John S. Child ![]() Jamil Aboulhosn
Jamil Aboulhosn
A little over a hundred years ago, Sir William Osler, in his classic textbook The Principles and Practice of Medicine (New York, Appleton & Co, 1892, pp 659–663), devoted only five pages to “Congenital Affections of the Heart,” with the first sentence declaring, that “[t]hese [disorders] have only limited clinical interest, as in a large proportion of cases the anomaly is not compatible with life, and in others nothing can be done to remedy the defect or even to relieve symptoms.” Fortunately, in the intervening century, considerable progress has been made in understanding the basis for these disorders and their effective treatment.
The most common birth defects are cardiovascular in origin. These malformations are due to complex multifactorial genetic and environmental causes, but recognized chromosomal aberrations and mutations of single genes account for <10% of all cardiac malformations. Congenital heart disease (CHD) complicates ~1% of all live births in the general population—about 40,000 births/year—but occurs more frequently in the offspring (about 4–5%) of women with CHD. Owing to the remarkable surgical advances over the last 60 years, >90% of afflicted neonates and children now reach adulthood; women with CHD may now frequently successfully bear children after competent repairs. As such, the population with CHD is steadily increasing. Women with aortic disease (e.g., aortic coarctation or Marfan’s syndrome) risk aortic dissection. Patients with cyanotic heart disease, pulmonary hypertension, or Marfan’s syndrome with a dilated aortic root generally should not become pregnant; those with correctable lesions should be counseled about the risks of pregnancy with an uncorrected malformation versus repair and later pregnancy.
More than 1 million adults with operated or unoperated CHD live in the United States today and, thus, outnumber the 800,000 children with CHD. Because true surgical cures are rare, and all repairs—be they palliative or corrective—may leave residua, sequelae, or complications, most require some degree of lifetime expert surveillance. The anatomic and physiologic changes in the heart and circulation due to any specific CHD lesion are not static but, rather, progress from prenatal life to adulthood. Malformations that are benign or escape detection in childhood may become clinically significant in the adult. For example, a functionally normal congenitally bicuspid aortic valve may thicken and calcify with time, resulting in significant aortic stenosis; a well-tolerated left-to-right shunt of an atrial septal defect (ASD) may result in cardiac decompensation or pulmonary hypertension only after the fourth to fifth decade.
CARDIAC DEVELOPMENT (ALSO SEE CHAPTER 1)
CHD is generally the result of aberrant embryonic development of a normal structure or failure of such a structure to progress beyond an early stage of embryonic or fetal development. This brief section serves to introduce the reader to normal development so that defects may be better understood; by necessity, it is not exhaustive. Cardiogenesis is a finely tuned process with transcriptional control of a complex group of regulatory proteins that activate or inhibit their gene targets in a location- and time-dependent manner. At about 3 weeks of embryonic development, two cardiac cords form and become canalized; at that point, the primordial cardiac tube develops from two sources (cardiac crescent or the first heart field, pharyngeal mesoderm or the second heart field); by 21 days, these fuse into a single cardiac tube beginning at the cranial end. The cardiac tube then elongates and develops discrete constrictions with the following segments from caudal to cranial location: sinus venosus receives the umbilical, vitelline, and common cardinal veins: atrium, ventricle, bulbus cordis, truncus arteriosus, aortic sac, and the aortic arches. The cardiac tube is fixed at the sinus venosus and arterial ends.
Subsequently, in the next few weeks, differential growth of cells causes the tube to elongate and loop as an “S” with the bulboventricular portion moving rightward and the atrium and sinus venosus moving posterior to the ventricle. The primitive atrium and ventricle communicate via the atrioventricular canal from which the endocardial cushion develops into two parts (ventrally and dorsally). The cushions fuse and divide the atrioventricular canal into two atrioventricular inlets and also migrate to help form the ventricular septum. The primitive atrium is divided first by a septum primum membrane, which grows down from the superior wall to the cushions; as this fusion occurs, the midportion resorbs in the center forming the ostium secundum. Rightward of the septum primum, a second septum secundum membrane grows down from the ventral-cranial wall toward—but not reaching—the cushions, and covering most, but not all, of the ostium secundum, resulting in a flap of the foramen ovale. The primitive ventricle is partitioned by a finely tuned set of events. The interventricular septum grows up toward the cushions, and the cushions form an upper inlet septum; between the two portions is a hole called the interventricular foramen. The left and right ventricles begin to develop side by side, and the atria and their respective inlet valves align over their ventricles. Finally, these two parts of the septum fuse with the bulboventricular ridges, which, once having septated the truncus arteriosus, extend into the ventricle. The bulbocordis divides into a subaortic portion as the muscular conus resorbs, while the subpulmonary section has elongation of its muscular conus. Spiral division of the common truncus arteriosus rotates and aligns the pulmonary artery and aortic portions over their respective outflow tracts, the aortic valve moving posterior over the left ventricle (LV) outflow tract and the pulmonary valve moving anterior over the right ventricle (RV) outflow tract, with a wraparound relationship of the two great arteries.
Early on, the venous systems are bilateral and symmetric and enter 2 horns of the sinus venosus. Ultimately, except for the coronary sinus, most of the left-sided portions and the left sinus–venosus horn regress and the systemic venous system empties into the right horn via the inferior and superior vena cavae. The pulmonary venous system, initially connecting to the systemic venous system, develops as buds from the developing lungs fuse together in the pulmonary venous confluence at which point the connection to the systemic system regresses. Simultaneously, a projection from the back wall of the left atrium (the common pulmonary vein) grows posteriorly to merge with the confluence, which then becomes a part of the posterior left atrial wall.
The truncus arteriosus and aortic sac initially develop six paired symmetric arches, which curve posteriorly and become the paired dorsal aortae. The detailed description of the selective regression of some of the arches is not presented in this chapter. In brief summary, this process results in the development of arch 3 as the internal carotid arteries, left arch 4 as the aortic arch and right subclavian artery, and part of arch 6 as the patent ductus arteriosus. The two dorsal thoracic aortae fuse in the abdomen with persistence of the left dorsal aorta.
SPECIFIC CARDIAC DEFECTS
Tables 19-1, 19-2, and 19-3 list CHD malformations as simple, intermediate, or complex. Simple defects generally are single lesions with a shunt or a valvular malformation. Intermediate defects may have two or more simple defects. Complex defects generally have components of an intermediate defect plus more complex cardiac and vascular anatomy, often with cyanosis, and frequently with transposition complexes. The goal of these tables is to suggest when cardiology consultation or advanced CHD specialty care is needed. Patients with complex CHD (which includes most “named” surgeries that usually involve complex CHD) should virtually always be managed in conjunction with an experienced specialty adult CHD center. Patients with intermediate lesions should have an initial consultation and subsequent occasional intermittent follow-up with a cardiologist. Patients with simple lesions often may be managed by a well-informed internist or general cardiologist, although consultation with a specifically trained adult congenital cardiologist is occasionally advisable.
TABLE 19-1
SIMPLE ADULT CONGENITAL HEART DISEASE
TABLE 19-2
INTERMEDIATE COMPLEXITY CONGENITAL HEART DISEASE
ATRIAL SEPTAL DEFECT
ASD is a common cardiac anomaly that may be first encountered in the adult and occurs more frequently in females. Sinus venosus ASD occurs high in the atrial septum near the entry of the superior vena cava into the right atrium and is associated frequently with anomalous pulmonary venous connection from the right lung to the superior vena cava or right atrium. Ostium primum ASDs lie adjacent to the atrioventricular valves, either of which may be deformed and regurgitant. Ostium primum ASDs are common in Down syndrome; the more complex atrioventricular septal defects with a common atrioventricular valve and a posterior defect of the basal portion of the interventricular septum are more typical of this chromosomal defect. The most common ostium secundum ASD involves the fossa ovalis and is midseptal in location; this should not be confused with a patent foramen ovale.
TABLE 19-3
COMPLEX ADULT CONGENITAL HEART DISEASE
Anatomic obliteration of the foramen ovale ordinarily follows its functional closure soon after birth, but residual “probe patency” is a common normal variant; ASD denotes a true deficiency of the atrial septum and implies functional and anatomic patency. The magnitude of the left-to-right shunt depends on the ASD size, ventricular diastolic properties, and the relative impedance in the pulmonary and systemic circulations. The left-to-right shunt causes diastolic overloading of the right ventricle and increased pulmonary blood flow. Patients with ASD are usually asymptomatic in early life, although there may be some physical underdevelopment and an increased tendency for respiratory infections; cardiorespiratory symptoms occur in many older patients. Beyond the fourth decade, a significant number of patients develop atrial arrhythmias, pulmonary arterial hypertension, bidirectional and then right-to-left shunting of blood, and right heart failure. Patients exposed to the chronic environmental hypoxemia of high altitude tend to develop pulmonary hypertension at younger ages. In older patients, left-to-right shunting across the ASD increases as progressive systemic hypertension and/or coronary artery disease (CAD) result in reduced compliance of the left ventricle.
Physical examination
Examination usually reveals a prominent RV impulse and palpable pulmonary artery pulsation. The first heart sound is normal or split, with accentuation of the tricuspid valve closure sound. Increased flow across the pulmonic valve is responsible for a mid-systolic pulmonary outflow murmur. The second heart sound is widely split and is relatively fixed in relation to respiration. A mid-diastolic rumbling murmur, loudest at the fourth intercostal space and along the left sternal border, reflects increased flow across the tricuspid valve. In ostium primum ASD, an apical holosystolic murmur indicates associated mitral or tricuspid regurgitation or a ventricular septal defect (VSD).
These findings are altered when increased pulmonary vascular resistance causes diminution of the left-to-right shunt. Both the pulmonary outflow and tricuspid inflow murmurs decrease in intensity, the pulmonic component of the second heart sound and a systolic ejection sound are accentuated, the two components of the second heart sound may fuse, and a diastolic murmur of pulmonic regurgitation appears. Cyanosis and clubbing accompany the development of a right-to-left shunt (see “Ventricular Septal Defect” later). In adults with an ASD and atrial fibrillation, the physical findings may be confused with mitral stenosis with pulmonary hypertension because the tricuspid diastolic flow murmur and widely split second heart sound may be mistakenly thought to represent the diastolic murmur of mitral stenosis and the mitral “opening snap,” respectively.
Electrocardiogram
In ostium secundum ASD, electrocardiogram (ECG) usually shows right-axis deviation and an rSr′ pattern in the right precordial leads representing enlargement of the RV outflow tract. An ectopic atrial pacemaker or first-degree heart block may occur with the sinus venous ASD. In ostium primum ASD, the RV conduction defect is accompanied by left superior axis deviation and counterclockwise rotation of the frontal plane QRS loop. Varying degrees of RV and right atrial (RA) enlargement or hypertrophy may occur with each type of defect, depending on the height of the pulmonary artery pressure. Chest x-rayshows an enlarged right atrium and right ventricle, and pulmonary artery and its branches; increased pulmonary vascular markings of left-to-right shunt vascularity will diminish if pulmonary vascular disease develops.
Echocardiogram
Echocardiography reveals pulmonary arterial and RV and RA dilatation with abnormal (paradoxical) ventricular septal motion in the presence of a significant right heart volume overload. The ASD may be visualized directly by two-dimensional imaging, color-flow imaging, or echo-contrast. In most institutions, two-dimensional echo-cardiography and Doppler examination have supplanted cardiac catheterization. Transesophageal echocardiography is indicated if the transthoracic echocardiogram is ambiguous, which is often the case with sinus venosus defects, or during catheter device closure (Fig. 19-1). Cardiac catheterization is performed if inconsistencies exist in the clinical data, if significant pulmonary hypertension or associated malformations are suspected, or if CAD is a possibility.
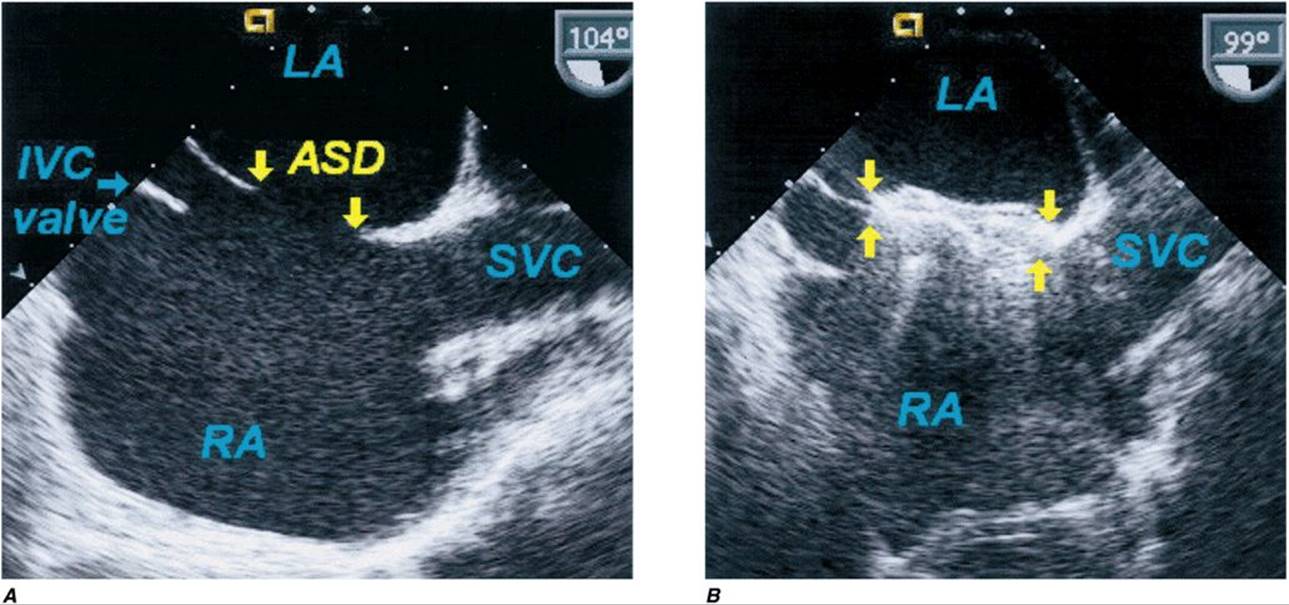
FIGURE 19-1
Secundum atrial septal defect. Transesophageal echocardiogram of secundum ASD and device closure. A. The atrial septal defect (ASD) between the left atrium (LA) and right atrium (RA) is shown. B. A percutaneous catheter–delivered device has occluded the defect. IVC, inferior vena cava; SVC, superior vena cava.
TREATMENT Atrial Septal Defect
Operative repair, usually with a patch of pericardium or of prosthetic material or percutaneous transcatheter device closure, if the ASD is of an appropriate size and shape, should be advised for all patients with uncomplicated secundum ASD with significant left-to-right shunting, i.e., pulmonary-to-systemic flow ratios ≥2:1. Excellent results may be anticipated, at low risk, even in patients >40 years, in the absence of severe pulmonary hypertension. In ostium primum ASD, cleft mitral valves may require repair in addition to patch closure of the ASD. Closure should not be carried out in patients with small defects and trivial left-to-right shunts or in those with severe pulmonary vascular disease without a significant left-to-right shunt.
Patients with sinus venosus or ostium secundum ASDs rarely die before the fifth decade. During the fifth and sixth decades, the incidence of progressive symptoms, often leading to severe disability, increases substantially. Medical management should include prompt treatment of respiratory tract infections; antiarrhythmic medications for atrial fibrillation or supraventricular tachycardia; and the usual measures for hypertension, coronary disease, or heart failure (Chap. 17), if these complications occur. The risk of infective endocarditis is quite low unless the defect is complicated by valvular regurgitation or has recently been repaired with a patch or device (Chap. 25).
Ventricular septal defect
A VSD is one of the most common of all cardiac birth defects, either as isolated defects or as a component of a combination of anomalies. The VSD is usually single and situated in the membranous or midmuscular portion of the septum. The functional disturbance depends on its size and on the status of the pulmonary vascular bed. Only small- or moderate-size VSDs are seen initially in adulthood, as most patients with an isolated large VSD come to medical or surgical attention early in life.
A wide spectrum exists in the natural history of VSD, ranging from spontaneous closure to congestive cardiac failure and death in infancy. Included within this spectrum are the possible development of pulmonary vascular obstruction, RV outflow tract obstruction, aortic regurgitation, or infective endocarditis. Spontaneous closure is more common in patients born with a small VSD, which occurs in early childhood in most. The pulmonary vascular bed is often a principal determinant of the clinical manifestations and course of a given VSD and feasibility of surgical repair. Increased pulmonary arterial pressure results from increased pulmonary blood flow and/or resistance, the latter usually the result of obstructive, obliterative structural changes within the pulmonary vascular bed. It is important to quantitate and compare pulmonary-to-systemic flows and resistances in patients with severe pulmonary hypertension. The term Eisenmenger’s syndrome is applied to patients with a large communication between the two circulations at the aortopulmonary, ventricular, or atrial levels and bidirectional or predominantly right-to-left shunts because of high resistance and obstructive pulmonary hypertension.
Patients with large VSDs and pulmonary hypertension are at greatest risk for developing pulmonary vascular obstruction. Large VSDs should be corrected surgically early in life when pulmonary vascular disease is still reversible or not yet developed. In patients with Eisenmenger syndrome, symptoms in adult life consist of exertional dyspnea, chest pain, syncope, and hemoptysis. The right-to-left shunt leads to cyanosis, clubbing, and erythrocytosis (see later). The degree to which pulmonary vascular resistance is elevated before operation is a critical factor determining prognosis. If the pulmonary vascular resistance is one-third or less of the systemic value, progression of pulmonary vascular disease after operation is unusual; however, if a moderate to severe increase in pulmonary vascular resistance exists preoperatively, either no change or a progression of pulmonary vascular disease is common postoperatively. Pregnancy is contraindicated in Eisenmenger syndrome. The mother’s health is most at risk if she has a cardiovascular lesion associated with pulmonary vascular disease and pulmonary hypertension (e.g., Eisenmenger physiology or mitral stenosis) or LV outflow tract obstruction (e.g., aortic stenosis), but she is also at risk of death with any malformation that may cause heart failure or a hemodynamically important arrhythmia. The fetus is most at risk with maternal cyanosis, heart failure, or pulmonary hypertension.
RV outflow tract obstruction develops in ~5–10% of patients who present in infancy with a moderate to large left-to-right shunt. With time, as subvalvular RV outflow tract obstruction progresses, the findings in these patients whose VSD remains sizable begin to resemble more closely those of the cyanotic tetralogy of Fallot. In ~5% of patients, aortic valve regurgitation results from insufficient cusp tissue or prolapse of the cusp through the interventricular defect; the aortic regurgitation then complicates and dominates the clinical course. Two-dimensional echocardiography with spectral and color Doppler examination defines the number and location of defects in the ventricular septum and associated anomalies and the hemodynamic physiology of the defect(s). Hemodynamic and angiographic study may be occasionally required to assess the status of the pulmonary vascular bed and clarify details of the altered anatomy.
TREATMENT Ventricular Septal Defect
Surgery is not recommended for patients with normal pulmonary arterial pressures with small shunts (pulmonary-to-systemic flow ratios of <1.5 to 2:1). Operative correction or transcatheter closure is indicated when there is a moderate to large left-to-right shunt with a pulmonary-to-systemic flow ratio >1.5:1 or 2:1, in the absence of prohibitively high levels of pulmonary vascular resistance.
In the Eisenmenger VSD patient, pulmonary arterial vasodilators and both single-lung transplantation with intracardiac defect repair and total heart-lung transplantation show promise for improvement in symptoms (Chap. 18). Chronic hypoxemia in cyanotic CHD results in secondary erythrocytosis due to increased erythropoietin production (Chap. 6). The term polycythemia is a misnomer; white cell counts are normal and platelet counts are normal to decreased. Compensated erythrocytosis with iron-replete equilibrium hematocrits rarely result in symptoms of hyperviscosity at hematocrits < 65% and occasionally not even with hematocrits ≥70%. For this reason, therapeutic phlebotomy is rarely required in compensated erythrocytosis. In contrast, patients with decompensated erythrocytosis fail to establish equilibrium with unstable, rising hematocrits and recurrent hyperviscosity symptoms. Therapeutic phlebotomy, a two-edged sword, allows temporary relief of symptoms but limits oxygen delivery, begets instability of the hematocrit, and compounds the problem by iron depletion. Irondeficiency symptoms are usually indistinguishable from those of hyperviscosity; progressive symptoms after recurrent phlebotomy are usually due to iron depletion with hypochromic microcytosis. Iron depletion results in a larger number of smaller (microcytic) hypochromic red cells that are less capable of carrying oxygen and less deformable in the microcirculation; with more of them relative to plasma volume, viscosity is greater than for an equivalent hematocrit with fewer, larger, iron-replete, deformable cells. As such, iron-depleted erythrocytosis results in increasing symptoms due to decreased oxygen delivery to the tissues.
Hemostasis is abnormal in cyanotic CHD, due, in part, to the increased blood volume and engorged capillaries, abnormalities in platelet function, and sensitivity to aspirin or nonsteroidal anti-inflammatory agents, as well as abnormalities of the extrinsic and intrinsic coagulation system. Oral contraceptives are often contraindicated for cyanotic women because of the enhanced risk of vascular thrombosis. Adults with cyanotic CHD do not appear to be at increased risk for stroke unless there are excessive injudicious phlebotomies, inappropriate use of aspirin or anticoagulants, or the presence of atrial arrhythmias or infective endocarditis. Symptoms of hyperviscosity can be produced in any cyanotic patient with erythrocytosis if dehydration reduces plasma volume. Phlebotomy for symptoms of hyperviscosity not due to dehydration or iron deficiency is a simple outpatient removal of 500 mL of blood over 45 min with isovolumetric replacement with isotonic saline. Acute phlebotomy without volume replacement is contraindicated. Iron repletion in decompensated iron-depleted erythrocytosis reduces iron-deficiency symptoms, but must be done gradually to avoid an excessive rise in hematocrit and resulting hyperviscosity.
Patent ductus arteriosus
The ductus arteriosus is a vessel leading from the bifurcation of the pulmonary artery to the aorta just distal to the left subclavian artery. Normally, the vascular channel is open in the fetus but closes immediately after birth. The flow across the ductus is determined by the pressure and resistance relationships between the systemic and pulmonary circulations and by the cross-sectional area and length of the ductus. In most adults with this anomaly, pulmonary pressures are normal and a gradient and shunt from aorta to pulmonary artery persist throughout the cardiac cycle, resulting in a characteristic thrill and a continuous “machinery” murmur with late systolic accentuation at the upper left sternal edge. In adults who were born with a large left-to-right shunt through the ductus arteriosus, pulmonary vascular obstruction (Eisenmenger syndrome) with pulmonary hypertension, right-to-left shunting, and cyanosis have usually developed. Severe pulmonary vascular disease results in reversal of flow through the ductus; unoxygenated blood is shunted to the descending aorta; and the toes—but not the fingers—become cyanotic and clubbed, a finding termed differential cyanosis. The leading causes of death in adults with patent ductus are cardiac failure and infective endocarditis; occasionally severe pulmonary vascular obstruction may cause aneurysmal dilatation, calcification, and rupture of the ductus.
TREATMENT Patent Ductus Arteriosus
In the absence of severe pulmonary vascular disease and predominant left-to-right shunting of blood, the patent ductus should be surgically ligated or divided. Transcatheter closure using coils, buttons, plugs, and umbrellas has become commonplace for appropriately shaped defects. Thoracoscopic surgical approaches are considered experimental. Operation should be deferred for several months in patients treated successfully for infective endocarditis because the ductus may remain somewhat edematous and friable.
Aortic root–to-right-heart shunts
The three most common causes of aortic root–to-right-heart shunts are congenital aneurysm of an aortic sinus of Valsalva with fistula, coronary arteriovenous fistula, and anomalous origin of the left coronary artery from the pulmonary trunk. Aneurysm of an aortic sinus of Valsalva consists of a separation or lack of fusion between the media of the aorta and the annulus of the aortic valve. Rupture usually occurs in the third or fourth decade of life; most often, the aorticocardiac fistula is between the right coronary cusp and the right ventricle; but occasionally, when the noncoronary cusp is involved, the fistula drains into the right atrium. Abrupt rupture causes chest pain, bounding pulses, a continuous murmur accentuated in diastole, and volume overload of the heart. Diagnosis is confirmed by two-dimensional and Doppler echocardiographic studies; cardiac catheterization quantitates the left-to-right shunt, and thoracic aortography visualizes the fistula. Medical management is directed at cardiac failure, arrhythmias, or endocarditis. At operation, the aneurysm is closed and amputated, and the aortic wall is reunited with the heart, either by direct suture or with a patch or prosthesis.
Coronary arteriovenous fistula, an unusual anomaly, consists of a communication between a coronary artery and another cardiac chamber, usually the coronary sinus, right atrium, or right ventricle. The shunt is usually of small magnitude and myocardial blood flow is not usually compromised; if the shunt is large, there may be a coronary “steal” syndrome with myocardial ischemia and possible angina or ventricular arrhythmias. Potential complications include infective endocarditis; thrombus formation with occlusion or distal embolization with myocardial infarction; rupture of an aneurysmal fistula; and, rarely, pulmonary hypertension and congestive failure. A loud, superficial, continuous murmur at the lower or midsternal border usually prompts a further evaluation of asymptomatic patients. Doppler echocardiography demonstrates the site of drainage; if the site of origin is proximal, it may be detectable by two-dimensional echocardiography. Angiography (classic catheterization, CT, or magnetic resonance angiography) permits identification of the size and anatomic features of the fistulous tract, which may be closed by suture or transcatheter obliteration.
The third anomaly causing a shunt from the aortic root to the right heart is anomalous origin of the left coronary artery from the pulmonary artery. Myocardial infarction and fibrosis commonly lead to death within the first year, although up to 20% of patients survive to adolescence and beyond without surgical correction. The diagnosis is supported by the ECG findings of an anterolateral myocardial infarction and left ventricular hypertrophy (LVH). Operative management of adults consists of coronary artery bypass with an internal mammary artery graft or saphenous vein–coronary artery graft.
Congenital aortic stenosis
Malformations that cause obstruction to LV outflow include congenital valvular aortic stenosis, discrete subaortic stenosis, or supravalvular aortic stenosis. Bicuspid aortic valves are more common in males than in females. The congenital bicuspid aortic valve, which may initially be functionally normal, is one of the most common congenital malformations of the heart and may go undetected in early life. Because bicuspid valves may develop stenosis or regurgitation with time or be the site of infective endocarditis, the lesion may be difficult to distinguish in older adults from acquired rheumatic or degenerative calcific aortic valve disease. The dynamics of blood flow associated with a congenitally deformed, rigid aortic valve commonly lead to thickening of the cusps and, in later life, to calcification. Hemodynamically significant obstruction causes concentric hypertrophy of the LV wall. The ascending aorta is often dilated, misnamed “poststenotic” dilatation; this is due to histologic abnormalities of the aortic media similar to those in Marfan’s syndrome and may result in aortic dissection. Diagnosis is made by echocardiography, which reveals the morphology of the aortic valve and aortic root and quantitates severity of stenosis or regurgitation. The clinical manifestations and hemodynamic abnormalities are discussed in Chap. 20.
TREATMENT Valvular Aortic Stenosis
Medical management includes prophylaxis against infective endocarditis and, in patients with diminished cardiac reserve, the administration of digoxin and diuretics and sodium restriction while awaiting operation. A dilated aortic root may require beta blockers. Aortic valve replacement is indicated in adults with critical obstruction, i.e., with an aortic valve area <0.45 cm2/m2, with symptoms secondary to LV dysfunction or myocardial ischemia, or with hemodynamic evidence of LV dysfunction. In asymptomatic children or adolescents or young adults with critical aortic stenosis without valvular calcification or these features, aortic balloon valvuloplasty is often useful (Chap. 36). If surgery is contraindicated in older patients because of a complicating medical problem such as malignancy or renal or hepatic failure, balloon valvuloplasty may provide short-term improvement. This procedure may serve as a bridge to aortic valve replacement in patients with severe heart failure.
![]() Subaortic stenosis
Subaortic stenosis
The discrete form of subaortic stenosis consists of a membranous diaphragm or fibromuscular ring encircling the LV outflow tract just beneath the base of the aortic valve. The jet impact from the subaortic stenotic jet on the underside of the aortic valve often begets progressive aortic valve fibrosis and valvular regurgitation. Echocardiography demonstrates the anatomy of the subaortic obstruction; Doppler studies show turbulence proximal to the aortic valve and can quantitate the pressure gradient and severity of aortic regurgitation. Treatment consists of complete excision of the membrane or fibromuscular ring.
![]() Supravalvular aortic stenosis
Supravalvular aortic stenosis
This is a localized or diffuse narrowing of the ascending aorta originating just above the level of the coronary arteries at the superior margin of the sinuses of Valsalva. In contrast to other forms of aortic stenosis, the coronary arteries are subjected to elevated systolic pressures from the left ventricle, are often dilated and tortuous, and are susceptible to premature atherosclerosis. In most patients, a genetic defect for the anomaly is located in the same chromosomal region as elastin on chromosome 7. Supravalvular aortic stenosis is the most commonly associated cardiac defect in Williams-Beuren syndrome, typically comprising the following: “elfin” facies, low nasal bridge, cheerful demeanor, mental retardation with retained language skills and love of music, supravalvular aortic stenosis, and transient hypercalcemia.
Coarctation of the aorta
Narrowing or constriction of the lumen of the aorta may occur anywhere along its length but is most common distal to the origin of the left subclavian artery near the insertion of the ligamentum arteriosum. Coarctation occurs in ~7% of patients with congenital heart disease, is more common in males than females, and is particularly frequent in patients with gonadal dysgenesis (e.g., Turner syndrome). Clinical manifestations depend on the site and extent of obstruction and the presence of associated cardiac anomalies; most commonly a bicuspid aortic valve. Circle of Willis aneurysms may occur in up to 10%, and pose a high risk of sudden rupture and death.
Most children and young adults with isolated, discrete coarctation are asymptomatic. Headache, epistaxis, cold extremities, and claudication with exercise may occur, and attention is usually directed to the cardiovascular system when a heart murmur or hypertension in the upper extremities and absence, marked diminution, or delayed pulsations in the femoral arteries are detected on physical examination. Enlarged and pulsatile collateral vessels may be palpated in the intercostal spaces anteriorly, in the axillae, or posteriorly in the interscapular area. The upper extremities and thorax may be more developed than the lower extremities. A mid-systolic murmur over the left interscapular space may become continuous if the lumen is narrowed sufficiently to result in a high-velocity jet across the lesion throughout the cardiac cycle. Additional systolic and continuous murmurs over the lateral thoracic wall may reflect increased flow through dilated and tortuous collateral vessels. The ECG usually reveals LV hypertrophy. Chest x-ray may show a dilated left subclavian artery high on the left mediastinal border and a dilated ascending aorta. Indentation of the aorta at the site of coarctation and pre- and poststenotic dilatation (the “3” sign) along the left paramediastinal shadow are essentially pathognomonic. Notching of the third to ninth ribs, an important radiographic sign, is due to inferior rib erosion by dilated collateral vessels (Figs. 19-2 and 19-3). Two-dimensional echocardiography from suprasternal windows identifies the site of coarctation; Doppler quantitates the pressure gradient. Transesophageal echocardiography and MRI or three-dimensional CT allow visualization of the length and severity of the obstruction and associated collateral arteries (Figs. 19-2 and 19-3). In adults, cardiac catheterization is indicated primarily to evaluate the coronary arteries or to perform catheter-based intervention (angioplasty and stent of the coarctation).
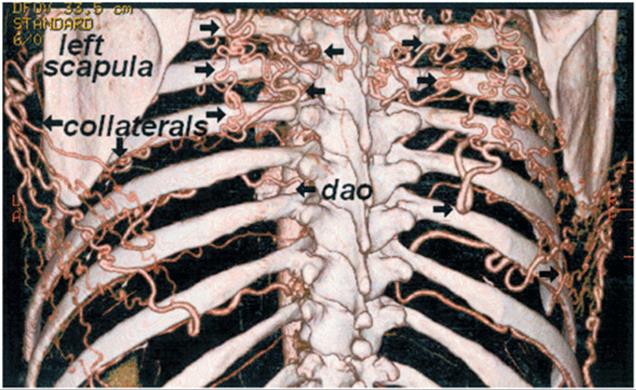
FIGURE 19-2
Aortic coarctation. The extensive collaterals (left) underneath the ribs and in the periscapular region are shown on a posterior view of a three-dimensional CT angiogram, which are responsible for rib notching on chest x-ray. dao, descending aorta.
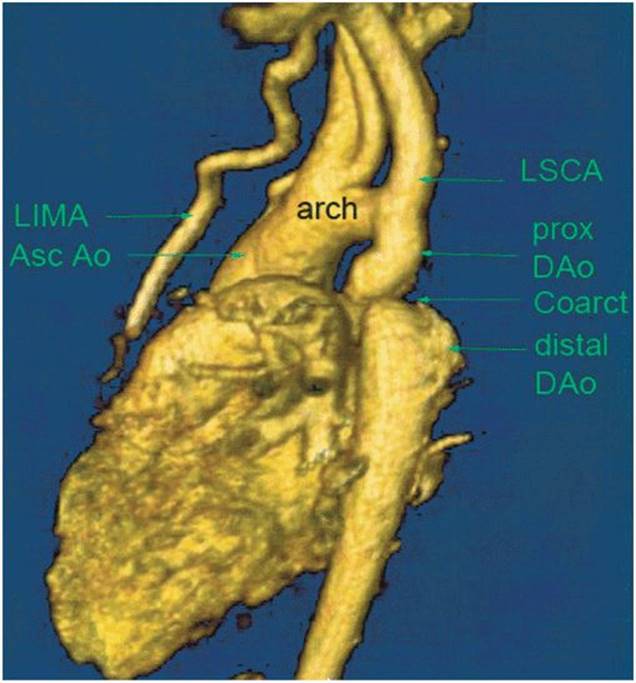
FIGURE 19-3
Aortic coarctation. The coarctation (Coarct) of the aorta is shown in the typical “adult” location in the descending aorta (DAo) just distal to the dilated left subclavian artery (LSCA) in this three-dimensional reconstruction of an MR angiogram. There is a post-coarct aneurysm that is in part due to intrinsic aortic medial tissue weakness. The left internal mammary artery (LIMA) is dilated. Asc Ao, ascending aorta; prox, proximal.
The chief hazards of proximal aortic severe hypertension include cerebral aneurysms and hemorrhage, aortic dissection and rupture, premature coronary arteriosclerosis, and LV failure; infective endarteritis may occur on the coarctation site or endocarditis may settle on an associated bicuspid aortic valve, which is estimated to be present in up to 75% of patients.
TREATMENT Coarctation of the Aorta
Treatment is surgical or involves percutaneous catheter balloon dilatation with stent placement; the details of selection of therapy are beyond this review. Late postoperative systemic hypertension in the absence of residual coarctation is related partly to the duration of preoperative hypertension. Follow-up of rest and exercise blood pressures is important; many have systolic hypertension only during exercise, in part due to a diffuse vasculopathy. All operated or stented coarctation patients deserve a high-quality MRI or CT procedure in follow-up.
Pulmonary stenosis with intact ventricular septum
Obstruction to RV outflow may be localized to the supravalvular, valvular, or subvalvular levels or occur at a combination of these sites. Multiple sites of narrowing of the peripheral pulmonary arteries are a feature of rubella embryopathy and may occur with both the familial and sporadic forms of supravalvular aortic stenosis. Valvular pulmonic stenosis (PS) is the most common form of isolated RV obstruction.
The severity of the obstructing lesion, rather than the site of narrowing, is the most important determinant of the clinical course. In the presence of a normal cardiac output, a peak systolic pressure gradient <30 mmHg indicates mild PS and >50 mmHg indicates severe PS; processes between these limits are considered to indicate moderate stenosis. Patients with mild PS are generally asymptomatic and demonstrate little or no progression in the severity of obstruction with age. In patients with more significant stenosis, the severity may increase with time. Symptoms vary with the degree of obstruction. Fatigue, dyspnea, RV failure, and syncope may limit the activity of older patients, in whom moderate or severe obstruction may prevent an augmentation of cardiac output with exercise. In patients with severe obstruction, the systolic pressure in the RV may exceed that in the LV, because the ventricular septum is intact. RV ejection is prolonged with moderate or severe stenosis, and the sound of pulmonary valve closure is delayed and soft. RV hypertrophy reduces the compliance of that chamber, and a forceful RA contraction is necessary to augment RV filling. A fourth heart sound; prominent a waves in the jugular venous pulse; and, occasionally, presystolic pulsations of the liver reflect vigorous atrial contraction. The clinical diagnosis is supported by a left parasternal lift and harsh systolic crescendo-decrescendo murmur and thrill at the upper left sternal border, typically preceded by a systolic ejection sound if the obstruction is due to a mobile nondysplastic pulmonary valve. The holosystolic murmur of tricuspid regurgitation may accompany severe PS, especially in the presence of congestive heart failure. Cyanosis usually reflects right-to-left shunting through a patent foramen ovale or ASD. In patients with supravalvular or peripheral pulmonary arterial stenosis, the murmur is systolic or continuous and is best heard over the area of narrowing, with radiation to the peripheral lung fields.
In mild cases, the ECG is normal, whereas moderate and severe stenoses are associated with RV hypertrophy. The chest x-ray with mild or moderate PS shows a heart of normal size with normal lung vascularity. In pulmonary valvular stenosis, dilatation of the main and left pulmonary arteries occurs in part due to the direction of the PS jet and in part due to intrinsic tissue weakness. With severe obstruction, RV hyper-trophy is generally evident. The pulmonary vascularity may be reduced with severe stenosis, RV failure, and/or a right-to-left shunt at the atrial level. Two-dimensional echocardiography visualizes pulmonary-valve morphology; the outflow tract pressure gradient is quantitated by Doppler echocardiography.
TREATMENT Pulmonary Stenosis
The cardiac catheter technique of balloon valvuloplasty (Chap. 13) is usually effective. Direct surgical relief of moderate and severe obstruction may be accomplished at a low risk. Multiple stenoses of the peripheral pulmonary arteries are usually inoperable, but narrowing of a proximal branch or at the bifurcation of the main pulmonary trunk may be surgically corrected or undergo balloon dilatation and stenting.
Tetralogy of Fallot
The four components of the tetralogy of Fallot are malaligned VSD, obstruction to RV outflow, aortic override of the VSD, and RV hypertrophy due to the RV’s response to aortic pressure via the large VSD (Fig. 19-4).
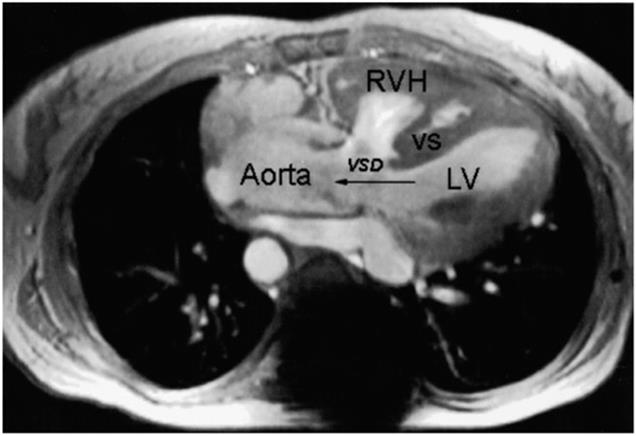
FIGURE 19-4
Tetralogy of Fallot. Magnetic resonance angiogram. A midsystolic frame showing the malaligned ventricular septal defect (VSD) with the aorta overriding the ventricular septal defect. LV, left ventricle; RVH, RV hypertrophy; VS, ventricular septum.
The severity of RV outflow obstruction determines the clinical presentation. The severity of hypoplasia of the RV outflow tract varies from mild to complete (pulmonary atresia). Pulmonary valve stenosis and supravalvular and peripheral pulmonary arterial obstruction may coexist; rarely, there is unilateral absence of a pulmonary artery (usually the left). A right-sided aortic arch and descending thoracic aorta occur in ~25%.
The relationship between the resistance of blood flow from the ventricles into the aorta and into the pulmonary artery plays a major role in determining the hemodynamic and clinical picture. When the RV outflow obstruction is severe, pulmonary blood flow is reduced markedly, and a large volume of desaturated systemic venous blood shunts right-to-left across the VSD. Severe cyanosis and erythrocytosis occur, and symptoms of systemic hypoxemia are prominent. In many infants and children, the obstruction is mild but progressive.
The ECG shows RV hypertrophy. Chest x-ray shows a normal-sized, boot-shaped heart (coeur en sabot) with a prominent right ventricle and a concavity in the region of the pulmonary conus. Pulmonary vascular markings are typically diminished, and the aortic arch and knob may be on the right side. Two-dimensional echocardiography demonstrates the malaligned VSD with the overriding aorta and the site and severity of PS, which may be subpulmonic (fixed or dynamic), at the pulmonary valve or in the main or branch pulmonary arteries. Classic contrast angiography may provide details regarding the RV outflow tract, pulmonary valve and annulus, and caliber of the main branches of the pulmonary artery as well of possible associated aortopulmonary collaterals. Coronary arteriography identifies the anatomy and course of the coronary arteries. In experienced centers, these issues are often well demonstrated in adults by MRI (Fig. 19-4) or CT angiography with three-dimensional reconstruction.
TREATMENT Tetralogy of Fallot
For a variety of reasons, only a few adults with tetralogy of Fallot have not had some form of previous surgical intervention. Reoperation in adults is most commonly for severe pulmonary regurgitation. Long-term concerns about ventricular function persist. Ventricular and atrial arrhythmias may require medical treatment or electrophysiologic study and ablation. Interventional catheterization may be needed in selected patients (i.e., angioplasty and stenting of branch pulmonary stenosis). The aortic root has a medial tissue defect; it is commonly enlarged and associated with aortic regurgitation. Endocarditis remains a risk despite surgical repair.
Complete transposition of the great arteries
This condition is commonly called dextro- or D-transposition of the great arteries. The aorta arises rightward anteriorly from the right ventricle, and the pulmonary artery emerges leftward and posteriorly from the LV, which results in two separate parallel circulations; some communication between them must exist after birth to sustain life. Most patients have an interatrial communication, two-thirds have a patent ductus arteriosus, and about one-third have an associated VSD. Transposition is more common in males and accounts for ~10% of cyanotic heart disease. The course is determined by the degree of tissue hypoxemia, the ability of each ventricle to sustain an increased workload in the presence of reduced coronary arterial oxygenation, the nature of the associated cardiovascular anomalies, and the status of the pulmonary vascular bed. By the third decade of life, ~30% of patients will have developed decreased RV function and progressive tricuspid regurgitation, which may lead to congestive heart failure. Pulmonary vascular obstruction develops by 1 to 2 years of age in patients with an associated large VSD or large patent ductus arteriosus in the absence of obstruction to LV outflow.
TREATMENT Transposition of the Great Arteries
The balloon or blade catheter or surgical creation or enlargement of an interatrial communication in the neonate is the simplest procedure for providing increased intracardiac mixing of systemic and pulmonary venous blood. Systemic pulmonary–artery anastomosis may be indicated in the patient with severe obstruction to LV outflow and diminished pulmonary blood flow. Intracardiac repair may be accomplished by rearranging the venous returns (intraatrial switch, i.e., Mustard or Senning operation) so that the systemic venous blood is directed to the mitral valve and, thence, to the left ventricle and pulmonary artery, while the pulmonary venous blood is diverted through the tricuspid valve and right ventricle to the aorta. The late survival after these repairs is good, but arrhythmias (e.g., atrial flutter) or conduction defects (e.g., sick sinus syndrome) occur in ~50% of such patients by 30 years after the intraatrial switch surgery. Progressive dysfunction of the systemic subaortic right ventricle, tricuspid regurgitation, ventricular arrhythmias, or cardiac arrest and late sudden death are worrisome features. Preferably, this malformation is corrected in infancy by transposing both coronary arteries to the posterior artery and transecting, contraposing, and anastomosing the aorta and pulmonary arteries (arterial-switch operation). For those patients with a VSD in whom it is necessary to bypass a severely obstructed LV outflow tract, corrective operation employs an intracardiac ventricular baffle and extracardiac prosthetic conduit to replace the pulmonary artery (Rastelli procedure).
Single ventricle
This is a family of complex lesions with both atrioventricular valves or a common atrioventricular valve opening to a single ventricular chamber. Associated anomalies include abnormal great artery positional relationships, pulmonic valvular or subvalvular stenosis, and subaortic stenosis. Survival to adulthood depends on a relatively normal pulmonary blood flow, yet normal pulmonary resistance and good ventricular function. Modifications of the Fontan approach are generally applied to carefully selected patients with creation of a pathway(s) from the systemic veins to the pulmonary arteries.
Tricuspid atresia
This malformation is characterized by atresia of the tricuspid valve; an interatrial communication; and, frequently, hypoplasia of the right ventricle and pulmonary artery. The clinical picture is usually dominated by severe cyanosis due to obligatory admixture of systemic and pulmonary venous blood in the left ventricle. The ECG characteristically shows RA enlargement, left-axis deviation, and LV hypertrophy.
Atrial septostomy and palliative operations to increase pulmonary blood flow, often by anastomosis of a systemic artery or vein to a pulmonary artery, may allow survival to the second or third decade. A Fontan atriopulmonary or total cavopulmonary connection may then allow functional correction in those patients with normal or low pulmonary arterial resistance pressure and good LV function.
Ebstein’s anomaly
Characterized by a downward displacement of the tricuspid valve into the right ventricle, due to anomalous attachment of the tricuspid leaflets, the Ebstein tricuspid valve tissue is dysplastic and results in tricuspid regurgitation. The abnormally situated tricuspid orifice produces an “atrialized” portion of the RV lying between the atrioventricular ring and the origin of the valve, which is continuous with the RA chamber. Often, the RV is hypoplastic. Although the clinical manifestations are variable, some patients come to initial attention because of either (1) progressive cyanosis from right-to-left atrial shunting, (2) symptoms due to tricuspid regurgitation and RV dysfunction, or (3) paroxysmal atrial tachyarrhythmias with or without atrioventricular bypass tracts (Wolff-Parkinson-White [WPW] syndrome). Diagnostic findings by two-dimensional echo-cardiography include the abnormal positional relation between the tricuspid and mitral valves with abnormally increased apical displacement of the septal tricuspid leaflet. Tricuspid regurgitation is quantitated by Doppler examination. Surgical approaches include prosthetic replacement of the tricuspid valve when the leaflets are tethered or repair of the native valve.
Congenitally corrected transposition
The two fundamental anatomic abnormalities in this malformation are transposition of the ascending aorta and pulmonary trunk and inversion of the ventricles. This arrangement results in desaturated systemic venous blood passing from the right atrium through the mitral valve to the LV and into the pulmonary trunk, whereas oxygenated pulmonary venous blood flows from the left atrium through the tricuspid valve to the RV and into the aorta. Thus, the circulation is corrected functionally. The clinical presentation, course, and prognosis of patients with congenitally corrected transposition vary depending on the nature and severity of any complicating intracardiac anomalies and of development of dysfunction of the systemic subaortic RV. Progressive RV dysfunction and tricuspid regurgitation may also develop in one-third of patients by age 30; Ebsteintype anomalies of the left-side tricuspid atrioventricular valve are common. VSD or PS due to obstruction to outflow from the right-sided subpulmonary (anatomic left) ventricle may coexist. Complete heart block occurs at a rate of 2–10% per decade. The diagnosis of the malformation and associated lesions can be established by comprehensive two-dimensional echocardiography and Doppler examination.
Malpositions of the heart
Positional anomalies refer to conditions in which the cardiac apex is in the right side of the chest (dextrocardia), or at the midline (mesocardia), or in which there is a normal location of the heart in the left side of the chest but abnormal position of the viscera (isolated levocardia). Knowledge of the position of the abdominal organs and of the branching pattern of the main stem bronchi is important in categorizing these malpositions. When dextrocardia occurs without situs inversus, when the visceral situs is indeterminate, or if isolated levocardia is present, associated, often complex, multiple cardiac anomalies are usually present. In contrast, mirror-image dextrocardia is usually observed with complete situs inversus, which occurs most frequently in individuals whose hearts are otherwise normal.
SURGICALLY MODIFIED CONGENITAL HEART DISEASE
Owing to the enormous strides in cardiovascular surgical techniques that have occurred in the past 60 years, a large number of long-term survivors of corrective operations in infancy and childhood have reached adulthood. These patients are often challenging because of the diversity of anatomic, hemodynamic, and electrophysiologic residua and sequelae of cardiac operations.
The proper care of the survivor of operation for CHD requires that the clinician understand the details of the malformation before operation; pay meticulous attention to the details of the operative procedure; and recognize the postoperative residua (conditions left totally or partially uncorrected), the sequelae (conditions caused by surgery), and the complications that may have resulted from the operation. Except for ligation of an uncomplicated patent ductus arteriosus, almost every other surgical repair leaves behind or causes some abnormality of the heart and circulation that may range from trivial to serious. Intraoperative transesophageal echocardiography assists in detecting unsuspected lesions, in monitoring the repair, and in verifying a satisfactory result or directing further repair. Thus, even with results that are considered clinically to be good to excellent, continued long-term postoperative follow-up is advisable.
Cardiac operations importantly involving the atria, such as closure of ASD, repair of total or partial anomalous pulmonary venous return, or venous switch corrections of complete transposition of the great arteries (the Mustard or Senning operations), may be followed years later by sinus node or atrioventricular node dysfunction or by atrial arrhythmias (especially atrial flutter). Intraventricular surgery may also result in electrophysiologic consequences, including complete heart block necessitating pacemaker insertion to avoid sudden death. Valvular problems may arise late after initial cardiac operation. An example is the progressive stenosis of an initially nonobstructive bicuspid aortic valve in the patient who underwent aortic coarctation repair. Such aortic valves may also be the site of infective endocarditis. After repair of the ostium primum ASD, the cleft mitral valve may become progressively regurgitant. Tricuspid regurgitation may also be progressive in the postoperative patient with tetralogy of Fallot if RV outflow tract obstruction was not relieved adequately at initial surgery. In many patients with surgically modified CHD, inadequate relief of an obstructive lesion, or a residual regurgitant lesion, or a residual shunt will cause or hasten the onset of clinical signs and symptoms of myocardial dysfunction. Despite a good hemodynamic repair, many patients with a subaortic RV develop RV decompensation and signs of left heart failure. In many patients, particularly those who were cyanotic for many years before operation, a preexisting compromise in ventricular performance is due to the original underlying malformation.
A final category of postoperative problems involves the use of prosthetic valves, patches, or conduits in the operative repair. The special risks include infective endocarditis, thrombus formation, and premature degeneration and calcification of the prosthetic materials. There are many patients in whom extracardiac conduits are required to correct the circulation functionally and often to carry blood to the lungs from the right atrium or right ventricle. These conduits may develop intraluminal obstruction, and, if they include a prosthetic valve, it may show progressive calcification and thickening. Many such patients face reintervention (interventional cardiac catheterization or surgical reoperation) one or more times in their lives. Such care should be directed to centers specializing in adults with complex congenital cardiovascular malformations. The effect of pregnancy in postoperative patients depends on the outcome of the repair, including the presence and severity of residua, sequelae, or complications. Contraception is an important topic with such patients. Tubal ligation should be considered in those in whom pregnancy is strictly contraindicated.
Endocarditis prophylaxis
Two major predisposing causes of infective endocarditis are a susceptible cardiovascular substrate and a source of bacteremia. The clinical and bacteriologic profile of infective endocarditis in patients with CHD has changed with the advent of intracardiac surgery and of prosthetic devices. Prophylaxis includes both antimicrobial and hygienic measures. Meticulous dental and skin care are required. Routine antimicrobial prophylaxis is recommended for bacteremic dental procedures or instrumentation through an infected site in most patients with operated CHD, particularly if foreign material, such as a prosthetic valve, conduit, surgically constructed shunt, etc., is in place. In the case of patches, in the absence of a high-pressure patch leak, prophylaxis is usually recommended for 6 months until there is endothelialization. Individuals with unrepaired cyanotic heart disease are also generally recommended to receive prophylaxis (Chap. 25).