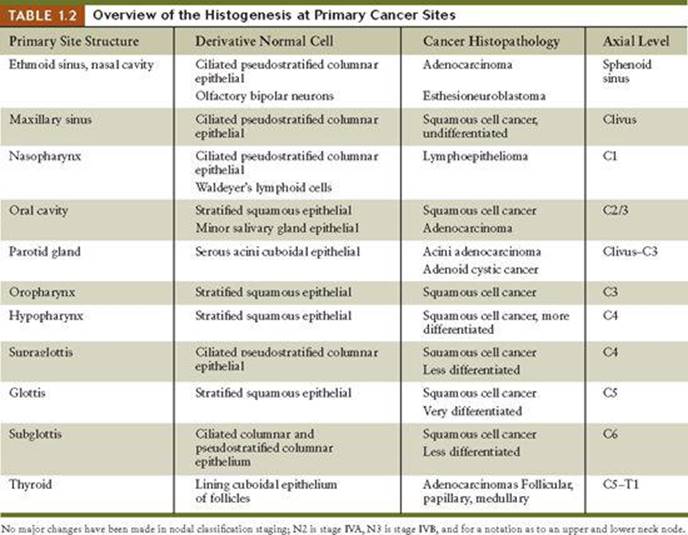
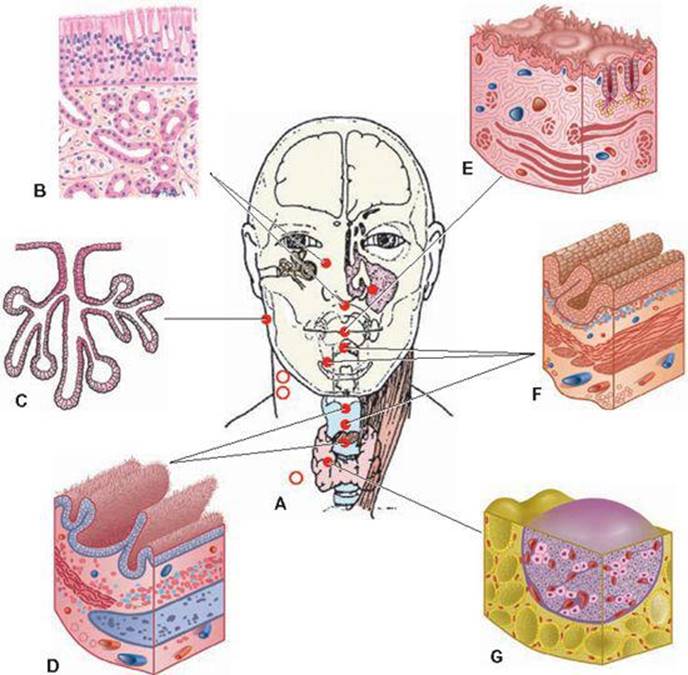
Figure 1.2 | Overview of Histogenesis. A. Primary cancer site isocenters. B. Paranasal sinus and nasopharynx. C. Salivary gland. D. Supraglottic and subglottic larynx. E. Oral cavity and tongue. F. Oropharynx and hypopharynx. G.Thyroid.
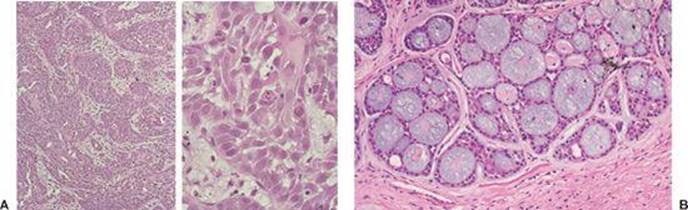
Figure 1.3 | A. Squamous cell carcinoma. Left (LM): An infiltrative neoplasm is composed of cohesive nests of tumor. Right (HM): A less differentiated tumor displays cells with pleomorphic nuclei, prominent nucleoli, brightly eosinophilic cytoplasm indicating keratinization, and intercellular bridges connecting adjacent cells. B: Adenoid cystic carcinoma showing cribriform growth in which cystlike spaces are filled with basophilic material. The cyst spaces are really pseudocysts surrounded by myoepithelial cells.
TNM STAGING CRITERIA
TNM STAGING CRITERIA
The head and neck area is generally considered one anatomic and physiologic unit because their boundaries are not well defined. Cancers arising in the different sites of the upper aerodigestive passages spread into the neck nodes as first station nodes. The specific site of the first node to be affected varies according to the origin of the primary tumor. In fact, every primary site drains into the cervical nodes as noted, but each site has a preference for a specific sentinel node. This is often the first evidence of cancer somewhere in the head, of an unknown primary. Because many midline areas drain bilaterally, both sides of the neck are vulnerable to cancer spread. Bilateral and contralateral lymphatic involvement also are common. Once one node is affected, the entire complex of lymph nodes in the neck is at risk because of altered flow into collateral channels.
The classification and staging of head and neck cancers are excellent prototypes for the classification and staging of cancer in general. There has always been a guiding principle to maintain uniform criteria across all anatomic primary sites. Two major modifications of T and N categories and stage grouping have been made based on survival data of clinical trials. Major changes in nodal criteria occurred with the third edition (1987) when criteria as N2 mobility versus N3 fixation of lymph nodes were changed to size. Size of nodes was adopted as the criterion to be more objective. A fixed node to the carotid artery was replaced by >6 cm in greatest diameter, and the N definitions N1 ≤3 cm, N2 3 to 6 cm, and N3 >6 cm have been uniformly applied across all head and neck sites except for the nasopharynx. In the sixth edition (2002), a major change in all sites was dividing the primary cancer into stage IVA T4a resectable, stage IVB T4b N2 unresectable, and stage IVC is for distant metastases.
In general, every effort has been made to bring the stage groupings of the head and neck to a relatively uniform combination of TNM criteria for all sites. This useful attribute would be beneficial to adopt at other anatomic cancer sites.
SUMMARY OF CHANGES SEVENTH EDITION AMERICAN JOINT COMMITTEE ON CANCER (AJCC)
• The terms “resectable” and “unresectable” are replaced with “moderately advanced” and “very advanced”
• No major changes have been made in the N staging for any sites except that a descriptor has been added. Extracapsular spread (ECS) of disease is added as ECS + or ECS − as a descriptor. These descriptors will not influence staging system.
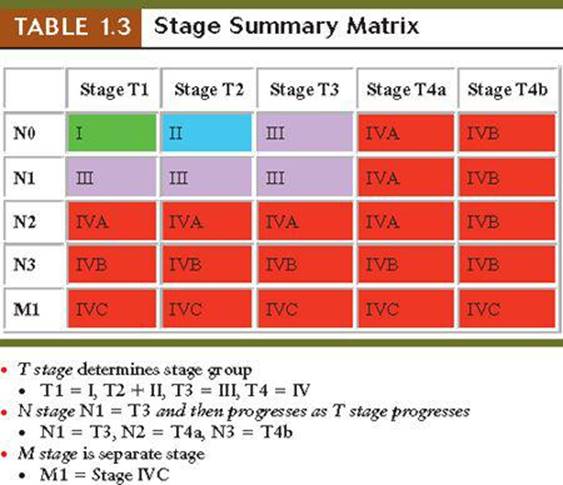
• The T stage determines the stage grouping with modifications by N stage. Size implying depth of invasion is the key criterion for primary tumors: T1 is >2 cm, T2 is 2 to 4 cm, and T3 > 4 cm. A uniform description of advanced tumors has been recommended: T4 lesions are divided into T4a resectable, T4b unresectable, and assignment to stage IVA and stage IVB, respectively. Stage IVC is metastatic disease.
• In the 7th Edition there have been moderate changes 2+ in Nasopharynx, and minor changes 1+ in the Thyroid.
• A new cancer site staging system for Muscosal Melanoma, which is illustrated in the Ethmoid Sinus chapter (Chapter 2).
Linguistically the T stage determines the stage group with modification by N stage. A major modification occurred when stage IV in fifth edition was divided into IVA, IVB, and IVC based on nodal extent (i.e., N1, N2, N3). In the sixth edition, T4 was divided into T4a and T4b and stage IVA and stage IVB, respectively. Size of primary tumor (2, 4, 4 cm) and size of regional lymph nodes (3, 6, 6 cm) remain the most important staging criteria. Figure 1.4 shows the TNM staging criteria for four key sites in the Head and Neck.
Genesis and Evolution of TNM Stages: First to Seventh Editions
The head and neck TNM staging system has remained relatively consistent over five decades with an important guiding principle; that is to maintain uniform definitions of T and N across all sites. Modifications of T and N categories in stage grouping are based on survival data of clinical trials in the literature using the American Joint Committee on Cancer/International Union Against Cancer (AJCC/UICC) systems. Benchmark survival curves are presented for major primary sites by stage.

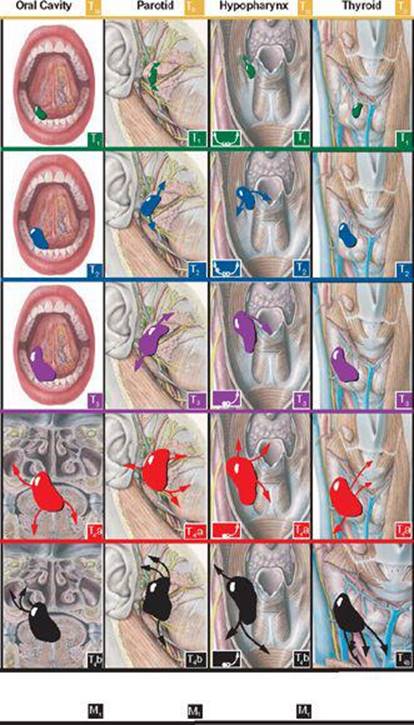
Figure 1.4 | T stage grouping. Vertical presentations of stage groupings for Oral Cavity, Parotid, Hypopharynx, and Thyroid, which follow same color code for cancer stage advancement are organized in horizontal lanes: Stage 0, yellow; I, green; II, blue; III, purple; IVA, red; and IVB, black. Definitions of TN on left and stage grouping on right.
T-ONCOANATOMY
ORIENTATION OF T-ONCOANATOMY: ODYSSEY OF PRIMARY SITES
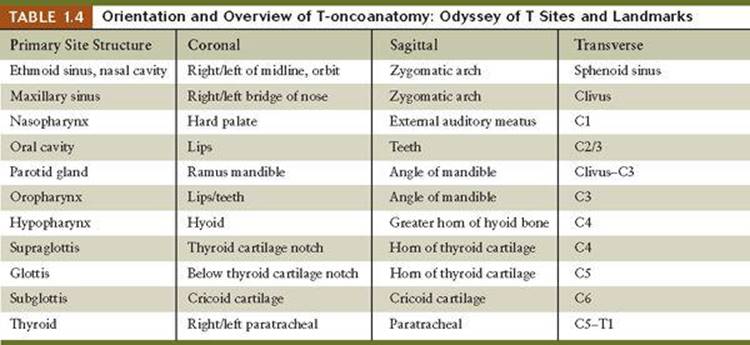
The anatomic isocenter of a primary cancer site is the intersection of the three planar T-oncoanatomy views: coronal, sagittal, and transverse, taken from Grant's Atlas of Human Anatomy. The axial orientation of the vertebral level is an important imaging reference point. Surface anatomy can vary from patient to patient; however, it is presented as a guide for the localization of the cancer in both accessible and internal anatomic sites that cannot be assessed on routine physical examination. The red bullets in our multilayered coronal (Fig. 1.5A) and sagittal (Fig. 1.5B) planes are a combination of both superficial and deep landmarks to identify primary sites. The tabulation of oncologic anatomy in the head and neck region starts at the base of the skull, and primary sites of head and neck cancers are noted in an axial fashion from cephalad to caudad and are arranged along planes anterior to the entire cervical spine from C1 to C7. There are two major anatomic sectors with 11 distinct cancer primary sites currently staged (Fig. 1.5C; Table 1.4). These sectors are the upper aerorespiratory passage consisting of the nasal cavity, paranasal sinuses, the nasopharynx and the larynx; and the upper digestive passage, which contains the oral cavity, lips, oropharynx, and hypopharynx. Taken together, the anatomic physiologic complexity lies in the oropharynx, which is common to both systems.
Cervical fascial planes are important for compartmentalizing the neck and have a major impact on staging. To appreciate the neck compartments, axial and sagittal views are required. The anterior compartment is defined by an investing fascia that envelopes the sternocleidomastoid muscle, and superficial muscles, which are usually considered resectable (Stage IVA), and houses the pharynx, larynx, and thyroid gland. Therefore, when pharyngeal cancer spread is anterior and inferior, it is more often amenable to surgical removal. With posterior and superior invasion patterns, pharyngeal cancers penetrate the prevertebral fascia into the prevertebral space, which is not resectable (Stage IVB). Lateral spread into the carotid sheath is also an ominous sign; fixation of lymph nodes to the carotid artery renders the cancer unresectable. Clinically, it is difficult to diagnose cancer fixation to arteries; therefore, cancer node size >6 cm makes the evaluation more objective and has been shown to correlate with carotid artery involvement. The retropharyngeal space is ideal for pharyngeal cancer (Fig. 1.3C) spread vertically, but once the prevertebral fascia has been invaded, the cancer is no longer resectable. A concise overview (odyssey) of the 11 primary sites follows:
1. Cancers of the ethmoid sinus are the most superior in the head and neck region, whereas frontal sinuses and the sphenoid sinus tumefaction are rare and secondary to other neoplastic processes. Esthesioneuroblastoma can arise in the roof of the nasal cavity and involve the cribriform plate. Paranasal sinus cancer spread into other sinuses and orbital invasion are common.
2. Cancers of the nasopharynx can be insidious in onset and highly metastatic to lymph nodes. Cranial nerve involvement is due to cancer entry of the cavernous sinus via the foramen lacerum involving cranial nerves III, IV, V, and VI. In contrast, enlarging cervical metastatic lymph nodes, the highest in the deep cervical chain (Rouviere's node), can compress cranial nerves IX, X, XI, and XII.
3. Cancers of the maxillary antra can masquerade as unilateral sinusitis and only become evident as the paper-thin bones (lamina papyracea) erode, loosening of molar teeth occurs, erosion into the cheek, destroying the zygomatic arch, occurs, and most catastrophically erosion into the orbit. The sentinel node tends to be submaxillary and therefore misleading.
4. Cancer of the lips and oral cavity can arise at numerous subsites that initiate the upper digestive passage. The common sites of malignancies are the food gutters, namely the floor of mouth and lateral border of the tongue. The sentinel nodes are often a function of the exact anatomic location of the primary cancer. With 10 different oral cavity subsites, anterior cancers lead to submental and submaxillary nodal invasion, whereas posterior neoplasms result in jugulodigastric nodes.
5. Neoplasms of the parotid gland are highly varied, and even benign mixed pleomorphic adenomas tend to recur, as can low-grade mixed mucoepidermoid cancers. Perineural invasion of cranial nerves VII, V, or both is a characteristic of cylindromas. The parotid gland lymph nodes are both the regional and sentinel nodes in this location. Prolonged survival even in the face of pulmonary metastasis is a peculiarity of some salivary gland cancers.
6. Cancer of the oropharynx arises at the isocenter of the upper aerodigestive passage, which houses Waldeyer's ring, a favored site for malignant transformation. The underlying muscular planes predetermine spread patterns. The sentinel node is the jugulodigastric. Odynophagia referred to the middle ear is due to Jacobson's branch of cranial nerve IX.
7. Cancers of the hypopharynx may surround the larynx and block the food bolus, leading to aspiration into the larynx. Dysphagia can be caused by local invasion as well as cranial nerve involvement. The jugulo-omohyoid is often the sentinel node and can be invaded in contiguity with a primary.
8–10. Cancers of the larynx are divided into three parts: the supraglottis, glottis, and subglottis. Vocal cord involvement can be an early sign of malignancy. The malignant gradient varies with true glottic cancers being most readily detected in the earlier stages and therefore highly curable, whereas both the supraglottic and especially the subglottic cancers can be silent and more egregious in onset. Transglottic cancers advance as the cancer crosses the vocal cords. Paratracheal or paralaryngeal nodes can be the sentinel nodes. Odynophagia referred to the outer external ear is due to Arnold's nerve, a branch of the vagus (cranial nerve X), which supplies sensation to the larynx.
11. Thyroid cancers, although considered part of head and neck tumors, are unique because they arise from an endocrine gland and not an epithelial surface. The cancers can be well-differentiated colloid or papillary adenocarcinomas compatible with long survival despite lymph node invasion. Although the Delphic lymph node located above the isthmus can be the sentinel node, more often the inferior deep jugulo-omohyoid nodes are at risk. Anaplastic cancers can be highly lethal and metastasize early to the lungs.
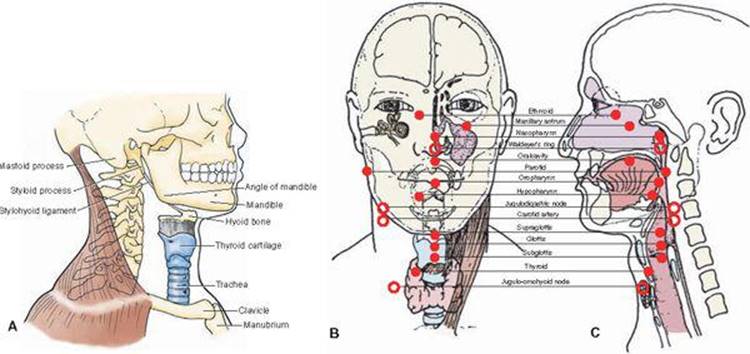
Figure 1.5 | Orientation of T-oncoanatomy. The locations of 11 primary cancer sites are indicated at their anatomic isocenters with red bullets. Open circles are important lymph nodes. A. Bone and cartilage frame for head and neck primary sites. B. Coronal. C. Sagittal.
N-ONCOANATOMY
ORIENTATION OF REGIONAL LYMPH NODES: N-ONCOANATOMY
Understanding the complex anatomy of the neck is essential to appreciate the many nuances and evolution of changes. Most important is an appreciation that the major regional nodal areas are divided into superficial and deep cervical node chains; the latter includes the high retropharyngeal and parapharyngeal nodes. Each of the major head and neck cancer sites drain into a specific region of neck nodes—sentinel nodes (Fig. 1.6; Table 1.5). Some have unilateral drainage, others bilateral. The most commonly involved lymph nodes are those along the internal jugular vein, which are subdivided into superior, mid, and inferior deep cervical node chains. They include the jugulodigastric and jugulo-omohyoid, and the scalene nodes in the anterior aspect of the supraclavicular fossae. A series of two planar orientation diagrams of regional lymph nodes and their lymphatics are shown in anterior and lateral views (Fig. 1.6A–C). Each primary anatomic site or subsite has a sentinel node or favored nodes to which it drains preferentially. This can be determined clinically by injecting a radiocolloid such as Tc99m or methylene blue dye at the primary site and dissecting the node that concentrates the most radioactivity. It is equally important to be aware of all the lymph nodes at risk. The clinician needs to locate first station nodes in three planes to determine if they are accessible for physical examination.
Traditionally, the triangles of the neck are used to define the topographic anatomy that consists of anterior and posterior triangles (Fig. 1.6D). The sternocleidomastoid muscle divides the neck into these two major triangles; many other small triangles exist. The external jugular vein and the platysma muscle are superficial to the sternocleidomastoid muscle. Deep to the sternocleidomastoid are the carotid artery, internal jugular vein, and some cranial nerves. Deep cervical lymph nodes also surround the carotid sheath. The lymphatic channels and lymph nodes are located more anteriorly as they follow the sternocleidomastoid muscle inferiorly. The nodes in the neck make up one of the most important sections of oncologic anatomy. The lymphatics of the head are, in essence, the lymphatic channels in the neck and their lymph nodes. Regional nodes are not always the closest anatomically to the primary site nor are the sentinel nodes solely involved with cancers of the head and neck. Distant primary sites both above and below the diaphragm can spread to neck nodes, especially supraclavicular nodes (Virchow's node).
The nomenclature we use is that of The International Anatomical Terminology, and this correlates with various staging systems and terms proposed by the AJCC. The AJCC has grouped regional lymph nodes in the neck into seven levels and subdivided specific anatomic subsites (Fig. 1.6D). Each level is designated by a roman numeral (I–VII). Lymph node-bearing region is promulgated by Hodgkin's lymphoma staging rather than anatomic physiologic considerations and deserves to be reconsidered in terms of cancer spread. According to AJCC/UICC clinical staging for Hodgkin's lymphoma, each side of the neck is one lymph node–bearing region (Fig. 1.6E). The lymphoid tissue of Waldeyer's ring is an extranodal lymphoid collection that forms the palatine tonsils. The lymphoid tissue extends superiorly into the pharyngeal wall and the roof of the nasopharynx and inferiorly into the base of the tongue. Midline anatomic sites such as Waldeyer's ring drain bilaterally, whereas paired or parallel structures drain unilaterally to their respective deep jugular nodes, right or left.
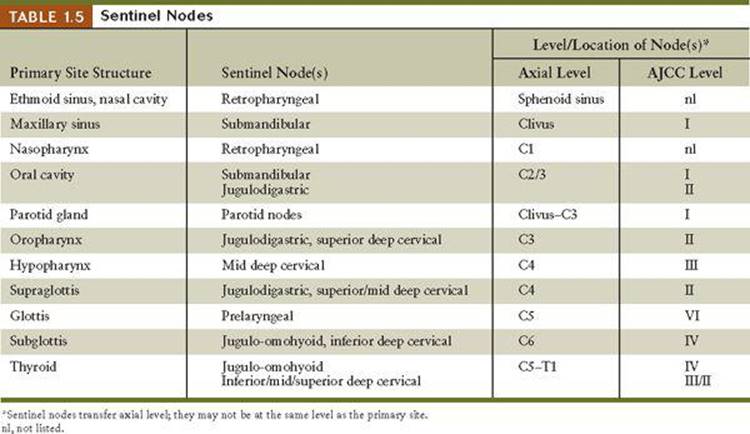
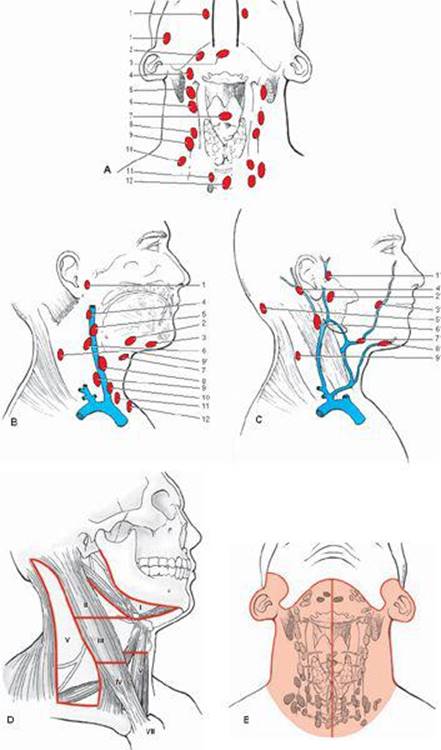
Figure 1.6 | Orientation of N-oncoanatomy. The neck or cervical nodes are regional nodes for the 11 primary cancer sites. Any cluster can be a sentinel node that drains a specific site (A, B, C). These are assigned using the international anatomical terminology and are identified by number to note clusters of regional nodes that could be sentinel nodes. A. Anterior view of deep jugular nodes. B. Lateral view of deep nodes with the sternocleidomastoid muscle removed. Anterior deep jugular (A) and lateral (no sternocleidomastoid muscle, (B) lymph nodes: (1) retropharyngeal; (2) submandibular; (3) submental; (4) superior deep cervical; (5) jugulodigastric; (6) mid deep jugular; (7) prelaryngeal; (8) jugulo-omohyoid; (9) inferior deep cervical (jugular); (10) supraclavicular; (11) paratracheal; and (12) pretracheal. (C) Lateral view of superficial nodes: (1′) prearicular; (2′) parotid; (3′) facial; (4′) mastoid; (5′) superficial cervical; (7′) submandibular; (8′) submental; and (9′) spinal accessory. D. AJCC nomenclature of seven levels of cervical lymph nodes. E. Node-bearing region according to staging in Hodgkin's lymphoma.
M-ONCOANATOMY
M-ONCOANATOMY OF REGIONAL VEINS AND THE NEUROVASCULAR BUNDLE
The head and neck are generally considered an anatomic and physiologic unit; all sites share a common regional arterial blood supply and venous drainage (Fig. 1.7A). Most of the upper aerodigestive passages are supplied by the branches of the carotid artery. Their venous drainage is through the pterygoid venous plexus deep to the masseter muscle and is retropharyngeal, next to the posterior aspect of the parotid gland and then by way of the jugular veins. Cancer can disseminate hematogenously through vascular routing most often to the superior vena cava to the right side of the heart and lung via the pulmonary circulation and then to other organs systemically. Lung is the target organ for the first signs of distant metastases for the majority of head and neck cancers.
The cranial nerves become peripheral as they exit the skull to innervate the head and neck region. Cranial nerves IX, X, XI, and XII descend in the neck with the carotid artery and internal jugular vein and constitute the major neurovascular bundle in the head and neck region (Fig. 1.7B). Metastatic cancer to the deep chain of jugular lymph nodes can produce cranial neuropathy. Rouviere's node is the highest cervical node; it is clinically inaccessible and retropharyngeal in location (Fig. 1.7C,D).
Jugular foramen syndrome is characterized by loss of the gag reflex (cranial nerve IX), vocal cord paralysis (cranial nerve X), atrophy of the trapezius muscle (cranial nerve XI), and deviation of the uvula (cranial nerve X) and tongue on protrusion (cranial nerve XII).
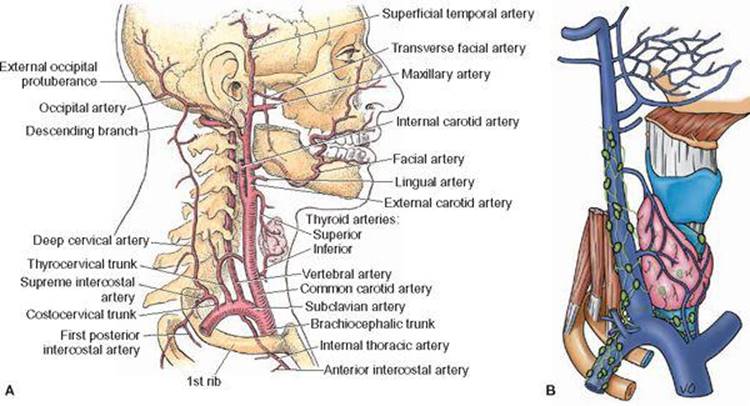
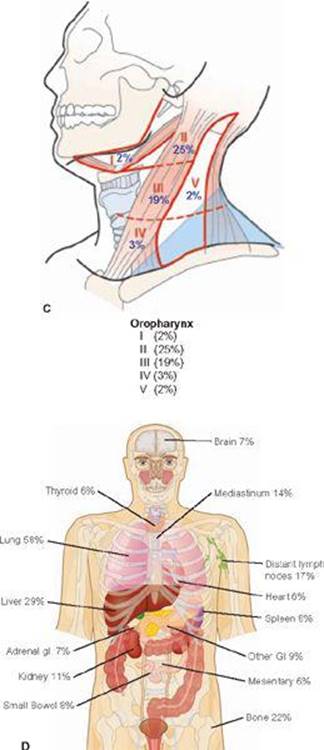
Figure 1.7 | Orientation of M-oncoanatomy. A. Carotid artery with major branches shown. B. Pterygoid plexus of veins drains most of head and neck sites into internal deep jugular. Note green small normal lymph nodes are juxtaposed. The jugular vein drains into the superior vena cava and then into the right heart, making lung the target organ. C&D| C. Percent of positive nodes in clinically negative (N0) neck in Oropharyngeal cancer according to AJCC levels. D. The Incidence and Distribution of Distant Metastases of Oropharyngeal Cancers. The oropharyngeal cancers can serve as a prototype for head and neck cancers. Lung (58%) is the target organ with liver metastases next (29%) and bone metastases third (22%) followed by distant lymph nodes (17%), mediastinum (14%). The remainder of sites are 11% (kidney) or less than 10%.
CRANIAL NERVES AND NEUROVASCULAR BUNDLE
The importance of appreciating the complex anatomy of cranial nerves lies in the patterns of cancer spread at the primary cancer site as well as nodal spread patterns. Perineural invasion or compression by metastatic lymph nodes often is manifested by specific neurologic symptoms and signs. The overview of cranial nerves provides an intricate roadmap as to points of vulnerability (Figure 1.8).
Cranial nerve invasion can produce specific syndromes and neurologic evaluation is a vital part of physical diagnosis in all head and neck cancers.
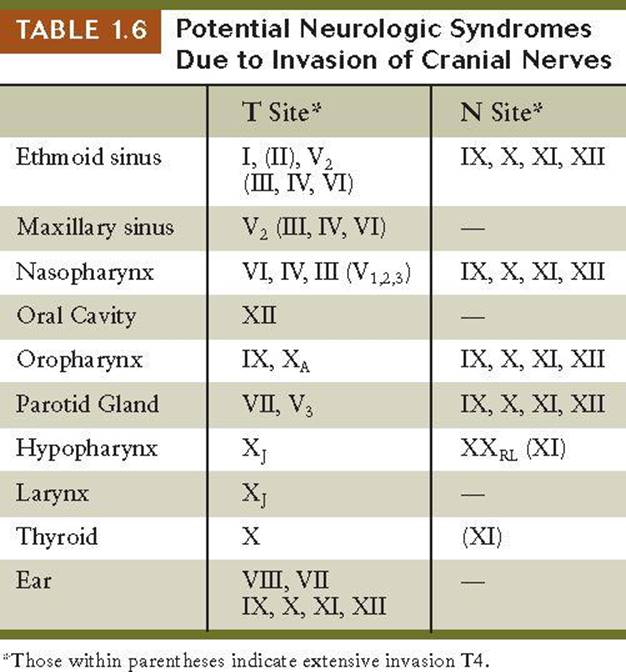
A tabulation of potential neurologic syndromes either due to perineural invasion at the primary site or nodal compression will alert the astute clinician to extent of cancer advancement anatomically (Table 1.6).
1. Ethmoid sinus cancers are midline and invade the nasal cavity at the crista galli and the penetrating branches of the olfactory nerve. The esthesioneuroblastoma arises from the ganglion organ of Jacobson. Cancers pick off the V2, resulting in hypesthesia of upper lip, then invade the orbit, can compress III, IV, VI, and optic nerve II. Nodal drainage to retropharyngeal nodes (Rouviere's node) can lead to compression of IX, X, XI, or XII as they exit along the carotid artery and jugular vein.
2. Maxillary antrum cancers tend to invade lamina papyrea, then bone walls (i.e., superiorly the infraorbital nerve will result in a circle of anesthesia below the lower eyelid and then invasion of the orbit resulting extraocular invasion of III, IV, VI and eventually II posteriorly).
3. Nasopharynx cancers enter the parapharyngeal space and then invade through the foramen lacerum, enter the cavernous sinus and pick off CN V, IV, and III in that order causing diplopia. As it extends laterally, the Gasserian ganglion is encountered. V1 eyelid anesthesia, V2 upper lip and nasal anesthesia, and V3 lower face anesthesia can occur when Retropharyngeal (Rouviere's) node compresses the neurovascular bundle of CN IX, X, XI, and XII, exiting the skull alongside the carotid artery and jugular vein.
4. Oropharynx cancers invade the CN IX first and refer pain on swallowing along the vagus nerve to the middle ear (Jacobson's nerve). The sytlopharyngeal muscle as well as palate is paralyzed and there is absence of gag reflex. Taste is affected on the posterior third of the tongue. Retropharyngeal nodes can entrap (CN IX, X, XI, and XII) in the neurovascular bundle.
5. Salivary gland or parotid gland cancers tend to invade the facial nerve CN VII as it exists from the stylohyoid foramen and result in impairment of facial musculature depending on its invasion of branches versus the main nerve. Sensory taste in the anterior two thirds of the tongue and soft palate can be altered. Cylindromas are notorious for perineural invasion and if branches of V3 mandibular nerve are involved, it can penetrate into the Gasserian ganglion into the middle fossa.
Retroparotidean nodes can compress IX, X, XI, and XII, especially if the primary involves the deep lobe. Retroparotidean nodes can compress IX, X, XI, and XII, especially if the primary involves the deep lobe. Retroparotidean nodes can compress IX, X, XI, and XII, especially if the primary involves the deep lobe.
6. Oral cavity cancers can invade the floor of the mouth and the hypoglossus CN XII leads to unilateral paralysis with tongue on protrusion pointing to the paralytic side. Invasion of V3 mandibular branch results in sensory loss of lower third of face. Muscle impairment of mastication muscles can result in drooling. Submandibular nodes rarely lead to neurologic events.
7. Hypopharyngeal cancers tend to invade the CN X vagus nerve, causing vocal cord paresis and pain on swallowing is referred to external ear (Arnold's nerve).
Deep cervical nodes on the right side can extend into the supraclavicular nodes and entrap the recurrent laryngeal nerve on that side. Massive extranodal invasion could involve the spinal accessory nerve CN XI and lead to paresis of sternocleidomastoid muscle and trapezius.
8. Larynx cancers directly invade into vocal cord, and hoarseness results rather than nerve invasion. Supraglottic cancers can lead to referred pain and swallowing along CN X Arnold's nerve to outer ear.
Deep cervical nodes in advanced stages can entrap the recurrent laryngeal nerve on the right side.
9. Ear tumors vary depending on location:
Acoustic neuromas lead to deafness and can compress the intermediate branch of CN VII, altering taste in the anterior two thirds of the tongue.
Jugular foramen chemodectomas can compress the neurovascular bundle and mimic retropharyngeal node, impairing CN IX, X, XI, and, by eypansion, XII.
External auditory canal cancers can invade and involve the facial nerve CN VII and lead to unilateral facial muscular paresis. External auditory canal cancers can invade and involve the facial nerve CN VII and lead to unilateral facial muscular paresis. External auditory canal cancers can invade and involve the facial nerve CN VII and lead to unilateral facial muscular paresis.
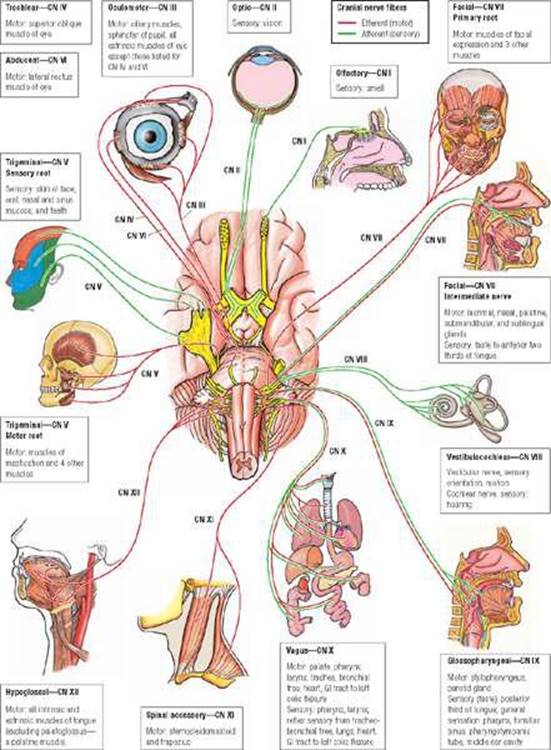
Figure 1.8 | Cranial nerves
STAGING WORKUP
RULES FOR CLASSIFICATION AND STAGING
Clinical Staging and Imaging
Clinical staging is an essential step in establishing meaningful data. Physical examination includes visualization of upper aerodigestive passage whenever possible and is often combined with mirror or direct endoscopy. Palpation is critical to define endophytic induration whenever feasible. Imaging is important, particularly spiral computed tomography (CT) and magnetic resonance imaging (MRI), which can provide superb visualization of the three-planar anatomy. MRI provides better visualization of soft tissue cancer infiltration; CT better detects bone destruction. The difference in density of tissue planes allows for viewing fat as black on CT and white on MRI, in contrast to the gray of muscles and viscera in contrasting these diagnostic modes (Fig. 1.9). Cancer can be enhanced by contrast administration owing to a greater degree of tumor neovascularization versus normal tissue vascularity. However, MRI is better than CT in that tumorous infiltrates appear intensely white. Identification of enlarged lymph nodes (>1 cm2) requires contrast visualization of arteries and veins (white) on CT; blood flow allows for a black image of the neck vessels on MRI. Each anatomic site is discussed for nuances, imaging highlights, and notations. Suspicious neck nodes need fine needle aspiration for confirmation (Table 1.7). An excellent reference from which oncoimaging notations highlight important aspects of cancer spread and staging at each primary site is by Bragg, Rubin, and Hricak (2002).
Pathologic Staging
Gross specimen should be evaluated for margins. Unresected gross residual tumor must be reported and marked with clips. All resected lymph node specimens should describe size, number, and level of involved nodes and whether there is extracapsular spread. Specimens postradiation and/or chemotherapy need to be so noted. Specimen shrinkages may occur up to 30% after resection itself. Designations pT and pN should be used after histopathologic evaluation. Perineural invasion deserves special notation.
Histogenesis
The histopathology grading of squamous cell cancers are recommended to be defined in a four-grade system generally is defined as:
Gx Grade cannot be assessed
G1 Well differentiated
G2 Moderately differentiated
G3 Poorly differentiated
G4 Undifferentiated
Lymph node dissections are defined as:
Selective when six nodes are removed, if there is a lesser number they should still be pathologically assessed.
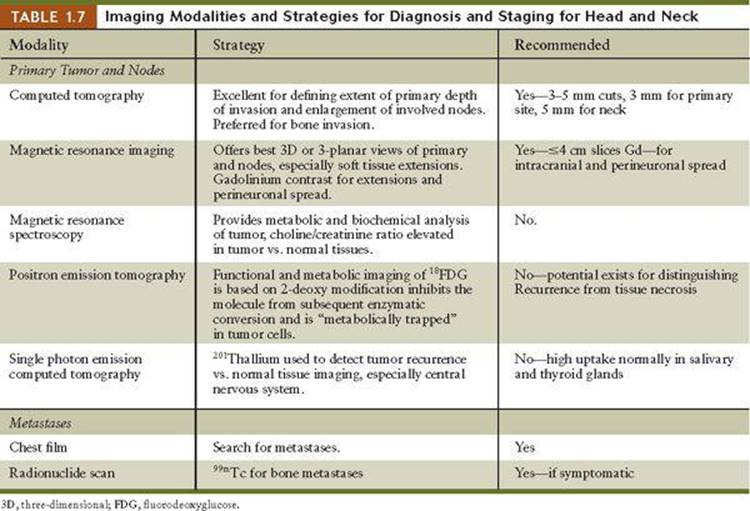
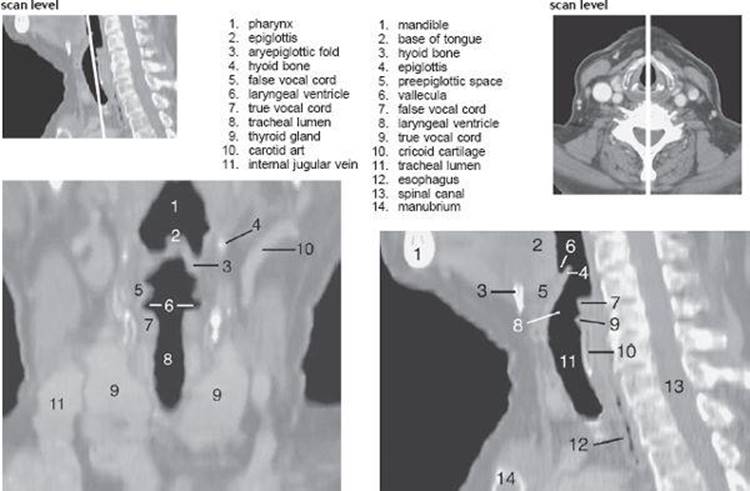
Figure 1.9 | CT scans of head and neck. Another new feature is the addition of CT or MR images to correlate with the axial level in each site specific chapter.
Radical or modified radical requires at least 10 or more nodes are removed.
Imaging criteria for nodal involvement in addition to size are noted for extracapsular spread (ECS) (i.e., speculated margins, loss of intranodal fat, and change in shape from oval to round).
General performance can impact survival. The Performance Scale (ZuGrod, European Cooperative Oncology Group [ECOG]) should be used:
0. Fully active, able to carry on all predisease activities without restriction (Karnofsky 90–100)
1. Restricted in physically strenuous activity but ambulatory and able to carry work of a light or sedentary nature. For example, light housework, office work (Karnofsky 70–80).
2. Ambulatory and capable of all self-care but unable to carry out any work activities. Up and about more than 50% of waking hours (Karnofsky 50–60).
3. Capable of only limited self-care, confined to bed or chair 50% or more of waking hours (Karnofsky 30–40).
4. Completely disabled. Cannot carry on self-care. Totally confined to bed (Karnofsky 10–20).
5. Death (Karnofsky 0).
• Comorbidities are advised to be included in medical record such as depression and diabetes; infection such as human papilloma virus (HPV) or AIDS/HIV.
• Lifestyle habits as tobacco use in past years and alcohol use as drinks/day/week/month, etc.
• Weight loss of more than 10%.
Head and Neck Glossary
(U) Upper
(L) Lower
(ESC) Extracapsular Spread (E) Evident and on clinical/imaging work up
(En) No Extranodal Extension Applies to ECS
(Em) Microscopic Applies to ECS
(Eg) Gross Applies to ECS
(NMSC) Non melanoma skin cancer
(PPS) Prestyloid space
(CS) Carotid space
(RPS) Retropharyngeal space
(PVS) Prevertebral space
pN Selective neck dissection 6 nodes
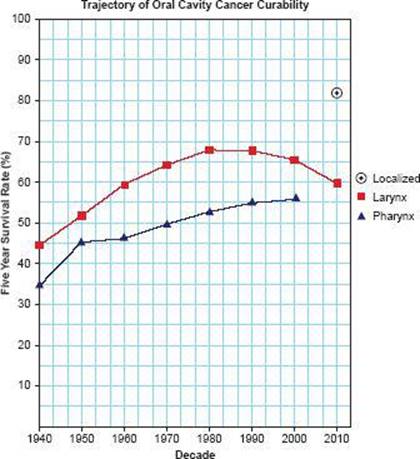
Figure 1.10 | Survival Graph. Survival of cancer in head and neck over seven decades: 1940 through 2010 based on ACS SEER data.
PROGNOSIS AND SURVIVAL
Prognostic Factors
Prognostic factors related to the host are variously cited throughout the head and neck sites.
Specific Tabulation of prognostic factors that are Site Specific Factors recommended for collection is a new feature and varies in its details.
Clinically significant:
• Size of lymph nodes
• Extracapsular extension from lymph nodes for head and neck
• Head and neck lymph nodes levels I-III
• Head and neck lymph nodes levels IV-V
• Head and neck lymph nodes levels VI-VII
• Other lymph node group
• Clinical location of cervical nodes
• Extracapsular spread (ECS) clinical
• Extracapsular spread (ECS) pathologic
• Human papillomavirus (HPV) status
• Tumor thickness*
CANCER STATISTICS AND SURVIVAL
Cancers of the oral cavity and pharynx—the upper digestive passage—account for 36,540 new cases per year. In addition,
*The foregoing passage is from Edge SB, Byrd DR, and Compton CC, et al, AJCC Cancer Staging Manual, 7th edition. New York, Springer, 2010, p. 38.
cancers of the larynx provide another 12,720 patients and thyroid cancers, 44,670. Approximately 25% of head and neck cancer patients die annually, often from other causes. For long-term survival, thyroid cancers, with only 1,500 deaths (5%), are the exception. The improvement in oral cavity and pharyngeal tumors from 1950 to 2000 was modest (14%) and matches larynx (15%). A multidisciplinary approach is vital and normal tissue conservation and reconstructive techniques have added greatly to quality of life. Unfortunately, this patient population comprises ethanol and nicotine abusers and it is difficult to change their habits. Persistence of smoking and drinking contributes to their demise, often from second malignant tumors in adjacent sites (Fig. 1.10).
Remarkably, >55% of patients are alive at 5 years; the majority live to 10 years. When treatment fails, death is within 2 years in 90% of patients and is often painful and disfiguring. African Americans in particular tend to die at a higher rate (75%). Another source for assessing the gains in survival in head and neck cancers is based on the multidisciplinary approach to management in national cooperative groups. The large database accumulated by the Radiation Therapy Oncology Group allows for 5-year survival analysis by major anatomic sites and their subsites as a function of stage. Stage I patients survive at the 60% to 80% level, stage II at 40% to 60%, stage III at 30% to 60%, and stage IV at 15% to 30%. With combined modality treatment, chemoradiation and surgery yields complete response rates of 45% to 95% depending on stage and often allows for preservation of normal structures (e.g., larynx).
In reviewing, the AJCC 7th Edition data confirms the importance of early diagnosis in head and neck cancers where survival is better than 50% prior to development of lymph node metastases (Fig. 1.11).
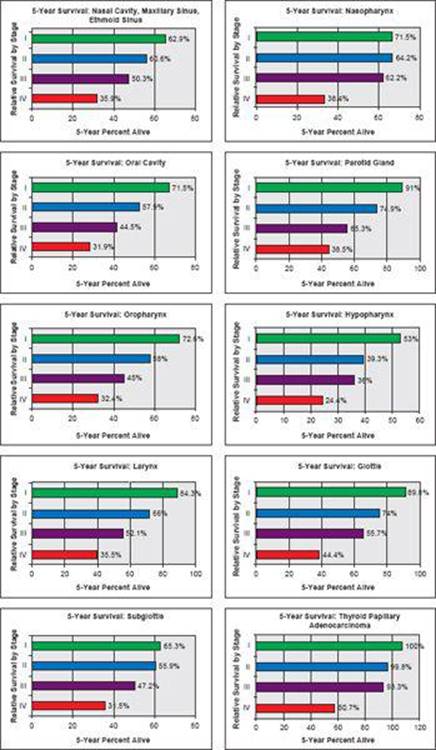
Figure 1.11 | AJCC 7th Edition data confirms the importance of early diagnosis in head and neck cancers where survival is better than 50% prior to development of lymph node metastases. Once cervical lymph node metastases occurs, the survival decreases to 30–40% but varies with larynx cancer still yielding 50–55% survival in advanced Stage III due to effective chemoradiation regimens. Exception to the rule is thyroid papillary/follicular adenocarcinomas that have 90–100% survival for stage I–III. (Data from Edge SB, Byrd DR, and Compton CC, et al, AJCC Cancer Staging Manual, 7th edition. New York, Springer, 2010.)