Face (Figs 2.1–2.7) 10
Facial bones (Figs. 2.3, 2.4) 10
Facial muscles (Fig. 2.6) 12
Lateral aspect of the head (Figs 2.8–2.18) 12
Surgical incisions of the skull and parotid gland (Fig. 2.16) 14
Temporomandibular joint (Fig. 2.17) 15
Eye (Figs 2.19–2.21) 16
Nose (Fig. 2.22) 17
Oral cavity (Figs 2.23–2.27) 18
Ear (Fig. 2.28) 19
Face (Figs 2.1-2.7)
Facial bones (Figs. 2.3, 2.4)
The forehead is formed by the smooth convexity of the frontal bone. The inferior, curved borders of the bone, sharp medially and rounded laterally, form the superior margin of each orbit. The palpable supraorbital notch (or foramen) is sited at the junction of the medial and middle third of each margin; it transmits the supraorbital vessels and nerve, and the artery may be palpable. Medially, above the orbital margins, are the superciliary arches, which are more prominent in the adult male. The arches are united across the midline by a prominent ridge, the glabella; the depression beneath this is the nasion.

2.1 Anterior aspect of the face
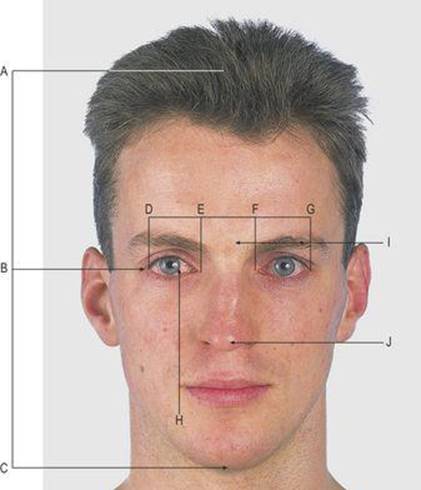
2.2 Facial alignment
A, B, C In the adult, the eyes are sited halfway between the vertex and the chin, whereas at birth they are at the junction of the middle and lower thirds
D, E, F, G The eyes are an eye width apart
H The angle of the mouth is in line with the medial border of the iris
I, J The tip of the ear is in line with the eyebrow and the glabella, and the lobule is in line with the tip of the nose
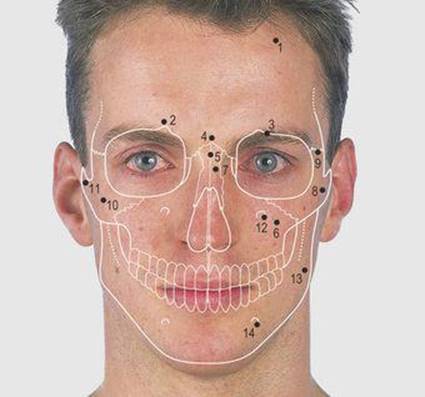
2.3 Anterior aspect of the face: bones
1 Frontal bone
2 Superciliary arch
3 Supraorbital notch
4 Glabella
5 Nasion
6 Maxilla
7 Nasal bone
8 Zygomatic bone
9 Frontozygomatic suture
10 Prominence of cheek
11 Zygomatic arch
12 Infraorbital foramen
13 Mandible
14 Mental foramen
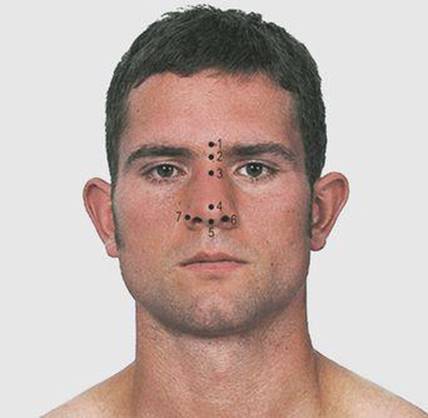
2.4 Anterior aspect of the face: palpable structures
1 Supraorbital artery
2 Superficial temporal artery
3 Facial artery
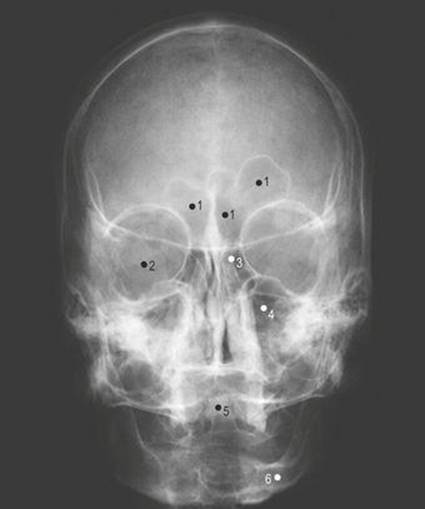
2.5 Skull radiograph: anterior view
1 Frontal air sinus
2 Orbit
3 Ethmoidal air sinus
4 Maxillary air sinus
5 Odontoid process of axis vertebra
6 Ramus of mandible
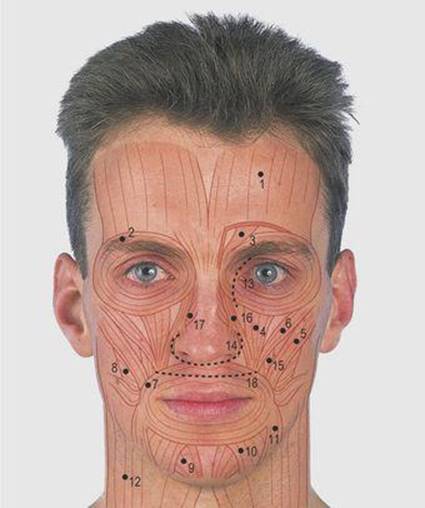
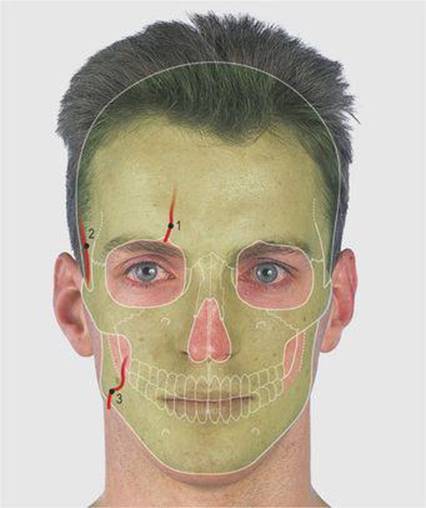
2.6 Anterior aspect of the face: muscles and incisions
1 Frontalis
2 Orbicularis oculi
3 Corrugator
4 Levator labii superioris
5 Zygomaticus major
6 Zygomaticus minor
7 Orbicularis oris
8 Buccinator
9 Mentalis
10 Depressor labii inferioris
11 Depressor anguli oris
12 Platysma
13 Medial orbital incision
14 Infranasal incision
15 Levator anguli oris
16 Levator labii superioris aleque nasi
17 Nales
18 Sublabial incision
2.7 Muscles are used to produce various facial expressions
The frontal bone articulates with the frontal process of the maxillary bone along the medial aspect of the orbit and, together with the lacrimal bone, houses the lacrimal drainage apparatus just within the orbit (p. 16).
The two nasal bones articulate with each other, with the frontal bone and with the frontal process of the maxillary bone. The internasal and frontonasal sutures meet at the nasion. The lateral border of the orbit is formed by the frontal and zygomatic bones and the frontozygomatic suture can be palpated along this margin. The zygomatic bone forms the prominence of the cheek and, with the maxillary bone, the inferior margin of the orbit. It has a posterior process which, with the zygomatic process of the temporal bone, forms the zygomatic arch (Fig. 2.17).
The inferior alveolar margin of each maxilla carries the sockets for the teeth and the bone houses the maxillary air sinus. It also forms parts of the lateral wall of the nose and the hard palate (Fig. 2.25). The infraorbital foramen in the maxilla is in line with the supraorbital notch; it is 1cm below the inferior orbital margin and transmits the infraorbital nerve.
The mandible contains the sockets for the lower teeth. The mental foramen transmits the mental vessels. At birth it is near the inferior margin, but in the adult it is midway between the alveolar and inferior margin of the mandible; it becomes nearer the upper margin with tooth loss and bone resorption.
Facial muscles (Fig. 2.6)
The skin around the face is thin, vascular, sensitive and, in the male, hairy with abundant sweat and sebaceous glands. There is a variable amount of fat but no deep fascia. The skin over the nose is adherent to the nasal cartilages but not to the nasal, frontal or maxillary bones. The two nasal cavities are separated by the midline nasal septum and open anteriorly at the anterior nares. Examination of these openings using a torch reveals the wider vestibule within the expanded ala and usually the anterior end of the inferior turbinate bone. The muscles of facial expression are arranged as sphincters and dilators around the orbit, nose and mouth (Fig. 2.6). Their actions are linked with the mood of an individual and they are innervated by the facial (7th cranial) nerve (Fig. 2.13). The frontalis muscle blends with the occipital aponeurosis, and the platysma with the subcutaneous tissue of the neck and upper thorax.
In deep cuts of the face, sutures are placed in the muscles as well as the skin. Incisions follow skin creases, such as around the side and base of the nose and along the medial aspect of the orbit, or are mucosal within a cavity such as the mouth. The three incisions shown in Figure 2.6 can all be used to gain access to the sphenoidal air sinus and the pituitary gland in spite of the depth of the latter structure. A microscope, a strong light and long fine instruments are used.
Lateral aspect of the head (Figs 2.8-2.18)
The lateral aspect of the skull vault is formed of the frontal, parietal and occipital bones; the first two meet in the midline at the bregma and the last two at the lambda (Fig. 2.9). These sites are unfused at birth and are known respectively as the anterior and posterior fontanelles. The triangular-shaped posterior fontanelle (lambda) closes 2–3 months after birth and the diamond-shaped anterior (bregma) at approximately 18 months. Four bones (frontal, parietal, greater wing of sphenoid and the squamous temporal bone) meet in H-shaped fashion in the temporal region, overlying the middle meningeal artery; this point is known as the pterion. A burr hole is placed through the skull at the pterion to evacuate the blood clot when there is uncontrolled haemorrhage from a damaged middle meningeal artery, as in a skull fracture. (The pterion is also called the sylvian point because it overlies the stem of the sylvian, or lateral, cerebral sulcus.)

2.8 Lateral aspect of the head
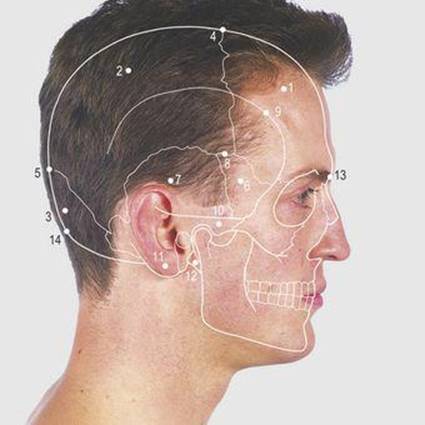
2.9 Lateral aspect of the head: bones
1 Frontal
2 Parietal
3 Occipital
4 Bregma (anterior fontanelle)
5 Lambda (posterior fontanelle)
6 Greater wing of sphenoid
7 Squamous temporal
8 Pterion
9 Temporal line
10 Zygomatic arch
11 Mastoid process
12 Styloid process
13 Glabella
14 Inion (external occipital protuberance)
2.10 Lateral aspect of head: palpable structures
1 Superficial temporal artery
2 Facial artery
3 Maxillary artery
4 Tip of transverse process of atlas vertebra

2.11 Skull radiograph: lateral view
1 Mandible
2 Frontal bone
3 Parietal bone
4 External occipital protuberance
5 Spine of second cervical vertebra
6 Sphenoid air sinus
7 External acoustic meatus
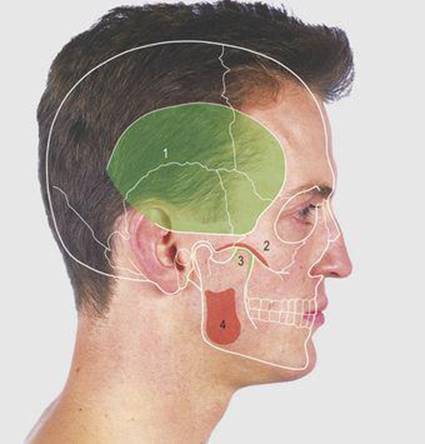
2.12 Lateral aspect of the head: muscle attachments
1 and 3 Temporalis
2 and 4 Masseter
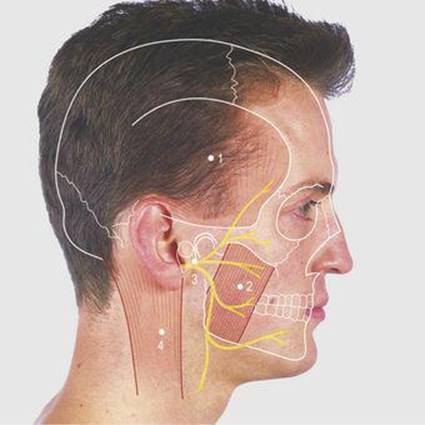
2.13 Lateral aspect of the head: soft tissues
1 Temporalis muscle
2 Masseter muscle
3 Divisions of the facial nerve
4 Sternocleidomastoid muscle
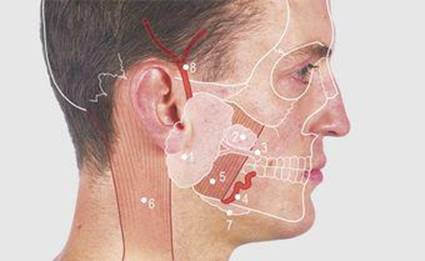
2.14 Parotid gland
1 Parotid gland
2 Accessory lobe
3 Parotid duct
4 Facial artery
5 Masseter muscle
6 Sternocleidomastoid muscle
7 Submandibular gland
8 Superficial temporal artery
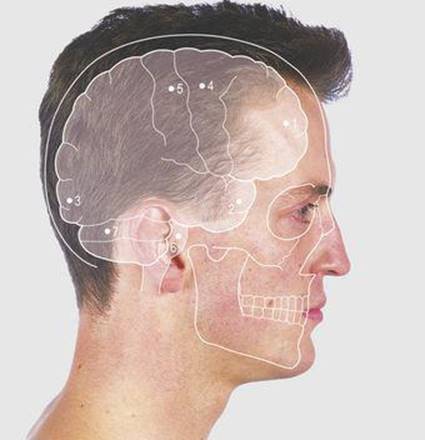
2.15 Lateral aspect of the skull: the surface markings of the brain
1 Frontal pole
2 Temporal pole
3 Occipital pole
4 Precentral gyrus
5 Postcentral gyrus
6 Pons
7 Cerebellum
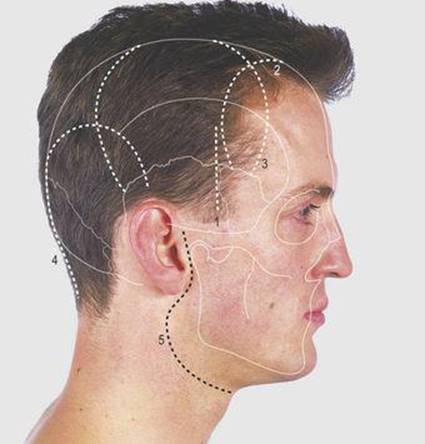
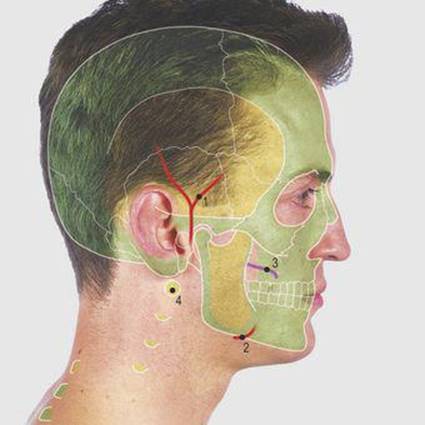
2.16 Surgical incisions of the skull and parotid gland
1 Surgical approach to the pterion
2–4 Frontal, temporoparietal and occipital craniotomy incisions
5 Incision for surgical approach to the parotid gland
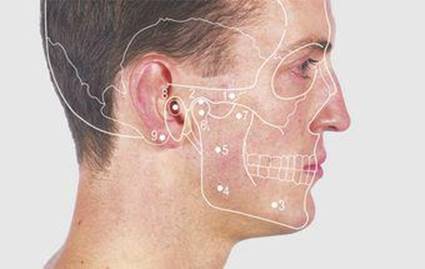
2.17 Temporomandibular joint
1 Zygomatic arch
2 Temporomandibular joint
3 Body of mandible
4 Angle of mandible
5 Ramus of mandible
6 Condyle of mandible
7 Coronoid process of mandible
8 External acoustic meatus
9 Mastoid process
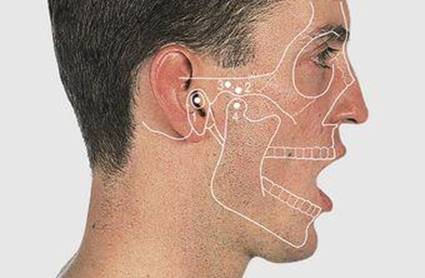
2.18 Opening the jaw
1 External acoustic meatus
2 Articular tubercle
3 Zygomatic arch
4 Condyle of mandible
The processes of the frontal and zygomatic bones, forming the lateral border of the orbit, also form the anterior border of the temporal fossa. The palpable temporal line gives attachment to the temporalis fascia. The temporalis muscle is attached below this line and can be felt when biting (Fig. 2.13); it is supplied by the mandibular nerve. The temporalis fascia is attached inferiorly to the zygomatic arch which is formed by the temporal process of the zygomatic bone and the zygomatic process of the squamous temporal bone.
The masseter muscle passes from the outer posterior inferior aspect of the mandible to the inferior margin of the zygomatic arch. Its shape is accentuated by clenching the teeth, and the facial artery is palpable crossing the inferior margin of the mandible just in front of the anterior border of the muscle. The masseter is supplied by the mandibular nerve.
The parotid gland is wedged between the ramus of the mandible anteriorly, with the masseter superficial and medial pterygoid muscles deep to the bone (Fig. 2.14). Posteriorly is the mastoid process, with the sternocleidomastoid superficial and the posterior belly of the digastric muscle's deep to the process. Medially lies the styloid process (Fig. 2.9) with its attached and related structures; superiorly, the cartilaginous external acoustic meatus and the temporomandibular joint. The accessory lobe of the gland lies superficial to the masseter muscle and the parotid duct can be felt passing anteriorly over the contracted muscle. The duct then turns medially to pierce the buccinator muscle and open into the vestibule of the mouth opposite the crown of the second upper molar tooth. Swellings in the lower pole of the parotid gland can present just posterior to the angle of the mandible and may be mistaken for swellings originating in the submandibular region.
Surgical incisions of the skull and parotid gland (Fig. 2.16)
Emergency surgery is sometimes required when fractures across the temporal fossa damage the middle meningeal artery. Blood collects between the bone and the dura and needs to be relieved by removal of some overlying bone. The vertical incision is through the skin and temporalis fascia and muscle. Bone over the pterion is removed, centred 3.5cm posterior and 1.5cm above the frontozygomatic suture. Access to the brain can be gained either through a single bony hole, allowing biopsy of the underlying brain, or by raising a flap of bone (craniotomy). The incisions marked indicate common sites for craniotomy, allowing access to different cortical regions.
The surgical approach to the parotid gland follows the anterior border of the auricle and then passes along the upper anterior border of the sternocleidomastoid muscle. The skin and superficial tissues are dissected forward off the gland. The facial nerve passes through the parotid gland but the superficial portion of the gland and its duct can be excised without damaging the nerve, provided it is identified and preserved and the disease for which the operation is being undertaken does not involve the nerve. The nerve can be identified by a nerve stimulator, observing contraction of the appropriate facial muscles.
Temporomandibular joint (Fig. 2.17)
The inferoposterior margin of the zygomatic arch forms the upper articulation for the temporomandibular joint. The body, the angle and the ramus of the mandible are palpable. The condyle of the mandible is the inferior articulation of the temporomandibular joint; it is not easily palpable with the jaw closed, because of a prominent lateral ligament, but it becomes so when the jaw is opened and the condyle moves forward on the articular eminence of the joint (Fig. 2.18). The joint is divided into superior and inferior compartments by a fibrocartilaginous disc that is attached around its perimeter to the joint capsule. The coronoid process of the mandible gives attachment to the temporalis muscle but it lies deep to the zygomatic arch and is impalpable. Movement of the mandible involves both temporomandibular joints. Similar movement occurs in both joints in descent, elevation, protrusion and retraction, but contrary movement is present in the two joints during rotation and grinding. The most powerful movement is elevation, as in the bite (Fig. 2.12); it is produced by the temporalis, masseter and medial pterygoid muscles, while the medial and lateral pterygoid muscles act together in protrusion. Abnormalities of dental occlusion may give rise to pain and stimulate remodelling of the joint articular surfaces. Dislocation of the temporomandibular joints can only take place in an anterior direction, this occurring when trauma is applied to the open mouth.
The external acoustic meatus opens below the posterior end of the zygomatic arch. The palpable mastoid process projects downwards behind the meatus. The superficial temporal artery (Fig. 2.10) is palpable as it crosses the zygomatic arch just in front of the external acoustic meatus and its anterior and posterior branches can be traced by palpation over the temporal region.
Eye (Figs 2.19-2.21)
The orbit is limited anteriorly by the upper and, smaller, lower eyelids, which are united medially and laterally, limiting the palpebral fissure (Fig. 2.19). Each lid contains a dense fibrous tarsal plate and numerous modified sebaceous (tarsal) glands opening onto the margin behind the eyelashes; the latter are arranged in two or three irregular rows. Medially the eyelids enclose a pinkish elevation, the lacrimal caruncle. An elevation on the medial end of each lid, the lacrimal papilla, has a punctum through which tears are drained into the lacrimal apparatus (Fig. 2.20). The conjunctiva lining the inner aspect of each eyelid is continuous with that over the front of the eyeball. Closure of the eyelids thus produces a sealed cavity into which lacrimal fluid secreted by the lacrimal gland can circulate, lubricating the conjunctiva and passing medially to drain into the lacrimal apparatus through the lacrimal canaliculi. The eyelids are closed by the orbicularis oculi muscle and the upper lid is raised by levator palpebrae superioris.
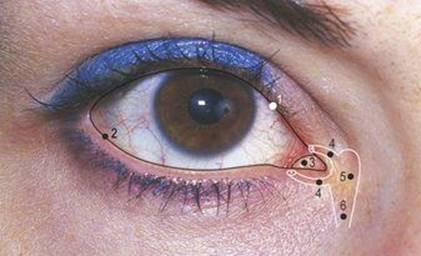
2.19 The eye
1 Upper eyelid
2 Lower eyelid The opening between the upper and lower lids is the palpebral fissure
3 Lacrimal caruncle
4 Lacrimal canaliculi
5 Lacrimal sac
6 Nasolacrimal duct

2.20 The eye
The lower lid has been everted to show:
1 Lacrimal papilla
2 Lacrimal punctum
3 Conjunctival fornix
4 Plica semilunaris
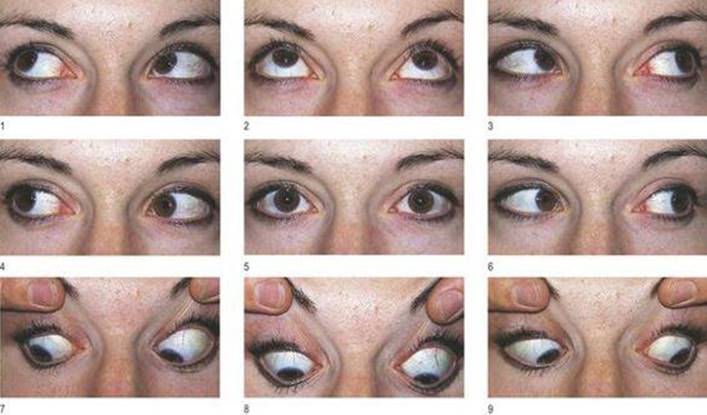
2.21 The nine cardinal positions of gaze
The action of the lateral rectus muscle is seen in the right eye in position 4. The superior oblique muscle, acting independently, depresses the eyeball and is a weak abductor. However, the line of the oblique portion of the muscle is nearest the visual axis in adduction. Thus the maximum depressor effect of the right superior oblique muscle is in position 9. When the right eye is abducted, depression (position 7) is produced primarily by the inferior rectus muscle and the pull of the oblique portion of the superior oblique is at right angles to the visual axis. In this position, the prime action of the superior oblique muscle is in torsion, pulling the top of the eyeball towards the nose.
The eyeball is embedded in orbital fat. The suspensory ligaments supporting the globe are attached to the medial and lateral margins of the orbit, and the position of the eye is controlled by the extraocular muscles. The anterior segment of each eye opens to the exterior through the palpebral fissure between the eyelids. It is lined by conjunctiva and lubricated by the secretions of the lacrimal gland, passing into the conjuctival sac through approximately 12 ducts under the lateral aspect of the upper lid. Drainage of fluid through the lacrimal puncta and the nasolacrimal apparatus into the nose is facilitated by the muscular action of blinking.
The orbit can be entered for surgery on the eye muscles and abnormalities within the orbital cavity by incision of the conjunctiva along the upper or lower margin of the conjunctival sac (conjunctival fornices).
The extraocular muscles contract and relax in a coordinated fashion, enabling the two eyes to focus on and to follow an object. Looking to the left involves the left lateral rectus muscle, supplied by the abducent (6th cranial) nerve; looking down and to the left involves the left superior oblique muscle supplied by the trochlear (4th cranial) nerve. The other extraocular muscles are supplied by the oculomotor (3rd cranial) nerve.
Abnormalities of gaze may indicate intracranial damage to these cranial nerves or their nuclei (Fig. 2.21).
Touching the cornea with a whisk of cotton wool produces a blink (corneal reflex); shining a bright light into the pupil produces reflex pupillary contraction of both the stimulated and the contralateral eye (pupillary reflex and consensual response). The pupils also contract when changing focus from a distant to a near object (accommodation reflex).
Nose (Fig. 2.22)
The pyramidal-shaped external nose has two inferior elipsoid apertures – the nostrils, or external nares, situated behind the tip and separated by the nasal septum. The nose is expanded lateral to each nostril as the ala nasi (Fig. 2.22). Each nostril leads into a nasal cavity that lies alongside the nasal septum. The supporting framework of the nose is made up of the two nasal bones superiorly, and surrounded by the frontal process and body of each maxilla (Fig. 2.3, p.10). The remaining framework is made up of a series of nasal cartilages. The nose is prone to injury, and although the cartilage usually recoils to its normal position, fracture of the nasal bones may be accompanied by deformity, sometimes requiring refashioning.
2.22 The nose
1 Glabella
2 Nasion
3 Bridge of nose
4 Tip of nose
5 Nasal septum
6 External nares
7 Ala nasi
Oral cavity (Figs 2.23-2.27)
The oral cavity is the first part of the alimentary tract and extends from the lips to the isthmus of the fauces. It contains the tongue and alveolar arches with the gums and teeth, and receives the openings of the salivary glands. Its mucous membrane starts on the oral aspect of the lips at the red margin. The alveolar arches and teeth divide the cavity into an outer vestibule and an inner mouth cavity proper. The vestibule is a slit-like cavity when the lips and teeth are opposed, communicating with the mouth cavity behind the molar teeth (Fig. 2.23). The parotid duct opens into the vestibule just above the crown of the second upper molar tooth (Fig. 2.23). In the mouth cavity proper, the roof is formed by the hard and soft palates, the former being formed by processes from the maxilla and palatine bones. The soft palate ends posteriorly as a free margin, with a centrally projecting uvula (Figs 2.24, 2.26).
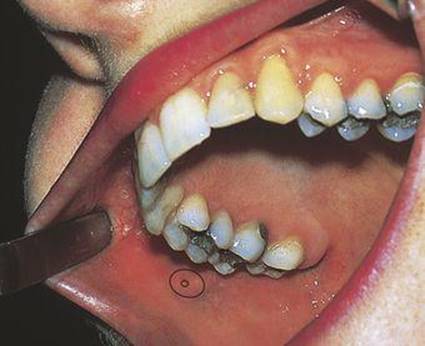
2.23 The vestibule
The opening of the parotid duct is shown opposite the crown of the second upper molar tooth.
2.24 Soft palate and uvula at rest
1 Anterior pillar of the fauces
2 Soft palate
3 Uvula
4 Circumvallate papillae at the junction of the anterior two-thirds and posterior third of the tongue
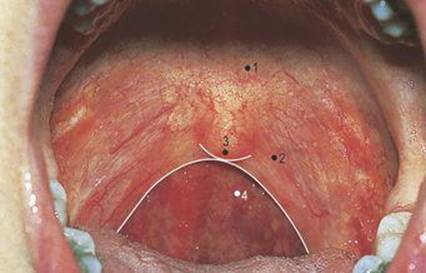
2.25 Soft palate and uvula raised
1 Hard palate
2 Soft palate
3 Uvula
4 Oropharynx

2.26 Palatine tonsil
1 Anterior arch of the fauces
2 Posterior arch of the fauces
3 Tonsillar fossa
4 Upper border of the palatine tonsil
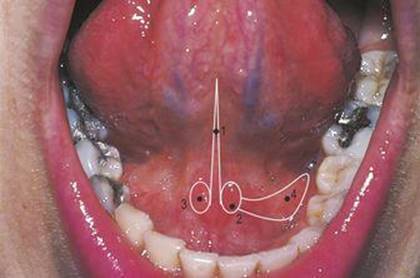
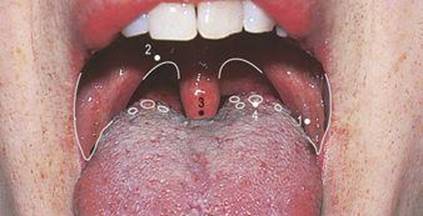
2.27 Under surface of the tongue
1 Frenulum
2 Submandibular papillae
3 Opening of submandibular duct
4 Sublingual fold
The posterior opening of the oral cavity is the faucial isthmus, which is bounded laterally by the palatoglossal fold (the anterior arch of the fauces), superiorly by the soft palate and inferiorly by the tongue (Figs 2.24, 2.26). The palatine tonsil lies behind the fold, between it and the palatopharyngeal fold (the posterior arch of the fauces) (Fig. 2.26). The palate is raised by asking the subject to say ‘ah’ (Fig. 2.25).
The tongue lies in the floor of the mouth. A V-shaped sulcus terminalis, with the point posteriorly, divides the anterior two-thirds from the posterior third which has different embryological origins and nerve supply. A midline fold of mucous membrane, the frenulum, connects the undersurface of the tongue to the floor of the mouth. On each side of this is a sublingual papilla onto which opens the submandibular duct (Fig. 2.27). Passing backwards from the papilla on each side sublingual folds of mucous membrane overlie the sublingual glands.
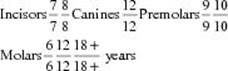
Average eruption time of the teeth of each half of the upper and lower jaws:
Deciduous teeth
![]()
Permanent teeth
The teeth of the upper jaw are innervated by the posterior and superior alveolar nerves; the upper gums, on the labial surface, by the infraorbital and posterior alveolar nerves and, on the lingual surface, by the nasopalatine and greater palatine nerves. Local anaesthesia is usually by injection around the tooth. The lower teeth are supplied by the inferior alveolar nerve, the labial surface of the gums by the mental and buccal nerves, and the lingual surface by the lingual nerve. The incisors are bilaterally innervated and are anaesthetised by injection of local anaesthetic adjacent to the teeth. Injection around the inferior alveolar nerve as it passes to enter its canal and the adjacent lingual nerve anaesthetises the lower gums, the teeth and the tongue.
Ear (Fig. 2.28)
The auricle is a single irregularly shaped piece of elastic cartilage covered by firmly adherent skin. It has a dependent lobule (which lacks cartilage) and an anterior tragus overlapping the opening of the external acoustic meatus. Other parts of the auricle are labelled in Figure 2.28. Three vestigial muscles attached superiorly to the auricle are supplied by the facial nerve. The external acoustic meatus is mainly cartilaginous laterally and bony medially. The tympanic plate of the temporal bone forms the anterior and inferior bony skeleton and the squamous temporal bone, the roof and upper posterior wall. The meatus is approximately 4cm long and ends medially at the tympanic membrane. It has numerous ceruminous glands in its cutaneous lining and is innervated anteriorly by the auriculotemporal nerve and posteriorly by the vagus (10th cranial) nerve.

2.28 The ear
1 Helix
2 Crus of helix
3 Auricular tubercle
4 Antihelix
5 Crura of antihelix
6 Triangular fossa
7 Tragus
8 Antitragus
9 Intertragic incisure
10 Lobule
11 and 12 Upper and lower parts of concha
13 Arrow leading to external acoustic meatus
The vibration of the tympanic membrane may be inhibited by an excess of wax or by inflammatory changes in the meatus or the middle ear. Inflammation is accompanied by pain and a purulent discharge. Discharge from the meatus is to the exterior. Pus in the middle ear is discharged through the eustachian tube to the nasopharynx, but if this exit is blocked, pus may perforate and discharge through the tympanic membrane.