Anatomical position 2
Movement (Figs 1.2-1.8) 2
Pathological terms 3
Anatomy and clinical practice 4
Clinical assessment 4
General examination 5
Instruments of clinical examination (Figs 1.9-1.11) 5
Anatomical position
The anatomical position, about which anatomical relationships are orientated, is one in which the subject stands upright, with feet together, eyes looking forward and arms straight down by the sides of the body with palms facing forward (Fig. 1.1). The structures in front are termed anterior (ventral), those behind posterior (dorsal). An exception to this rule is the foot, which is rotated inwards during development: the under (plantar) surface is referred to as ventral and the upper as dorsal. Structures may be nearer to (medial) or further from (lateral) the midline and those in the midline are called median. Structures above are superior (cranial, rostral) and those below are inferior (caudal). A sagittal plane passes vertically, anteroposteriorly through the body (the midsagittal plane being in the midline). A coronal plane passes vertically at right angles to the sagittal plane. Transverse (horizontal) planes pass horizontally through the body. Proximal and distal are terms indicating the proximity of a structure to the centre of the body; the wrist is proximal to the hand and the ankle is distal to the knee.
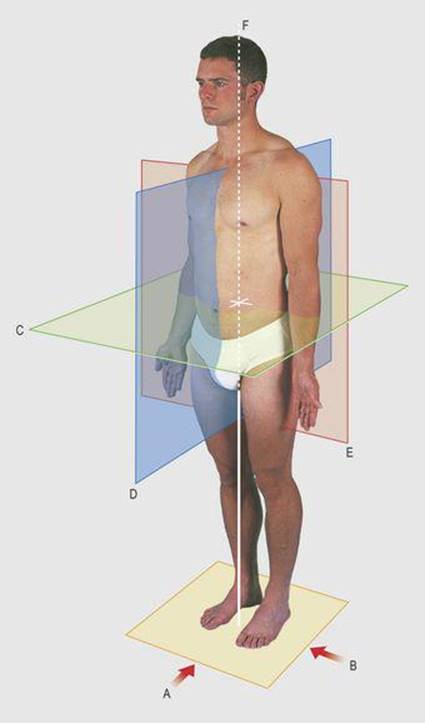
1.1 Anatomical position
A, anterior aspect; B, lateral aspect; C, transverse plane; D, sagittal plane; E, coronal plane; F, median line
Movement (Figs 1.2-1.8)
Forward movement in a sagittal plane is usually flexion and backward movement extension. Owing to the rotation of the lower limb during development, backward movement of the leg extends the hip and flexes the knee. Upward movement of the ankle is dorsiflexion (extension) and downward movement is plantarflexion (flexion). Downward movement of the toes is flexion.
1.2 Flexion

1.3 Extension

1.4 Abduction

1.5 Adduction
1.6A Medial rotation


1.6B Lateral rotation

1.7 Pronation

1.8 Supination
Movement away from the midline in the coronal plane is abduction and movement towards the midline is adduction. In the case of the digits (excluding the thumb), however, abduction is away from the central line of the middle finger or second toe and adduction is towards it.
Note that the functional axis of the foot is the centre line of the second toe.
The thumb is regarded as ‘rotated’ through 90° with respect to digits 2–5, i.e. its nail faces laterally. Thus extension is lateral movement in the plane of the palm (coronal); flexion is medial movement across the palm; abduction is movement in the sagittal plane (90° to the palmar plane); adduction is return from the abducted position; and opposition is a combination of the above movements with medial rotation. (This also applies to the little finger – Fig. 7.64, p. 89.)
Side-to-side movement of the neck and trunk is termed lateral flexion. Circumduction is the movement when the distal end of a bone describes the base of a cone, with its apex at the proximal end.
Rotation occurs in the long axis of the bone. In the limbs it may be medial, towards the midline, or lateral, away from it. In the upper limb, medial rotation of the forearm is termed pronation and lateral rotation (from the prone to the anatomical position) is termed supination. Turning the sole of the foot towards the midline is termed inversion and away from the midline eversion.
Pathological terms
This text demonstrates normal anatomy, but abnormal features that are commonly encountered in clinical practice are noted. The pathological terms considered in this section are subsequently used without definition. The study of abnormal (diseased) tissue is termed pathology. Pathologists examine tissues directly by eye (macroscopically), such as in the postmortem room and tissues removed at surgery, or microscopically, when small samples of tissue are specially prepared and looked at under a microscope. Diseases can be classified by their cause and each disease has characteristic clinical and pathological features.
Congenital disease indicates that the abnormality is present before or at birth, although occasionally it does not become apparent until later life. There is sometimes a familial tendency in a disease; it is then also termed hereditary. Trauma usually indicates physical violence, with a blunt or sharp instrument. It may also be due to raised or lowered temperature, irradiation, chemicals and the ingestion of poisons. Severe trauma may break bones (fractures) and displace articular surfaces of joints (dislocation). Penetrating wounds (e.g. from a knife or bullet) may damage deep organs, vessels and nerves.
Inflammation is the body's cellular response to injury. It is usually in response to harmful bacteria or viruses, and this is termed infection, but it also occurs around sites of trauma and around malignant tumours. Cells may reproduce without a stimulus such as infection and form an abnormal mass of tissue known as a tumour or neoplasm (the process being neoplasia). This mass may be slow-growing and well circumscribed and is termed a benigntumour.
Rapidly enlarging tumours growing into adjacent structures are termed malignant. Carcinoma is a malignancy of epithelial tissue, but the term is often used as a synonym for any malignancy. Bits of malignant tumour may break off and be carried along lymph and blood vessels to start growing elsewhere. These additional growths are termed secondaries or metastases. Secondary growths often occur in lymph nodes; specific sites for lymph node metastases are mentioned in the text.
As the body grows older it functions less efficiently and specific degenerative diseases can occur such as dementia, from loss of cerebral cells, and hardening and blocking of the arteries (arteriosclerosis). Malfunction of metabolicprocesses and endocrine function may produce detectable physical, as well as biochemical, abnormalities.
Anatomy and clinical practice
In clinical practice, clinicians examine living anatomy, and surface anatomy may be the only anatomy encountered in many professional practices. However, all doctors and other clinical professionals need to know the range of normal anatomy, to be able to identify bony and prominent structures, and to know the position of deeply related structures. Superficial and deep tenderness may accompany inflammation and abnormal lumps may be congenital abnormalities, or benign or malignant tumours. Pain and tenderness accompany trauma, and bones and joints are palpated for fractures and dislocations, and deeper relations considered, particularly after penetrating injuries.
Clinical assessment
Examination of the adult patient requires the patient's consent. In the clinical setting, this usually follows taking a history of the patient's present and past illnesses and general health. It requires an explanation of what is proposed, and the patient's verbal acceptance. For more invasive procedures, including all surgical operations, written consent must be obtained.
The clinical examination must be undertaken in an organised manner, so that it is comprehensive and reproducible, and of a form that inspires confidence in the patient. It is primarily directed at the current clinical problem, but usually involves a general examination of all systems in order to exclude coexistent, sometimes unexpected, disease.
Clinical (bedside) examination involves assessment of each region of the body by inspection, palpation, percussion and auscultation. To this is added the assessment of active and passive movement of the joints and of neurological function. Inspection requires a warm, appropriate, secluded area so that the region being studied is fully exposed and in optimal lighting. The patient is usually lying on his/her back on a couch and the clinician stands on the right side, having first washed and warmed his/her hands. The skin and contours are observed from different angles to identify superficial structures, abnormal swellings and scars, vascular pulsations and movements, such as those related to breathing, swallowing and coughing.
Palpation of superficial structures delineates their shape, surface and consistency. Bony contours can be examined when they are not covered by prominent muscles or other structures. Some superficial nerves and glands are palpable. Lymph nodes such as those inferior to the angle of the mandible, the groin and in the axilla are often palpable and regular examination of these sites is required to appreciate the range of normality.
Movement against resistance makes a muscle belly more prominent; it will thus be more easily palpable and structures deep to it will become less prominent. A superficial artery is most easily palpated when it can be compressed on an adjacent bony surface. The pulps of two or more fingers are placed together along the line of the artery and the distal finger pressed onto the bone to compress the vessel. The proximal finger (or fingers) resting gently on the skin is then used for palpation. The heartbeat can usually be felt by placing the flat of the right hand on the left anterior chest wall. The flat of the hand will also demonstrate chest movements during respiration. Palpation of the abdomen allows a number of abdominal viscera to be felt.
If the middle finger of the right hand is tapped on a table top, first over the central unsupported area and then over one of its legs, the difference between the hollow and the firmer areas will be both heard and felt. If the palm of the left hand is now placed over the same two areas and the right middle finger is used to tap (staccato fashion) the dorsum of the middle phalanx of the left middle finger, the differences of sound and feel will be magnified. This principle is extended to clinical examination by the process of percussion. The palm of the left hand is placed over a body cavity or organ and tapping is carried out as already described. Air-filled organs such as the lungs and the gut sound more hollow than more solid organs such as the heart and liver. Tapping bony surfaces such as the clavicle and skull vault directly with the middle finger can be used to compare the two sides of the body.
Auscultation is the process of listening over the body. This was originally carried out by applying an ear directly over an area. Development of the stethoscope has simplified the manoeuvre and serves to conduct and localise underlying sounds. These sounds include the closing of heart valves, blood flow in some arteries and the movement of air in the trachea, lungs and gut. The bell of the stethoscope is small enough to give easy access to most areas of the body, but the diaphragm of the stethoscope is better for detecting high-pitched sounds.
Assessment of cranial nerve function includes examination of smell, vision, taste, balance and hearing. Pupillary reflexes are assessed by shining a light in the eye and by observing pupil size on alternating near and far vision. Somatic tactile sensation is assessed by the light touch of a finger or a piece of cotton wool; pain is assessed with a gently applied sterilised pin.
Two-point discrimination can be assessed with a blunt-pointed set of dividers. Appreciation of the two ends as separate points of contact ranges from 3–5 mm on the finger tips to 4–5 cm on the back.
Vibration sense is assessed with the footpiece of a vibrating clinical tuning fork and temperature by comparing the side of the examiner's finger with the cold prong of the tuning fork. In other sensory tests the subject closes his/her eyes while a digit is moved backwards and forwards to assess position sense, or the subject is asked to name figures or numbers which have been gently written out on a limb with a blunt instrument.
Motor function is assessed by muscle tone, power, coordination and reflexes, the latter being assessed by gently tapping a tendon with a tendon hammer. Muscle mass is compared visibly and by circumferential measurement, and abnormal movements noted. In the assessment of lower limb function, the subject is observed walking and standing on one and on both legs.
Assessment of joints is under the headings of look, feel, move, measure and X-ray, movements being active, passive and resisted. Initial observations provide information on the gait and posture, and detect pain, disability and deformity, such as malalignment and contractures. Compare the two sides of the body; it is helpful to examine the non-symptomatic side first when this is normal. The bones and soft tissues around the joint are palpated; resting the hand over a joint during movement may elicit a soft grating sensation know as crepitus due to irregularity of the bony surfaces. Crepitus is also present between the broken ends of a fractured bone but is painful to elicit and fractures can usually be recognised by local tenderness and the abnormal shape of a bone. Active movement is first carried out by the subject. This indicates any limitation of the range of movement, suggesting discomfort or disability. After this has been observed, and following discussion with the subject, the examiner undertakes passive movement. This may reveal rigidity or contracture of the muscles, and fixity or abnormal movement of the joints, due to bony or ligamentous abnormalities. Pain noted in active movement can be confirmed by gentle passive movement in the same plane, and may also be revealed in other directions. In resisted movement, the examiner exerts counter-pressure as individual muscles are contracted, in order to assess power, pain and discomfort.
The angles of passive and active movement are measured by eye or with a goniometer, and a tape measure is used to compare length and circumference of limbs, the latter being taken at appropriate distances from a bony prominence. The circumference may be affected by trauma, inflammation, tumour or muscle wasting. Although a tape measure should always be available to measure normal and abnormal anatomy, some indication of size can be quickly obtained by comparison with part of the examiner's hand: an adult male thumb is approximately 2.5 cm wide, the thumb to the metacarpophalangeal joint 7.5 cm, and the index finger to this joint 10 cm.
General examination
An examination of a subject in clinical practice commences with observation of general features, gaining an impression of the health of the individual and noting sex, age and physique. This part of the examination is based on examination of the head, neck, hands and feet and the shape of the body, without exposing the trunk. It is followed by regional examination of the subject from the head to the feet. This sequence partly follows the systematic pattern by which the examination is reported, but detailed examination of the nervous system is undertaken as a separate entity, so that sensory and motor function are compared throughout the body. It is important to develop a set routine for a complete examination, incorporating thoroughness and, later, speed of execution.
The general health of the subject is assessed by facies, colour, nutrition, hair distribution and shape. Observe normal and abnormal sexual features, such as muscle and fat distribution, and the features of ageing, such as change of stature and loss of skin elasticity. Obesity is noted and any lax skin indicating recent weight loss. General pallor is related to reduced circulating haemoglobin (anaemia) and is best estimated by gently pulling down the lower eyelid and, by so doing, everting it; the colour of the inside of the lid is then assessed. Yellow pigmentation due to raised circulating bilirubin (jaundice) is assessed by the degree of staining of the white sclera of the eyeball. In this general clinical examination, particular attention is given to the hands: the palms, the nails and the texture of the skin over the dorsum provide evidence of nutritional and other pathological disturbances.
Instruments of clinical examination (Figs 1.9-1.11)
The stethoscope, tape measure, cotton wool, sterile pin, torch, tendon hammer and tuning fork have already been referred to.

1.9 Instruments of clinical examination
(Disposable gloves are required for oral, rectal and vaginal examination)
1 Patellar hammer
2 Tuning fork
3 Stethoscope
4 Torch
5 Skin pencil
6 Tape measure
7 Cotton wool
8 Sterile needle
9 Red and white headed pins
10 Wooden spatula
11 Magnifying glass

1.10 Speculae and endoscopes
1 Rigid sigmoidoscope
2 Proctoscope
3 Vaginal speculum
4 Laryngeal mirror
5 Nasal speculum
6 Laryngoscope
7 Ophthalmoscope
8 Auroscope
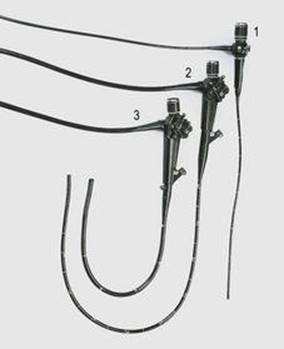
1.11 Fibreoptic endoscopes
1 Bronchoscope
2 Gastroscope
3 Flexible sigmoidoscope
Blood pressure measurement is a routine part of clinical examination. A bandage tied tightly around the upper arm will occlude the brachial artery. If the bell of the stethoscope is placed lightly over the artery distal to this point and the tie gradually released, a pulse is heard as the blood flow is restored. The point at which the sound appears equates to the systolic blood pressure and the point at which the noise suddenly becomes very faint before disappearing, equates to the diastolic blood pressure.
The instrument used to measure blood pressure, the sphygmomanometer, makes use of these principles. A broad, long band of material (the cuff) with an inflatable balloon in its base, is wrapped around the arm. The balloon is attached to a calibrated mercury manometer, so the pressure within it can be measured. After application, the balloon is blown up to a level above the systolic blood pressure, a stethoscope is applied over the brachial artery in the cubital fossa, and the pressure within the balloon slowly released, enabling systolic and diastolic pressures to be measured from the sounds, as already described.
Different cuff sizes are available to measure blood pressure in adults and children. A wider cuff is required for thigh compression, and a Doppler probe to detect the systolic blood pressure, i.e. the point of reappearance of flow when the cuff is deflated. In clinical practice, a number of devices are used to measure the reappearance of the blood pressure on release of the occlusion, together with automatic compression devices to record blood pressure at timed intervals.
A number of optical aids have been designed to examine the various recesses, cavities and hollow organs of the body. The ophthalmoscope allows the examination of the retina through the cornea and lens, and the auroscope is designed to view the tympanic membrane. A nasal speculum and a light source allow the examination of the anterior nasal cavities. Nasal endoscopes are used to examine the nasal cavities. The mouth is examined with the aid of a spatula, to depress the tongue, and a torch. A small, angled mirror mounted on a metal rod can be introduced into the oropharynx, without touching its walls, and be turned upwards or downwards to assess the posterior nares or the larynx. The curved lighted smooth metal blade of a laryngoscope allows direct viewing of the larynx, particularly in the anaesthetised patient when the instrument can be used gently to pull the tongue and jaw anteriorly to improve the view.
A large variety of other flexible fibreoptic instruments are used to view the interior of the body. A bronchoscope is used to examine the larynx, trachea and main bronchi. Longer and firmer instruments can be passed along the upper alimentary tract to observe the oesophagus, stomach, duodenum and sphincter of Oddi. The distal end of these instruments is moveable to allow the lumen to be identified and the instrument advanced under direct vision. The original bronchoscope and oesophagoscope were lighted, rigid, hollow metal tubes; these are still occasionally used if a wider exposure is required for specific operative procedures on a lesion.
The anal canal, lower rectum and vagina are examined with a gloved finger and through lighted metal tubes (proctoscope, sigmoidoscope, vaginal speculum). The lower alimentary tract can be examined from the anal canal to the ileocaecal valve with a colonoscope. The urethra and bladder can be visualised through flexible or rigid instruments identifying the ureteric orifices, which themselves can be entered by catheters and contrast medium introduced to outline the renal pelvis and ureter. Other fibreoptic instruments can be introduced through small incisions to examine body cavities such as the pleural cavity (thoracoscopy), mediastinum (mediastinoscopy), peritoneal cavity (peritonoscopy) and the interior of joints (arthroscopy).
Abnormal surface tissue can be sampled (biopsied) and submitted to subsequent pathological examination. A knowledge of the surface markings of the superficial and larger, deep, blood vessels allows the introduction of needles or cannulae to obtain blood samples, measure pressures or introduce radiological contrast medium, fluid requirements and drugs. Interventionists from various disciplines access the circulation, for procedures on the heart and vessels such as dilating stenosed heart valves and arteries.
Needles may be introduced into a hollow, cystic or solid organ or mass, to inject into them or to obtain fluid or solid biopsy samples. Sampling of deeper organs and masses is usually undertaken under ultrasound guidance. Knowledge of the position and distribution of peripheral nerves allows injection of local anaesthetic to relieve pain or to undertake pain-free operative procedures.
A surgeon requires to know the detailed topographical anatomy of each operation undertaken, but all clinicians should be aware of the common surgical incisions and the likely procedure that has been undertaken through an old operation scar.
Bony structures show up on conventional radiographs and these can be related to examination findings. Injection of radio-opaque material into the bloodstream, body cavities or hollow organs allows vessels, cavities and organs to be outlined. Scanning apparatus, such as ultrasound, computed tomography (CT) and magnetic resonance imaging (MRI), demonstrate normal and abnormal bone and soft tissues, supporting clinical findings. Spiral CT provides a three-dimensional image of structures; it can be rotated on screen to define their contours. Isotope scans measure radiation from isotopes passing through or accumulating in a specific region, indicating blood flow and metabolic activity.