
Figure 3.79 Crypt architectural disturbance pattern. This pattern encompasses the general features of “chronicity” including crypt distortion and branching (pictured here), crypt dropout, crypt shortfall, and pyloric metaplasia.
CHECKLIST: Etiologic Considerations for the Architectural Disturbance Pattern
![]() Inflammatory Bowel Disease
Inflammatory Bowel Disease
![]() Diaphragm Disease
Diaphragm Disease
![]() Ischemia
Ischemia
![]() Graft Versus Host Disease
Graft Versus Host Disease
![]() Acute Medication Reaction (Mycophenolate Mofetil and Mycophenolic Acid)
Acute Medication Reaction (Mycophenolate Mofetil and Mycophenolic Acid)
![]() Allograft Rejection
Allograft Rejection
![]() Radiation Duodenitis
Radiation Duodenitis
![]() Pouchitis and Pouch-Related Changes
Pouchitis and Pouch-Related Changes
At scanning magnification, the appearance of crypt architectural disturbance can be seen as: crypt distortion, crypt dropout, crypt shortfall with or without basal lymphoplasmacytosis, or microcrypt formation (Fig. 3.79). Note that this pattern is exclusive of villous architectural changes (i.e., villous blunting), which, instead, is a feature of malabsorption pattern and confers a different group of differential diagnoses. Although some might consider villous blunting a feature of chronic injury, isolated architectural disturbances of the villi should be investigated as a malabsorption pattern. Furthermore, although many of these features indicate chronic injury, this pattern spans a histologic spectrum from subtle to striking, encompassing features from the earliest crypt disturbance (a single withered crypt) to marked crypt distortion. Crypt architectural disturbance is a nonspecific pattern of injury, the etiology of which encompasses IBD, mesenteric ischemia, graft versus host disease, allograft rejection, short gut syndrome, radiation duodenitis, and (ileal) pouchitis. Incisive readers will note that crypt disturbances are a minor histologic pattern in many of these entities, and indicate chronic injury. Accordingly, examination for other primary features (e.g., increased apoptotic bodies in graft vs. host disease) and correlation with clinical circumstances are required to arrive at an etiology.
INFLAMMATORY BOWEL DISEASE
Crohn disease is a chronic idiopathic inflammatory disorder characteristically involving the distal 15 to 25 cm of the terminal ileum; however the gastrointestinal manifestations of Crohn disease are remarkably diverse and may include variations such as ileocolic Crohn disease (30% to 50% of patients with Crohn disease), localized or extensive disease of the small bowel (25% to 50%), isolated Crohn colitis (15% to 30%), anorectal Crohn disease (5% to 19%), or gastric, esophageal and duodenal Crohn disease (5% to 30%).19–22 Histologically, the disease manifests in a patchy distribution with a combination of activity (cryptitis, crypt abscess, erosion, and ulceration) and chronicity (villous blunting, crypt architectural distortion, crypt dropout, crypt shortfall, basal lymphoplasmacytosis, increased lamina propria chronic inflammation, pyloric metaplasia, transmural lymphoid aggregates, and neuromuscular hyperplasia&emdash;with or without granulomata). For an expanded discussion on the general features of Crohn disease, see also Inflammatory Bowel Disease, Chronic Colitis Pattern, Colon Chapter.
In the duodenum, Crohn disease produces typical lesions in approximately 0.5% to 4% of patients.23 These lesions usually coexist with ileal involvement, and may extend proximally and distally to involve the stomach or jejunum. By comparison, “regional jejunitis” rarely coexists with duodenal disease and may locally or diffusely involve the jejunum. Progressive transmural inflammation with scarring and deep ulceration may ultimately lead to symptoms associated with intestinal obstruction, perforation, bleeding, or fistula formation. When obstruction develops, it usually does so in the distal ileum, and deep linear ulcers or fistulae may give rise to profound gastrointestinal bleeding. Gross and full-thickness microscopic examination of the small bowel are considered the gold standard for diagnosis. Gross pathology shows thickening of the bowel wall, fistula formation, strictures, serpiginous ulcers, aphthous ulcers, and creeping mesenteric fat. The corresponding histology shows a combination of variable activity (cryptitis, villitis, crypt abscess, erosion, and ulcer) and chronicity (villous blunting, crypt architectural distortion, crypt dropout, crypt shortfall, basal lymphoplasmacytosis, increased lamina propria chronic inflammation, pyloric metaplasia, transmural lymphoid aggregates, and neuromuscular hyperplasia&emdash;with or without granulomata) (Figs. 3.80–3.87).
FAQ: What is “creeping fat?”
Answer: The antimesenteric serosal surface of the small bowel and colon is usually smooth and devoid of adipose tissue. In Crohn disease, repeated cycles of transmural damage can result in an irregular antimesenteric serosal surface composed of prominent fibrosis and fat (“creeping fat”). This creeping fat is used by surgeons to identify the extent of affected bowel for resection. In addition, this finding should be documented at the grossing bench as it can help differentiate Crohn disease from ulcerative colitis.

Figure 3.80 Crypt architectural disturbance, Crohn disease. The crypt architectural disturbances are evident at low magnification. Normally, the crypts rest directly on the muscularis mucosae. In this example, the base of a crypt falls short of touching the muscularis mucosae. This gap between the muscularis mucosae and the crypt is called “crypt shortfall” (arrow). Also, note the irregularly shaped crypts, or abnormal crypt configuration, in addition to areas of total glandular loss, or “crypt dropout.”

Figure 3.81 Crypt architectural disturbance, Crohn disease. Crypt architectural disturbances are seen with irregularly shaped crypts and bifid branching crypts (arrowhead). Note also the presence of cryptitis within this same crypt and the loosely-formed granuloma (arrow).

Figure 3.82 Crypt architectural disturbance, Crohn disease. Residual villous projections are present, but the major pattern here is crypt architectural disturbances, including crypt distortion, crypt shortfall, and crypt dropout. The lamina propria is expanded with increased chronic inflammation and prominent pyloric metaplasia (arrowheads) is present.

Figure 3.83 Crypt architectural disturbance, pyloric metaplasia. Pyloric-type glands are normally limited to the pylorus at the junction of the stomach and small bowel. When seen in the terminal ileum, these metaplastic glands indicate chronicity.

Figure 3.84 Crypt architectural disturbance, pyloric metaplasia. These pyloric glands have abundant foamy-to-clear cytoplasm and small, round or ovoid nuclei that may be flattened against the basement membrane.

Figure 3.85 Crypt architectural disturbance, pyloric metaplasia. Although pyloric metaplasia (arrowhead) indicates chronicity, it is not specific for Crohn disease, and can be found in other chronic conditions, such as diaphragm disease of the terminal ileum.

Figure 3.86 Crypt architectural disturbance, Crohn disease. This example shows crypt distortion and expansion of the lamina propria with an inflammatory infiltrate. Areas of pyloric metaplasia (arrow) are also present.

Figure 3.87 Crypt architectural disturbance, Crohn disease. Although chronic injury features are evident at low power, higher magnification is required to see areas of active inflammation (activity) indicated by neutrophils. Seen here are cryptitis (arrow) and lamina propria acute inflammation (arrowhead).
FAQ: Does involvement of resection margins by Crohn disease have prognostic significance?
Answer: No.
The status of resection margins is not predictive of disease recurrence.24 Postoperative recurrence of Crohn disease is more common in patients with greater disease extent, perforating disease, and medically refractory Crohn disease.25
DIAPHRAGM DISEASE
NSAIDs cause a wide spectrum of histologic changes in the small bowel, some of which are segment specific, such as diaphragm disease of the terminal ileum. Mild lesions consist of superficial erosions with nonspecific neutrophilic, eosinophilic and plasmacytic infiltrates. These erosions may be multiple, can coalesce forming deep ulcers, and may result in hemorrhage. Repeat cycles of ulceration and healing can cause submucosal scarring and web-like mucosal septa that project into the lumen. These resulting circumferential stenosing lesions appear as multiple diaphragm-like narrowings and are more commonly seen in the distal small bowel, particularly the terminal ileum (Figs. 3.88 and 3.89). Accordingly, the patients often present with a surgically emergent obstruction. This so-called diaphragm disease can be accompanied by a wide array of additional abnormalities, including crypt architectural disturbances mimicking IBD, eosinophilic enteritis, enteritis cystica profunda, and neuromuscular and vascular hamartoma-like changes (Figs. 3.90–3.92).26 By comparison, NSAID injury in the proximal small bowel often results in subtle and nonspecific reactive duodenopathy-type changes, rather than chronic architectural changes. See also Malabsorption Pattern, this chapter. A diagnosis of diaphragm disease can be suggested by the endoscopic or pathologic findings but requires correlation with the patient’s medication list for definitive diagnosis. Distinction from ileal Crohn disease can be particularly challenging if a history of NSAID use cannot be documented; in general, there is minimal chronic inflammation in NSAID-associated injury, whereas it is abundant in Crohn enteritis. Anecdotally, we have seen surreptitious NSAID abuse lead to segmental resection of obstructing diaphragms; family members of the patients may be able to provide the clinical correlation in these cases.

Figure 3.88 Diaphragm disease, endoscopic view. Chronic NSAID injury in the distal small bowel causes cycles of ulceration and healing that result in circumferential stenosing lesions (“diaphragms”) and can lead to obstruction.

Figure 3.89 Crypt architectural disturbance, diaphragm disease. Low power magnification of the diaphragm shows raised mucosa pushed upward by a thickened and fibrotic submucosa.

Figure 3.90 Crypt architectural disturbance, diaphragm disease, submucosal fibrosis. Dense collagen replaces the normally loose submucosal tissues after repeat cycles of ulceration and healing.

Figure 3.91 Crypt architectural disturbance, diaphragm disease, pyloric metaplasia. Diaphragm disease is found almost exclusively in the ileum and can demonstrate chronic injury features such as crypt architectural distortion and pyloric metaplasia (arrowheads). The main differential diagnosis is with inflammatory bowel disease.

Figure 3.92 Crypt architectural disturbance, diaphragm disease. Longstanding diaphragm disease can show mucosal abnormalities similar to those seen in inflammatory bowel disease, and can be a diagnostic pitfall.
KEY FEATURES of Diaphragm Disease:
• Caused by chronic NSAID use or abuse.
• Repeat cycles of ulceration and submucosal scarring result in diaphragm-like narrowing of the terminal ileum.
• Features can mimic IBD, with ileal stricturing and histologic features of chronicity.
• Correlation with clinical use of NSAIDs is required.
ISCHEMIA
Acute insufficiency of mesenteric arterial blood flow accounts for 60% to 70% of cases of mesenteric ischemia, and results in mortality rates exceeding 60%.27 Severe pain is a common presentation of small bowel ischemia compared with ischemia of the colon, in which extreme pain is usually not as prominent a feature. Specific risk factors include advanced age, atherosclerosis, low cardiac output states, cardiac arrhythmias, severe cardiac valvular disease, recent myocardial infarction, and intra-abdominal malignancy.27 The causes of intestinal ischemia are many (Table 3.2), but can be classified into four major categories28,29:
TABLE 3.2: Causes of Intestinal Ischemia

• Superior mesenteric artery (SMA) embolism (50%):
This is most frequently due to a dislodged thrombus from the left atrium, left ventricle, or cardiac valves. The SMA is anatomically most susceptible to embolism due to its large caliber and narrow take-off angle from the aorta.29The embolus usually lodges 3 to 10 cm distal to the origin of the SMA, in a tapered segment distal to the take-off of the middle colic artery. Concomitant arteriolar vasoconstriction usually occurs, further impairing splanchnic blood flow and exacerbating ischemia. The middle segment of the jejunum is most often involved in the ischemic process, as it is most distant from the collateral circulation of the celiac and inferior mesenteric arteries.
• Superior mesenteric artery thrombosis (15% to 25%):
Acute thrombosis of the mesenteric circulation usually occurs as a superimposed phenomenon in patients with a history of chronic intestinal ischemia from progressive atherosclerotic stenosis, but may also happen in the setting of abdominal trauma or infection. There does not appear to be a significant association between inherited coagulation defects and mesenteric arterial thrombosis.30,31
• Mesenteric venous thrombosis (5%):
Risk factors include hypercoagulable states, portal hypertension, abdominal infections, blunt abdominal trauma, pancreatitis, splenectomy, and malignancy in the portal region.32 Ischemia is due to the resistance in mesenteric venous blood flow, which subsequently causes diminished arterial flow.27
• Nonocclusive ischemia (20% to 30%):
This is thought to be caused by splanchnic hypoperfusion and vasoconstriction,33 and it occurs most frequently in patients with atherosclerotic vascular disease. Inciting events include aortic insufficiency, sepsis, cardiac arrhythmias, and medications such as digoxin and alpha-adrenergic agonists. Ischemia secondary to cocaine use has also been described.34,35
Mesenteric angiography remains the gold standard diagnostic study, and most patients do not receive endoscopic examination due to the risk of bowel perforation. As such, it is quite rare to diagnose small bowel ischemia by endoscopic biopsy. Naturally, the histologic findings are similar to those seen in the colon, namely mucosal coagulative necrosis. Early and minimal injury occurs first at the villous tips due to splanchnic shunting of blood away from the mucosa. This is noted as degeneration and sloughing of superficial epithelial cells, edema, and vascular congestion (Fig. 3.93). Later, the epithelial cells become markedly attenuated and the crypts appear compressed and atrophic (“microcrypts”) as the lamina propria swells and hemorrhages (Fig. 3.94). Within 5 hours of total acute occlusion, almost the entire intestinal wall appears necrotic (Fig. 3.95). These changes are all devoid of acute inflammation (Fig. 3.96) until reperfusion occurs. And, paradoxically, reperfusion further injures the tissues by introducing oxygen free radical formation,36 the severity of which is dependent upon the duration of the preceding hypoxia (Figs. 3.97–3.100).

Figure 3.93 Crypt architectural disturbance, ischemic enteritis, earliest signs. Marked congestion of capillaries with sloughing of epithelial cells along the villous surface are present in the absence of an inflammatory infiltrate. At these earliest stages, the crypts remain intact.

Figure 3.94 Crypt architectural disturbance, ischemic enteritis. The lamina propria has become hemorrhagic and the crypt architecture is abnormal with areas of crypt dropout and mirocrypt formation.

Figure 3.95 Crypt architectural disturbance. End stage ischemic bowel with necrosis.

Figure 3.96 Crypt architectural disturbance, ischemic enteritis. This example lacks the striking hemorrhage seen previously, but the epithelial cells have sloughed off, leaving slightly necrotic villous tips and residual microcrypts (arrowheads) at the base.

Figure 3.97 Crypt architectural disturbance, ischemic enteritis. This example shows the marked crypt architectural disturbance that can accompany ischemic enteritis. The lamina propria has hemorrhage and hyalinization, yielding an eosinophilic appearance. The crypt lumina have sloughed degenerated epithelial cells that mimic crypt abscesses (arrowhead).

Figure 3.98 Crypt architectural disturbance, ischemic enteritis. Higher magnification of the crypts shows that they are filled with karyorrhectic debris from sloughed epithelial cells and not neutrophils.

Figure 3.99 Crypt architectural disturbance, ischemic enteritis. There is marked crypt architectural distortion at low power, and the lamina propria appears hemorrhagic and hyalinized.

Figure 3.100 Crypt architectural disturbance, ischemic enteritis. Higher magnification of the previous figure reveals focal microcrypt formation. The abundant fibrin deposition in the lamina propria imparts a homogenous eosinophilic/hyalinized appearance.
KEY FEATURES of Ischemia:
• Mesenteric ischemia can be clinically categorized as SMA embolism, SMA thrombosis, mesenteric venous thrombosis, and nonocclusive ischemia.
• Severe pain is a common presentation in mesenteric ischemia, but not colonic ischemia.
• Early histologic findings include sloughing of superficial epithelial cells, edema, and vascular congestion.
• Later stages include lamina propria hemorrhage, hyalinization, microcrypt formation, followed by coagulative necrosis.
• Acute inflammation is absent unless reperfusion has occurred.
• Beware not to overcall crush artifact from biopsy forceps as ischemic change.
• Inflammatory changes can mimic vasculitis.
PEARLS & PITFALLS
Crush Artifact from Biopsy Forceps Can Mimic Ischemic Injury
Biopsy forceps may strip epithelial cells from villi and cause crushed glands that can be mistaken for atrophic microcrypts. True ischemic injury shows lamina propria hemorrhage and degenerative cellular changes, such as loss of the apical brush border and ghostlike nuclei (Figs. 3.101–3.103).

Figure 3.101 Crypt architectural disturbance, ischemic enteritis mimic, crush artifact. Forceps biopsies can sometimes cause crush artifact that mimics ischemic injury. These crypt epithelial cells have “popped” out of their rightful place (arrows) as a result of crush injury. Note how the detached epithelial cells lack degenerative features, and how the lamina propria looks intact, without hemorrhage, fibrin deposition, hyalinization, or fibrosis.

Figure 3.102 Crypt architectural disturbance, ischemic enteritis mimic, crush artifact. The sloughing epithelial cells leave some villi without intact epithelium; however one can be reassured this is the result of endoscopic (or laboratory) manipulation because the epithelial cells lack degenerative changes, and the lamina propria of the villi (arrowheads) lack edema, hemorrhage, fibrin deposition, hyalinization, and fibrosis.

Figure 3.103 Crypt architectural disturbance, ischemic enteritis. A row of microcrypts is present in a fibrotic lamina propria. Microcrypts are highly specific for ischemic injury. Compare this Figure to the mimics above.
PEARLS & PITFALLS
Evaluation for Underlying Vasculitis
Ischemic damage can cause vascular thrombi, and reperfusion injury may cause inflammatory changes, neither of which should be confused for an underlying causal vasculitis. Primary vascular injury should only be evaluated in areas not directly subjacent to ischemia or ulceration (Figs. 3.104 and 3.105).

Figure 3.104 Crypt architectural disturbance, ischemic enteritis, adjacent vasculitis mimic. When encountering ischemic enteritis, it is prudent to search for vasculitis as a possible underlying etiology; however beware as vessels that are directly subjacent to ischemic areas may show inflammation and occlusion secondary to the mucosal damage (as opposed to the cause of the mucosal injury). This muscular artery is involved by marked acute inflammation and fibrin deposition.

Figure 3.105 Crypt architectural disturbance, ischemic enteritis, adjacent vasculitis mimic. This higher magnification of the previous Figure shows karyorrhectic debris (arrowhead) and neutrophils within the smooth muscle wall of the artery. Overinterpretation as vasculitis is a pitfall. Vasculitis assessment is best performed in areas away from the acute injury.
PEARLS & PITFALLS
Distinction from Infectious Enteritides
There are no reliable histologic features to distinguish ischemic enteritis from infectious enteritis; correlation with endoscopic impression, clinical information and microbiologic studies is imperative. Infectious enteritides that are toxin mediated, such as Escherichia coli 0157:H7 can cause hemorrhagic enteritis. In addition, while the pseudomembrane of Clostridium difficile colitis is highly characteristic, pseudomembranes are also frequently seen in ischemic enteritis (Fig. 3.106).

Figure 3.106 Crypt architectural disturbance, ischemic enteritis, pseudomembrane formation. Compare the ischemic right side of this Figure with the intact mucosa on the left. Note the crypt architectural disturbances on the right, in addition to the hemorrhagic and hyalinized appearance of the lamina propria. The surface is covered with a pseudomembrane, similar to that seen in C. difficile colitis.
GRAFT VERSUS HOST DISEASE
Graft versus host disease (GVHD) is the donor T lymphocyte mediated destruction of host tissues that occurs following allogeneic transplant. Although allogeneic bone marrow and stem cell transplantation has the highest frequency of GVHD (40% to 80% of patients), GVHD can also occur in donor lymphocyte, whole blood, and solid organ transplantation.37–39 Although in mild cases apoptotic bodies may be the only morphologic clue to GVHD, in more severe cases cystic dilatation of glands or crypts lined by regenerative epithelium, crypt abscesses, and frank epithelial destruction are seen. Thus, scanning magnification view of the biopsies will show architectural disturbance and loss of crypts that correlates with severity of histologic grade (Figs. 3.107 and 3.108). Histologic grading of GVHD is not performed in all transplantation centers, some preferring to use a qualitative approach by reporting “mild, moderate, or severe” GVHD, but when used, a modification of the system for colonic GVHD described by Lerner40 is most common (Figs. 3.109–3.113):
Grade 1: Isolated apoptotic epithelial cells
Grade 2: Loss or damage of isolated crypts with or without crypt abscesses
Grade 3: Loss of 2 or more contiguous crypts
Grade 4: Extensive crypt loss with mucosal denudation
See also GVHD, Lymphocytic Pattern, Esophagus Chapter.
KEY FEATURES of Graft Versus Host Disease:
• GVHD is an immune-mediated destruction of host tissue following bone marrow and stem cell transplantation.
• GVHD may also follow solid organ transplantation, donor T lymphocyte transfusion, and whole blood transfusion.
• Grading of GVHD may be done based on histologic findings (Lerner system) or on diagnostic confidence (NIH system).
• Crypt architectural disturbance in GVHD indicates at least moderate GVHD (grade 2 and higher by the Lerner system).
• Crypt apoptotic activity is the histologic hallmark of GVHD, but is nonspecific.
• The differential diagnosis for apoptotic injury includes infection, chemotherapeutic condition regimen, and the immunosuppressant medication mycophenolate mofetil.

Figure 3.107 Crypt architectural disturbance, graft versus host disease. Crypt architectural disturbance is present in the form of mild crypt distortion and crypt shortfall (arrowhead) involving at least two contiguous crypts (Lerner grade 2 of 4). In addition, the proliferative compartment of the crypts appears expanded and hyperchromatic.

Figure 3.108 Crypt architectural disturbance, graft versus host disease (GVHD). This duodenal biopsy shows marked crypt dropout in this patient with GVHD. The villous architecture remains relatively intact.

Figure 3.109 Crypt architectural disturbance, graft versus host disease. Marked glandular injury and dropout have occurred as a result of GVHD in this patient with a bone marrow transplant.

Figure 3.110 Crypt architectural disturbance, graft versus host disease. Residual crypt bases are seen. Note the relative abundance of entero-endocrine cells (arrowheads), which are not as affected by apoptotic injury.

Figure 3.111 Crypt architectural disturbance, graft versus host disease. This biopsy shows marked crypt architectural changes due to graft versus host disease. At this power, it might be easy to misdiagnose a crypt abscesses.

Figure 3.112 Crypt architectural disturbance, graft versus host disease. Higher magnification of the previous figure shows sloughed epithelial cells in the crypt lumen (not acute inflammation as would be expected in a crypt abscess).

Figure 3.113 Crypt architectural disturbance, graft versus host disease. Complete loss of epithelium and crypts are seen in this example of severe GVHD (Lerner grade 4 of 4).
PEARLS & PITFALLS
Apoptosis is a Nonspecific Pattern of Injury, and Not Singularly Diagnostic for GVHD
False positive interpretations may be due to effects of chemotherapeutic conditioning regimens, concomitant infections, and medications. As a result of induction chemotherapy, an apoptotic pattern of injury can be seen within the first 20 days of bone marrow ablation,41 rendering the diagnosis of acute GVHD difficult. In addition, apoptoses are commonly seen in cytomegalovirus infection42 and cryptosporidiosis,43 which are prevalent in this immunocompromised population. Further complicating the picture may be the use of the immunosuppressant mycophenolate mofetil posttransplantation, which can cause acute mucosal injury with focal ulceration and marked crypt cell apoptosis (see below).44
FAQ: How many apoptotic bodies are required for a diagnosis of GVHD?
Answer: Advances in healthcare allow clinicians to suspect GVHD at much earlier stages, and morphologic features may be more subtle than reported in earlier studies. Correspondingly, minimum thresholds have not been established, but many pathologists require the finding of at least one apoptotic body per biopsy tissue fragment to suggest the diagnosis of GVHD.45,46 Other published thresholds include (1) the total number of apoptotic bodies at least equal to the number of pieces, or (2) scattered apoptotic bodies in more than one crypt.40,45,47 Take note, however, that surface epithelial apoptoses may occur as the result of bowel preparatory regimens, and therefore should not be considered diagnostic for GVHD.
FAQ: How can I tell if this an apoptotic body or a lymphocyte?
Answer: Apoptotic cells contain intracytoplasmic vacuoles filled with nuclear dust and other karyorrhectic debris. These apoptotic fragments appear as small, dark, round bodies surrounded by a white halo. Similarly, IELs may have a clear halo; however by comparison, lymphocytes retain a uniform size of about 10 microns in diameter. To differentiate the two, simply identify a lymphocyte or plasma cell nucleus in the lamina propria and use this as your benchmark for size comparison. Because of their fragmented nature, apoptotic bodies are typically much smaller and variably sized (Fig. 3.114).

Figure 3.114 Crypt architectural disturbance, graft versus host disease. At the crypt bases, numerous apoptotic bodies (circled) are seen. Note how the nuclear fragments have a much smaller diameter and are more variably sized than the mononuclear cells in the lamina propria.
MEDICATIONS (MYCOPHENOLATE MOFETIL AND MYCOPHENOLIC ACID)
Mycophenolate mofetil and mycophenolic acid are immunosuppressants commonly prescribed to transplant recipients and are used in the treatment of some autoimmune diseases. This reversible inhibitor of inosine monophosphate dehydrogenase results in inhibition of purine synthesis and causes a reduction in B and T lymphocytes. At high dosages, epithelial cell damage can also occur, which leads to clinical diarrhea and histologic findings of prominent apoptotic injury with crypt damage and distortion (Figs. 3.115–3.121).44,48 These changes overlap with Crohn disease, GVHD, and ischemia.44,48–51 Further complicating the picture, dual pathology is frequently present in patients prescribed mycophenolate.50 Fortunately, a reduction in dosage or discontinuation of the medication yields rapid clinical response. In difficult cases, a note suggesting modification of the medication list may be helpful to clinicians.
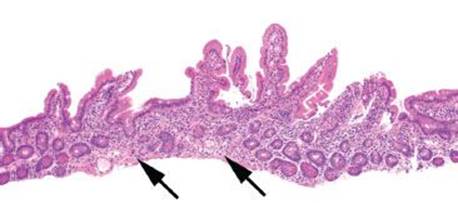
Figure 3.115 Crypt architectural disturbance, mycophenolate-induced injury. This low magnification view of the duodenum, from a patient with unexplained diarrhea, shows very mild crypt architectural disturbance with very focal crypt dropout (arrows). Although the villous architecture is preserved, isolated disturbances of the crypts should prompt further investigation.

Figure 3.116 Crypt architectural disturbance, mycophenolate-induced injury. An area of crypt dropout from the previous case is shown at higher magnification and features apoptotic activity (arrowheads). Although up to 4 apoptoses per 10 duodenal crypts may be considered normal, the presence of apoptoses in confluent crypts is abnormal.

Figure 3.117 Crypt architectural disturbance, mycophenolate-induced injury. Additional crypts from the previous case show numerous apoptotic bodies (arrowheads). Investigation into the patient’s medical record revealed use of mycophenolate mofetil for immunosuppression in the setting of cardiac transplantation.

Figure 3.118 Crypt architectural disturbance, mycophenolate-induced injury. Additional crypts from the previous case show contiguous crypts, each containing apoptotic bodies. This finding should prompt further investigation.

Figure 3.119 Crypt architectural disturbance, mycophenolate-induced injury. This biopsy of the duodenum is from a kidney transplant patient experiencing unexplained diarrhea. Very focal dropout of the crypts, crypt shortfall and basal lymphoplasmacytosis (brackets), and a possible crypt abscess (arrow) are visible at low magnification. Note that the disturbances in this biopsy are limited to the crypts, while the villi appear intact. These mild disturbances of the crypt architecture at low magnification should prompt higher magnification examination.

Figure 3.120 Crypt architectural disturbance, mycophenolate-induced injury. Higher power magnification of the previous case reveals marked apoptotic destruction of the crypts (arrowheads) rather than crypt abscesses. This finding should prompt review of the medication list in any transplant patient.

Figure 3.121 Crypt architectural disturbance, mycophenolate-induced injury. Higher magnification of other crypts from those in the previous figures reveals confluent apoptotic activity (arrowhead) with numerous apoptotic bodies in the proliferative compartment (i.e., base) of the crypts. Cessation of mycophenolate use in this patient resulted in dramatic clinical improvement within 48 hours.
ALLOGRAFT REJECTION, SMALL BOWEL
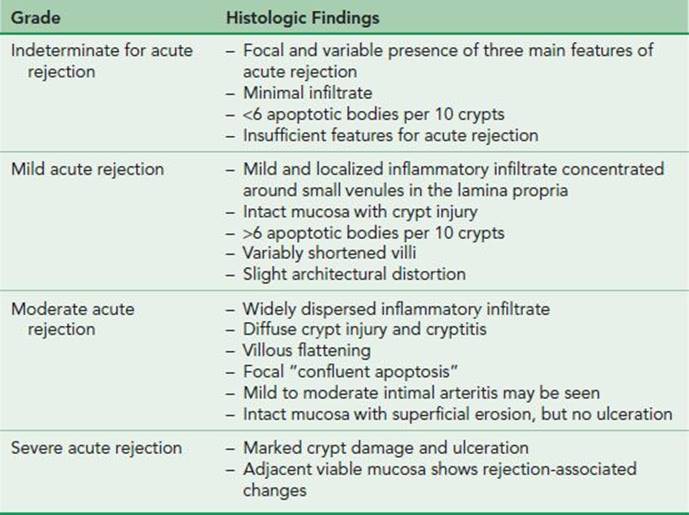
Small bowel transplantation is increasingly performed to treat patients with irreversible intestinal failure. Because the intestine is a lymphoid-rich organ, intestinal transplantation requires complex immunologic events to occur for the graft to function; for example, the donor mucosal immune system must be replaced by the host, and a chimeric state is essential for allograft function.52 Clinical features of acute rejection include fever, nausea and vomiting, diarrhea, and abdominal pain and distension. Severe cases may be accompanied by septic shock, metabolic acidosis, hypotension, and adult respiratory distress syndrome. Surveillance endoscopy can be performed through the ileostomy stoma, and endoscopists should be encouraged to biopsy away from the stoma since stoma sites contain inflammatory and regenerative changes. In addition, since features of acute cellular rejection may be patchy, multiple biopsies should be obtained from both endoscopically normal and abnormal areas. Diagnosis of acute cellular rejection requires clinicopathologic correlation, and requires immediate aggressive immunosuppressive therapy, since progression of allograft rejection can advance to graft loss or mortality. The histologic diagnosis of acute intestinal rejection is similar to that of GVHD and is based on a varying combination of three main features which can be used to determine a rejection grade (Table 3.3) (Figs. 3.122–3.128)52–55:
TABLE 3.3: Grading Schema for Small Bowel Allograft Acute Cellular Rejection52
1. Infiltration by a mixed but primarily mononuclear inflammatory population, including immunoblasts or activated lymphocytes
2. Crypt inflammation and injury, characterized by cytoplasmic basophilia, nuclear enlargement and hyperchromasia, decreased cell height and mucin depletion
3. Increase in crypt apoptotic bodies
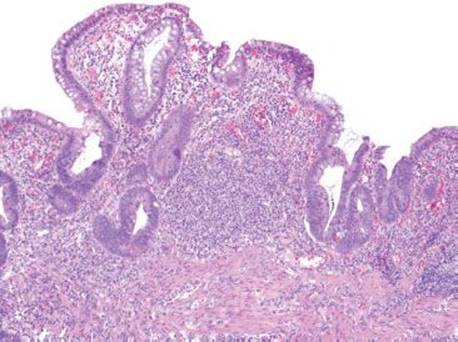
Figure 3.122 Crypt architectural disturbance, small bowel allograft rejection. This example of small bowel allograft rejection shows marked crypt architectural disturbances, such as crypt distortion and branching with areas of crypt dropout. The lamina propria is markedly expanded by chronic inflammatory cells.

Figure 3.123 Crypt architectural disturbance, small bowel allograft rejection. Higher magnification of the previous figure shows abundant apoptotic bodies (circled) within the crypt epithelium. Note how the nuclear debris is smaller and more irregular than the mononuclear cells in the adjacent lamina propria.

Figure 3.124 Crypt architectural disturbance, small bowel allograft rejection. This small bowel allograft shows crypt dropout. Some areas with residual crypt profiles show sloughed epithelial cells within their lumen (arrowhead).

Figure 3.125 Crypt architectural disturbance, small bowel allograft rejection, moderate to severe. Although the villous architecture is relatively intact, there is only one residual crypt (bottom right). The marked crypt loss indicates moderate to severe allograft rejection.

Figure 3.126 Crypt architectural disturbance, indeterminate for small bowel allograft rejection. There are very mild architectural changes in this biopsy, but the crypt epithelium and villi appear intact.

Figure 3.127 Crypt architectural disturbance, indeterminate for small bowel allograft rejection. Higher magnification of the previous figure shows multiple apoptotic bodies (arrowheads) within the crypt epithelium. In this setting, the biopsy is best considered indeterminate for acute cellular rejection and close clinical follow-up is recommended. Comparison of these bodies to a mononuclear cell (arrow) in the lamina propria emphasizes their small size and helps differentiate them from IELs.

Figure 3.128 Crypt architectural disturbance, indeterminate for small bowel allograft rejection. Additional apoptotic body examples (arrowheads).
KEY FEATURES of Allograft Rejection:
• Surveillance of small bowel allografts can be performed endoscopically through the stoma site.
• Biopsies should be taken away from the stoma to avoid chronic and regenerative changes.
• Histologic features are similar to GVHD and include increased chronic inflammation, crypt inflammation and injury, and apoptotic activity.
• The presence of crypt injury and crypt architectural disturbance indicates at least moderate acute rejection.
• Immediate and aggressive immunosuppressive therapy is required for small bowel allograft rejection to prevent graft loss and mortality.
FAQ: How many apoptotic bodies are required to establish a diagnosis of acute allograft rejection?
Answer: As many as or more than six apoptotic bodies per 10 crypts in addition to crypt injury and lymphocytic infiltration. If all three of the criteria are not met, the case is best considered as indeterminate for acute rejection.
RADIATION ENTERITIS
Advances in technology allow more precise delivery of radiation dosage and result in less side scatter damage; however the small bowel remains more susceptible to radiation injury than the large bowel, and a number of factors enhance radiation injury, particularly the presence of other diseases such as diabetes, hypertension, atherosclerosis, prior intestinal injury, and cardiovascular disease.56 The mechanism of injury is similar to that of ischemic enteritis whereby endothelial cell damage results in edema, fibrin deposition, and increases in vascular permeability.56 Correspondingly, the histologic features are similar to those seen in ischemic mesenteritis and include epithelial degeneration, mucosal denudation, crypt disintegration, mucosal edema, and necrosis (Figs. 3.129 and 3.130). Features indicating that tissues were within a radiation field include hyaline sclerosis of small vessels, intimal thickening and fibrosis of muscular arteries, endarteritis obliterans, and enlarged bizarre nuclei of endothelial cells and fibroblasts (Figs. 3.131 and 3.132).
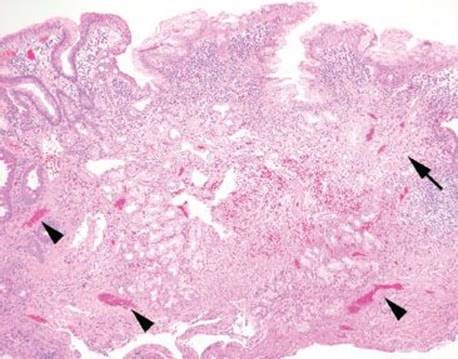
Figure 3.129 Crypt architectural disturbance, radiation enteritis. Low magnification shows crypt architectural disturbances including mild crypt distortion and loss of crypts (arrow). The lamina propria contains hemorrhage and muscular arteries show congestion (arrowheads). Surface foveolar gastric metaplasia is also present, but may be unrelated to the radiation changes.

Figure 3.130 Crypt architectural disturbance, radiation enteritis. Higher magnification of the previous figure highlights congested muscular arteries (arrowhead) and ectatic capillaries in the lamina propria (arrows).

Figure 3.131 Crypt architectural disturbance, radiation enteritis. Higher magnification of the previous figures shows an abnormally prominent muscular artery. Also note the lamina propria hemorrhage and early hyalinization.

Figure 3.132 Crypt architectural disturbance, radiation enteritis. Higher magnification of the artery in the previous figures shows enlarged endothelial cells with mild nuclear atypia.
POUCHITIS AND POUCH-RELATED CHANGES
Ileal pouch anal anastomosis (IPAA) is a procedure that consists of a total colectomy with stripping of the rectal mucosa and preservation of the anal sphincter. An ileal reservoir/pouch is constructed (sometimes termed “J-pouch”) and anastomosed either to the residual rectal cuff at the anus or directly to the anus itself (Fig. 3.133). This procedure is favored over total proctocolectomy with permanent ileostomy because it allows patients to retain sphincter function and intestinal continuity; it has been most often employed in patients with ulcerative colitis and familial adenomatous polyposis (FAP). Traditionally, the diagnosis of Crohn disease was an absolute contraindication for an IPAA because of high rates of pouch complications and failure; however recent studies have demonstrated good functional outcomes in the majority of Crohn disease patients, and suggest that trial IPAA may be offered to highly motivated patients wishing to avoid a permanent stoma.57–59 The most frequently observed long-term complication of IPAA is “pouchitis,” an acute and/or chronic inflammation of the ileal reservoir that remains poorly defined in regards to its true prevalence (reported as 7% to 44%),60–64 etiology, and natural history. Five to 10% of patient with IPAA develop chronic antibiotic-refractory pouchitis or Crohn disease of the pouch, both of which are leading causes of permanent diversion or pouch failure.65,66 Preoperative risk factors for pouchitis include use of steroids prior to colectomy, severe pancolitis, appendiceal involvement, extraintestinal manifestations of colitis and primary sclerosing cholangitis.61,67–69 Postoperative risk factors include bacterial overgrowth due to stasis, closure of ileostomy site, nonsteroidal anti-inflammatory drug use, and lack of short chain fatty acids in diet.70,71 Serologic markers show increased risk for pouchitis in patients with perinuclear anticytoplasmic antibodies (ANCA), whereas positive antibodies to anti-Saccharomyces cerevisiae (ASCA) have been linked to developing postoperative fistulas and a change in diagnosis to from ulcerative colitis to Crohn disease in patients with an IPAA.72

Figure 3.133 Ileal-pouch anal anastomosis (IPAA). Closure of a total proctocolectomy requires either an ostomy/stoma site or an IPAA (in this illustration the colon is “greyed out” to represent removal). IPAA is the preferred surgical approach because it maintains GIT continuity and avoids the need for a permanent enterostomy bag. IPAA involves anastomosis of the ileum either to the rectal cuff at the anus or directly to the anus itself. A reservoir is created by stitching two loops of ileum together and removing the internal walls. The resulting reservoir is in the shape of a “J” and often termed a “J-pouch.” Historically, IPAA was the standard of care for ulcerative colitis patients but was generally contraindicated in Crohn cases because of increased risks of disease flares, a view that has evolved.
Clinical manifestations of pouchitis include increased stool frequency, urgency, hematochezia, abdominal pain, and fever. These symptoms trigger biopsy of the pouch to exclude specific infection (such as cytomegalovirus) and other etiologies. If histologic changes support pouchitis, antibiotic therapy is instituted (Figs. 3.134 and 3.135). It should be noted, however, that histologic changes in the pouch are nonspecific. For example, long-standing pouches invariably contain chronic inflammation, villous blunting, crypt architectural disturbance and colonic metaplasia (Figs. 3.136 and 3.137).73,74 Moreover, while acute inflammation can support a clinical impression of pouchitis, neutrophils could also indicate residual/recurrent IBD, the histologic distinction of which should not be attempted without strong clinical correlation. IBD may be a consideration in the following scenarios:
• Biopsies of the rectal cuff show active chronic features discordant with those of the pouch proper; consider residual/recurrent ulcerative colitis (also referred to as “cuffitis”) (Figs. 3.138–3.143).
• Pouchitis has been refractory to multiple rounds of antibiotic therapy; consider pouch involvement of Crohn disease.

Figure 3.134 Crypt architectural disturbance, pouchitis. Pouchitis refers to acute and/or chronic inflammation of the ileal reservoir or “pouch” as a result of an ileal pouch anal anastomosis (IPAA). At low magnification, the mild crypt distortion, crypt dropout, expansion of the lamina propria with chronic inflammation and loss of villi are apparent.

Figure 3.135 Crypt architectural disturbance, moderate acute pouchitis. The presence of cryptitis and crypt abscesses (arrow) are consistent with moderate acute pouchitis, in the proper clinical setting.

Figure 3.136 Crypt architectural disturbance, chronic pouch changes. Over time, all pouches show chronic injury features, regardless of whether there is a history of acute pouchitis. This example lacks acute inflammation, but shows some mild crypt distortion and villous blunting.

Figure 3.137 Crypt architectural disturbance, chronic pouch changes mimicking colonic mucosa. This biopsy of a long-standing pouch shows residual Paneth cells (arrowheads) but no intact villi. Identical findings could be seen with cuffitis or inflammatory bowel disease involving the residual colon mucosa. Unfortunately, there are no reliable histologic features to distinguish pouchitis from cuffitis. In such cases, it is best that the endoscopist separately submit biopsies of the pouch and the rectal cuff in separate jars.

Figure 3.138 Crypt architectural disturbance, chronic pouch changes mimicking rectal cuff. It can be difficult to differentiate chronic pouchitis changes from rectal cuff tissue. Histologically, this biopsy could represent a pouch with chronic changes or rectal cuffitis. Samples from both the pouch and the rectal cuff sent in separate jars are most helpful in this distinction.

Figure 3.139 Crypt architectural disturbance, rectal cuffitis. This biopsy was taken from the rectal cuff and shows continued involvement by ulcerative colitis. There is crypt distortion and cryptitis present in a background of marked chronic inflammation.

Figure 3.140 Paired intact pouch. This pouch biopsy is paired with the previous cuffitis. The pouch shows intact architecture and long villi, with only mild expansion of the lamina propria. The stark contrast between the cuff and the pouch allows for easier distinction of which disease state is present –pouchitis or cuffitis. Based on separate submission of the pouch and cuff, this case features cuffitis, or inflammatory bowel disease changes involving the residual rectal cuff.

Figure 3.141 Crypt architectural disturbance, rectal cuffitis. Another example of rectal cuffitis demonstrates active and chronic features of ulcerative colitis, with crypt distortion and branching, crypt shortfall/basal lymphoplasmacytosis (arrow), crypt dropout, and marked lamina propria chronic inflammation. Moderate active and chronic pouchitis can look similar.

Figure 3.142 Crypt architectural disturbance, rectal cuffitis. Higher magnification of the previous figure shows cryptitis (arrowhead). Paneth cell metaplasia is also seen in the lower left crypt.

Figure 3.143 Paired intact pouch. This pouch biopsy is paired with the previous cuffitis. The intact and noninflamed pouch is a striking comparison to the cuffitis seen previously, allowing for confident differentiation between cuffitis and pouchitis. This case features cuffitis, or inflammatory bowel disease changes involving the residual rectal cuff.
• Extraintestinal and intestinal manifestations of Crohn disease become apparent (i.e., mucosal granulomata, uveitis, arthritis, small bowel stricture or fistula, perianal disease, etc.).
KEY FEATURES of Pouchitis:
• Ileal pouch anal anastomosis (IPAA) is a sphincter-sparing proctocolectomy that results in a small bowel reservoir (or “pouch”) attached to either the residual rectal cuff or directly to the anus.
• Pouchitis is a poorly defined inflammatory complication of this procedure.
• Symptoms include: stool frequency, urgency, hematochezia, abdominal pain, and fever.
• Biopsies of the pouch are sent to exclude specific infection (e.g., cytomegalovirus) and confirm active and chronic inflammation
• Histologic features of activity and chronicity support a clinical impression of pouchitis, but are nonspecific.
• There are no reliable histologic features to distinguish IBD from pouchitis.
• Residual or recurrent IBD involving the rectal cuff is known as “cuffitis.”
• Crohn disease should only be suggested if strong clinical correlation is available, such as:
• Antibiotic-refractory pouchitis
• Extraintestinal manifestations of Crohn disease
• Perianal disease
• Small bowel strictures or fistulas
PEARLS & PITFALLS
Recall that a residual cuff of rectal mucosa can remain distal to the pouch in construction of an IPAA. Detection of residual IBD in this rectal cuff (“cuffitis”) is important for prognostic and treatment purposes; however take caution, as metaplastic changes in the pouch can cause it to appear colonic and thus mistaken for cuffitis. Likewise, the chronic changes of IBD (i.e., Paneth cell metaplasia) in the rectal cuff can mimic small bowel mucosa and be mistaken for pouchitis; thus, ideally rectal cuff and pouch biopsies should be submitted separately by the endoscopist, and clearly labeled. IBD might be suggested by the pathologist when there is major histologic discordance among biopsy samples (i.e., one tissue fragment shows marked active and chronic changes, while the remaining fragments are unremarkable); see sample note below (Figs. 3.139 and 3.140).

Figure 3.144 Crypt architectural disturbance, prepouch biopsy with chronic changes. This prepouch biopsy shows marked lamina propria chronic inflammation, including lymphoid aggregate formation. Findings such as this may be found in the prepouch small bowel and should not be over-interpreted as Crohn disease.

Figure 3.145 Crypt architectural disturbance, prepouch biopsy with chronic changes. Another example of a prepouch biopsy showing chronic features (crypt distortion, dropout, and shortfall/basal lymphoplasmacytosis). Chronic changes such as this may be found in prepouch biopsies and do not indicate Crohn disease.
FAQ: Does active and chronic inflammation in the prepouch biopsy indicate the presence of Crohn disease?
Answer: No.
Inflammation proximal to the pouch, or “prepouch ileitis,” is common in patients with pouchitis (13%) and does not imply missed Crohn disease or predict pouch failure.75 The majority of patients (86%) with prepouch ileitis respond to antibiotic treatment, further supporting that prepouch ileitis is not a manifestation of Crohn disease.76 A diagnosis of Crohn disease can only be made in the proper clinical context; for example, if the patient demonstrates extraintestinal manifestations of Crohn disease, perianal disease, or small bowel strictures or fistulas (Figs. 3.144 and 3.145).
FAQ: Is pyloric gland metaplasia in ileal pouch biopsies a definitive marker for Crohn disease?
Answer: No.
Pyloric gland metaplasia (Fig. 3.146) is more common in patients who experience complication following an IPAA (55%) as compared to those who follow a normal postoperative course (12%). The prevalence is higher in patients with Crohn disease of the pouch (77%) as compared to ulcerative colitis patients with chronic pouchitis (22%), but cannot be used as a definitive marker for Crohn disease.77

Figure 3.146 Pyloric metaplasia (arrowheads) in chronic pouch changes does not necessarily implicate Crohn disease. It is a nonspecific sign of chronic mucosal injury.
FAQ: Can pouchitis be distinguished from IBD histologically?
Answer: No.
The histologic changes of active and chronic pouchitis are nonspecific and cannot be distinguished from the active and chronic changes seen in IBD. The function of pouch biopsies is to exclude other etiologies (e.g., cytomegalovirus infection) and to confirm the clinical impression of pouchitis. A diagnosis of Crohn disease can only be made in the proper clinical context (Figs. 3.147–3.152).

Figure 3.147 Anal transition. A helpful tip can sometimes be found in the biopsy. If biopsies contain the anal transition (arrowhead) of columnar mucosa to squamous, the biopsy is from the rectal cuff and not the pouch.

Figure 3.148 Crypt architectural disturbance, pouch with Crohn disease. This pouch shows nonspecific features of chronicity, including crypt branching and distortion and increased chronic inflammation. Following an IPAA procedure, this patient developed extraintestinal manifestations of Crohn disease, including uveitis, iritis, and arthritis. This case illustrates that, unfortunately, there are no reliable histologic features to distinguish pouchitis from inflammatory bowel disease: identical findings can be seen in both settings. Correlation with the clinical setting offers the best means to distinguish pouchitis from inflammatory bowel disease.

Figure 3.149 Crypt architectural disturbance, pouch with Crohn disease. Additional biopsies of the pouch from the same patient show marked crypt shortfall/basal lymphoplasmacytosis and chronic inflammation.

Figure 3.150 Crypt architectural disturbance, prepouch biopsies in patient with Crohn disease. Biopsies of the prepouch small bowel in the same patients show crypt distortion and crypt abscesses (arrowhead).

Figure 3.151 Crypt abscess in prepouch biopsy from previous case.

Figure 3.152 Crypt architectural disturbance, prepouch biopsies in patient with Crohn disease. Additional prepouch biopsies show features of chronicity. In the absence of pertinent clinical information, the findings are nonspecific.
SAMPLE NOTE: UNCOMPLICATED POUCH BIOPSY WITH ACUTE INFLAMMATION AND CHRONIC CHANGES FOR “SUSPECT POUCHITIS”
Ileum, Pouch, Biopsy:
• Mild acute inflammation with chronic mucosal changes, consistent with clinical impression of mild active chronic pouchitis.
SAMPLE NOTE: POUCH BIOPSY SENT FOR “RULE OUT CROHN DISEASE”
Ileoanal Pouch, Biopsy:
• Small intestinal mucosa with moderate acute inflammation and chronic mucosal injury changes.
Note: The histologic sections show small intestinal mucosa with crypt abscesses and chronic changes (marked villous blunting and increased lamina propria chronic inflammation) without granulomata. The features are nonspecific and are compatible with active chronic pouchitis in the proper clinical setting. Involvement by Crohn disease can show similar changes and this possibility cannot be entirely excluded. Correlation with clinical information is recommended.
SAMPLE NOTE: DISTAL POUCH OR RECTAL CUFF BIOPSY WITH FEATURES SUSPICIOUS FOR INFLAMMATORY BOWEL DISEASE
Ileum, Distal, and Postpouch Biopsies:
• Intestinal-type mucosa with moderately active chronic inflammatory disease and patchy ulceration.
Note: Long-standing chronic pouchitis may show metaplastic changes that mimic colonic mucosa; however, it is suspected this biopsy was taken from the rectal cuff and the findings represent active IBD (“cuffitis”). Correlation with endoscopic and clinical findings is suggested. No dysplasia identified.