Anterior chest wall (Figs 4.1–4.6) 32
Posterior thorax (Fig. 4.7), pleura and lungs (Figs 4.8, 4.9) 34
Pleura and lungs (Figs 4.8, 4.9)
34
Anterior thorax, heart and great vessels (Figs 4.10–4.12) 35
Thoracic incisions and access points (Fig. 4.13) 37
Lateral chest wall, breast and axilla (Figs 4.14–4.17) 37
Anterior chest wall (Figs 4.1-4.6)
The chest extends from the clavicles above to the inferior costal margin below. It is formed of the ribs and costal cartilages, the sternum and associated muscles; the two sides of the chest are usually symmetrical. The rate, depth and character of respiration can be observed, as can the apex beat of the heart on the left side. The midline sternum is made up of the manubrium, the body and the xiphisternum from above downwards (Fig 4.2). The suprasternal notch on the superior aspect of the manubrium is palpable. The manubrium and body are also palpable throughout their length and they are united by a secondary cartilaginous joint forming the sternal angle (the angle of Louis). The angle is at the level of the lower border of the fourth thoracic vertebral body. It forms an important landmark for the description of structures inside the chest. Ribs are counted from this site, as it is consistently palpable: the second costal cartilage articulates on each side of the manubriosternal joint. The xiphisternum is covered by the rectus abdominis muscles and is less easily palpable. It is of variable length and when long, and suddenly noted by a subject, may be thought to be abnormal. The xiphisternal joint is at the level of the ninth thoracic vertebral body.
4.1 Anterior chest wall
4.2 Anterior chest wall: bones
1 Clavicle
2 Suprasternal notch
3 Manubrium
4 Sternoclavicular joint
5 Body of sternum
6 Xiphisternum
7 Coracoid process
8 True ribs (1–7)
9 False ribs (8–10)
10 Costal cartilages
11 Costal margin
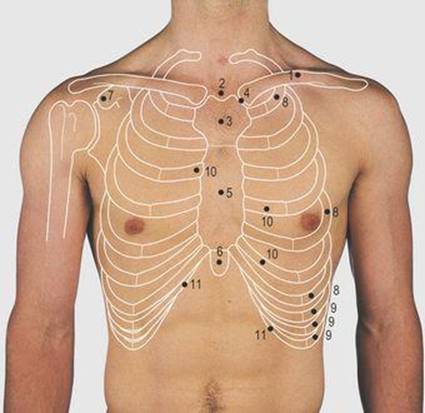
4.3 Anterior chest wall: palpable structures
1 Clavicle
2 Coracoid process of scapula
3 Manubrium sterni
4 Manubriosternal joint (angle of Louis)
5 Second costal cartilage
6 Body of sternum
7 Xiphisternum
8 Fifth, 6th and 7th costal cartilage (true ribs)
9 Eighth, 9th and 10th (false) ribs

4.4 Chest radiograph: anterior view
1 Clavicle
2 Ribs
3 Left dome of diaphragm
4 Right costophrenic angle
5 Right border of heart
6 Left border of heart
7 Pulmonary conus
8 Aortic knuckle
4.5 Anterior chest wall: muscle attachments
1 and 2 Pectoralis major
3 and 8 Pectoralis minor
4 Coracobrachialis
5 Short head of biceps
6 Deltoid
7 Serratus anterior
9 External oblique
10 Rectus abdominis
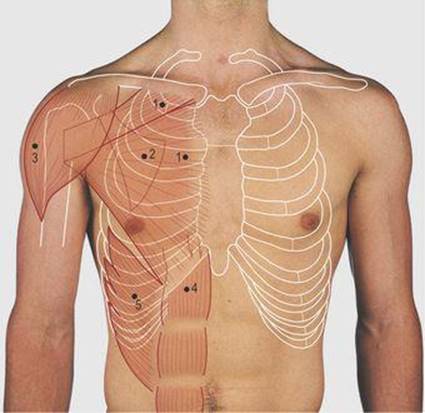
4.6 Anterior chest wall: muscles
1 Pectoralis major
2 Pectoralis minor (deep to 1)
3 Deltoid
4 Rectus abdominis
5 External oblique
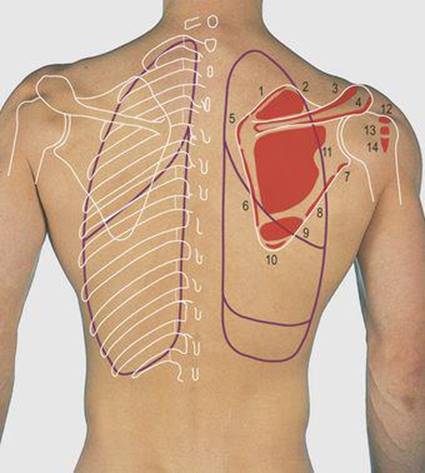
4.7 Posterior chest wall: muscle attachments
1 Letvator scapulae
2 and 12 Supraspinatus
3 Trapezius
4 Deltoid
5 Rhomboideus minor
6 Rhomboideus major
7 Long head of triceps
8 and 14 Teres minor
9 Teres major
10 Latissimus dorsi
11 and 13 Infraspinatus
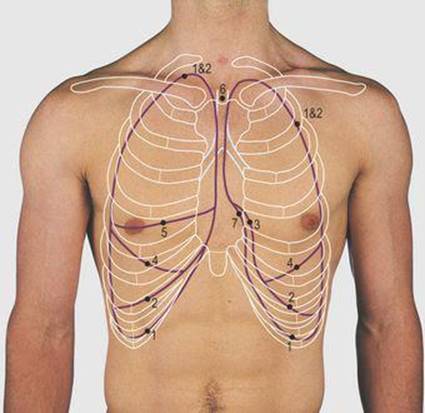
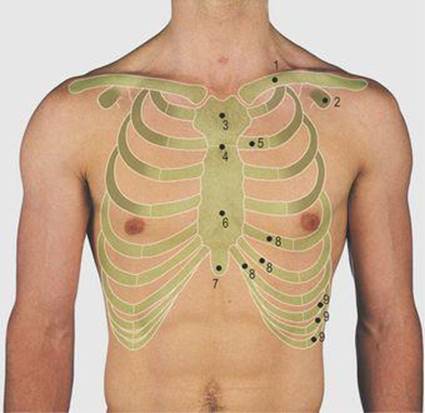
4.8 Surface markings of the lungs and pleura
1 Pleural markings
2 Lung markings
3 Cardiac notch
4 Oblique fissure
5 Horizontal fissure
6 Trachea
7 Mediastinal pleural recess
The rib cage is made up of 12 pairs of ribs, each having a posterolateral bony and an anterior costal cartilaginous component (Fig 4.2). In a thin male subject, many ribs are visible but they may be obscured by overlying muscle, fat or breast tissue. These structures can also make it difficult to count ribs by palpation. The first rib is not easily palpated, being deep to the fibres of the pectoralis major muscle and the clavicle. The second is consistently palpable at its cartilaginous articulation with the manubriosternal junction. The upper seven (true) ribs articulate directly with the sternum via their costal cartilages, whereas the eighth to 10th (false) ribs articulate via their costal cartilages with the cartilage of the rib above. The 11th and 12th (floating) ribs are considered in Figure 4.9 (p. 35). The lower costal margin is formed by the lower six ribs and their costal cartilages. The number of the ribs and intercostal spaces are used when describing normal and abnormal findings of the chest wall or thoracic cavity. The intercostal spaces are filled by the intercostal muscles, attached to the adjacent ribs.
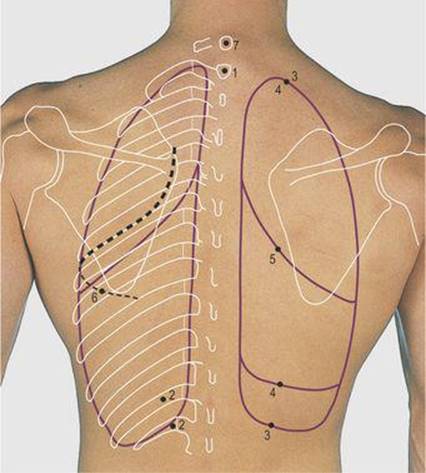
4.9 Posterior chest wall: ribs, lungs and pleura
1 Spine of first thoracic vertebra
2 Floating ribs (11 and 12)
3 Pleural markings
4 Lung markings
5 Oblique fissure
6 Posterolateral thoracotomy incision
7 Vertebra prominens
The clavicle is palpable throughout its length; it articulates medially at the sternoclavicular joint. Like the temporomandibular joint, it has a fibrocartilaginous covering of its articular surfaces and contains a fibrocartilaginous disc. The pectoralis major muscle is attached medially to the clavicle and upper five to seven costal cartilages, their related half of the sternum, and from the sheath of the rectus abdominis (Fig 4.6). Its fibres pass laterally to the lateral lip of the bicipital groove of the humerus and form the bulk of the anterior axillary fold (Fig 4.14, p. 38). The pectoralis minor muscle is overlapped by the pectoralis major, but its tendon may be palpable high in the anterior axillary wall as it passes to the coracoid process. The coracoid process can be felt by deep palpation 1cm below the clavicle under the medial anterior fibres of the deltoid muscle.
The deltoid muscle forms the rounded contour of the shoulder overlapping the shoulder joint. The muscles of the abdominal wall gain a wide attachment to the lower ribs and costal cartilages and are considered in Figure 5.4 (p. 43).
Severe injury to the chest wall can fracture the ribs. Although this is a painful condition, bony union is usually uncomplicated. However, the fractured bone ends may damage the underlying lung, producing leakage of air into the pleural cavity (pneumothorax), or lacerate other adjacent viscera, notably the liver and spleen.
Posterior thorax (Fig. 4.7), pleura and lungs (Figs 4.8, 4.9)
The lower three cervical, and all the thoracic, vertebral spines are palpable in the midline. The spine and acromion of the scapula are subcutaneous and its upper, lower and medial angles can be observed and palpated during arm movements. In the anatomical position, the scapula overlies the second to seventh ribs on the posterolateral aspect of the chest wall. Laterally it articulates with the clavicle and humerus but has no medial bony attachment, being free to move over the chest wall in movements of the upper limb (Fig. 7.16, p. 70). Much of the rib cage is impalpable posteriorly, being covered by powerful erector spinae muscles alongside the midline and the scapula and its muscle attachments more laterally. The 11th and 12th (floating) ribs articulate with their respective vertebrae but are free laterally and these ends can be palpated and this mobility confirmed.
The trapezius and latissimus dorsi muscles have attachments to the trunk. Their prime function is in movement of the shoulder girdle; they are considered in Figure 7.16 (p. 70). The deltoid muscle forms the rounded contour of the shoulder, gaining attachment from the clavicle and the scapula (Fig. 7.10, p. 67).
Pleura and lungs (Figs 4.8, 4.9)
Each pleural cavity extends superiorly 3 cm above the middle of the medial third of the clavicle and the possibility of damage in surgical procedures in the neck is considered in Figure 3.17 (p. 28). The anterior border of the pleural cavity reaches the midline at the sternal angle. The left moves away from the midline at the fourth costal cartilage, the right at the sixth costal cartilage and both cross the midclavicular line at the eighth costal cartilage, the midaxillary line at the 10th cartilage and pass along the line of the 12th rib posteriorly (to be remembered by the even numbers). These markings indicate the extent of the pleura around the outer chest wall. The diaphragm bulges up into each pleural cavity from below, reaching as high as the fourth intercostal space on the right side and the fifth on the left. The cardiac notch on the left side, at the fourth costal cartilage, is produced by the heart which bulges into the medial surface of both cavities but more markedly on the left.
The lung markings coincide with those of the pleura, except inferiorly, where they do not extend down into the lateral recesses and are approximately two rib spaces higher. The oblique fissure of each lung, separating its upper and lower lobes, follows a line from the third thoracic vertebra to the sixth costochondral junction. The horizontal fissure, dividing the right upper and middle lobes, follows a horizontal line from the oblique fissure to the fourth right costal cartilage. The position of the trachea in the neck is always identified when examining the lungs and pleural cavities. It should lie in the midline deep to the sternal notch and a finger passes into the slight hollow on either side of it. The trachea divides at the level of the sternal angle.
Respiratory movements can be magnified by placing the flat of each hand on the chest wall with the thumbs pointing towards each other near the midline. The hands are separated and the ribs are more horizontally placed in inspiration than in expiration. Reverberation felt with the flat of the hand over the chest wall when a subject talks is known as tactile vocal fremitus. This is accentuated in certain lung diseases. The lungs are resonant to percussion, as can be demonstrated over the clavicles, the upper chest and the axillary regions. When percussing from the left axilla towards the midline, a duller sound is heard and felt as the left border of the heart is encountered. The right border of the heart usually lies near the sternum and is not easily detected in the normal person. It is generally easier to detect borders by percussion from resonant to dull. Percussion downwards from the clavicle on the right side demonstrates the dull sound produced by the upper border of the liver at about the fourth intercostal space.
If the bell of a stethoscope is pressed onto the upper chest in the midaxillary line, air is heard to enter the lungs in inspiration, the noise extending slightly into the beginning of expiration. The sound stops during the remainder of expiration.
This normal pattern is known as vesicular breathing. If the stethoscope is placed over the larynx, noise will be heard during both inspiration and expiration with a break in-between. This is known as bronchial breathing. The latter pattern may also occur over the peripheral area of the chest in certain lung diseases. If the patient speaks during auscultation the sound is transmitted to the chest wall; this is known as vocal resonance and its character may be altered by lung disease. In disease there may also be added noise to the respiratory pattern. Inflammation of the lung (pneumonia) fills the alveoli with purulent exudate, reducing oxygen transfer and producing dyspnoea (breathlessness). The breath sounds in the consolidated lung become more prominent. The sounds are reduced if a part of the lung collapses (atelectasis), or when fluid (effusion) or air (pneumothorax) collects in the pleural cavity.
Anterior thorax, heart and great vessels (Figs 4.10-4.12)
The thoracic cavity can be divided into a central (mediastinal) region and, on each side, a pleural cavity containing a lung. The mediastinum is divided for descriptive purposes into superior, above a horizontal plane joining the sternal angle to the lower part of the body of the fourth thoracic vertebra, and, below this line, into a central part containing the heart, and the anterior and posterior mediastinum, in front of and behind the heart. The apex of the heart is usually in the left midclavicular line in the fifth intercostal space (Fig. 4.10). The inferior (‘acute’) border passes horizontally from this point across the midline and the right border bulges slightly laterally along the right border of the sternum. The left (‘obtuse’) border curves from the apex upwards and medially to the sternal end of the second left intercostal space. Figure 4.10 indicates the cardiac chambers, sulci and great vessel roots that constitute these borders. The surface markings of the valves indicate the atrioventricular junction and the origin of the aorta and pulmonary trunk (Fig. 4.11). The aortic arch, curving posteriorly and to the left, is sited in the superior mediastinum.
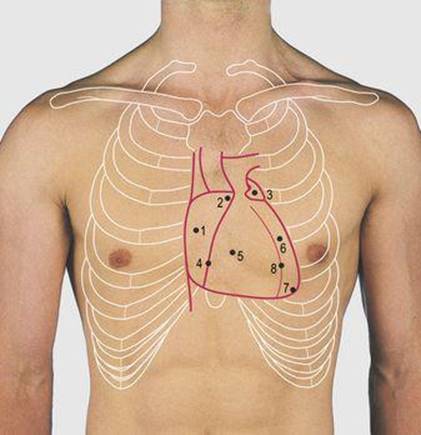
4.10 Surface markings of the chambers of the heart
1 Right atrium
2 Right auricular appendage
3 Left auricular appendage
4 Anterior atrioventricular (coronary) sulcus
5 Right ventricle
6 Left ventricle
7 Apex of heart
8 Anterior interventricular sulcus
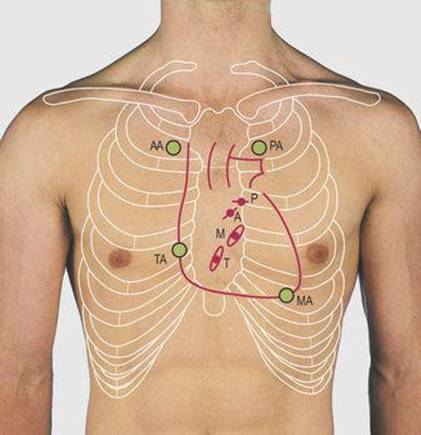
4.11 Surface markings of the cardiac valves and their optimal sites for auscultation
T Tricuspid
P Pulmonary
M Mitral
A Aortic
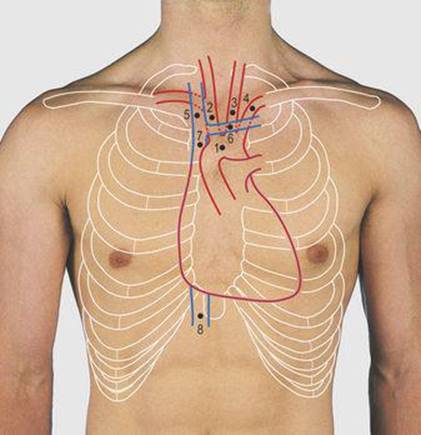
4.12 Surface markings of the great vessels of the superior mediastinum
1 Aortic arch
2 Innominate (brachiocephalic) artery
3 Left common carotid artery
4 Left subclavian artery
5 Right brachiocephalic vein
6 Left brachiocephalic vein
7 Superior vena cava
8 Inferior vena cava
The innominate artery bifurcation lies behind the right sternoclavicular joint and the subclavian arteries arch over the apex of each lung (Fig. 4.12). The brachiocephalic veins are formed by the union of the internal jugular and subclavian veins, just lateral to the sternoclavicular joint. The right vein descends vertically along the right border of the sternum and the left crosses obliquely behind the manubrium; they join at the level of the sternal angle to form the superior vena cava. The inferior vena caval opening through the diaphragm is just to the right of the xiphisternum at the level of the eighth thoracic vertebra. The descending thoracic aorta and the oesophagus are sited in the posterior mediastinum and pass through the diaphragm at the level of the 12th and 10th thoracic vertebrae, respectively. These marked differences in vertebral levels (eighth, 10th and 12th) reflect the steep half-domed nature of the diaphragm (high anteriorly and low posteriorly) and the relative anteroposterior positions of the orifices. The apex beat of the heart can usually be felt by placing the flat of the hand over the left side of the chest, centred over the fifth intercostal space in the midclavicular line.
On listening over the heart, two distinct noises are heard close together at the beginning of each beat. These are usually referred to as ‘lubb-dupp’. The first is produced by the closure of the mitral and tricuspid valves and the second by the aortic and pulmonary valves. Each valve is heard most clearly over specific areas of the anterior chest. The two valves in the systemic circulation provide most of the noise. The mitral valve is heard best over the apex of the heart. If this is not palpable, the stethoscope should be placed over the left fifth intercostal space in line with the nipple (the midclavicular line). Auscultation of this area in the female may require raising a pendulous breast. The aortic area is just to the right of the sternum in the first intercostal space and the pulmonary area at an equivalent site to the left of the sternum. The tricuspid area is over the right side of the sternum at the level of the fourth costal cartilage. Abnormalities of the heart and valves may alter or produce additional heart sounds.
Disease of the coronary arteries compromises the blood supplied to the heart muscle. This may produce pain on exercise, i.e. when the muscle requires more blood, a condition known as angina. Severe deprivation of the blood supply to the myocardium may produce an area of cardiac muscle death (myocardial infarction, MI). Infarction interferes with muscle contraction and may also damage the conducting system of the heart, giving rise to abnormal rhythms, possibly with a fatal result.
Thoracic incisions and access points (Fig. 4.13)
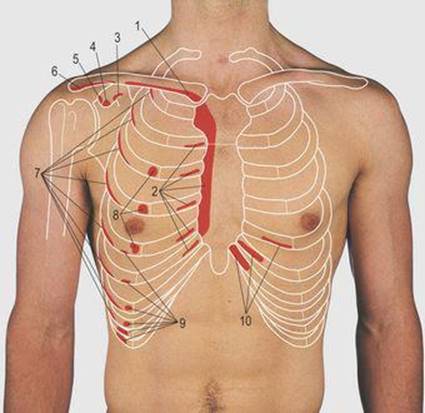
The majority of cardiac operations are undertaken through a midline sternal splitting incision. After dividing the skin and subcutaneous tissues the bone is divided by a vibrating bone saw or specific bone-cutting instruments. On separating the two halves of the sternum the chest wall and pleural cavities are pulled laterally exposing the pericardium and great vessels. The left brachiocephalic vein crosses the superior mediastinum and is put on a stretch by this manoeuvre; it has to be carefully freed to avoid damage.
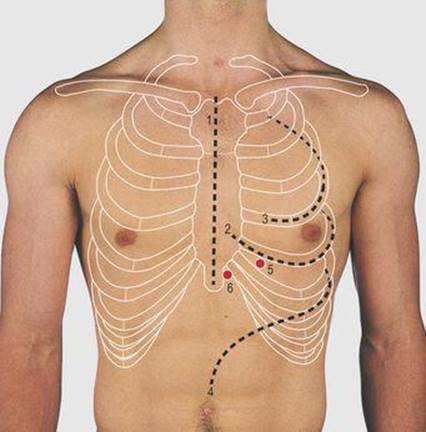
4.13 Applied anatomy of the anterior chest wall
1 Midline sternotomy approach to the mediastinum
2 Left anterolateral thoracotomy through bed of fifth rib
3 Posterolateral thoracotomy through bed of fourth rib
4 Thoraco-abdominal incision
5 Point for insertion of a needle into ventricles
6 Point for insertion of a needle into pericardial cavity for emergency pericardiocentesis
The ventricles, mitral valve and pulmonary trunk may also be exposed through an incision following the anterolateral aspect of the left fifth rib. The incision passes through skin and subcutaneous tissue onto the rib and the periosteum is divided along the outside of the rib. By stripping the periosteum from the inferior margin of the rib a further incision can be made through the periosteum and parietal pleura in the rib bed to enter the pleural cavity. In this incision the rib is not removed but may be divided posteriorly, or the incision taken transversely across the sternum, to obtain greater exposure.
To expose the hilum of the lung, a posterolateral incision is made through the chest wall with the patient lying on the opposite side and the free arm flexed to pull the scapula forward around the rib cage. The incision follows the line of the fourth rib and fibres of the trapezius and latissimus dorsi muscles are divided in line with the incision (Fig. 4.9, p. 35). Exposure of the posterior mediastinum is through the bed of the seventh or eighth ribs. This incision may be continued across the costal margin to open the abdominal cavity as in operations on the gastro-oesophageal junction.
An intracardiac injection can be made through the medial aspect of the fifth intercostal space. A needle inserted alongside the xiphisternum and passed cranially deep to the body of the sternum will enter the pericardial cavity.
The intercostal nerves run deep to the inferior margin of each rib and they can be anaesthetised by injection of local anaesthetic for pain relief. The site chosen is usually along the posterior axillary line deep to the inferior border of one or more ribs.
Lateral chest wall, breast and axilla (Figs 4.14-4.17)
The lateral chest wall is formed of the rib cage; this is bounded inferiorly by the costal margin and superiorly it projects into the axilla. It is continuous with the anterior and posterior chest wall without any demarcating line (Fig. 4.14). Ribs can usually be palpated along the length of this wall but, as the topmost rib felt in the axilla varies, counting is either from the floating ribs or by following a numbered rib from the sternum. The serratus anterior muscle is attached along the length of the anterior medial border of the scapula; its fibres pass laterally and form eight slips, attached to the upper eight ribs. These slips can be seen in a thin subject, together with their interdigitations with the external oblique muscle on the middle four ribs. It is supplied by the long thoracic nerve, from the brachial plexus.
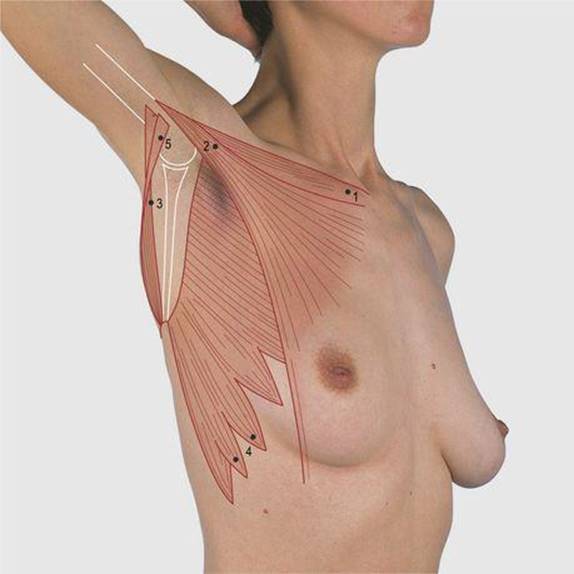
4.14 Lateral chest wall and axilla
1 Clavicle
2 Anterior axillary fold made up primarily of clavicular and sternocostal heads of pectoralis major muscle
3 Posterior axillary fold formed by teres major, with the tendon of latissimus dorsi wrapping around it
4 Slips of the serratus anterior passing onto lateral aspect of ribs
5 Latissimus dorsi
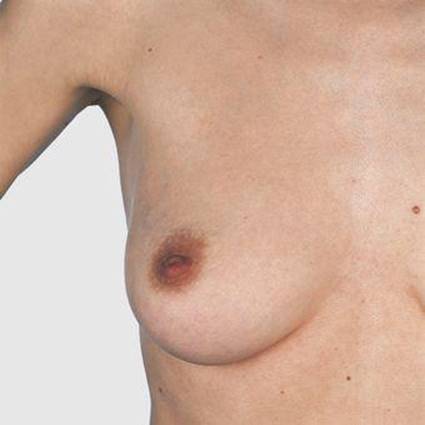
4.15 Female breast
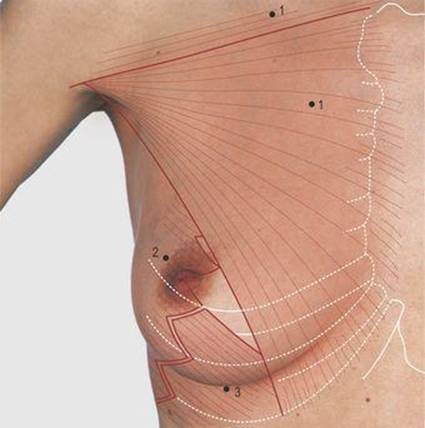
4.16 Female breast: relation to the chest wall
1 Pectoralis major
2 Serratus anterior
3 External oblique
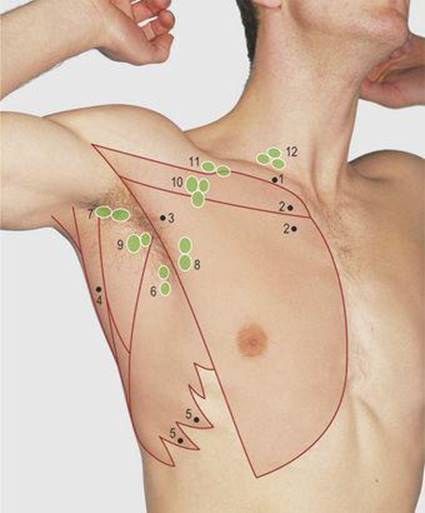
4.17 Axillary lymph nodes
1 Clavicle
2 Pectoralis major
3 Anterior axillary fold
4 Tendon of latissimus dorsi
5 Serratus anterior
6–10 Groups of nodes
6 Medial
7 Lateral
8 Anterior
9 Posterior
10 Apical
11 Infraclavicular
12 Supraclavicular
The female breast extends from the second to the seventh ribs and from the lateral border of the sternum to the anterior axillary wall. It overlies the pectoralis major, the serratus anterior and the external oblique muscles (Fig. 4.16). The axillary tail of the breast extends superolaterally around the lower border of the pectoralis major muscle into the axilla. The size of the breast and level of the nipple are variable in the female. In the male the nipple is in the midclavicular line over the fourth intercostal space.
The axilla is a fat-filled pyramidal cavity separating the chest and arm. Its medial wall is formed by the upper six ribs and the anterior and posterior walls converge laterally onto the palpable upper shaft of the humerus. The anterior and posterior walls can be felt between finger and thumb; the anterior is higher and is formed mainly of the pectoralis major muscle (Fig. 4.16). The posterior wall is mainly from the teres major muscle, passing from the medial edge of the scapula to the medial lip of the bicipital groove of the humerus; the tendon of latissimus dorsi wraps around the inferior border of the teres major muscle (Fig. 4.14). The apex of the axilla leads into the neck through a narrow opening, the cervico-axillary canal. This transmits the axillary vessels and the cords of the brachial plexus. The artery can be palpated laterally on the posterior axillary wall. The cords of the brachial plexus are closely applied to the axillary artery within the axillary sheath; local anaesthetic can be injected into the sheath to spread along it to produce regional anaesthesia. The axilla contains many lymph nodes and is covered inferiorly by skin arching from the chest wall onto the arm.
The breast is palpated for abnormal masses with the flat of the hand, compressing it against the chest wall. Its mobility over underlying muscle is assessed by subjects pressing their hands on their hips. Malignancy of the breast may spread to lymph nodes in the axilla. These nodes may also be involved in infection and malignancy at other sites. The nodes are sited in anterior, posterior, medial, lateral and apical groups; the apical group is high in the axilla, communicating through the cervico-axillary canal with the infraclavicular and supraclavicular nodes, and lymph channels forming the subclavian lymph trunk (Fig. 4.17). Normal axillary lymph nodes may be palpable, mainly as small nodules of 4–8mm in diameter, often termed ‘shotty’ nodes.
The axillary contents are palpated with the subject's arm slightly abducted, flexed at the elbow and with the hand resting on the chest. The examiner's left hand is used to examine the right axilla and the right hand the left axilla. During this manoeuvre, the non-palpating hand holds the elbow of the subject to support the weight of the arm. The apical and medial nodes are palpated with a cupped hand passing up the lateral aspect of the axilla, feeling the axillary contents against the chest wall as the hand is drawn downwards. Other groups of lymph nodes are examined by compressing the axillary contents against the anterior and posterior axillary walls and laterally against the humerus.