Fabio Facchinetti1 , Giulia Dante1 and Isabella Neri1
(1)
Mother-Infant Department, University of Modena and Reggio Emilia, Modena, MO, Italy
Fabio Facchinetti
Email: fabio.facchinetti@unimore.it
13.1 Introduction
In the last decades, scientific interest has been directed to study the inositol family (INS) to understand their role in health and diseases. Among them, myo-inositol (MI) and D-chiro-inositol (DCI) play a key function owing to their involvement as second messengers of insulin in various insulin-dependent processes. Nowadays, an alteration in insulin signaling is recognized as the main driver in the pathophysiology of polycystic ovary syndrome (PCOS) [1]. PCOS is the most common reason of infertility, affecting approximately up to 10 % of women in reproductive age. Although MI and DCI exert different physiological functions, their respective roles in the etiology and treatment of PCOS are still debated.
13.2 Inositol(s) Story
Myo-inositol (MI), the first molecule to be known among INS (in the year 1850), can exist in nine possible stereoisomeric forms, consequently to the epimerization of the six OH- groups [2]. Natural sources for INS are dietary intake and endogenous biosynthesis. In food, these compounds are found especially in citrus fruits (with the exception of lemon), beans, and whole grains [3]. Among the nine stereoisomers, only MI shows a wide distribution in organisms, and it participates to the regulation of several hormone signals including insulin, follicle-stimulating hormone (FSH), thyroid-stimulating hormone (TSH), and serotonin. D-Chiro-inositol (DCI), another biologically relevant stereoisomer, is enzymatically converted from MI through an insulin-dependent epimerase. Despite their similarities, MI and DCI display different biological function. Considering that glucose metabolism is regulated by insulin whereas the activation of glucose transporters and glucose utilization are due to MI, the glycogen synthesis is controlled through DCI [4–6]. On the other hand, MI in the ovary is devoted to glucose uptake and FSH signaling, while DCI mediates insulin-induced testosterone synthesis. MI constitutes almost all (>99 %) INS in the intracellular pool of most tissues, whereas the remainder is DCI. Noteworthy, every tissue has its own specific MI:DCI ratio, which translates into the different tissue function [7]. Accordingly, in order to set a proper treatment for PCOS, it is necessary to restore and maintain the appropriate MI:DCI ratio. In this chapter, we will report, for the first time, MI and DCI plasma ratio in healthy subjects, discussing the trials that have investigated a therapeutic option based on this ratio and some results of the international consensus conference held on myo-inositol and D-chiro-inositol in obstetrics and gynecology.
13.3 MI:DCI Physiological Plasma Ratio
We identified two studies [8, 9], both from the same group, reporting the pharmacokinetic (PK) profile of a pharmaceutical preparation of MI. In these studies were measured MI plasma levels, but also DCI levels were recorded. We had permission from the authors to access their data to calculate the physiological plasma ratio from each study. Study 1 was performed in 20 volunteers (eight males, 12 females), aged between 18 and 35 years, with a body mass index (BMI) ranging between 21 and 25 kg/m2. Study 2 was performed in 12 volunteers (all women) aged between 20 and 40 years with a BMI between 18 and 24. By pooling data from the two studies, we have found a MI:DCI ratio of 40:1 (Fig 13.1).
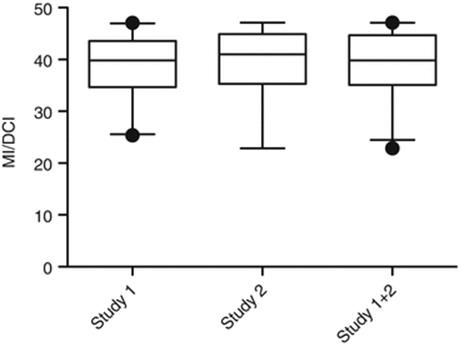
Fig. 13.1
Plasma ratio (40:1) and pharmacokinetics of MI and DCI. Data of two different studies in human volunteers
Recently, three different studies evaluated the efficacy of a treatment based on the physiological plasma ratio between MI and DCI of 40:1 in PCOS women. The idea behind this therapy is that an INS dysregulation plays a central role in nurturing PCOS. Indeed, epimerase dysregulation changes the MI:DCI ratio, which in turn could impair hormone signaling, namely, of both insulin and FSH.
Various evidences supported a deficiency concerning the availability and/or utilization of MI and/or DCI in tissues of PCOS women, and this impairment likely contributes to the insulin resistance typical of that syndrome [6, 10]. Unlike other tissues, such as muscles and liver, the ovaries are not insulin resistant. Because the epimerase activity, regulating the MI:DCI ratio, is insulin dependent, PCOS patients are affected by a boosted MI to DCI epimerization into the ovary, leading to overproduction of DCI and MI deficiency [11], as shown by two independent laboratories [6, 10]. Thus, a specific MI depletion and a DCI overload characterize the ovary of PCOS women. The poor oocyte quality observed in PCOS patients can be explained by this imbalance, responsible also for the impaired FSH signaling [12, 13].
Literature evidences have already shown that MI supplementation is able to correct PCOS metabolic aspects. Two trials demonstrated that the same effect was obtained even in a more effective way by administering MI and DCI in a physiological ratio (40:1). Indeed, the improved parameters were diastolic blood pressure, fasting glucose, fasting insulin, and both insulin and glucose AUCs [14, 15]. Additional improved parameters were those linked to the CVD, namely, HOMA index, triglycerides, and both HDL and LDL cholesterol. Noteworthy, ovulation was restored in the majority of the women.
Furthermore, by moving from the metabolic aspects of the syndrome to the reproductive ones, a trial has shown that the treatment of PCOS women undergoing ICSI, with a MI:DCI 40:1 based therapy, retains the beneficial effects of MI treatment alone, outperforming the DCI treatment [12].
In particular, the treatment is able to improve ovarian response and oocyte and embryo quality. Recently, the interest of the scientific world on MI and DCI has pushed the PRESIS to organize an international consensus conference in order to clarify this issue and lay the foundations of future researches.
13.4 Conference Aim and Methods
Since the knowledge of the differences between MI and DCI is not well established among researchers, as it is proven by a systematic and a Cochrane review mixing trials performed using MI or DCI, the PREIS School (Permanent International and European School in Perinatal Neonatal and Reproductive Medicine) has organized the “2013 Florence International Consensus Conference on Myo and D-CHIRO-INOSITOL in Obstetrics and Gynecology and Assisted Reproduction Technology (ART)” aimed at elucidating some controversial points with the contribution of opinion leaders in the fields of cell biology, mammalian embryology, human endocrinology, metabolism, obstetrics, and gynecology. Two separate panels of this Committee worked on the roles of MI:DCI in metabolic syndrome (mainly PCOS) therapy and of MI in ART and drew up two lists of hot topics. Our review reports only the published results in the paper on myo-inositol and ART [16].
The following is a set of research questions concerning ART:
1.
2.
3.
4.
13.5 MI and ART
13.5.1 Physiological Involvement of INS in Oocyte Maturation
13.5.1.1 Role of MI in Oogenesis and Early Embryogenesis
In mammalian females including humans, an elevated MI content in the follicular fluid fosters oocyte quality and pregnancy outcome [17, 18]. MI activity is in connection with the InsP3 function on the modulation of intracellular calcium ion concentration, influenced by LH and FSH hormones [16]. In oocytes, MI, among different functions at the ovarian level, positively affects the maturation process [16]. The decrease of intracellular MI stores impairs oocyte maturation, and MI supplementation in culture medium has been shown to increase the development of fertile eggs [16]. The implantation rate and post-implantation viability of embryos rise if the oocytes are cultured in a medium containing MI and then fertilized in vitro and transferred for promoting pregnancy [16–19]. During in vitro fertilization (IVF) cycles, the treatment of women with MI before the hormonal stimulation has reduced the FSH quantity to be administered and the number of days required for the appropriate stimulation. All these parameters are positively related to the possibility of pregnancy and improved quality of oocytes and embryos and, probably, the implantation rate [12, 16]. Thus, MI administered 3 months before ovulation induction can produce a rise in the number of high-quality embryos obtained in IVF cycles.
13.5.1.2 MI and Oogenesis: A Lesson from Polycystic Ovary Syndrome
Further proofs confirming the essential role of MI in follicular fluid for safeguarding egg quality derived from the PCOS studies were previously examined. It is therefore clear that MI depletion in a PCOS ovary impairs dominant follicle recruitment and appropriate oocyte growth/maturation. These data support the fundamental observations by Chiu et al. [18] showing that proper content of MI in follicular fluid indicates a required condition to ensure egg quality.
13.5.2 INS Involvement in the Physiology of Spermatozoa Function
In agreement with the MI high levels in female generative system, the same condition can be found in mammalian male, where MI content is more elevated in reproductive organs than in blood serum and increases from the caput to the cauda epididymis [16]. In males, FSH-responsive Sertoli cells are the main producers of MI, which is implicated in processes such as the regulation of spermatozoa motility, capacitation, and acrosome reaction. MI increases sperm cell parameters in male patients suffering from oligoasthenoteratozoospermia (OAT), a severe pathology impairing sperm cell number, morphology, and function [16]. This evidence suggests that MI use in the treatment of semen samples during IVF cycles can raise fertilization rate and embryo quality, in this way, giving higher chances of pregnancy. Treating OAT patients’ sperm cells with MI gives the following changes: the presence of amorphous material and semen viscosity decreases, midpiece volume improves, and mitochondrial cristae morphology is restored, regularizing the mitochondria structures [16]. At the functional level, a key step is the direct MI action on mitochondria, raising the membrane potential [16]. High values of mitochondrial membrane potential attest to the integrity of this structure, meaning, optimal levels of activity and proper cell viability. Therefore, MI treatment of sperm cells from both OAT patients and normal subjects enhances the recovery of cells usable in IVF cycles after swim-up [16], supporting its use as supplement in sperm cells manipulation in the procedures of medical-assisted reproduction.
13.5.3 Usefulness of INS Treatment During ART Cycles
As shown before, the pre-treatment of the PCOS patients with MI looks really very encouraging. The MI effect has been verified also in non-PCOS women needing fertility treatment owing to male or tubal anomalies [16]. All these data are in keeping with the evidence by Chiu et al. [18] that the gonadotropin quantity necessary for ovarian stimulation is lower in patients with follicular fluid characterized by higher MI levels.
13.5.4 Comparison of the Clinical Efficacy Between Supplementation with MI and/or DCI
As highlighted previously, for exerting its physiological function, the ovary would not need high doses of DCI. Moreover, the poor oocyte quality in PCOS ovary could be caused by decreased energy metabolism, and in turn, it is an effect of the down-regulation of the genes controlling glucose uptake [13, 20]. These findings agree with those obtained by Unfer et al. [12], showing that MI but not DCI exerts an action at the ovarian level and leading to the previously quoted DCI paradox. Therefore, the positive MI activity on oocyte quality could be related with its function in glucose cell uptake, which ameliorates the energy status of the ovary, and in FSH signaling and induction of calcium release, which allows proper germ cell maturation.
13.6 Conclusions
Experimental data demonstrated that in the baseline condition, the MI:DCI ratio in healthy volunteers is set at 40:1. According to the International Consensus Conference, it is now clear that both MI and DCI are involved in various physiological and pathological functions (mainly the transduction of insulin and FSH signal), although with differentiated roles. INS supplementation could exert a positive action in different pathophysiological features in obstetrics and gynecology. The MI supplementation is very promising, with clear benefits, in the treatment of PCOS women and also in the prevention of gestational diabetes mellitus. A much larger amount of clinical data are available for MI in comparison with DCI, but the existence of tissue-specific ratios also in the ovary has suggested to develop a treatment based on both MI:DCI combination (ratio 40:1), in agreement with the “DCI paradox” [11].
On the other hand, INS by itself or through its derivatives exerts a pivotal role in reproduction, namely, in oocyte and spermatozoa development. MI depletion induces a defect in glucose uptake, reducing glucose availability in the ovary for both oocytes and follicular cells. The impairment of sugar availability in oocytes compromises their quality [21]. MI treatment in ART has demonstrated undeniable positive effects, and the use of MI, alone or in combination with DCI, at the 40:1 ratio, should be definitely considered a predictive factor for the improvement of ART outcome.
References
1.
Dunaif A (1997) Insulin resistance and the polycystic ovary syndrome: mechanism and implications for pathogenesis. Endocr Rev 18:774–800PubMed
2.
Murthy PPN (2006) Structure and nomenclature of inositol phosphates, phosphoinositides, and glycosylphosphatidylinositols. In: Lahiri Majumder A, Biswas BB (eds) Biology of inositols and phosphoinositides. Springer, New York, pp 1–19CrossRef
3.
Clements RS Jr, Darnell B (1980) Myo-inositol content of common foods: development of a high-myo-inositol diet. Am J Clin Nutr 33(9):1954–1967PubMed
4.
Larner J, Huang LC, Tang G, Suzuki S, Schwartz CFW, Romero G, Roulidis Z, Zeller K, Shen TY, Oswald AS, Luttrell L (1988) Insulin mediators: structure and formation. Cold Spring Harb Symp Quant Biol 53(Pt 2):965–971CrossRefPubMed
5.
Sun TH, Heimark DB, Nguygen T, Nadler JL, Larner J (2002) Both myoinositol to chiro-inositol epimerase activities and chiro-inositol to myo-inositol ratios are decreased in tissues of GK type 2 diabetic rats compared to Wistar controls. Biochem Biophys Res Commun 293:1092–1098CrossRefPubMed
6.
Heimark D, McAllister J, Larner J (2014) Decreased myo-inositol to chiro-inositol (m/c) ratios and increased m/c epimerase activity in pcos theca cells demonstrate increased insulin sensitivity compared to controls. Endocr J 61:111–117CrossRefPubMed
7.
Pak Y, Huang LC, Lilley KJ, Larner J (1992) In vivo conversion of [3H] myoinositol to [3H]chiroinositol in rat tissues. J Biol Chem 267:16904–16910PubMed
8.
Carlomagno G, De Grazia S, Unfer V, Manna F (2012) Myo-inositol in a new pharmaceutical form: a step forward to a broader clinical use. Expert Opin Drug Deliv 9(3):267–271. doi:10.1517/17425247.2012.662953CrossRefPubMed
9.
De Grazia S, Carlomagno G, Unfer V, Cavalli P (2012) Myo-inositol soft gel capsules may prevent the risk of coffee-induced neural tube defects. Expert Opin Drug Deliv 9(9):1033–1039. doi:10.1517/17425247.2012.701616, Epub 2012 Jul 5CrossRefPubMed
10.
Unfer V, Carlomagno G, Papaleo E, Vailati S, Candiani M, Baillargeon JP (2014) Hyperinsulinemia alters myoinositol to d-chiroinositol ratio in the follicular fluid of patients with PCOS. Reprod Sci 21:854–858CrossRefPubMed
11.
Carlomagno G, Unfer V, Roseff S (2011) The D-chiro-inositol paradox in the ovary. Fertil Steril 95:2515–2516CrossRefPubMed
12.
Unfer V, Carlomagno G, Rizzo P, Raffone E, Roseff S (2011) Myo-inositol rather than D-chiro-inositol is able to improve oocyte quality in intracytoplasmic sperm injection cycles. A prospective, controlled, randomized trial. Eur Rev Med Pharmacol Sci 15:452–457PubMed
13.
Arya BK, Haq AU, Chaudhury K (2012) Oocyte quality reflected by follicular fluid analysis in polycystic ovary syndrome (PCOS): a hypothesis based on intermediates of energy metabolism. Med Hypotheses 78:475–478CrossRefPubMed
14.
Nordio M, Proietti E (2012) The combined therapy with myo-inositol and D-chiro-inositol reduces the risk of metabolic disease in PCOS overweight patients compared to myo-inositol supplementation alone. Eur Rev Med Pharmacol Sci 16:575–581PubMed
15.
Minozzi M, Nordio M, Pajalich R (2013) The combined therapy myo-inositol plus D-chiro-inositol, in a physiological ratio, reduces the cardiovascular risk by improving the lipid profile in PCOS patients. Eur Rev Med Pharmacol Sci 17:537–540PubMed
16.
Bevilacqua A, Carlomagno G, Gerli S, Montanino Oliva M, Devroey P, Lanzone A, Soulange C, Facchinetti F, Di Renzo GC, Bizzarri M, Hod M, Cavalli P, D’Anna R, Benvenga S, Chiu TT, Kamenov ZA (2015) Results from the International Consensus Conference on myo-inositol and D-chiro-inositol in Obstetrics and Gynecology – assisted reproduction technology. Gynecol Endocrinol. doi:10.3109/09513590.2015.1006616PubMed
17.
Chiu TT, Tam PP (1992) A correlation of the outcome of clinical in vitro fertilization with the inositol content and embryotrophic properties of human serum. J Assist Reprod Genet 9:524–530CrossRefPubMed
18.
Chiu TT, Rogers MS, Law EL, Briton-Jones CM, Cheung LP, Haines CJ (2002) Follicular fluid and serum concentrations of myo-inositol in patients undergoing IVF: relationship with oocyte quality. Hum Reprod 17:1591–1596CrossRefPubMed
19.
Colazingari S, Fiorenza MT, Carlomagno G, Najjar R, Bevilacqua A (2014) Improvement of mouse embryo quality by myo-inositol supplementation of IVF media. J Assist Reprod Genet 31:463–469PubMedCentralCrossRefPubMed
20.
Ma X, Fan L, Meng Y, Hou Z, Mao YD, Wang W, Ding W, Liu JY (2007) Proteomic analysis of human ovaries from normal and polycystic ovarian syndrome. Mol Hum Reprod 13:527–535CrossRefPubMed
21.
Chaudhary K, Babu KN, Joshi VN, Srivastava S, Chakravarty BN (2011) NMR-based metabolomics reveals differently expressed metabolites in follicular fluid of PCOS women: potential biomarkers for good quality oocyte? Hum Reprod 26:i226–i246CrossRef