
Figure 1.103 Esophageal eosinophilia. Numerous eosinophils are present in the squamous epithelium. This change is frequently, but not always, accompanied by basal compartment hyperplasia, elongation of the vascular papillae, and widened intercellular spaces (sometimes referred to as intercellular edema or spongiosis). In the absence of clinical history, the findings are nonspecific.
Eosinophils are a normal constituent of some mucosal real estate in the gastrointestinal tract, such as the lamina propria of the small intestine and colon (Fig. 1.103). However, the esophagus is unique in being devoid of eosinophils under normal conditions. While some disease entities are practically defined by a minimum number of eosinophils, the category “eosinophilic pattern of injury” is intended to capture the full spectrum of intraepithelial eosinophilia in the esophagus, whether there is only a single intraepithelial eosinophil, or >100 eosinophils in one high power field (HPF). Analogous to the other patterns of injury in this book, the differential diagnoses considered in the following pages are most applicable if eosinophilia is the primary pattern of injury. The presence of eosinophils is often, but not always, accompanied by additional findings including basal layer hyperplasia, elongation of the vascular papillae, intercellular edema or “spongiosis,” lamina propria sclerosis, acute inflammation, and intraepithelial lymphocytosis. These ancillary features may influence the priority order of the differential diagnoses, but none are specific. The end result is that the presence of eosinophils in the esophagus is a nonspecific finding, and is best regarded simply as a pattern of injury requiring correlation with clinical information.
FAQ: What are the constituents of the eosinophil’s cytoplasmic granules?
Answer: Eosinophils are distinctive white blood cells with bilobed nuclei and cytoplasm that contains numerous eosinophilic secondary granules composed of cytotoxic molecules (eosinophil peroxidase, major basic protein, eosinophil cationic protein, and eosinophil-derived neurotoxin).
CHECKLIST: Eosinophilic Pattern of Injury in the Esophagus
![]() Gastroesophageal Reflux Disease
Gastroesophageal Reflux Disease
![]() Idiopathic Eosinophilic Esophagitis
Idiopathic Eosinophilic Esophagitis
![]() Drug Reaction
Drug Reaction
![]() Food Allergy
Food Allergy
![]() Photodynamic Therapy
Photodynamic Therapy
![]() Systemic Collagen Vascular Disorders (Scleroderma)
Systemic Collagen Vascular Disorders (Scleroderma)
GASTROESOPHAGEAL REFLUX DISEASE
GERD is a condition in which the stomach contents backflow into the esophagus leading to esophageal damage and, when longstanding and severe, can eventually lead to metaplasia and neoplasia.28–34 Clinically, patients may present with odynophagia, heartburn, chest pain, regurgitation, hoarseness, or chronic cough. Treatment includes lifestyle modifications, such as weight loss and avoidance of citrus foods, spices, caffeine, alcohol, chocolate, and smoking. Medications to neutralize or inhibit acid production, including antacids, proton pump inhibitors (PPIs), H2-receptor blockers, and mucoprotective agents are common treatments. Surgical procedures such as endoscopic injection of the lower esophageal sphincter or Nissen fundoplication are effective alternatives for patients’ refractory to medical management. Endoscopically, esophageal erythema, erosions, and/or ulcerations can be seen. The severity of injury can vary greatly, but reflux disease typically affects the distal esophagus, starting at the gastroesophageal junction (Z-line) and extending proximally with tapering of inflammation. When proximal endoscopic irregularities are seen, iatrogenic or infectious etiologies are more likely.
KEY FEATURES of GERD (Figs. 1.104–1.108):
• Dilatation of intercellular spaces
• Basal hyperplasia, >15% of epithelial thickness
• Elongation of the vascular papillae, extending to top half of epithelium thickness
• Intraepithelial eosinophils
• Vascular lakes
• Increased intraepithelial T lymphocytes (squiggle cells)
• Balloon cells (epithelial cells with abundant pale cytoplasm)

Figure 1.104 Eosinophilic pattern, GERD. This example of GERD shows mild hyperplasia of the basal cell compartment, elongation of the vascular papillae, and scattered eosinophils in the squamous epithelium. Lamina propria is present in this biopsy, and it does not contain inflammatory cells or show evidence of sclerosis.

Figure 1.105 Eosinophilic pattern, GERD. This biopsy demonstrates characteristic reactive epithelial changes of basal cell hyperplasia, elongation of vascular papillae, and prominent intercellular edema (spongiosis). The inflammatory infiltrate is predominantly eosinophils. In the absence of clinical information, the findings of this biopsy are nonspecific. GERD, EoE, and other eosinophilic diseases of the esophagus are in the differential diagnosis.

Figure 1.106 Eosinophilic pattern, GERD. The biopsy fragment on the left of this field shows squamous epithelium with markedly increased eosinophils (arrowhead), intercellular edema (spongiosis), elongation of the vascular papillae, and basal cell hyperplasia (basal zone expansion). Alone, these findings are nonspecific and require clinical correlation for interpretation. However, the biopsy fragment on the right of the field clearly shows numerous goblet cells with bluish cytoplasmic mucin (arrow). The presence of intestinal metaplasia is consistent with Barrett esophagus and serves as histologic evidence of reflux disease, suggesting that the prominent eosinophilia seen in the squamous epithelium is secondary to reflux changes and not EoE.

Figure 1.107 Eosinophilic pattern, severe GERD. A single high-powered field in this biopsy shows >50 eosinophils in one high-powered field. Superficial layering of eosinophils toward the luminal surface (arrowhead) is also seen-–a feature that is more commonly seen in EoE than GERD. However, this biopsy comes from a patient with known severe reflux esophagitis, and it emphasizes the nonspecific nature of the histologic findings in both GERD and EoE. The parakeratotic debris seen on the surface is the result of adjacent ulceration and should not be mistaken for epithelial sloughing secondary to food impaction.

Figure 1.108 Eosinophilic pattern, severe GERD. Higher power of the previous figure. Careful examination of the background shows scattered eosinophil granules throughout this biopsy. This is a feature more commonly seen in EoE, but may also be seen GERD. The presence of neutrophils (arrowheads) is unusual for EoE, and these microabscesses may provide a clue that the histologic changes are secondary to GERD, despite the prominent eosinophilia and degranulation.
PEARLS & PITFALLS
When the eosinophils are few in number, limited to the distal esophagus, and are accompanied by a mixed inflammatory infiltrate, GERD is a more likely cause than eosinophilic esophagitis (EoE). However, in severe GERD, eosinophils can become a prominent finding, exceeding 15 eosinophils/HPF. As a result, histologic findings alone are not sufficient to discriminate eosinophilic esophagitis from GERD, and correlation with the clinicopathologic setting is important.
SAMPLE NOTE: NO CLINICAL HISTORY PROVIDED
Esophagus, Distal, Biopsy:
• Squamous esophageal mucosa with reactive epithelial changes and increased intraepithelial eosinophils (up to 20 intraepithelial eosinophils in one high-powered field).
Note: The biopsy shows prominent reactive changes and intraepithelial eosinophils. These findings are etiologically nonspecific and can be seen in the setting of GERD and/or EoE, among others. Correlation with the clinical information is necessary. In addition, if the possibility of EoE is a clinical consideration, tandem biopsies of the distal and mid- (or proximal-)esophagus are recommended.
EOSINOPHILIC ESOPHAGITIS (EOE)
EoE is defined as a clinicopathologic disease entity that is immune mediated (Figs. 1.109–1.122).28–34 It is characterized clinically by symptoms related to esophageal dysfunction and histologically by eosinophil-predominant inflammation. Clinically, patients commonly have concurrent allergic diatheses, especially food sensitization compared with the general population. Symptoms in the adult patient include dysphagia, chest pain, food impaction, and upper abdominal pain. In contrast, children tend to present with food aversion and vomiting. Frequently seen endoscopically are esophageal rings, either fixed or transient, which have also been described as corrugated rings, trachealization, or felinization of the esophagus (Fig. 1.109). Other findings include white exudates, longitudinal furrows (Fig. 1.110), edema, esophageal narrowing, and esophageal lacerations induced by passage of the endoscope (Fig. 1.111). The last finding, when severe, gives the esophagus the endoscopic appearance of crepe paper, and is thought to be a manifestation of mucosal fragility. However, all of these endoscopic features have been described in other conditions, and none can be considered pathognomonic for EoE. Histologically, one or more biopsy specimens must show a minimal peak value of 15 intraepithelial eosinophils/HPF, with few exceptions. For optimal pathologic evaluation, multiple biopsy specimens from both the proximal and distal esophagus should be obtained, as the distribution of eosinophils can be patchy. Unlike for reflux esophagitis, the presence of increased intraepithelial eosinophils proximally makes EoE more likely. EoE should remit with treatments of dietary exclusion, topical corticosteroids, or both (Table 1.1).

Figure 1.109 Endoscopic esophageal rings in EoE. Subtle circumferential rings are seen in the esophageal mucosa of this patient with eosinophilic esophagitis. This finding often raises the clinical suspicion of eosinophilic esophagitis, but only about one-third of patients with esophageal rings are confirmed to have esophageal eosinophils on biopsy.
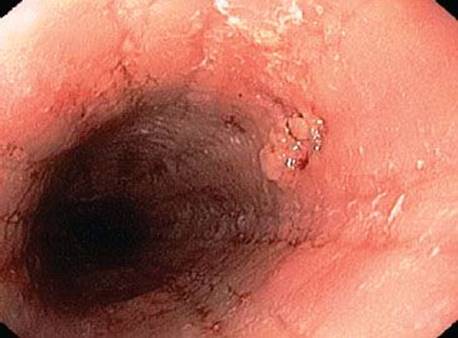
Figure 1.110 Endoscopic esophageal furrows in EoE. Linear furrows and whitish exudates can be seen in EoE. In the proper clinical setting, this finding can support but not establish a diagnosis of EoE.

Figure 1.111 Endoscopic esophageal trachealization in EoE. This dramatic endoscopic example shows fixed rings, or “trachealization,” and deep linear furrows in the esophagus of a patient with EoE. A mucosal laceration has been induced by the passage of the endoscope (arrow).

Figure 1.112 Feline esophagus. A cat esophagus from a veterinary necropsy shows the ridged esophageal mucosa from which the term “felinization” emerged to describe the endoscopic findings in EoE. (Photograph courtesy of Dr. Lysandra Voltaggio, Johns Hopkins Hospital.)

Figure 1.113 Eosinophilic pattern, basal cell hyperplasia in EoE. Although eosinophils may be difficult to readily identify at this low magnification, the presence of basal cell hyperplasia and elongation of the vascular papillae are striking, and are often the first clues to diagnosis. Also note the intercellular edema or “spongiosis,” which appears as a white lattice-like network.

Figure 1.114 Eosinophilic pattern, EoE. Higher magnification of a different EoE case shows similar features of basal cell hyperplasia, elongation of the vascular papillae, and spongiosis, as well as prominent intraepithelial eosinophils. The small amount of attached lamina propria at the base shows a suggestion of sclerosis, although it is difficult to confidently assess given the limited sample.

Figure 1.115 Eosinophilic pattern, eosinophilic microabscess in EoE. Some studies have shown that superficial layering of eosinophils toward the luminal surface and eosinophilic microabscesses (arrow) (defined as ≥4 eosinophils clustered together) are more common in EoE than in GERD.

Figure 1.116 Eosinophilic pattern, EoE. This example of EoE shows prominent eosinophils, but the additional features of basal cell hyperplasia, elongation of vascular papillae, and spongiosis are not as prominent, emphasizing that the histologic features exist along a spectrum, and may be patchy in the esophagus. Some superficial parakeratotic cells are shedding in this photo and is likely secondary to food impaction.

Figure 1.117 Eosinophilic pattern, EoE. Characteristic features of EoE are present, including prominent intraepithelial eosinophils, eosinophilic microabscesses, basal compartment hyperplasia, elongation of vascular papillae, and mild spongiosis. Careful examination of the photo will show numerous extracellular eosinophilic granules, evidence of eosinophil degranulation.

Figure 1.118 Eosinophilic pattern, eosinophil degranulation in EoE. At high magnification, eosinophil degranulation can be appreciated as a prominent feature in this case of EoE. Numerous superficial eosinophils and eosinophilic microabscesses are present, as well as prominent spongiosis. The surface squamous epithelial cells have faded nuclei or a “mummified” appearance. These squamous reactive changes are secondary to food impaction, which led to this patient’s endoscopy and diagnosis.
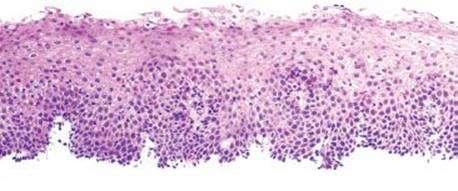
Figure 1.119 Eosinophilic pattern, food impaction in EoE. Characteristic low power features of basal compartment hyperplasia, elongation of vascular papillae, and spongiosis are present in this example. Intraepithelial eosinophils are present, as well as superficial reactive squamous epithelial changes. The faded appearance of some squamous epithelial cells and superficial parakeratosis are secondary to this patient’s food impaction.

Figure 1.120 Eosinophilic pattern, food impaction in EoE. Superficial parakeratosis and faded “mummified” squamous epithelial cells are present in this example of EoE with food impaction. The background epithelium shows markedly increased intraepithelial eosinophils and prominent spongiosis. Note the superficial eosinophilic microabscess (arrowhead).

Figure 1.121 Eosinophilic pattern, food impaction in EoE. Superficial parakeratosis is present in this biopsy from a patient with EoE and food impaction. The background epithelium shows mild spongiosis and increased eosinophils. The absence of lamina propria is common in esophageal biopsies.

Figure 1.122 Eosinophilic pattern, lamina propria sclerosis in EoE. Lamina propria is not frequently present in esophageal biopsies. However, this example shows abundant lamina propria with scattered eosinophils and densely pink collagenized stroma. This lamina propria sclerosis is a common finding in patients with EoE, and is not seen in patients with GERD. Compare the lamina propria in this photo with that seen in the photo of GERD (Fig. 1.104).
TABLE 1.1: Common Features of Eosinophilic Esophagitis (EoE) and Gastroesophageal Reflux Disease (GERD)

PEARLS & PITFALLS
Highlights of the 2011 Updated Consensus Recommendations31
• EoE is now the preferred abbreviation; EE has historically been reserved for erosive esophagitis.
• Definition: “EoE represents a chronic, immune/antigen-mediated, esophageal disease characterized clinically by symptoms of dysfunction and histologically by eosinophil-predominant inflammation.”
• EoE is a disease that is isolated to the esophagus, by definition. The presence of increased eosinophils in other areas of the gastrointestinal tract suggests the possibility of other disease entities, such as peripheral hypereosinophilic syndrome, idiopathic eosinophilic enteritis, connective tissue disease (particularly scleroderma), vasculitides, drug reaction, inflammatory bowel disease, and malignancies.
• There are no pathognomonic features of EoE, including no absolute lower limit of eosinophilia. However, a minimum peak value of 15 eosinophils/HPF is seen in the majority of cases.
• PPI-responsive esophageal eosinophilia is recommended to describe patients with eosinophilic-predominant esophageal disease who completely respond to PPI therapy.
FAQ: How does one quantify intraepithelial eosinophils for cases of “rule-out EoE”?
Answer: EoE is a clinicopathologic diagnosis and requires the presence of both pertinent clinical and histologic features: Neither component is diagnostic of EoE in isolation. The ideal practice pattern is to integrate the clinical setting, the endoscopic impression, and the morphologic findings of both the mid- or proximal esophagus and those at the distal esophagus to distinguish GERD from EoE. Specifically, the following elements can be included in reports.
• Approximate peak value eosinophil count of one HPF
• Presence of additional findings (microabscesses, surface layering, extracellular eosinophil granules, lamina propria fibrosis, and basal hyperplasia)
• Distribution of changes (e.g., proximal vs. distal esophagus)
• A comparison of these findings to previous material is often clinically requested, although its utility in the management of EoE remains unclear
FAQ: Eosinophilic infiltrates are seen in parasitic infections. Should the differential diagnosis of parasitic infection be raised when there is esophageal eosinophilia?
Answer: No. Parasitic infections essentially never affect the esophagus, and this does not need to be included in the differential diagnosis of esophageal eosinophilia unless prominent mucosal eosinophilia is also seen in other parts of the GI tract. In addition, while eosinophils may be part of the infiltrate of fungal or viral infections, the main injury pattern for these entities is typically acute esophagitis.

Figure 1.123 Eosinophilic pattern, pill esophagitis. An ibuprofen pill was lodged in this patient’s esophagus, resulting in an eosinophilic infiltrate (arrow), spongiosis and edema, mild parakeratosis, and reactive epithelial changes.

Figure 1.124 Eosinophilic pattern, pill esophagitis. This patient had an ibuprofen pill lodged in the esophagus. The resulting injury is interesting in its “tide-line” pattern (highlighted by arrowheads). Rare eosinophils may be found (between the two bottommost arrowheads).
SAMPLE NOTE: CLINICAL IMPRESSION SUGGESTIVE OF EOE
Esophagus, Mid, Biopsy:
• Squamous esophageal mucosa with markedly increased intraepithelial eosinophils (focally up to 35 eosinophils in one HPF).
Note: The history of food allergies, food impaction, and the clinical impression of esophageal linear furrows and trachealization is noted. The biopsies show a patchy increase in intraepithelial eosinophils with the peak eosinophil count at 35 eosinophils in one HPF. Additional findings include basal cell hyperplasia, elongation of the vascular papillae, and eosinophilic microabscesses. Changes in the midesophagus are more prominent than those in the distal esophagus. These findings would support a clinicopathologic diagnosis of eosinophilic esophagitis if in the proper clinical setting.
DRUG REACTION
Esophageal intraepithelial eosinophils can be seen in rare cases of drug reactions. It is unclear whether the eosinophilic inflammation is secondary to contact injury or a direct effect of the medication (Figs. 1.123–1.124).
ALLERGY
IgE-mediated food hypersensitivity has been implicated as an etiology for eosinophilic infiltrates in the esophagus. Allergic rhinitis, asthma, seasonal allergies, and eczema are also commonly seen in patients with high eosinophil counts in the esophagus. The distinction between known food allergies and EoE is not entirely clear, especially as the current etiology of EoE is also believed to be an antigen-driven process.31,33,35,36 However, identification and elimination of known allergens, such as food hypersensitivities, can resolve patient symptoms and esophageal eosinophilia. Thorough evaluation by an allergist or immunologist with evaluation of serum IgE levels and skin testing for immediate-type food allergy is warranted to identify food-induced allergic disease in patients with esophageal eosinophilia prior to diagnosis of idiopathic EoE (Fig. 1.125).
PHOTODYNAMIC THERAPY
Photodynamic therapy (PDT) is an endoscopic method of treatment for Barrett esophagus and associated dysplasia or early carcinoma.37 It was commonly used in the past and has largely been replaced by radiofrequency ablation (RFA). Many patients who have been treated with PDT remain under surveillance so their biopsies may be encountered. PDT uses a light source to activate an applied photosensitizing drug, resulting in activated oxygen molecules that ablate targets of interest. A small subset (3.4%) of patients who undergo PDT for Barrett esophagus demonstrate eosinophilic infiltrates that histologically resemble the changes seen in EoE. This eosinophilic infiltrate may present anywhere from several months to years following PDT, and the histologic features can include eosinophil degranulation, spongiosis, increased papillary height, and basal zone thickening (Figs. 1.126–1.128). However, unlike those with EoE, these patients do not have dysphagia.

Figure 1.125 Eosinophilic pattern, food allergy. Occasional scattered eosinophils (arrowheads) are seen in the esophageal biopsy of a patient with documented food allergies.

Figure 1.126 Eosinophilic pattern, photodynamic therapy (PDT). This esophageal biopsy shows basal zone expansion, elongation of the vascular papillae, marked intercellular edema, and prominent eosinophilic infiltrates, including superficial eosinophilic microabscess (arrowhead). While the histologic features are similar to those seen in EoE, this biopsy was obtained for follow-up of Barrett esophagus following photodynamic therapy. Importantly, this patient did not have clinical complaints of dysphagia, which essentially excludes EoE.

Figure 1.127 Eosinophilic pattern, PDT. This biopsy was taken from a patient who had received photodynamic therapy for dysplasia in Barrett esophagus. Note the intense eosinophilic infiltrate.

Figure 1.128 Eosinophilic pattern, PDT. This biopsy shows superficial layering of eosinophils, with eosinophilic microabscess formation and degranulation of eosinophils. These nonspecific features may raise the possibility of EoE, but correlation with clinical information is always a must. This patient had a history of photodynamic therapy for dysplasia in Barrett esophagus, a known cause of esophageal eosinophilia.

Figure 1.129 Eosinophilic pattern, scleroderma: An esophageal biopsy from a patient with scleroderma shows marked basal zone expansion and marked elongation of vascular papillae that nearly reach the surface epithelium (arrowheads). Scattered eosinophils are present throughout the biopsy, and a background of intraepithelial lymphocytes is also present. The presence of eosinophils in the esophagus is a nonspecific finding, and raises the possibility of collagen vascular disorders.
SYSTEMIC COLLAGEN VASCULAR DISORDERS (SCLERODERMA)
Systemic collagen vascular disorders, particularly scleroderma, have been reported to demonstrate increased mucosal eosinophils.38 While this finding is more common distally in the GI tract, some patients may demonstrate esophageal eosinophilia (Fig. 1.129).