Willis M. Wu and Samir R. Kapadia
Unstable angina, non–ST-segment-elevation myocardial infarction (NSTEMI), and ST-segment-elevation myocardial infarction (STEMI) represent a spectrum of ischemic coronary disease of similar etiology—atherosclerotic plaque instability and rupture—termed acute coronary syndrome (ACS). The role of risk stratification in ACS is to identify which patients have increased risk for adverse events and are therefore more likely to benefit from the array of mechanical and pharmacologic therapies available. Risk stratification after myocardial infarction (MI) begins during the initial clinical encounter, continues throughout the index hospitalization, and remains important after discharge. Although modern advances have had a significant impact on outcomes of MI, post-ACS morbidity (and mortality) remain a challenging problem, most notably recurrent ischemia and infarction, congestive heart failure (CHF), and sudden cardiac death (SCD).
Recent data favor an early invasive approach for most patients. Early aggressive lipid-lowering therapy post-MI is clearly beneficial, with lower targets for low-density lipo-protein (LDL) levels. The importance of neurohormonal blockade has become apparent, particularly in patients with left-ventricular systolic dysfunction. Antiplatelet therapies have become essential, both during and after ACS, but in particular following percutaneous coronary intervention (PCI). The role of the implantable cardioverter–defibrillator (ICD) after MI has become clearer, with recent trials indicating no benefit to ICD early in the course post-MI, but demonstrable subsequent benefit in patients with significant left ventricular (LV) dysfunction. The recognition of the role of inflammation in ACS has led to the development of clinical assays measuring inflammatory markers such as C-reactive protein (CRP) and brain natriuretic peptide (BNP), but their role in clinical practice is not well established. Lifestyle modification and risk-factor reduction remain important, including smoking cessation, diabetes, and hypertension management.
RISK STRATIFICATION FOR ST-ELEVATION MI
Identification of high-risk characteristics early after MI is important because 25% of deaths during the first postinfarction year occur within the first 48 hours of hospitalization, and more than one-half of deaths occur within the first month after STEMI. Demographic and clinical data, electrocardiogram (ECG), serum markers, and various diagnostic tests assist in the risk assessment.
Initial Presentation
Clinical and Demographic Factors
The most important predictors of death within 30 days are age, systolic blood pressure (SBP) and heart rate at presentation, evidence of CHF on physical examination, location of infarction, and previous infarction. In the Global Utilization of Streptokinase and TPA for Occluded Arteries-I (GUSTO-1) study, these predictors accounted for >90% of the total prognostic information. Additional important prognostic factors include female gender, history of diabetes, hypertension, smoking, and vascular disease (Table 43.1).
TABLE
43.1 Predictors of Mortality in STEMI
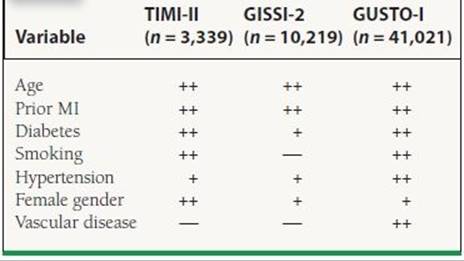
+ , univariate predictor; ++, multivariate predictor.
Advanced age has been recognized as an important predictor of mortality in several studies. In the NRMI (National Registry of Myocardial Infarction) registry, a community-based database with information on >350,000 patients with acute MI at U.S. hospitals, in-hospital mortality ranged from 3% for patients younger than 55 years of age to 28% for individuals more than 84 years of age. Older patients are more likely to possess a history of a prior MI, have more severe coronary disease, and consequently are more likely to develop CHF and cardiogenic shock after MI. Additionally, several reports have shown that older patients are also less likely to receive life-saving therapies such as immediate reperfusion therapy, beta-blockers, and aspirin, which may contribute to the worsened prognosis.
In several studies, women have been shown to have higher mortality after STEMI. In the GUSTO-1 trial, women had higher 30-day mortality (11.3% vs. 5.5%), occurrence of shock (9% vs. 5%), and reinfarction (5.1% vs. 3.6%) compared to men. Part of this increased risk can be explained by the advanced age and increased prevalence of preexisting diabetes and hypertension. Additionally, women are more likely to present late during an infarction.
Paradoxically, smokers possess a lower risk for early mortality, most likely because of their younger age. Diabetes mellitus has been associated with a 1.5 to 3.0 times higher mortality after STEMI. Whether this is due to a higher atherosclerotic burden or some other characteristic induced by the diabetic state, such as silent ischemia or a larger infarct size, remains unclear. Further, the nonfatal complications are also higher in diabetic patients, including a greater incidence of postinfarction angina, reinfarction, and heart failure.
Physical Examination
The clues to right ventricular (RV) and LV dysfunction on physical examination provide the most important prognostic information. Accordingly, variables predictive of a worsened outcome include hypotension, tachycardia, jugular venous distension, an S3 gallop, pulmonary edema, and evidence of peripheral hypoperfusion, many of which are captured by the Killip classification (Table 43.2). The physical examination can also help to identify mechanical complications of MI, such as acute mitral regurgitation, ventricular septal defect, and free wall rupture, all of which have been associated with significant mortality.
TABLE
43.2 Killip Classification and Mortality from GUSTO-I Trial
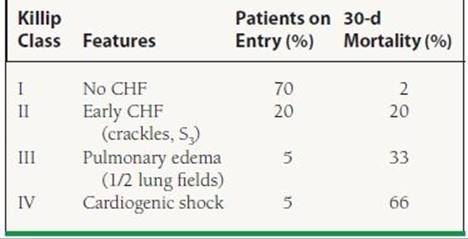
CHF, congestive heart failure.
Electrocardiogram
The ECG provides useful information about the location and size of infarction, likelihood of tissue reperfusion after treatment, presence of ongoing ischemia, and conduction system dysfunction. The finding of ST elevation or depression has similar prognostic implications (Fig. 43.1). Mortality is greater in patients experiencing anterior wall MI compared to after inferior MI, even when corrected for infarct size. Patients with RV infarction complicating inferior infarction have a higher mortality rate than patients sustaining an inferior infarction without RV involvement. Patients with multiple leads showing ST-segment elevation and those with a high degree of ST-segment elevation have increased mortality, especially if their infarct is anterior. Patients with persistent or advanced heart block (e.g., Mobitz type II, second-degree, or third-degree AV block) or new intraventricular conduction abnormalities (bifascicular or trifascicular) in the course of an acute MI have a worse prognosis than do patients without these abnormalities. The influence of high-grade conduction block is particularly important in patients with RV infarction, for such patients have a markedly increased mortality. Other ECG findings suggesting a worse outcome are persistent horizontal or downsloping ST-segment depression, Q waves in multiple leads, evidence of RV infarction accompanying an inferior infarction, ST-segment depressions in anterior leads in patients with an inferior infarction, and atrial arrhythmias (especially atrial fibrillation).
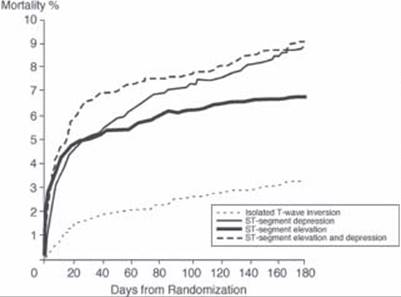
FIGURE 43.1 Mortality rate according to electrocardiographic findings on presentation with acute MI in the GUSTO IIb trial. (Adapted from Savonitto S, Ardissino D, Granger CB, et al. Prognostic Value of the Admission Electrocardiogram in Acute Coronary Syndromes.JAMA1999;281:707–713.)
Other than these well-established predictors on ECG, ST-segment resolution has generated renewed interest in determining effectiveness of reperfusion therapy. Resolution of ST elevation predicts successful perfusion at the myocardial level, which is the most important predictor of LV function and survival. Continuous ST-segment monitoring has been shown to yield important prognostic information after 60 minutes of observation. In the ASSENT 2 (Assessment of Safety and Efficacy of a New Thrombolytic) and ASSENT-PLUS studies, the optimal cutoff for ST-segment resolution analyses was found to be 50%, measured at 60 minutes. Patients with ST resolution (40%) by this criterion had a 30-day mortality of only 1.4%.
Biomarker Assessment
Two separate groups of biomarkers have been used to predict outcome after MI. One group includes the myocardial enzymes that predict infarct size and another group assesses the degree of systemic vascular inflammation. The prognostic value of CRP, endothelin, BNP, CD40, and CD40 ligand has recently been investigated extensively. These markers of inflammation seem to predict an active atherosclerotic disease process. Aggressive risk-factor modification may be more important when the levels of these markers are high.
More conventional markers of myocardial damage include troponin-I or -T, creatine kinase (CK), CK-MB 1 and 2 isoforms, CK-MB isoenzyme mass, and occasionally myoglobin. The presence and degree of troponin, CK, and CK-MB isoenzyme elevation on admission and thereafter have been associated with poorer outcome in the setting of both STEMI and NSTEMI. However, there is less information on troponin levels in STEMI. In the GUSTO IIa study, 30-day mortality was substantially higher among patients who were troponin-T positive. Given their more rapid return to baseline, CK and CK-MB isoenzymes are also helpful for identifying high-risk individuals by facilitating the diagnosis of reinfarction shortly after an STEMI or NSTEMI. Currently, infarct size is determined by CK-MB mass; the role of troponin-I or -T in this matter has been less well established.
Imaging
Imaging at the time of acute infarction is used to determine the amount of jeopardized myocardium. Contrast echocardiography and technetium-based imaging can be used to quantify perfusion noninvasively. Nuclear scanning is superior for quantifying perfusion, whereas echocardiography is better for assessing function. Acute imaging has been used principally in clinical trials to determine the degree of myocardial salvage, which is the percent of ischemic myocardium atpresentation that has adequate perfusion on follow-up.
During Hospitalization
Recurrent angina is an important predictor of a worsened outcome and the need for revascularization. Recurrent chest pain frequently signifies ischemic myocardium, either in the peri-infarct territory supplied by the infarct-related artery or ischemia at a distance secondary to a non–infarct-related artery. Early revascularization is required in many patients who have postinfarct angina. Other important predictors include LV or RV dysfunction and mechanical complications of MI. Cardiogenic shock possesses a very high mortality in which medical management is not effective. Early revascularization in patients who develop cardiogenic shock within 36 hours of an MI is recommended, based on the findings of the SHOCK (Should We Emergently Revascularize Occluded Coronary Arteries for Cardiogenic Shock) trial, which showed reduced mortality with early revascularization compared to medical stabilization (33.3% vs. 51.6%). Arrhythmias, including high-grade AV block, atrial fibrillation, or ventricular tachycardia, also predict poor outcome.
Predischarge Assessment
Although significant emphasis is placed on predischarge risk stratification, many high-risk patients will declare themselves clinically during their hospital stay. The challenge for the clinician during the predischarge phase is to distinguish the few patients who remain at higher risk from the many relatively lower-risk patients. Although multiple testing technologies have been developed to aid in this process, the low event rate in these patients (1-year mortality rates of 2% to 5%) mandates that these tests must be highly sensitive and specific if they are to have clinical value. What tests should be routinely performed for predischarge risk stratification is highly debated. Risk stratification at discharge can be accomplished by determining three factors: (a) resting LV function, (b) residual potentially ischemic myocardium, and (c) susceptibility to serious ventricular arrhythmias. More sophisticated testing may provide additional data but may not be as useful in changing patient outcomes.
LV Function Assessment
Assessment of LV function is typically performed by echocardiography or by ventriculography at the time of cardiac catheterization. However, imaging of the left ventricle at rest may not distinguish between infarcted, irreversibly damaged myocardium and hibernating myocardium. Therefore, many different techniques have been used to determine viable myocardium, including dobutamine echocardiography, rest-redistribution thallium, positron emission tomography (PET) scanning, and magnetic resonance imaging (MRI). Dobutamine echocardiography can provide functional assessment along with information on viability and ischemia. However, the results are directly dependent on the expertise and experience of the interpreter. Radionucleotide imaging provides higher sensitivity to detect ischemia, but specificity can be compromised by the size of the patient, diaphragmatic or breast attenuation. Further, regional wall motion assessment is not as precise as with echocardiography. Regardless of the imaging modality chosen, the prognosis is worse if there is significant LV dysfunction, or if there is a large amount of ischemic myocardium.
Stress Testing
Patients who do not have high-risk features after successful thrombolysis should be considered for exercise stress testing. Although the predictive accuracy of exercise stress testing has diminished in the reperfusion era as a result of the lower incidence of adverse outcomes, it is still given a Class I indication under current American College of Cardiology/American Heart Association (ACC/AHA) guidelines. In addition, although it is not known whether exercise testing can effectively risk-stratify patients who have not received acute reperfusion therapy, it is also assumed to be effective in this setting. Low-level exercise appears to be safe in patients who have been free of angina or heart failure and who possess a stable baseline ECG during the previous 2 to 3 days. Patients who are unable to exercise or who have baseline ECG abnormalities that would preclude interpretation should undergo an exercise test with imaging. Patients who cannot achieve a 3 or 4 MET workload, those who develop ischemia at a low level of exercise, or those in whom blood pressure (BP) drops during exercise should undergo coronary angiography. No further testing should be necessary in patients without these high-risk findings.
Assessment for Risk of Sudden Cardiac Death
Determination of risk for SCD after MI is important because it is highest in the first 1 to 2 years after the index event. The most important predictor for SCD is LV dysfunction. Provocative electrophysiology studies are not necessary for risk stratification. Signal-averaged ECG, heart-rate variability, QT dispersion, and baroreflex sensitivity have been investigated to select specific patients with LV dysfunction who might benefit from an ICD. The presence of a filtered QRS complex duration >120 milliseconds and abnormal late potentials recorded on a signal-averaged ECG after acute MI signifies somewhat higher risk for SCD. However, the signal-averaged ECG suffers from a high false-positive rate, which makes the test clinically less useful. Depressed heart-rate variability is an independent predictor of mortality and arrhythmic complications after acute MI. A depressed baroreflex sensitivity value (3.0 millisecond/mm Hg) is associated with about a threefold increase in the risk of mortality. These tests may provide useful prognostic information, but at present, only assessment of ejection fraction (EF) is necessary to determine eligibility for a device, where significant LV dysfunction qualifies a patient for ICD placement. Recent data indicate, however, that ICD therapy is not beneficial in the early post-MI period, and should be delayed for at least 1 month after an infarction. ICD implantation is generally deferred for 3 months after revascularization, either surgically or percutaneously, at which time reevaluation of LV function can be performed.
Predischarge Management
In contemporary practice, most patients with MI will undergo cardiac catheterization, even after receiving thrombolytics for STEMI, based on the CARESS in AMI and TRANSFER AMI trials and the most recent guidelines. In the minority of patients who do not undergo catheterization initially, a judgment is made as to the presence of clinical variables indicative of high risk for future cardiac events. Patients with spontaneous episodes of ischemia or depressed LV function who are considered suitable candidates for revascularization based on their overall medical condition should be referred for cardiac catheterization. These patients are at increased risk of recurrent infarction (and subsequent increased mortality), and may benefit from revascularization if severe coronary artery disease (CAD) is identified at catheterization.
NON–ST-ELEVATION ACS
Many patients with ACS present without ST elevation on ECG. It is important to note that although the risk of mortality during the index hospitalization is less than in those with ST-elevation ACS, the prognosis at 1 year is similar (see Fig. 43.1). Typically, the underlying pathophysiology is a high-grade stenosis with plaque rupture, but unlike STEMI, the vessel is not totally occluded. Indeed, fibrinolysis has been shown to be of no benefit and may actually be harmful in this patient cohort. Multiple trials have investigated the role of early angiography and PCI versus conservative management in these patients, and it appears that early invasive strategy in the high-risk population provides the best outcome and may even be more cost effective than a conservative strategy.
Non–ST-Elevation MI Risk Stratification
Initial Presentation
A number of historical features predictive of a worse prognosis following non–ST-elevation ACS have been derived from existing trial data. These features are summarized in Table 43.3. The most important are older age, greater number of cardiac risk factors, known CAD, peripheral vascular or cerebrovascular disease, prior MI, previous PCI or coronary artery bypass graft surgery, history of CHF, a more severe anginal pattern, and the use of aspirin within a week of presentation.
TABLE
43.3 Predictors of a Worse Prognosis in NSTEMI
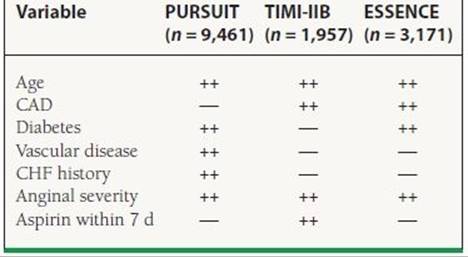
Other study predictors include female gender, number of risk factors, previous MI, prior PCI/CABG.
Electrocardiogram
Among patients with non–ST-elevation ACS, the presence of Q waves, ST changes associated with angina or at presentation (in particular, ST-segment depression), T-wave inversions of significant amplitude (i.e., >0.2 mV), or the absence of ECG changes during angina are important predictors of future events (see Fig. 43.1). When clinical variables are also considered, heart rate and the presence of ST depression on admission ECG are the most important multivariable predictors.
Biomarkers
The presence and degree of troponin elevation on admission and thereafter can identify patients who are at increased risk of experiencing adverse outcomes. Cardiac troponin-I and troponin-T are particularly useful in identifying high-risk patients with non–ST-elevation ACS. Other markers of inflammation, such as CRP, CD-40, CD-40 ligand, fibrinogen levels, or brain natriuretic peptide (BNP) can add to the prognostic information in ACS. Adding multiple markers to assess a patient may add important prognostic information, as illustrated in the OPUS-TIMI 16 (Oral Glycoprotein IIb/IIIa Inhibition with Orbofiban in Patients with Unstable Coronary Syndromes) trial and the TACTICS-TIMI 18 (Treat Angina with Aggrastat and Determine Cost of Therapy with an Invasive or Conservative Strategy) analyses (Fig. 43.2). However, at the present time, there is no clear consensus on how to incorporate these markers in patient management.
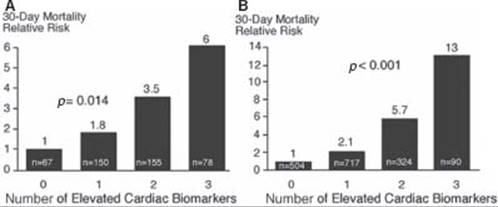
FIGURE 43.2 Relative 30-day mortality risks in OPUS-TIMI 16 (A) and TACTICS-TIMI 18 (B) in patients stratified by the number of elevated cardiac biomarkers (TnI, CRP, and BNP). (From Sabatine MS, Morrow DA, de Lemos JA, et al. Multimarker Approach to Risk Stratification in Non-ST Elevation Acute Coronary Syndromes. Circulation 2002;105:1760, with permission from Wolters Kluwer Health.)
Risk Scores
An essential element of risk stratification following an ACS is the quantification of short-term and long-term risk. Although there are many historical, physical exam, ECG, and biomarker variables that are significantly and independently associated with worse short-term outcome, the integration of these into an accurate estimation of risk is complex and has traditionally required the use of sophisticated multivariable modeling (Figs. 43.3 and 43.4). Nevertheless, simplified nomograms and risk scores incorporating the most important variables have been derived from a number of these analyses and allow for a reasonably accurate categorization of patients into low-risk, intermediate-risk, and high-risk groups. In the analysis by Boersma et al. patient age, heart rate, SBP, ST-segment deviation, signs of heart failure, and elevation of cardiac markers were the most important predictors of death or MI at 30 days. In the analysis by Antman et al. (TIMI risk score, see Fig. 43.3), age >65 years, >3 coronary risk factors, prior CAD, ST deviation, >2 angina episodes in last 24 hours, use of aspirin within 7 days, and elevated cardiac markers were important in determining death, reinfarction, or recurrent severe ischemia requiring revascularization (termed TIMI risk score).
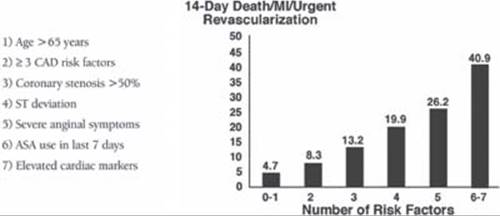
FIGURE 43.3 TIMI risk score (Adapted from Antman EM, Cohen M, Bernink PJLM, et al.The TIMI Risk Score for Unstable Angina/Non-ST Elevation MI. JAMA 2000;284:835–842.)
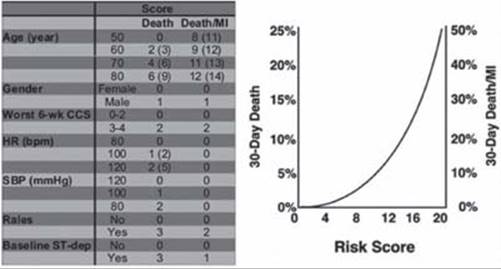
FIGURE 43.4 PURSUIT risk score 30-day outcome after non–ST-elevation ACS. (From Boersma E,Pieper KS, Steyerberg EW, et al. Predictors of Outcome in Patients With Acute Coronary Syndromes Without Persisent ST-Segment Elevation: Results From an International Trial of 9461 Patients.Circulation. 2000;101:2557–2567, with permission from Wolters Kluwer Health.)
During-Hospitalization and Predischarge Risk Stratification
According to current ACC/AHA guidelines, patients who are deemed to be high risk, including those with recurrent ischemia or reinfarction, CHF, hemodynamic compromise, or life-threatening arrhythmias, are candidates for early angiography. Additionally, the guidelines recommend angiography in those who have had prior PCI in the past 6 months, elevated cardiac biomarkers, new ST changes on EKG, high- risk score, or prior coronary artery bypass grafting (CABG).
The FRISC II (Fast Revascularization during Instability in Coronary Artery Disease) and TACTICS-TIMI 18 studies reported significant decreases in the rate of death or MI at 6 months among patients randomized to early angiography with revascularization as needed (i.e., early invasive approach.) The ISAR-COOL trial also demonstrated a decrease in death or large MI at 30-day follow-up in patients assigned to undergo angiography within 6 hours of presentation compared with 3 to 5 days. The TIMACS trial reflects contemporary medical practice by including patients treated with aspirin, clopidogrel, heparin, fondaparinux, and glycoprotein IIb/IIIa inhibitors. In this trial, the patients in the early invasive arm experienced less refractory ischemia, and patients with a higher GRACE risk score had fewer events of death, MI, and stroke.
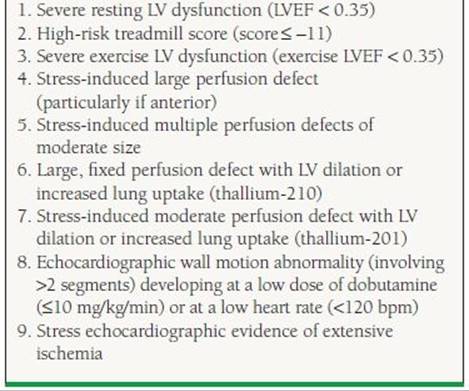
In the absence of high-risk clinical features or post-ACS complications, patients who have not undergone coronary angiography should be considered at low or intermediate risk pending the results of further risk stratification. Noninvasive testing provides useful supplementary information beyond that available from clinically based assessments of risk in this cohort. The purpose of noninvasive testing is to identify ischemia and estimate prognosis. Accordingly, noninvasive evaluation should include an assessment of LV function and/or ischemia in order to identify patients who are at increased risk for adverse outcomes who are likely to benefit from coronary angiography and revascularization. High-risk findings on noninvasive testing should direct patients to coronary angiography if they are eligible for revascularization (Table 43.4). It is not clear whether LV function assessment or myocardial perfusion imaging (with rest and during exercise or pharmacologic stress) is superior in assessing prognosis. The ability of most noninvasive tests to dichotomize patients into low-risk and high-risk groups appears similar (Table 43.5). Selection of the appropriate test should be based on patient characteristics, availability of the test, and institutional expertise in performance and interpretation.
TABLE
43.4 High-Risk Findings on Noninvasive Testing Leading to Coronary Angiography EKG-Abnormalities that Preclude Accurate Interpretation of an Exercise Stress Test
TABLE
43.5 Stress Test Predictors of Cardiac Death and MI
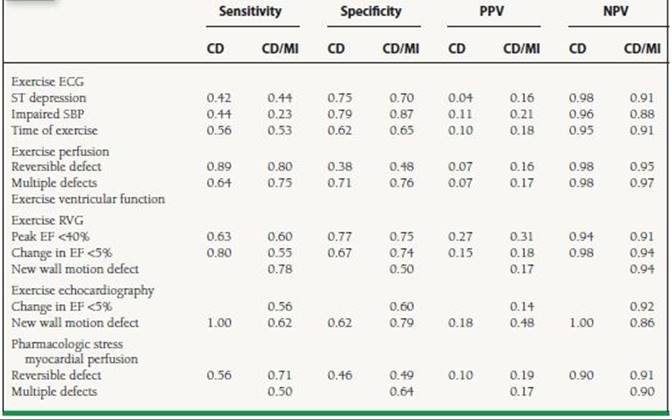
PPV, positive predictive value; NPV, negative predictive value; SBP, systolic blood pressure; RVG, radionuclide ventriculography; EF, ejection fraction.
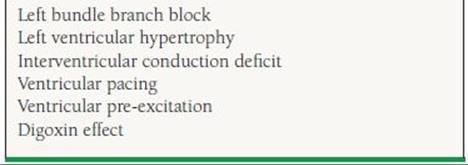
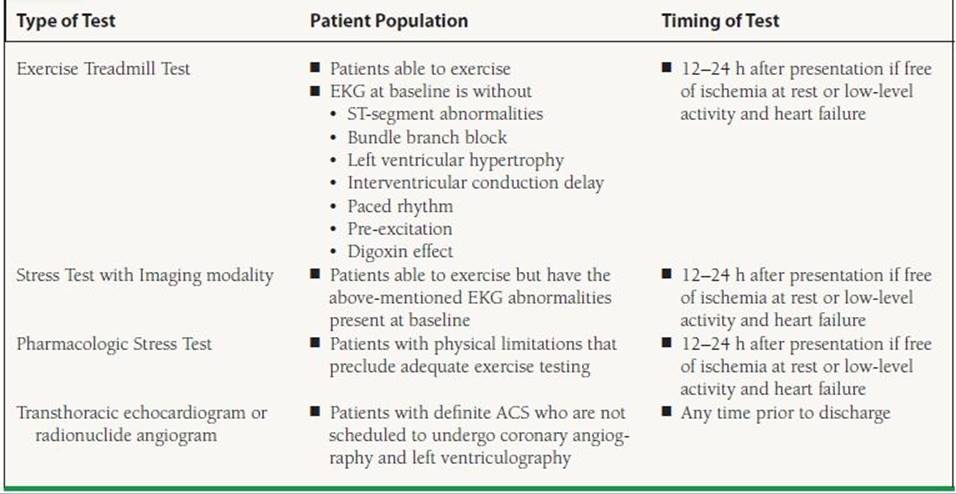
The ACC/AHA Guidelines recommend exercise ECG as the primary mode of noninvasive stress testing. Patients with baseline ECG abnormalities that preclude accurate interpretation (Table 43.6) should undergo an exercise test with imaging. Those who are unable to exercise (the cohort at highest risk of future adverse outcomes) should undergo pharmacologic stress testing with imaging. According to the ACC/AHA Guidelines, stress testing is safe in low-risk patients who have been free of ischemia or CHF for 12 to 24 hours in intermediate-risk patients (Table 43.7). Patients who do not have any high-risk findings on noninvasive evaluation require no further testing.
TABLE
43.6 EKG Abnormalities that Preclude Accurate Interpretation of an Exercise Stress Test
TABLE
43.7 Noninvasive Risk Stratification Prior to Discharge in Patients Managed with a Conservative Strategy who are Low to Intermediate Risk
POST–MYOCARDIAL INFARCTION THERAPY
After MI, secondary prevention of cardiovascular events depends on prompt institution of appropriate pharmacotherapy, lifestyle changes, and comorbid disease management. In this area, recent advances have revealed the significant benefits of antiplatelet therapy, neurohormonal blockade, and lipid-lowering therapy. The importance of diet and exercise, as well as smoking cessation, cannot be overemphasized. In addition, optimal management of diabetes and hypertension are paramount to preventing further events. Residual LV function after MI is a strong determinant of the proper approach to post-MI pharmacotherapy. This section outlines the role of these therapies as well as lifestyle changes in the post-MI patient.
Antiplatelet Therapy
A large number of randomized, controlled trials, summarized in meta-analysis by the Antiplatelet Trialists’ Collaboration, have documented the benefit of daily aspirin therapy after MI. Aspirin should be taken on a daily basis indefinitely by post-MI patients who can tolerate it, based on a reduction in recurrent infarction, stroke, or vascular death.
In patients treated without stenting, a daily dose of 75 to 162 mg should be prescribed. After percutaneous intervention, a dose of 162 to 325 mg should be prescribed for at least 1 month after bare metal stent implantation, 3 months for sirolimus-eluting stent implantation, and 6 months for paclitaxel-eluting stent implantation. Thereafter, a daily dose of 75 to 162 mg should be prescribed. Although the universal application of aspirin therapy among patients without contraindications is accepted, a subset of patients can be shown to exhibit either biochemical or clinical resistance to aspirin. Such patients may potentially benefit from dual antiplatelet therapy, with the addition of a thienopyridine. Regardless of aspirin-resistance status, clopidogrel has also been shown to be beneficial when added to aspirin among patients with UA/NSTEMI. The CURE (Clopidogrel in Unstable Angina to Prevent Recurrent Events) study demonstrated a 20% reduction in composite endpoint of nonfatal MI, stroke, and cardiovascular death after 9 months follow-up. Clopidogrel therapy after MI is also indicated for reduction in recurrent events in the setting of coronary stent implantation, based on analysis of the CREDO (Clopidogrel for the Reduction of Events during Observation) trial. Currently, the ACC/AHA recommendation is that patients who are treated medically for MIs be treated with clopidogrel 75 mg daily for at least 1 month and ideally up to 1 year. Patients who undergo percutaneous intervention should continue thienopyridine therapy for at least a year. Based on the recent TRITON TIMI-38 trial which demonstrated superior efficacy of prasugrel over clopidogrel in decreasing ischemic events in patients with ACS, the ACC/AHA guidelines have incorporated the use of prasugrel as an alternative to clopidogrel use. In appropriate patients, a 60 mg loading dose of prasugrel should be given to patients no later than 1 hour after PCI once the coronary anatomy has been established and should be continued at a maintenance dose of 10 mg daily for at least a year. Absolute contraindications to prasugrel include prior stroke or TIA. Patients at increased risk for bleeding on prasugrel include age >75 years and weight <60 kg, and caution is needed before prescribing this medication in these subgroups. In patients with increased risk of bleeding, earlier termination of thienopyridine therapy may be considered.
Of note, ibuprofen may attenuate the beneficial effects of aspirin in patients with cardiovascular disease, and its regular use should be discouraged for patients taking aspirin after MI. In fact, the most recent ACC/AHA guidelines discourage the use of all nonsteroidal anti-inflammatory agents except aspirin during hospitalization for MI due to an increased risk of mortality, reinfarction, hypertension, heart failure, and myocardial rupture. After discharge, patients should substitute nonsteroidal anti-inflammatory drugs (NSAIDs) for an alternative medication such as acetaminophen if available.
Anticoagulation
The primary use of oral anticoagulation (warfarin) in the post-MI patient has been shown to be at least as effective as aspirin in terms of risk reduction for recurrent MI. Its use as a substitute for aspirin is only recommended among aspirin-allergic patients, however, as the difficulty of administering oral anticoagulation and risk for major bleeding makes this a less than optimal alternative. In fact, the use of a thieno-pyridine (clopidogrel) appears more practical than warfarin in aspirin-allergic patients based in part on the CAPRIE trial which demonstrated superior efficacy with clopidogrel over aspirin in preventing vascular outcomes. Combination therapy with aspirin and low-intensity warfarin (INR < 2.0) has not been shown to be superior to aspirin alone. Moderate and high-intensity oral anticoagulation plus aspirin has been shown to reduce subsequent cardiac events over aspirin alone, with increased bleeding risk only among the high-intensity patients. The use of oral anticoagulation with dual antiplatelet therapy has not been extensively studied. Current guidelines suggest considering the use of warfarin in post-MI patients with atrial fibrillation, LV thrombus, or other indication for anticoagulation such as arterial or venous thrombosis. It may also be used for secondary prevention, in combination with aspirin, among patients with LV dysfunction, with or without CHF, and/or extensive regional wall motion abnormalities.
Neurohormonal Blockade
Renin–Angiotensin–Aldosterone System Inhibition
The finding of LV dysfunction after MI is a strong predictor of subsequent mortality. The renin–angiotensin–aldosterone system (RAAS) is pivotal in modulating the extent of post-MI remodeling and LV dysfunction. Pharmacologic agents have been developed to block this critical pathway at various levels. Many well-designed trials have indicated that angiotensin-converting enzyme inhibitor (ACE inhibitor) use can improve long-term survival and attenuate the progression of LV failure and LV dilatation among post-MI patients with LV dysfunction. This is particularly true for patients with large, anterior STEMI. Current ACC/AHA Guidelines for UA/NSTEMI extend a class I indication to their use only to patients with CHF with LV dysfunction, hypertension, or diabetes. This recommendation was initially founded on the results of the HOPE (Heart Outcomes Prevention Evaluation) trial, which evaluated the effect of long-term ACE inhibitors among high-risk patients, many of whom (52%) had a prior MI. This trial found a highly significant reduction in MI, stroke, and cardiovascular mortality among such patients. In addition, subsequent secondary analysis of the initial trials confirmed the extension of benefit to all post-MI patients. Many different ACE inhibitors have been studied, and it does appear that ACE inhibitors demonstrate a “class effect,” leading to no specific recommendation on the brand of ACE inhibitor.
Similar to ACE inhibitors, positive results have been found for the use of angiotensin-receptor blockers (ARBs) in post-MI patients. This class of medications should be provided as an alternative to ACE inhibitors among patients with intolerance or allergy to ACE inhibitors when LV dysfunction or clinical heart failure is present. However, given the extensive clinical experience with ACE inhibitors, and the potential positive effects of ACE inhibitors on the vascular endothelium through the bradykinin pathway, ACE inhibitors remain the first line of therapy in patients without contraindication. The combination of ACE inhibitor (captopril) and ARB (valsartan) has been evaluated in immediately post-MI patients in the VALIANT trial (Valsartan in Acute Myocardial Infarction Trial). In this population, combination ACE inhibitor and ARB did not show any benefit over ACE inhibitor alone or ARB alone, although the combination did have increased adverse effects. Of note, valsartan was roughly equivalent to captopril in outcomes. The CHARM trial (Candesartan in Heart Failure Assessment in Reduction of Mortality) focused on patients with chronic CHF, although 60% of the patients studied had an ischemic etiology. This trial found a small absolute risk reduction with the addition of candesartan to an ACE inhibitor. Based on the findings of these two trials, the combination of ACE inhibitor and ARB can be considered in the long-term management of STEMI patients with persistent symptomatic heart failure and left ventricular ejection fraction (LVEF) < 0.40 (CHARM), but should be avoided in the acute setting (VALIANT).
Finally, aldosterone blockade has been shown to be beneficial in post-MI patients. The RALES trial (Randomized Aldactone Evaluation Study) evaluated patients with New York Heart Association Class III or IV heart failure (55% of patients had ischemic cardiomyopathy) and found a 24% relative risk reduction in all-cause mortality with 25 to 50 mg of spironolactone daily. More recently, the EPHESUS trial (Eplerenone Post–Acute Myocardial Infarction Heart Failure Efficacy and Survival Study) evaluated the use of an aldoster-one-receptor blocker, eplerenone, in acute MI patients with LV dysfunction (EF ≤ 0.40). The patients in this trial received optimal therapy, with reperfusion, aspirin, ACE inhibitor, beta-blockers, and statins. A significant relative risk reduction for all-cause mortality of 15% was seen among patients receiving eplerenone. It is important to note that patients with severe renal impairment (serum creatinine >2.5 mg/dL) or hyperkalemia (serum potassium >5.0 mmol/L) were excluded from this trial. These findings led to the inclusion of aldosterone blocking agents for post-MI patients with an EF < 40% and symptomatic heart failure or diabetes who are already on a therapeutic dose of an ACE inhibitor into the ACC/AHA guidelines with a class I indication.
Beta-Receptor Blockade
Beta-receptor blockade (beta-blockers) has long been considered important in patients with acute MI to reduce myocardial ischemia by decreasing oxygen demand. However, long-term beta-blocker therapy in the convalescent phase of MI has also been demonstrated to be beneficial in numerous trials, as demonstrated in Figure 43.5.
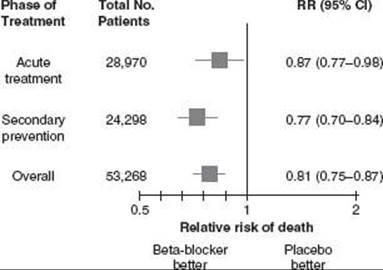
FIGURE 43.5 Summary of data from a meta-analysis of trials of beta- blockers for acute MI. (Reprinted from Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:E1–E211, with permission from Elsevier).
The postulated mechanism of benefit is similar to that seen with the RAAS, which is modulation of LV remodeling and LV dysfunction post-MI. After MI, the sympathetic nervous system has been found to increase infarct size, activate the RAAS, and promote myocyte injury. Oral beta- blockade should be initiated within the first 24 hours post- MI in the absence of signs of heart failure, a low output state, increased risk for cardiogenic shock (age >70, SBP < 120 mm Hg, heart rate >110 or <60 beats/min (bpm), increased time since onset of symptoms), or other relative contraindications to beta blockade (PR interval >240 milliseconds, second- or third-degree heart block, active asthma or reactive airways disease). Intravenous betablocker use is reasonable, but no longer has a class I recommendation level in the guidelines after the COMMIT trial demonstrated an increased risk of cardiogenic shock with IV betablocker use in STEMI patients, The BHAT trial (Beta-Blocker Heart Attack Trial), a prethrombolytic study, compared 180 to 240 mg of propranolol daily to placebo in post-MI patients, finding a 26% relative risk reduction for all-cause mortality, and a 28% reduction in sudden death. Although metoprolol and atenolol are frequently prescribed to post- MI patients, these agents have not been demonstrated to reduce mortality during long-term therapy. The MERIT-HF (Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure) trial evaluated the use of metoprolol in chronic CHF with EF < 40% and found a 33% reduction in mortality. This trial included 66% of patients with ischemic cardiomyopathy. The COMET (Carvedilol or Metoprolol European Trial) compared carvedilol, a nonselective beta-blocker with alpha-blocking capability, with metoprolol in patients with chronic CHF, and found a 17% reduction in the risk of death from carvedilol, relative to metoprolol. More recently, the CAPRICORN trial (Carvedilol Post-Infarct Survival Control in Left Ventricular Dysfunction) tested carvedilol in post-MI patients with significant LV dysfunction (EF ≤ 0.40). This trial found similar reductions in all-cause mortality and sudden death to the BHAT trial. Current ACC/AHA Guidelines support the use of beta blockers indefinitely in all post-MI patients without contraindication, and recommend an approach that incorporates gradual titration in those patients with moderate or severe LV dysfunction.
Lipid Management
Pharmacologic lipid management after MI is crucial for secondary prevention of cardiac events. Patients should have a lipid profile checked prior to hospital discharge after MI and should have statin therapy initiated before leaving the hospital. The National Cholesterol Education Program (NCEP) published guidelines in 2001 (ATP III) for lipid-lowering therapy that encourage the use of therapeutic lifestyle changes” including weight reduction, increased physical activity, increased fiber intake, and reduced intake of saturated fats and cholesterol. The recommended drug therapy for lipid lowering includes statins, bile acid sequestrants, nicotinic acid (niacin), or fibric acids, depending on the patient’s lipid profile and potential side effects.
The ATP III guidelines also established a LDL goal of <100 mg/dL among patients with known cardiovascular disease. However, since publication of that document, several trials have demonstrated that there is added benefit to additional LDL lowering in very-high-risk patients. This finding has led the ACC/AHA Guidelines writers to recommend targeting an LDL goal of “substantially <100 mg/dL” among STEMI patients. The PROVE-IT TIMI 22 (Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22) study was pivotal in the change in recommendation. This trial compared moderate lipid lowering (40 mg of pravastatin) to aggressive lipid lowering (80 mg of atorvastatin) among patients with ACS. The LDL level attained with 40 mg of pravastatin was 95 mg/dL, while 80 mg of atorvastatin resulted in an LDL of 62 mg/dL, representing a 35% difference. The composite cardiovascular endpoint at 2 years was reduced by 16% with atorvastatin (Fig. 43.6).
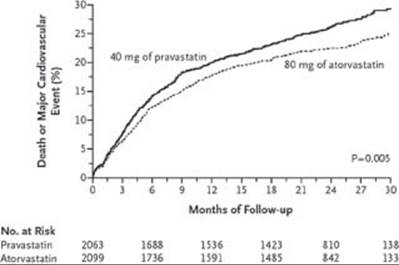
FIGURE 43.6 Kaplan–Meier estimates of the incidence of all-cause mortality in the PROVE-IT TIMI 22 study. (From Cannon C, Braunwald E, McCabe CH, et al. Intensive versus Moderate Lipid Lowering with Statins after Acute Coronary Syndromes. N Engl J Med.2004;350(15):1495–1504, with permission.)
This trial, as well as other recent trials such as MIRACL (Myocardial Ischemia Reduction with Acute Cholesterol Lowering), and Phase Z of the A to Z trial, demonstrates that more intensive LDL lowering does result in additional benefit in high-risk patients. It may be that the additional benefit to aggressive lipid lowering relates to reduction in inflammation, as evidenced by recent data from the REVERSAL (Reversal of Atherosclerosis with Aggressive Lipid Lowering) trial, showing a relationship between progression of atherosclerosis and CRP levels.
Risk-Factor Management
Diabetic patients represent a high-risk subset because of macrovascular and microvascular complications including severe CAD, hypertension, peripheral vascular disease, and renal dysfunction. Prior conventional management of diabetes in the setting of ACS dictated strict management of glucose levels, but recent evidence has suggested potential harm with this strategy. The NICE-SUGAR trial enrolled patients in an ICU setting and demonstrated increased incidence of hypoglycemia and death with an intense glucose control that attempted to keep the glucose level between 81 and 108 mg/dL. Standard therapy allowed for glucose levels up to 180 mg/dL. Similarly, the ACCORD trial demonstrated increased mortality in type 2 diabetics who were assigned to the intensive therapy arm that targeted an A1c level below 6% versus those in the standard therapy group that aimed for A1c levels between 7% and 7.9%. The American Diabetes Association still recommends treating diabetic patients to achieve a target goal A1c of 7% or less, but care should be taken to avoid hypoglycemia.
Besides medical management of hyperglycemia, other clinical trials have shown that combined neurohormonal blockade with ACE inhibitors, aldosterone antagonists, and beta-blockers are essential in treatment of diabetic patients with prior MI, and these medications should be continued with this patient population. There is some concern about beta-blockers masking the symptoms of hypoglycemia in diabetic patients, but they have been shown to be beneficial and should be used with appropriate caution in this high-risk subset.
Hypertension management post-MI is important in risk reduction for subsequent MI. In addition to important lifestyle changes such as weight control, exercise, and sodium restriction, current guidelines state that treatment of BP with drug therapy post-MI should be initiated to reach a target BP of 140/80 for all patients, and 130/80 for diabetics and patients with renal insufficiency. However, it is reasonable to treat all patients post-MI to a target BP of 120/80, considering the high-risk population represented by post-MI patients. These recommendations are based on the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). The same committee recommends the initiation of two agents if the BP is more than 20/10 mm Hg above goal. From a practical perspective, the post-MI patient should already be receiving a beta-blocker and ACE inhibitor for reasons detailed above, especially among patients with LV dysfunction (EF < 40%). Although achieving maximal doses of these medications is essential, the optimal method of reaching target dose is a matter of conjecture. In addition to beta-blockers and ACE inhibitors, thiazide diuretics and long-acting calcium channel antagonists are excellent antihypertensive therapy choices with excellent supporting data from large, multicenter randomized trials, in particular the ALLHAT results (Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial).
Obesity is a major risk factor for coronary disease and should be carefully addressed in the post-MI patient as part of a comprehensive secondary risk-reduction strategy. In particular, body mass index and waist circumference have been shown to be important in risk assessment. The desirable body mass index range is 18.5 to 24.9 kg/m2, and the desired waist circumference is <40 inches in men and 35 inches in women. Overweight patients should be advised regarding weight-management strategies and appropriate levels of physical activity. An initial weight loss of 10% of body weight over 6 months is the recommended target, at 1 to 2 pounds per week. Patients with an elevated waist circumference should be screened for the metabolic syndrome, a significant risk factor for coronary disease. In addition to decreasing caloric intake, patients should participate in aerobic activity, preferably individualized via an exercise prescription, for 30 to 60 minutes a day, at least five times a week. Cardiac rehabilitation has been shown to be beneficial in patients post-MI, especially for those patients with multiple modifiable risk factors and moderate-to high-risk patients that warrant a supervised exercise regimen.
Smoking cessation is a must for every post-MI patient. It is imperative that the treating physician provides adequate counseling and pharmacologic therapy to achieve this goal. Smoking has been shown to trigger coronary spasm, reduce effectiveness of beta-blockers, and increase mortality after STEMI. Patients recovering from MI should be provided with counseling and appropriate pharmacologic therapy. Of note, routine use of nicotine-replacement therapy during hospitalization with acute MI is not recommended because of the potential sympathomimetic effects of nicotine.
CONCLUSION
Risk stratification in MI is essential to determine appropriate therapy, and for allocation of limited health care resources to high-risk patients. In STEMI, the most important predictors of death include age, SBP and heart rate at presentation, CHF, and location of infarction. Early revascularization is critical to reducing the mortality rate. In NSTEMI, high-risk features, such as biomarker elevation or elevated TIMI risk score, can be used to determine which patients should be eligible for an early invasive strategy. Patients who develop evidence of recurrent ischemia or LV dysfunction after MI have a worse prognosis, so the identification of these features is important to guiding predischarge management.
The appropriate use of pharmacotherapy after MI also depends on identification of high-risk features. Under most circumstances, post-MI therapy should include daily aspirin, a statin, a beta-blocker, and clopidogrel (especially if a stent is placed). If significant LV dysfunction is present, an ACE inhibitor and/or ARB, potentially with aldosterone blockade, are needed. Lifestyle modification remains essential to post-MI management, including smoking cessation and control of risk factors such as diabetes, hypertension, and obesity.
SUGGESTED READINGS
Anderson JL, et al. ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction-Executive Summary. J Am Coll Cardiol. 2007;50:652–726.
Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:E1–E211.
Antman EM, Hand M, et al. 2007 Focused Update of the ACC/AHA 2004 Guidelines for the Management of Patients with ST-Elevation Myocardial Infarction. J Am Coll Cardiol. 2008;51:210–247.
Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients with Unstable Angina). J Am Coll Cardiol. 2002;40:1366–1374.
Griffin BP, Topol EJ. Manual of Cardiovascular Medicine. Philadelphia: Lippincott Williams & Wilkins; 2004.
Kushner FG, Hand M, Smith SC, King SB, et al. 2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients with ST-Elevation Myocardial Infarction (Updating the 2004 Guideline and 2007 Focused Update) and the ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (Updating the 2005 Guideline and 2007 Focused Update). J Am Coll Cardiol. 2009;54:2205–2241.
Topol EJ, Califf RM. Textbook of Cardiovascular Medicine. Philadelphia: Lippincott Williams & Wilkins; 2002.
Wright RS, Anderson JL, et al. 2011 ACCF/AHA Focused Update of the Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction (Updating the 2007 Guidelin). J Am Coll Cardiol. 2011;57:1–40.
Zipes DP, Braunwald E. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia: Elsevier Saunders; 2005.
QUESTIONS AND ANSWERS
Questions
1. A 52-year-old man presented to the Emergency Department with an acute anterior wall myocardial infarction (MI) and received successful lytic therapy. Physical exam findings were notable for a systolic blood pressure (SBP) of 90 mm Hg, a heart rate of 120 beats/min (bpm), and rales at both lung bases.The most important determinant of 30-day mortality in this patient is:
a. Age
b. Infarct location
c. Killip class
d. SBP
e. Heart rate
2. The patient in Question 1 had an uncomplicated in-hospital course. All of the following are acceptable risk‐factor stratification strategies except:
a. Assessment of left ventricular (LV) function
b. Predischarge cardiac catheterization
c. Submaximal stress on days 4 to 6
d. Symptom‐limited stress on days 10 to 14
e. Electrophysiology testing
3. The patient in Question 1 has a brief episode of chest pain (<1 minute) with transient ST depression on the morning of his scheduled submaximal stress test.The pain was relieved with one sublingual nitroglycerin tablet.You should:
a. Proceed with submaximal stress as planned.
b. Wait two or three additional days and proceed with stress testing if he remains asymptomatic.
c. Order echocardiography to see if there have been any additional wall motion abnormalities.
d. Schedule for coronary catheterization prior to discharge.
4. BF is a 48-year-old man who presents for a submaximal stress test prior to discharge after successful thrombolysis for an inferior wall MI. His baseline electrocardiogram (ECG) demonstrated a complete left bundle branch block (LBBB) but was unchanged during stress testing. He achieved 5.5 METs and the stress test was stopped because of general fatigue.You are asked to review his stress test and decide to:
a. Discharge the patient home and schedule him for a symptom-limited stress test in 10 to 14 days.
b. Schedule a symptom-limited stress test in 2 to 3 weeks.
c. Perform cardiac catheterization because of the low METs achieved.
d. Repeat the stress test with perfusion imaging secondary to baseline LBBB.
5. JT is a 65-year-old woman who presents with chest pain and her TIMI risk score is 1. She is referred for exercise stress testing. All of the following findings on EKG would preclude her except:
a. Left ventricular hypertrophy (LVH) with strain
b. Ventricular pre-excitation
c. Ventricular paced rhythm
d. Right bundle branch block
6. AH is a 79-year-old male with prior history of coronary artery disease (CAD) and prior stenting 5 years ago. He otherwise has hypertension, but no diabetes, hyperlipidemia, or other medical diagnoses. He has been having exertional chest discomfort twice a day for the last week, and is now admitted to the hospital. His daily medical regimen includes subligual nitroglycerin, metoprolol tartrate, lisinopril, and aspirin. On arrival, his EKG demonstrates ST depression in leads II, III, and F. His cardiac biomarkers are normal. Based on this information, his TIMI risk score is:
a. 5
b. 4
c. 3
d. 2
e. 1
7. Based on this patient’s TIMI risk score, the proper management strategy at this time is:
a. Exercise treadmill stress test if no symptoms of ischemia after 24 hours
b. Exercise stress test with nuclear imaging if no symptoms of ischemia after 24 hours
c. Pharmacologic nuclear stress test if no symptoms of ischemia after 24 hours
d. Dobutamine echo stress test if no symptoms of ischemia after 24 hours
e. Coronary angiography
8. A 74-year-old female presents to the hospital with 3 days of stuttering angina which is new. Her medical history is significant for diabetes, hypertension, hyperlipidemia, chronic kidney disease stage 2, peripheral vascular disease, and a TIA 5 years ago. She is 66 inches tall and weighs 65 kg. Her blood pressure (BP) on admission is 110/70 and her HR is 99 bpm. She is referred for coronary angiography with the intention of PCI. In addition to aspirin, the best option for an oral antiplatelet agent is:
a. Ticlopidine
b. Clopidogrel
c. Prasugrel
d. Cangrelor
9. A 70-year-old patient presents with a non–ST-segment-elevation myocardial infarction (NSTEMI) and undergoes implantation of a bare-metal stent. He is prescribed aspirin, clopidogrel, metoprolol, and atorvastatin. According to the most recent American College of Cardiology/American Heart Association (ACC/AHA) guidelines, the recommended duration for clopidogrel is:
a. 2 weeks
b. 4 weeks
c. 3 months
d. 6 months
e. At least 12 months
10. A 65-year-old patient with hypertension, chronic kidney disease stage 3, hyperlipidemia, and obesity is discharged from the hospital after a NSTEMI. She now presents to your outpatient office. Which of the following are the most appropriate targets for her BP and lipid panel?
a. BP < 145/90 and low-density lipoprotein (LDL) 100 mg/dL or less
b. BP < 140/90 and LDL 100 mg/dL or less
c. BP < 130/80 and LDL 100 mg/dL or less
d. BP < 130/85 and LDL 130 mg/dL
e. BP < 135/80 and LDL 130 mg/dL
Answers
1. Answer A: An analysis of 41,021 patients with acute MI enrolled in GUSTO-I, a trial of lytic therapy, found that age was the most significant predictor of 30-day mortality in a multivariable analysis. In addition, anterior infarct location, higher Killip class, elevated heart rate, and lower SBP were predictors, although they were not as significant as age.Together, these five characteristics included 90% of the prognostic information in the baseline clinical data (Lee et al., Circulation. 1995;91:1659–1668).
2. Answer E: The current ACC/AHA Guidelines for ST-segment-elevation myocardial infarction (STEMI) recommend assessment of LV function as part of a risk-stratification algorithm. It is acceptable to proceed to cardiac catheterization, particularly in patients with EF < 0.40 or with high-risk features. In patients who do not undergo cardiac catheterization, it is recommended that those with an interpretable ECG, and who can exercise, undergo exercise stress testing, either as a submaximal stress test on days 4 to 6 or a symptom-limited test on days 10 to 14. EP testing is not part of the recommended algorithm for risk stratification.
3. Answer D: Recurrent ischemia after MI is a high-risk predictor, and patients with recurrent ischemia should undergo cardiac catheterization and revascularization as indicated.
4. Answer D: LBBB precludes interpretation of a stress ECG and is a contraindication to exercise ECG testing in the absence of nuclear perfusion imaging.
5. Answer D: Baseline ECG abnormalities can preclude ECG stress test interpretation. LVH with strain,WPW, ventricular pacemaker, and baseline ST depression fall into this category. However, the ECG in right bundle branch block (RBBB) is interpretable, as ST segments are generally normal in this condition.
6. Answer A: The TIMI risk score (Entman et al. JAMA.2000; 284: 835–842) is comprised of: age >65 years old, at least three risk factors for CAD, significant coronary stenosis (prior stenosis ≥50%), aspirin use within the last 7 days, severe angina (≥2 episodes per day during the last 24 hours), ST deviation on EKG, and positive cardiac biomarkers. This patient’s score is 5, assuming his prior PCI was performed for a significant coronary stenosis.
7. Answer E: Based on the TIMI risk score, the expected rate of all-cause mortality, MI, and severe recurrent ischemia at 14 days is 26%. Patients with high-risk TIMI scores (≥3) should be referred for coronary angiography over noninvasive stress testing unless there is a contraindication.
8. Answer B: In the TRITON TIMI-38 trial (Wiviott et al. NEJM. 2007;357:2001–2015) subgroups that were at high risk for bleeding included patients older than or equal to 75 years, weight <60 kg, or prior history of TIA or stroke.Ticlopidine is not recommended over clopidogrel due to increased risk of neutropenia and agranulocytosis. Cangrelor is available only as an IV form and is not approved for clinical use.
9. Answer E: The new guidelines published by the ACC/AHA in 2011 recommends that all patients with NSTEMI continue a maintenance dose of clopidogrel 75 mg for at least 12 months unless there is a contraindication or high risk for morbidity or bleeding.
10. Answer C: According to the JNC 7 guidelines on hypertension (JAMA. 2003;289:2560–2572), patients with prior MI should have a BP goal of 140/90 for all patients and 130/80 for patients with diabetes or chronic kidney disease. According to the ATP III guidelines on lipid management (JAMA. 2001;285:2486-2497), patients with known CAD should have a LDL goal of 100 mg/dL or less.