Posterior aspect of the neck 54
Posterior aspect of the trunk 56
Structure and movement of the vertebral column 57
Spinal cord 60
The axial skeleton is made up of the skull (pp. 10 and 13), the spine and the rib cage (p. 32–34). The spine (vertebral column) is an osseocartilaginous structure lying posteriorly in the midline. It articulates with the skull superiorly and extends through the neck and trunk to the tip of the coccyx. It articulates with the rib cage, forms part of the pelvis and gives attachment to the muscles of the shoulder girdle. The column thus provides a rigid, yet flexible, axis for the head to pivot; the upper limbs to be suspended and carry loads; the thoracic cage to be attached and function as an expansile respiratory unit; and the transfer of the body weight to the legs, when standing and in locomotion, and to the ischial tuberosities when seated. The column also provides a protective covering for the spinal cord.
The vertebral column is made up of 33 vertebrae – seven cervical, 12 thoracic, five lumbar, five sacral and four coccygeal. Of these, 24 are mobile: the sacral vertebrae are fused and the coccygeal vestigial. The mobile vertebrae are united by fibrocartilaginous intervertebral discs, each comprising an outer firm ring, the annulus fibrosus, and a central gelatinous nucleus pulposus. The discs make up a quarter of the height of the column.
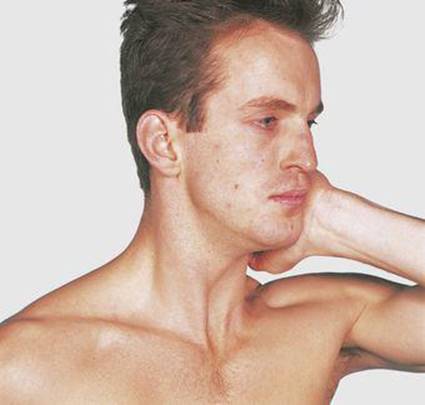
The embryonic and early fetal vertebral column is curved, concave ventrally (flexed) throughout its length – the primary curvature. Two secondary curvatures, concave dorsally, develop in the cervical and lumbar regions. The cervical curve starts as early as the 10th week ‘in utero’. After birth, further extension in the cervical region is produced by the muscles raising the head, and extension in the lumbar region accompanies the adoption of the erect posture. The thoracic and sacral regions retain the primary curvature (Figs 6.1 and 6.2).

6.1 Spinal curvatures
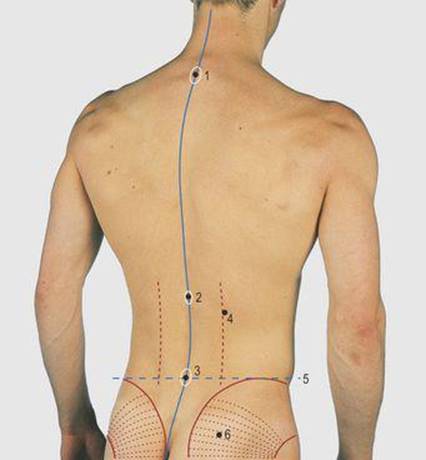
6.2 Spinal curvatures
1 Spine of first thoracic vertebra
2 Spine of twelfth thoracic vertebra
3 Spine of fourth lumbar vertebra
4 Lateral margin of erector spinae muscles
5 Supracristal plane
6 Gluteus maximus
Posterior aspect of the neck
The posterior aspect of the neck is bounded superiorly by the superior nuchal line of the occipital bone extending medially to the external occipital protuberance and laterally to the mastoid process (Figs 6.3-6.6).
6.3 Posterior aspect of the neck
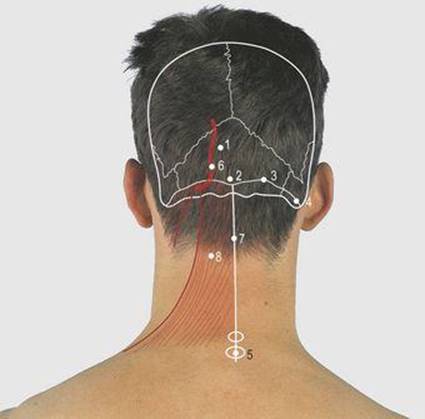
6.4 Posterior aspect of the neck: bones and soft tissues
1 Occipital bone
2 External occipital protuberance (inion)
3 Superior nuchal line
4 Mastoid process
5 Spine of first thoracic vertebra
6 Occipital artery
7 Ligamentum nuchae
8 Trapezius muscle

6.5 Posterior aspect of neck: palpable structures
1 External occipital protuberance
2 Superior nuchal line
3 Mastoid process
4 Spine of 7th cervical vertebra (vertebra prominens)
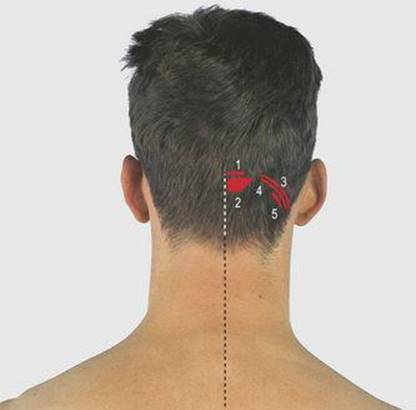
6.6 Posterior aspect of the neck: muscle attachments
1 Trapezius
2 Semispinalis capitis
3 Sternocleidomastoid
4 Splenius capitis
5 Superior oblique
The structures in the lower part of the neck are less easily discernible posteriorly as they are covered by the trapezius, splenius and powerful erector spinae muscles. The ligamentum nuchae lies in the midline between the muscles of the two sides, and is attached to the occipital bone and the cervical spines. The spines of the lower two or three cervical, and all the thoracic, vertebrae are palpable. The upper cervical spines are impalpable and overlain by a median furrow. The non-bifed lowest (seventh) cervical vertebral spine and the first thoracic are the most obvious, the former being termed the vertebra prominens.
The trapezius muscle has a wide attachment (Figs 6.7 and 6.8, see also p. 70). It lies superficially and is attached superiorly to the medial third of the superior nuchal line, to the ligament nuchae and the spines and interspinous ligaments of the cervical and thoracic vertebrae. Laterally, it is attached to the acromion and spine of the scapula, both of which are palpable from the tip of the shoulder to the medial angle of the bone. The sternocleidomastoid muscle is attached to the lateral third of the superior nuchal line and to the mastoid process. The occipital artery emerges medial to the muscle to pass over the skull; it is palpable at this site.
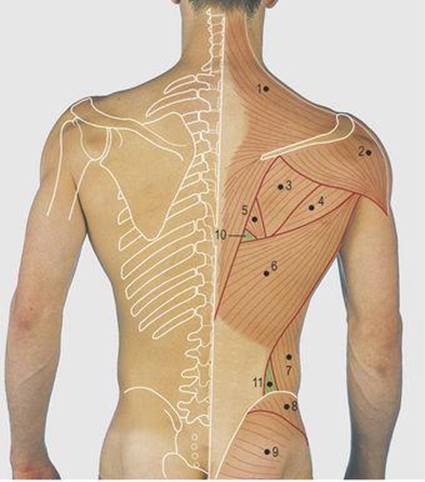
6.7 Posterior trunk: bones and superficial muscles
1 Trapezius
2 Deltoid
3 Infraspinatus
4 Teres major
5 Rhomboideus major
6 Latissimus dorsi
7 External oblique
8 Gluteus medius
9 Gluteus maximus
10 Auscultatory triangle
11 Lumbar triangle
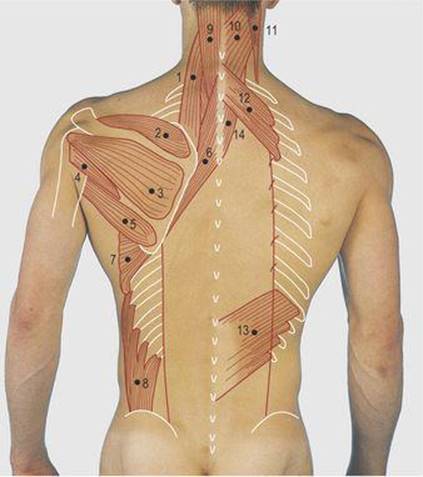
6.8 Posterior trunk: deep muscles of shoulder girdle
1 Levator scapulae
2 Supraspinatus
3 Infraspinatus
4 Teres minor
5 Teres major
6 Rhomboid muscles
7 Serratus anterior
8 External oblique
9 and 14 Semispinalis capitis
10 Splenius capitis
11 Sternocleidomastoid
12 Serratus posterior superior
13 Serratus posterior inferior
The superior nuchal line overlies the transverse venous sinus. The hindbrain lies below this level within the posterior fossa. The attachments of the trapezius, erector spinae and short occipital muscles have to be scraped off the surface of the occipital bone to allow surgical access to the posterior fossa. The vertebral artery lies deep to these muscles, crossing the suboccipital triangle.
Posterior aspect of the trunk
The thoracic vertebrae give attachment to the 12 pairs of ribs making up the rib cage (p. 34), and the muscles of the shoulder girdle (p. 69). The free ends of the floating ribs and the costal margins are palpable, but most of the ribs cannot be felt through the muscle mass or the scapula that overlies the second to seventh ribs; these levels equate, respectively, to the body of the fourth (spine of the third) and ninth (spine of the eighth) thoracic vertebrae. The downward projecting thoracic spines are all palpable; counting is facilitated by asking the subject to bend forwards, when they jut out slightly. The lowest thoracic and all of the lumbar spines are horizontal and easily palpable. A precise landmark at this level is the spine of L4, which is in the supracristal plane, i.e. the line through the crests of the iliac bones (Fig. 6.2).
The spines of the sacrum, sacral hiatus and coccyx are usually palpable, curving anteriorly, and their anterior surface can be felt on rectal examination. The sacrum forms part of the pelvis, uniting with the ilium of each side through the sacroiliac joints which, although synovial, are immobile and often fused. The crest of the ilium is palpable from the anterior superior iliac spine throughout its length to the posterior superior iliac spine, which is overlain by a skin dimple. The posterior inferior iliac spine and the sacroiliac joints may also be palpable and, through the gluteus maximus, the posterior aspect of the acetabulum. Inferiorly, the ischial tuberosities take the weight of the body when seated.
The female pelvis is relatively wider, has greater capacity, and its bones are thinner, smoother and lighter than those of the male. Other comparative features are a shallower acetabulum, a more vertical ilium, and a triangular rather than an oval-shaped obturator foramen; in addition, the width of the acetabulum is less than the distance from its anterior rim to the symphysis pubis, this distance being greater in the male. The inferior pubic angle is wider in the female.
Structure and movement of the vertebral column
The stability of the vertebral column is provided by the shape of the bones, including the curvatures, their intervertebral joints, strong ligaments and powerful muscles. The intervertebral discs act as shock absorbers between the short cylindrical vertebral bodies, conveying a certain resilience to the column.
Typical vertebrae have a body and a posterior bony arch; the body lies anteriorly, with a short stout pedicle on each side, completed posteriorly by the lamina, with a posterior projecting midline spine. The facets for the intervertebral synovial joints are sited at the junction of each pedicle and the lamina. The facets vary in shape in different regions, and this determines the type and amount of movement. Although the movement between adjacent vertebrae is small, a considerable range of movement is present in the vertebral column as a whole (Fig. 6.9). Flexion is most marked in the cervical region, rotation in the thoracic region, and extension and lateral flexion in the lumbar region.
6.9 Spinal flexion
The first (atlas) and the second (axis) cervical vertebrae are atypical. The axis is an oval ring of bone articulating with the condyles of the occipital bone superiorly (facilitating head flexion and extension) and the horizontal flat atlantoaxial facets inferiorly, allowing rotation of the head on the neck. The body of the atlas has become fused with the axis to produce a process (the dens) separate from its origin and acting as a pivot around which the atlas rotates (Figs 6.10 and 6.11). The movement between the remaining cervical vertebrae is predominantly flexion and extension. Some lateral flexion is present and accompanied by slight rotation. Head and neck movements are demonstrated in Figures 6.12-6.17.

6.10 Cervical spine: anterior view
1 Mastoid process
2 Base of skull
3 Anterior arch of atlas
4 Transverse process of first thoracic vertebra
5 Body of first thoracic vertebra
6 First rib

6.11 Cervical spine: lateral view
1 Angle of mandible
2 Occipital bone
3 Posterior arch of atlas
4 Spine of seventh cervical vertebra
5 Hyoid bone
6 Tracheal gas shadow
7 Clavicle
6.12 Neck flexion

6.13 Raising the head from the horizontal

6.14 Neck extension

6.15 Lateral flexion of the neck

6.16 Lateral rotation of the neck
6.17 Resisted lateral rotation of the neck
Rotation is brought about by contraction of the right sternocleidomastoid muscle
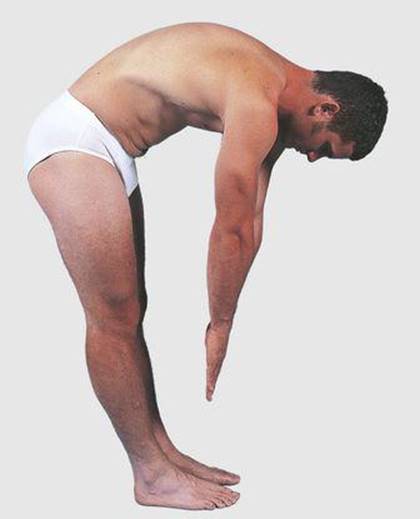
Movement of the thoracic spine is limited by the rib cage and by the need for uninhibited respiratory movements. Some rotation is present, particularly between the lower thoracic vertebrae (Fig. 6.18). Movement of the lumbar spine (Figs 6.19 and 6.20) is restricted to flexion and extension. This can be demonstrated by marking the lumbar spines and seeing their longitudinal separation when the subject is asked to touch his or her toes (Figs 6.21 and 6.22).
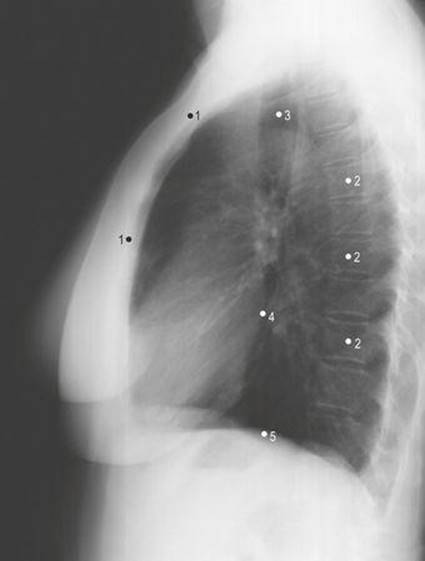
6.18 Thoracic spine: lateral view
1 Sternum
2 Bodies of thoracic vertebrae
3 Tracheal gas shadow
4 Posterior border of heart
5 Dome of diaphragm

6.19 Lumbar spine: anterior view
1 Body of twelfth thoracic vertebra
2 Twelfth rib
3 Body of fourth lumbar vertebra
4 Sacrum
5 Sacroiliac joint

6.20 Lumbar spine: lateral view
1 Body of fifth lumbar vertebra
2 Sacrum
3 Hip joint

6.21 Posterior aspect of the lower trunk: at rest
The two skin marks are over space between L3 and L4 spines

6.22 Lumbar flexion
The skin marks between L3 and L4 are stretched in relation to Fig. 6.21 but the palpable relation to the underlying spines has remained the same, demonstrating the contribution of the lumbar spine to trunk flexion
In the trunk, flexion is brought about by the rectus abdominis, aided by the prevertebral muscles. Lateral flexion is by the oblique abdominal wall muscles and quadratus lumborum, and rotation by the internal and external oblique abdominal muscles. The body’s centre of gravity lies anterior to the second piece of the sacrum. Movement of the body frequently carries the centre of gravity much further forward and a large powerful posterior muscle mass is required both to balance the effects of gravity and to restore the upright position. This is primarily by the erector spinae muscles.
The erector spinae (sacrospinalis) is a large muscle mass on each side of the vertebral column, extending from the sacrum to the skull. It is a collective term for many small muscle groups passing between adjacent vertebrae or across a number of vertebrae. It varies in bulk at different levels. In the sacral region it is relatively narrow, predominantly tendinous and of great strength. The most prominent part is in the lumbar region, and its cylindrical form is visible and palpable. In the thoracic region the mass flattens out, extending laterally to the angle of the ribs, to which it is also attached; it is covered by the scapula and muscles of the shoulder girdle. In the cervical region the cylindrical masses are covered by the trapezius and splenius muscles. Although three parallel columns can be identified in each erector spinae muscle, it is best considered as a powerful extensor unit acting on the vertebral column and the skull (Figs 6.23, p. 61).
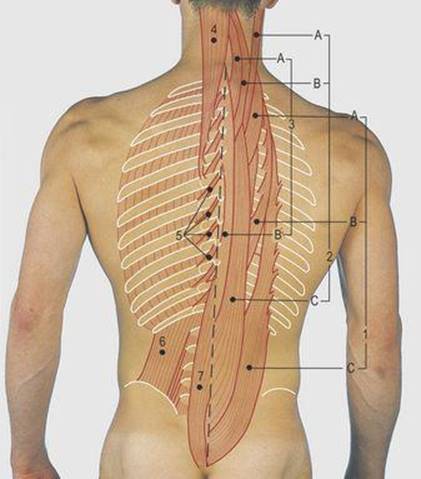
6.23 Posterior trunk: sacrospinalis
1 Iliocostalis
A Cervicis
B Thoracis
C Lumborum
2 Longissimus
A Capitis
B Cervicis
C Thoracis
3 Spinalis
A Cervicis
B Thoracis
4 Semispinalis capitis
5 Rotatores and levator costae
6 Quadratus lumborum
7 Multifidus
The lower lumbar vertebrae and discs, particularly the lumbosacral disc, are subject to the greatest load, stresses and strains. Musculoskeletal injuries are common in this region, resulting in low back pain. Degenerative changes in the annulus fibrosus allow protrusion of the nuclear content of a disc, with resultant pressure on adjacent tissues, such as the spinal cord or spinal nerves – the so-called ‘prolapsed’ (slipped) disc. Neurological signs may be present, together with spasm of the erector spinae muscles. Other clinical features are reduced spinal movement and loss of the normal lumbar lordosis.
Unilateral spasm causes scoliosis (lateral curvature in the coronal plain). Acute scoliosis of this form is usually compensated for by a compensatory curve in the thoracic region, the head and shoulders being maintained in line with the pelvis. Scoliosis is best observed from behind; it is made more obvious when the subject leans forward. Abnormalities of the spine may also produce lordosis and kyphosis – a concavity anteriorly and posteriorly, respectively, in the sagittal plain. In view of the fixed nature of the thoracic cage, scoliosis is usually accompanied by some rotation, producing a kyphoscoliotic spine.
Pain can be referred to the back from adjacent viscera. For example, disease of the descending thoracic aorta, such as rupture or dissection of an aneurysm, produces severe pain between the scapulae; in disease of the abdominal aorta, pain is projected to the lumbar region. Pancreatic disease produces central upper lumbar pain and the gall bladder right-sided pain at a similar level. Renal pain is characteristically in the subcostal region posteriorly. Pelvic disease, such as gynaecological infection and lower rectal pathology, can present with low back pain.
The muscle mass protects the abdominal viscera and lungs from injury, but major trauma can fracture ribs (putting the lungs, spleen and liver at risk) and damage the kidneys lying on the posterior abdominal wall.
Spinal cord
Collectively, the arches of the vertebrae, together with their ligaments, and the vertebral bodies anteriorly form a longitudinal cylindrical cavity – the vertebral canal – that houses and protects the spinal cord and its coverings. There are eight pairs of cervical spinal nerves; the number at other levels is the same as the number of vertebrae. The upper seven cervical nerves leave the vertebral canal through intervertebral foramina above the pedicles of the equivalent vertebrae. The eighth cervical nerve passes beneath the pedicle of the seventh cervical vertebra. The thoracic and lumbar spinal nerves pass beneath the pedicles of the equivalent vertebrae. The sacral nerves pass out through foramina in the fused bone, and the coccygeal nerves pass through the sacral hiatus to the perineum.
The spinal cord finishes at the level of the third lumbar vertebra at birth, and the first lumbar vertebra in the adult. The disparity of length of the spinal cord and the vertebral canal means that caudal nerves descend an increasing distance within the meningeal coverings. The dural sac extends to the second sacral vertebra. The collection of nerves below the spinal cord is known as the cauda equina. This anatomical arrangement has important clinical significance, since a needle can be introduced into the dural sac below the level of L3 in a baby and L1 in an adult without risk of damaging the spinal cord (Fig. 6.24). As noted, the fourth lumbar spine is in the supracristal plane – a needle is inserted above or below this spine in the procedure known as a lumbar puncture. It can be used to remove samples of cerebrospinal fluid, or introduce local anaesthetic into the extradural space, or dural sac, known, respectively, as epidural and spinal anaesthesia.
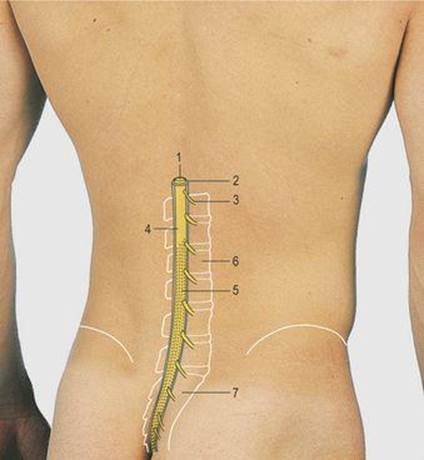
6.24 Spinal canal
1 Spinal cord
2 Dural sac
3 Spinal nerve
4 Conus medullaris
5 Cauda equina
6 Body of second lumbar vertebra
7 Sacrum
Injection of local anaesthetic into the sacral hiatus anaesthetises the lower spinal nerves, especially those supplying the perineal region. This is termed caudal anaesthesia and can be used to reduce the pain of childbirth. The lumbar spine and spinal cord are approached surgically through a posterior midline incision centred over the appropriate vertebra. One or more spines and laminae are removed to facilitate access (laminectomy).