
Figure 1.186 Inlet patch/gastric heterotopic mucosa. The biopsy shows oxyntic mucosa in a biopsy labeled as “proximal esophagus.” These findings are consistent with the clinicopathologic diagnosis of gastric inlet patch.

Figure 1.187 Inlet patch/heterotopic gastric mucosa. The corresponding endoscopic image shows a pink patch of mucosa (arrowheads) in the proximal esophagus.
The seemingly normal esophageal biopsy can hold clues to tricky diagnoses. Some of these entities are critical for patient care while others are more for academic interest and proper clinicopathologic agreement. While this list is by no means exhaustive, consider the following before releasing the apparent unremarkable esophageal biopsy.
GASTRIC INLET PATCH/HETEROTOPIC GASTRIC MUCOSA
Gastric inlet patches are most commonly found in the proximal, posterior cervical esophageal mucosa (Fig. 1.186). Some observers believe they are congenitally acquired through the incomplete replacement of the embryologic columnar esophageal epithelium by squamous epithelium, although others argue they are metaplastic growths in response to acid secretion.75–77 Gastric inlet patches were found in 0.18% of patients in a study of over 487,000 patients in tertiary centers.77 Most of the patients were men with a history of Barrett mucosa and, unexpectedly, they had an increased risk of adenocarcinoma arising in Barrett mucosa when compared to those without gastric inlet patches. These patients presented with dysphagia, odynophagia, globus sensation, hoarseness, cough, stridor, and asthma, and these symptoms correlated with the size of the lesion. The most common type of heterotopic gastric mucosa identified was oxyntic mucosa and up to 1% of gastric inlet patches contained intestinal mucosa (Figs. 1.186–1.187). Helicobacter infections were encountered in the gastric inlet patches, and these infections correlated with corresponding Helicobacter gastritis. Dysplasia and malignancy arising in the gastric inlet patch itself are exceedingly rare.
FAQ: What is the HGM classification scheme?
Answer: In 2004 von Rahden proposed a clinicopathologic classification scheme for esophageal heterotopic gastric mucosa (HGM) (inlet patch).75 While subclassification is not required in pathology reports, awareness of this scheme is worthwhile since it is occasionally encountered in clinical reports.
HGM I Asymptomatic
HGM II Symptomatic without pathologic findings
HGM III Symptomatic with morphologic changes
HGM IV Dysplasia present
HGM V Malignancy present
PANCREATIC HETEROTOPIA/METAPLASIA

Figure 1.188 Pancreatic heterotopia/metaplasia (PAS/AB). This focus was mistakenly diagnosed as Barrett esophagus because the pancreatic heterotopia/metaplasia (arrowheads) displayed alcianophilia on PAS/AB, mimicking the staining pattern of goblet cells.
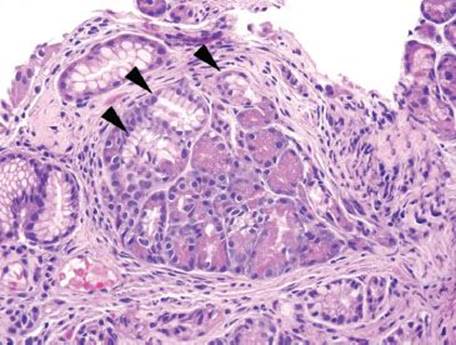
Figure 1.189 Pancreatic heterotopia/metaplasia. Comparison to the corresponding H&E reassures that there are no goblet cells. The pancreatic cells do not have distinct cytoplasmic distention (arrowheads), as would be expected for goblet cells.
Pancreatic acinar tissue occasionally raises concerns for goblet cells. Particularly challenging cases are those in which the pancreatic acinar tissue acquires an alcianophilia reminiscent of the deep basophilia of a goblet cell (Figs. 1.188 and 1.189). In such cases, it is worth noting that acinar cells lack distinct cytoplasmic distention and uniform strong purple staining, findings characteristic of goblet cells. Pancreatic heterotopia/metaplasia and oxyntic mucosa are also occasionally confused because, at low power, both entities have a similar two-toned admixture of cells displaying pink and purple staining. Pancreatic heterotopia, however, shows zonal distribution of color confined within an individual cell: The cytoplasm nearest the nucleus is purple, and the opposite is pink (Figs. 1.190–1.196). Oxyntic-type mucosa, in contrast, owes its two-toned appearance to a mixture of two distinct cell types (chief cells are purple and parietal cells are pink).

Figure 1.190 Pancreatic heterotopia/metaplasia. Pancreatic heterotopia/metaplasia can occasionally appear polypoid/nodular.

Figure 1.191 Pancreatic heterotopia/metaplasia (PAS/AB). Pancreatic heterotopia/metaplasia appears a dull blue (arrows) compared to the intermixed magenta cardiac glands (arrowheads).

Figure 1.192 Pancreatic heterotopia/metaplasia (PAS/AB). Higher power of previous figure.

Figure 1.193 Pancreatic heterotopia/metaplasia.

Figure 1.194 Pancreatic heterotopia/metaplasia. Higher power of previous figure. As shown here, pancreatic acinar cells show a zonal distribution of color with the cytoplasm nearest the nucleus purple, and the opposite pink. Oxyntic-type mucosa, in contrast, owes its two-toned appearance to a mixture of two distinct cell types (chief cells are purple and parietal cells are pink).

Figure 1.195 Pancreatic heterotopia/metaplasia.

Figure 1.196 Pancreatic heterotopia/metaplasia. Higher power of previous figure. Note the abundant eosinophilic zymogen granules, characteristic of pancreatic acinar cell differentiation.
GLYCOGENIC ACANTHOSIS

Figure 1.197 Glycogenic acanthosis. Low power shows characteristic epithelial hyperplasia with enlargement of mid-to-superficial cells. These cells of glycogenic acanthosis have abundant cytoplasm with a frosted-glass appearance, and they show no nuclear atypia. The basal compartment is unaffected.
Glycogenic acanthosis is a common esophageal lesion with a reported incidence 3% to 40% (Fig. 1.197).78–83 This benign hyperplasia of the squamous epithelium appears endoscopically as a gray-white mucosal plaque. The lesion is usually discrete with well-circumscribed borders, oval to round, and slightly raised (Figs. 1.197–1.209). The distal third of the esophagus is the most common site and lesions are usually multiple. Biopsies are often submitted to exclude Candida infection or neoplasia; the endoscopic appearance is indistinguishable from Candida, leukoplakia/epidermoid metaplasia, and lichen planus/“lichenoid” injury. Histologically, prominent cytoplasmic glycogen is seen, which distends the squamous epithelial cells and has a pale pink, frosted-glass texture. Typically, the basal layer is spared. PAS/D is helpful in equivocal cases and highlights a two-toned appearance of affected cells (Figs. 1.200and 1.209). Glycogenic acanthosis is benign and clinical follow-up or treatment is not necessary. Its diagnostic importance is in providing helpful feedback to the endoscopist to account for their abnormal clinical impression. Although rare associations with Cowden syndrome and celiac disease have been reported, the exact etiology of glycogenic acanthosis is not known.78,79 Some have postulated a relationship to GERD due to the predilection for the distal esophagus.

Figure 1.198 Glycogenic acanthosis nodule in the setting of Barrett esophagus. A well-circumscribed, raised white nodule (arrowhead) is present in the distal esophagus along with a salmon-colored patch (arrows) that is suggestive of Barrett esophagus. Glycogenic acanthosis typically shows multiple grey-white nodules or plaques.

Figure 1.199 Endoscopic view of glycogenic acanthosis. A discrete oval, gray-white plaque is seen in the distal esophagus (arrows). Endoscopically, the lesion can raise concern for Candida esophagitis.

Figure 1.200 Glycogenic acanthosis (PAS/D). A PAS/D stain from the previous case highlights the characteristic two-toned appearance with magenta accumulating on one aspect of the cell, the remaining cytoplasm cleared, and the basal layers uninvolved.

Figure 1.201 Glycogenic acanthosis (PAS/D). Higher power of previous. On PAS/D stain, the two-toned appearance is easily seen. Note the magenta stain marginalized to the superficial aspect of the cell and the remaining cytoplasm clear.

Figure 1.202 Raised nodule of glycogenic acanthosis. This lesion appeared as a nodule endoscopically, and was biopsied to exclude a neoplasm. The low-power view shows the epithelial hyperplasia that imparted that raised endoscopic appearance. The affected cells contain abundant pale cytoplasm, and the basal layer is unaffected.

Figure 1.203 Raised nodule of glycogenic acanthosis (PAS/D). A PAS/D stain highlights the two-toned appearance of the affected cells.

Figure 1.204 Raised nodule of glycogenic acanthosis (PAS/D). Higher power of previous. The two-toned appearance is the result of aggregation or marginalization of glycogen particles (magenta on PAS/D) and cytoplasmic clearing.

Figure 1.205 Focal glycogenic acanthosis. The abrupt transition between the lesion and the uninvolved epithelium is appreciated in this image. The enlarged cells have abundant pale cytoplasm with a frosted-glass texture.

Figure 1.206 Diffuse glycogenic acanthosis. In contrast to the previous image, this example shows diffusely involved epithelium. These cases can be subtle to the eye, as quick perusal might give the impression of normal or ballooned squamous cells. The clue to diagnosis is the abundant pale pink cytoplasm with a ground-glass or frosted-glass texture.

Figure 1.207 High power of glycogenic acanthosis cells: Higher power of previous. Unlike ballooned squamous cells, the cells of glycogenic acanthosis show abundant pale pink cytoplasm with a frosty appearance.

Figure 1.208 Glycogenic acanthosis with ballooned squamous cells. Epithelial hyperplasia and sparing of the basal compartment are characteristically present, as in this low-power view of glycogenic acanthosis. However, note that only the superficial most cells show the abundant pale pink and frosted-glass cytoplasm of glycogenic acanthosis (ovals). The remaining cells with cytoplasmic clearing have a hard basket weave appearance of ballooned squamous cells.

Figure 1.209 Glycogenic acanthosis with ballooned squamous cells. Only focal areas of this biopsy show cells affected by glycogenic acanthosis. These cells have abundant pale pink cytoplasm with a frosted-glass appearance (far left, and superficially) with rounded cytoplasmic borders. By comparison, the remaining cleared-out cells have dense, angulated cytoplasmic borders and a hard basket weave pattern.
FAQ: How can glycogenic acanthosis be distinguished from a balloon cell?
Answer: Glycogenic acanthosis shows pale pink, frosted-glass cytoplasm in distended squamous cells, and endoscopically presents as a nodule or plaque. A PAS/D confirms a two-tone appearance and the basal layer is uninvolved. Balloon cells are seen in a background of GERD-type changes and lack the above features.
SQUAMOUS PAPILLOMA

Figure 1.210 Squamous papilloma. Squamous papillomas are characterized by bland polypoid squamous mucosa overlying fibrovascular cores.
In the United States, squamous papillomas are rare lesions, seen in 0.07% of endoscopic material (Fig. 1.210). They are most often detected incidentally as a solitary nodule in the distal esophagus, more commonly in females (Fig. 1.211).84–87 Histologic sections show bland polypoid squamous mucosa with fibrovascular cores (Figs. 1.212–1.220). The majority of cases lack human papilloma viral cytopathic effect (koilocytosis, binucleation, hyperchromatic nuclei). The underlying etiology of these neoplasms is controversial. Some experts suggest squamous papillomas arise as a reparative response to chronic reflux disease based on their distal esophageal predominance. Others have suggested a possible role for human papillomavirus (HPV), particularly in the case of multiple, proximal papillomas with viral cytopathic effect. The inconsistent findings regarding an established link between squamous papilloma and HPV likely reflect variable population and assay technique. In general, the isolated squamous papilloma seldom progresses to dysplasia or carcinoma, and does not recur. Extensive papillomatosis, however, is even more rare with only few reports in the literature. This condition should prompt extensive sampling to exclude an underlying malignancy. Some experts include a comment on the presence or absence of viral cytopathic effect, dysplasia assessment, and HPV testing; however, this practice is not required, and is not universally adopted. A line-diagnosis “squamous papilloma” is sufficient, and inclusion of dysplasia assessment and viral cytopathic effect is necessary only when these features are present. HPV testing when viral cytopathic effect is present may be of academic interest, but is not currently a requirement. Importantly, correlation with the endoscopic impression is often worthwhile since tangential embedding of normal squamous mucosa can show similar features.
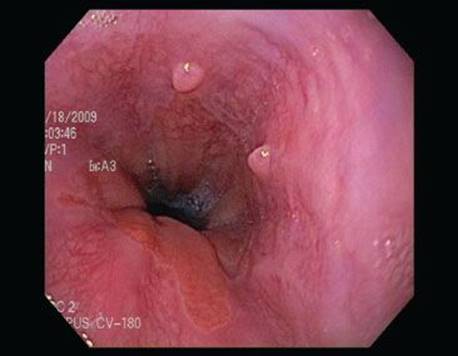
Figure 1.211 Squamous papilloma. Two smooth pink nodular lesions are seen just proximal to the gastroesophageal junction.

Figure 1.212 Squamous papilloma.

Figure 1.213 Squamous papilloma. Similar to this image, the majority of papillomas do not show viral cytopathic effect. The linkage between HPV and squamous papillomas of the esophagus varies among different patient populations.
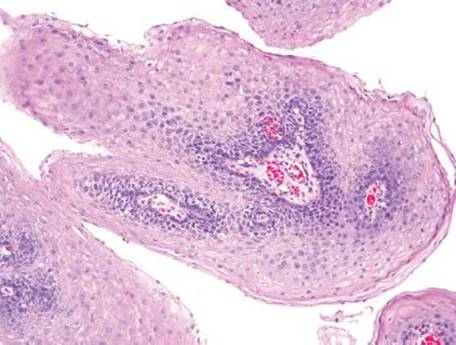
Figure 1.214 Squamous papilloma.

Figure 1.215 Squamous papilloma.

Figure 1.216 Squamous papilloma. Poor embedding or tangential sections can make squamous papillomas more difficult to recognize. This example does not show the typical papillary architecture, but the fibrovascular cores are present. The radiating pattern is a clue to the diagnosis of squamous papilloma.

Figure 1.217 Squamous papilloma.

Figure 1.218 Squamous papilloma.

Figure 1.219 Squamous papilloma.

Figure 1.220 Squamous papilloma with glycogenic acanthosis.
MULTILAYERED EPITHELIUM

Figure 1.221 Multilayered epithelium. Multilayered epithelium is a commonly encountered mimic of intestinal metaplasia. The epithelium shows a mixture of both squamoid and columnar features.

Figure 1.222 Multilayered epithelium (PAS/AB). A PAS/AB can be especially helpful in distinguishing the pseudogoblet cells of multilayered epithelium from the goblet cells of Barrett mucosa. The tinctorial properties of the mucin in multilayered mucosa (arrowheads) are a cross between those of goblet cells (purple) and foveolar mucosa (magenta).
Multilayered epithelium bears resemblance to both squamous and columnar mucosa with pseudogoblet cells (Figs. 1.221 and 1.222). Multilayered epithelium can appear quite atypical with complicated architecture and a striking resemblance to true goblet cells. Consequently, multilayered epithelium commonly raises concern for Barrett mucosa, or dysplasia arising in Barrett mucosa. Some experts regard multilayered mucosa as the precursor to Barrett mucosa.88–90 Literature in this area is limited and there are no official recommendations on the diagnosis or management of multilayered epithelium at this time. Consequently, this finding is nondiagnostic of Barrett mucosa and is not a required or recommended element of the pathology report.
PEARLS & PITFALLS
A PAS/AB can be quite helpful in distinguishing multilayered epithelium from Barrett mucosa: The tinctorial properties of the mucin in multilayered mucosa are a cross between those of goblet cells and foveolar epithelium (Fig. 1.222).
AMYLOID

Figure 1.223 Amyloidosis. Routine inspection of the lamina propria can lead to the recognition of subtle amyloid deposition. The lamina propria appears slightly glassy from the deposition of amyloid proteins. The characteristic cracking artifact is a helpful clue. A Congo red special stain confirmed the H&E diagnosis.
Abnormal deposition of amyloid proteins can occur anywhere along the GIT (Fig. 1.223). Deposition may occur within the lamina propria, muscularis mucosae, or vascular walls. The material appears glassy, amorphous, and occasionally fibrillary on routine H&E stain. The pale eosinophilic material may blend into the background appearing similar to collagen, but a characteristic cracking or “chatter” artifact is often present. Always consider the possibility of amyloid!
PEARLS & PITFALLS
Amyloid is one of the easiest findings to miss because of the subtle appearance of the deposition. In the esophagus, the diagnosis is especially challenging because the lamina propria is rarely provided in abundance. Routine inspection of the lamina propria, however, will forestall overlooking amyloid deposition.
GRANULAR CELL TUMOR

Figure 1.224 Granular cell tumor. Note the lamina propria at the far right aspects of this slide, which appears a bit smoother and more homogenous than the typical lamina propria. At this power, it is impossible to distinguish a granular cell tumor from amyloidosis or a sclerotic lamina propria.
Two percent of granular cell tumors originate in the esophagus, most in the distal esophagus (Fig. 1.224). Endoscopically, they appear as a well-marginated, submucosal nodule. Histologically, the neoplastic cells have abundant lightly pink, granular cytoplasm and small, pyknotic nuclei (Figs. 1.225–1.233). The cytoplasm contains abundant lysosomes, explaining the strong CD68 immunoreactivity despite their schwannian differentiation (GCT are also S100 immunoreactive). The cytoplasmic granules show retention upon periodic acid-Schiff staining with diastase digestion (PAS/D). Some lesions are associated with pseudoepitheliomatous hyperplasia, which can mimic invasive squamous cell carcinoma. While esophageal granular cell tumors are typically unifocal, benign lesions, rare reports of multicentricity and malignant transformation exist.91,92

Figure 1.225 Granular cell tumor. Higher power of previous figure. At higher power, rare cells with abundant eosinophilic cytoplasm and small pyknotic nuclei are seen (arrowhead). These cells showed strong and diffuse S100 protein reactivity. The overlying squamous mucosa shows striking pseudoepitheliomatous hyperplasia. This benign reactive epithelial change is characterized by irregular acanthosis with downward squamous proliferation that can mimic squamous cell carcinoma.

Figure 1.226 Granular cell tumor. Arrowheads highlight striking pseudoepitheliomatous hyperplasia. The surrounding lamina propria is expanded by a granular cell tumor.

Figure 1.227 Granular cell tumor. Higher power of previous figure. On higher power, the cells of the granular cell tumor show pale granular cytoplasm and mild nuclear atypia. Ultrastructural studies have shown these cells are filled with lysosomes. The pseudoepitheliomatous hyperplasia is seen extending downward, but the squamous cells lack prominent atypia or other features concerning for neoplasia.

Figure 1.228 Granular cell tumor. The pseudoepitheliomatous hyperplasia of this consultation case had been interpreted as invasive squamous cell carcinoma based on the infiltrative architecture of the squamous epithelium. However, examination of the underlying lamina propria shows numerous spindled and epithelioid eosinophilic cells with abundant granular cytoplasm. Recognition of the surrounding granular cell neoplasm was critical for arriving at the correct diagnosis.

Figure 1.229 Granular cell tumor. Higher power of previous figure. While the infiltrative squamous architecture is an eye-catching feature, always remember to check the underlying lamina propria before diagnosing a squamous cell carcinoma in the esophagus.

Figure 1.230 Granular cell tumor (S100 protein immunostain). Strong and diffuse S100 protein nuclear and cytoplasmic reactivity is seen in the granular tumor cells.
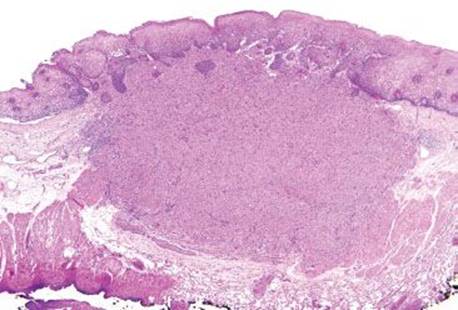
Figure 1.231 Granular cell tumor. This low-power view shows an unencapsulated submucosal-based mass extending upward to the epithelium and downward to the muscularis propria. The overlying squamous epithelium shows pseudoepitheliomatous hyperplasia with small finger-like projections downward. The finding should not be mistaken for invasive squamous cell carcinoma.

Figure 1.232 Granular cell tumor with prominent pseudoepitheliomatous hyperplasia. Higher power of previous figure. Irregular downward extension of squamous mucosa with mild reactive atypia. Never forget to examine the underlying lamina propria when this pattern is seen! The granular tumor cells in this example are slightly spindled, and should not be mistaken for lamina propria fibroblasts. When in doubt, an S100 protein immunostain is prudent, and can be especially helpful in small biopsies.
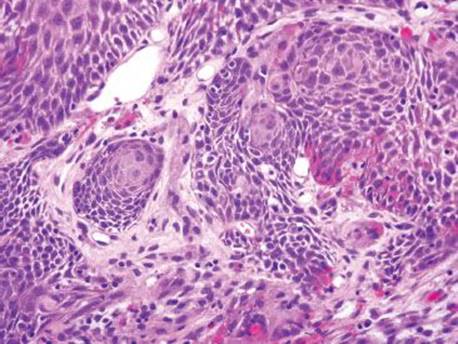
Figure 1.233 Granular cell tumor with prominent pseudoepitheliomatous hyperplasia. Higher power of previous figure.
PEARLS & PITFALLS
Granular cell tumor is yet another example of an entity that can be easily overlooked when only wisps of lamina propria are available. Typically, pseudoepitheliomatous hyperplasia is seen overlying the neoplasm, and this can serve as an important clue to the diagnosis. In addition, awareness of these benign epithelial changes is critical to avoid overdiagnosing invasive squamous cell carcinoma.
GRANULOMATA

Figure 1.234 Lamina propria granulomata. Poorly formed granulomata are important examples of other critical clues that can be hidden in the lamina propria.

Figure 1.235 Lamina propria granulomata. Higher power of previous case.
Poorly formed granulomata are important examples of other critical clues that can be hidden in the lamina propria (Fig. 1.234). This subtle finding is highly suggestive of Crohn disease and can be reliably identified if critical inspection of the lamina propria is routine (Figs. 1.235–1.239). AFB and GMS special stains for microorganisms are worthwhile.

Figure 1.236 Lamina propria granuloma. A poorly formed lamina propria granuloma in a patient ultimately diagnosed with Crohn disease.

Figure 1.237 Lamina propria granuloma. Higher power of previous case. AFB and GMS special stains were nonreactive.

Figure 1.238 Lamina propria granulomata. Poorly formed lamina propria granulomata in a patient with established Crohn disease.

Figure 1.239 Lamina propria granulomata. Higher power of previous case. AFB and GMS special stains were nonreactive.
APOPTOTIC BODY PROMINENCE

Figure 1.240 Apoptotic bodies. This esophageal biopsy features numerous apoptotic bodies. Upon chart review, the patient was a bone marrow recipient who presented with a cutaneous rash, fever, nausea, and vomiting. The patient was not taking mycophenolate mofetil and infectious etiologies had been excluded clinically. In this case, the prominent apoptotic bodies (arrowheads) were a manifestation of mild GVHD (grade I).

Figure 1.241 Apoptotic bodies associated with CMV infection. CMV esophagitis can also show a prominence of apoptotic bodies (arrowheads). In the setting of immunosuppression, a low threshold for ordering CMV immunohistochemistry is warranted.

Figure 1.242 CMV esophagitis. The corresponding CMV immunostain was reactive. In this case, increased apoptotic bodies was an important red flag to the underlying diagnosis of CMV esophagitis.
One apoptotic body per tissue fragment is permissible in the normal esophageal biopsy (Fig. 1.240). Conspicuous apoptotic bodies, however, can be clues to crucial diagnosis, listed below (Figs. 1.241 and 1.242). See also, GVHD, Lymphocytic pattern, this chapter.
• GVHD93
• Medication (i.e., NSAIDs, CellCept [MMF], among others)94–96
• CMV infection97
• Immunodeficiency disorders59
RING MITOSES (TAXOL AND COLCHICINE)
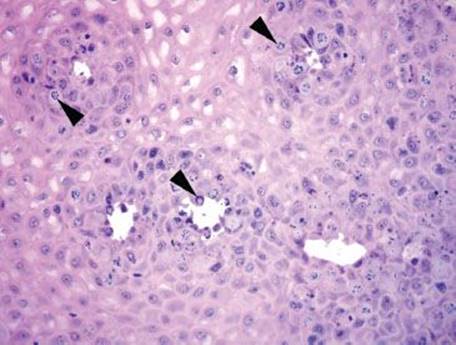
Figure 1.243 Taxane effect. Ring mitoses (arrowheads) can indicate taxane effect or colchicine toxicity; the latter is a clinical emergency requiring immediate notification of the clinician.

Figure 1.244 Taxane effect. Alternate field.
Taxanes (Taxol or paclitaxel, and Taxotere or docetaxel) are chemotherapeutic agents used in the treatment of breast, ovarian, and lung cancer, as well as Kaposi sarcoma (Figs. 1.243 and 1.244).98,99 Their mechanism of action involves stabilization of microtubules, resulting in mitotic ring forms and mitotic arrest. Importantly, recent taxane administration may cause changes that mimic high-grade dysplasia; therefore, biopsy immediately after Taxol administration should be avoided, if possible. In the setting of taxane administration, these histologic changes are indicative of taxane effect (not toxicity). In contrast, identical findings seen in the setting of colchicine usage would indicate colchicine toxicity, requiring immediate clinician notification.99
MALIGNANCY

Figure 1.245 Metastatic lobular breast carcinoma. This case featured an ulceration with nearby infiltration of cells with a “single file” configuration, occasional cytoplasmic vacuoles, scanty eosinophilic cytoplasm, and a mucinous background. The indicated cells were reactive for mammoglobulin and GCDFP-15, supporting the above diagnosis.
Certainly, complete evaluation always includes inspection for sneaky malignancies (Fig. 1.245).
References
1. Dent J. Microscopic esophageal mucosal injury in nonerosive reflux disease. Clin Gastroenterol Hepatol. 2007;5(1):4–16.
2. Geisinger KR. Endoscopic biopsies and cytologic brushings of the esophagus are diagnostically complementary. Am J Clin Pathol. 1995;103(3):295–299.
3. Bonacini M, Young T, Laine L. The causes of esophageal symptoms in human immunodeficiency virus infection. A prospective study of 110 patients. Arch Intern Med. 1991;151(8):1567–1572.
4. Wilcox CM, Schwartz DA. Endoscopic-pathologic correlates of Candida esophagitis in acquired immunodeficiency syndrome. Dig Dis Sci. 1996;41(7):1337–1345.
5. Lavery EA, Coyle WJ. Herpes simplex virus and the alimentary tract. Curr Gastroenterol Rep. 2008;10(4):417–423.
6. Lafferty WE, Coombs RW, Benedetti J, et al. Recurrences after oral and genital herpes simplex virus infection. Influence of site of infection and viral type. N Engl J Med. 1987;316(23):1444–1449.
7. Lafferty WE, Downey L, Celum C, et al. Herpes simplex virus type 1 as a cause of genital herpes: Impact on surveillance and prevention. J Infect Dis. 2000;181(4):1454–1457.
8. Goldblum JR, Richter JE, Vaezi M, et al. Helicobacter pylori infection, not gastroesophageal reflux, is the major cause of inflammation and intestinal metaplasia of gastric cardiac mucosa. Am J Gastroenterol. 2002;97(2):302–311.
9. Hackelsberger A, Günther T, Schultze V, et al. Prevalence and pattern of Helicobacter pylori gastritis in the gastric cardia. Am J Gastroenterol. 1997;92(12):2220–2224.
10. Abraham SC, Yardley JH, Wu TT. Erosive injury to the upper gastrointestinal tract in patients receiving iron medication: An underrecognized entity. Am J Surg Pathol. 1999;23(10):1241–1247.
11. Abraham SC, Bhagavan BS, Lee LA, et al. Upper gastrointestinal tract injury in patients receiving kayexalate (sodium polystyrene sulfonate) in sorbitol: Clinical, endoscopic, and histopathologic findings. Am J Surg Pathol.2001;25(5):637–644.
12. Seminerio J, McGrath K, Arnold CA, et al. Medication-associated lesions of the GI tract. Gastrointest Endosc. 2014;79(1):140–150.
13. Harel Z, Harel S, Shah PS, et al. Gastrointestinal adverse events with sodium polystyrene sulfonate (Kayexalate) use: A systematic review. Am J Med. 2013;126(3):264.e9–e24.
14. Rashid A, Hamilton SR. Necrosis of the gastrointestinal tract in uremic patients as a result of sodium polystyrene sulfonate (Kayexalate) in sorbitol: An underrecognized condition. Am J Surg Pathol.1997;21(1):60–69.
15. Lillemoe KD, Romolo JL, Hamilton SR, et al. Intestinal necrosis due to sodium polystyrene (Kayexalate) in sorbitol enemas: Clinical and experimental support for the hypothesis. Surgery.1987;101(3):267–272.
16. http://products.sanofi.us/kayexalate/kayexalate.pdf [cited 2013 February 16]. Available from: http://products.sanofi.us/kayexalate/kayexalate.pdf.
17. Slatopolsky EA, Burke SK, Dillon MA. RenaGel, a nonabsorbed calcium- and aluminum-free phosphate binder, lowers serum phosphorus and parathyroid hormone. The RenaGel Study Group. Kidney Int.1999;55(1):299–307.
18. Cozzolino M, Rizzo MA, Stucchi A, et al. Sevelamer for hyperphosphataemia in kidney failure: Controversy and perspective. Ther Adv Chronic Dis. 2012;3(2):59–68.
19. Qunibi WY, Hootkins RE, McDowell LL, et al. Treatment of hyperphosphatemia in hemodialysis patients: The calcium acetate renagel evaluation (CARE Study). Kidney Int. 2004;65(5):1914–1926.
20. Sonikian MA, Pani IT, Iliopoulos AN, et al. Metabolic acidosis aggravation and hyperkaliemia in hemodialysis patients treated by sevelamer hydrochloride. Ren Fail. 2005;27(2):143–147.
21. De Santo NG, Frangiosa A, Anastasio P, et al. Sevelamer worsens metabolic acidosis in hemodialysis patients. J Nephrol. 2006;19(suppl 9):S108–S114.
22. Pai AB, Shepler BM. Comparison of sevelamer hydrochloride and sevelamer carbonate: Risk of metabolic acidosis and clinical implications. Pharmacotherapy. 2009;29(5):554–561.
23. Swanson BJ, Limketkai BN, Liu TC, et al. Sevelamer crystals in the gastrointestinal tract (GIT): A new entity associated with mucosal injury. Am J Surg Pathol. 2013;37(11):1686–1693.
24. Chaplin AJ. The use of histological techniques for the demonstration of ion exchange resins. J Clin Pathol. 1999;52(10):776–779.
25. LiverTox: DRUG RECORD: Cholestyramine [cited 2013 February 15]. Available from: http://livertox.nih.gov/Cholestyramine.htm#insert.
26. Out C, Groen AK, Brufau G. Bile acid sequestrants: More than simple resins. Curr Opin Lipidol. 2012;23(1):43–55.
27. Abraham SC, Cruz-Correa M, Lee LA, et al. Alendronate-associated esophageal injury: Pathologic and endoscopic features. Mod Pathol. 1999;12(12):1152–1157.
28. Chehade M, Sampson HA, Morotti RA, et al. Esophageal subepithelial fibrosis in children with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2007;45(3):319–328.
29. Hurrell JM, Genta RM, Melton SD. Histopathologic diagnosis of eosinophilic conditions in the gastrointestinal tract. Adv Anat Pathol. 2011;18(5):335–348.
30. Lee S, de Boer WB, Naran A, et al. More than just counting eosinophils: Proximal oesophageal involvement and subepithelial sclerosis are major diagnostic criteria for eosinophilic oesophagitis. J Clin Pathol. 2010;63(7):644–647.
31. Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128(1):3–20.e6; quiz 21–22.
32. Rodrigo S, Abboud G, Oh D, et al. High intraepithelial eosinophil counts in esophageal squamous epithelium are not specific for eosinophilic esophagitis in adults. Am J Gastroenterol. 2008;103(2):435–442.
33. Rothenberg ME, Mishra A, Collins MH, et al. Pathogenesis and clinical features of eosinophilic esophagitis. J Allergy Clin Immunol. 2001;108(6):891–894.
34. Straumann A, Simon HU. The physiological and pathophysiological roles of eosinophils in the gastrointestinal tract. Allergy. 2004;59(1):15–25.
35. Mishra A, Hogan SP, Brandt EB, et al. An etiological role for aeroallergens and eosinophils in experimental esophagitis. J Clin Invest. 2001;107(1):83–90.
36. Straumann A, Bauer M, Fischer B, et al. Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J Allergy Clin Immunol. 2001;108(6):954–961.
37. Owens VL, Katzka DA, Lutzke LS, et al. Endoscopic ablative therapy for Barrett’s esophagus: A potential cause of eosinophilic esophagitis. Dis Esophagus. 2012;25(1):33–39.
38. DeSchryver-Kecskemeti K, Clouse RE. A previously unrecognized subgroup of “eosinophilic gastroenteritis”. Association with connective tissue diseases. Am J Surg Pathol. 1984;8(3):171–180.
39. Kaye MD. Esophageal leukoplakia. Gastrointest Endosc. 1987;33(3):254–259.
40. Lindsay JR. Esophageal lesions in diffuse scleroderma. Laryngoscope. 1949;59(2):83–112.
41. Singhi AD, Arnold CA, Crowder CD, et al. Esophageal leukoplakia or epidermoid metaplasia: A clinicopathological study of 18 patients. Mod Pathol. 2013;27(1):38–43.
42. Taggart MW, Rashid A, Ross WA, et al. Oesophageal hyperkeratosis: Clinicopathological associations. Histopathology. 2013;63(4):463–473.
43. Cameron RB. Esophagitis dissecans superficialis and alendronate: Case report. Gastrointest Endosc. 1997;46(6):562–563.
44. Carmack SW, Vemulapalli R, Spechler SJ, et al. Esophagitis dissecans superficialis (“sloughing esophagitis”): A clinicopathologic study of 12 cases. Am J Surg Pathol. 2009;33(12):1789–1794.
45. Hage-Nassar G, Rotterdam H, Frank D, et al. Esophagitis dissecans superficialis associated with celiac disease. Gastrointest Endosc. 2003;57(1):140–141.
46. Hokama A, Ihama Y, Nakamoto M, et al. Esophagitis dissecans superficialis associated with bisphosphonates. Endoscopy. 2007;39(suppl 1):E91.
47. Kaplan RP, Touloukian J, Ahmed AR, et al. Esophagitis dissecans superficialis associated with pemphigus vulgaris. J Am Acad Dermatol. 1981;4(6):682–687.
48. Rubio CA, Sjödahl K, Lagergren J. Lymphocytic esophagitis: A histologic subset of chronic esophagitis. Am J Clin Pathol. 2006;125(3):432–437.
49. Cohen S, Saxena A, Waljee AK, et al. Lymphocytic esophagitis: A diagnosis of increasing frequency. J Clin Gastroenterol. 2012;46(10):828–832.
50. Haque S, Genta RM. Lymphocytic oesophagitis: Clinicopathological aspects of an emerging condition. Gut. 2012;61(8):1108–1114.
51. Purdy JK, Appelman HD, Golembeski CP, et al. Lymphocytic esophagitis: A chronic or recurring pattern of esophagitis resembling allergic contact dermatitis. Am J Clin Pathol. 2008;130(4):508–513.
52. Abraham SC, Ravich WJ, Anhalt GJ, et al. Esophageal lichen planus: Case report and review of the literature. Am J Surg Pathol. 2000;24(12):1678–1682.
53. Calabrese C, Fabbri A, Benni M, et al. Squamous cell carcinoma arising in esophageal lichen planus. Gastrointest Endosc. 2003;57(4):596–599.
54. Chandan VS, Murray JA, Abraham SC. Esophageal lichen planus. Arch Pathol Lab Med. 2008; 132(6):1026–1029.
55. Dickens CM, Heseltine D, Walton S, et al. The oesophagus in lichen planus: An endoscopic study. BMJ. 1990;300(6717):84.
56. Quispel R, van Boxel OS, Schipper ME, et al. High prevalence of esophageal involvement in lichen planus: A study using magnification chromoendoscopy. Endoscopy. 2009;41(3):187–193.
57. Schwartz MP, Sigurdsson V, Vreuls W, et al. Two siblings with lichen planus and squamous cell carcinoma of the oesophagus. Eur J Gastroenterol Hepatol. 2006;18(10):1111–1115.
58. Salaria SN, Abu Alfa AK, Cruise MW, et al. Lichenoid esophagitis: Clinicopathologic overlap with established esophageal lichen planus. Am J Surg Pathol. 2013;37(12):1889–1894.
59. Daniels JA, Lederman HM, Maitra A, et al. Gastrointestinal tract pathology in patients with common variable immunodeficiency (CVID): A clinicopathologic study and review. Am J Surg Pathol.2007;31(12):1800–1812.
60. Agbaht K, Altintas ND, Topeli A, et al. Transfusion-associated graft-versus-host disease in immunocompetent patients: Case series and review of the literature. Transfusion. 2007;47(8):1405–1411.
61. Perri R, Assi M, Talwalkar J, et al. Graft vs. host disease after liver transplantation: A new approach is needed. Liver Transpl. 2007;13(8):1092–1099.
62. Velasco-Guardado A, López-Corral L, Alvarez-Delgado A, et al. Endoscopic evaluation and histological findings in graft-versus-host disease. Rev Esp Enferm Dig. 2012;104(6):310–314.
63. Thompson B, Salzman D, Steinhauer J, et al. Prospective endoscopic evaluation for gastrointestinal graft-versus-host disease: Determination of the best diagnostic approach. Bone Marrow Transplant.2006;38(5):371–376.
64. Cheung DY, Kim JI, Kim SS, et al. Endoscopic evaluation in gastrointestinal graft-versus-host disease: Comparisons with histological findings. Dig Dis Sci. 2008;53(11):2947–2954.
65. Ross WA, Ghosh S, Dekovich AA, et al. Endoscopic biopsy diagnosis of acute gastrointestinal graft-versus-host disease: Rectosigmoid biopsies are more sensitive than upper gastrointestinal biopsies. Am J Gastroenterol.2008;103(4):982–989.
66. Roy J, Snover D, Weisdorf S, et al. Simultaneous upper and lower endoscopic biopsy in the diagnosis of intestinal graft-versus-host disease. Transplantation. 1991;51(3):642–646.
67. Washington K, Bentley RC, Green A, et al. Gastric graft-versus-host disease: A blinded histologic study. Am J Surg Pathol. 1997;21(9):1037–1046.
68. Washington K, Jagasia M. Pathology of graft-versus-host disease in the gastrointestinal tract. Hum Pathol. 2009;40(7):909–917.
69. Lerner KG, Kao GF, Storb R, et al. Histopathology of graft-vs.-host reaction (GvHR) in human recipients of marrow from HL-A-matched sibling donors. Transplant Proc. 1974;6(4):367–371.
70. Shulman HM, Kleiner D, Lee SJ, et al. Histopathologic diagnosis of chronic graft-versus-host disease: National Institutes of Health Consensus Development Project on criteria for clinical trials in chronic graft-versus-host disease: II. Pathology Working Group Report. Biol Blood Marrow Transplant. 2006;12(1):31–47.
71. Star KV, Ho VT, Wang HH, et al. Histologic features in colon biopsies can discriminate mycophenolate from GVHD-induced colitis. Am J Surg Pathol. 2013;37(9):1319–1328.
72. Vigorito AC, Campregher PV, Storer BE, et al. Evaluation of NIH consensus criteria for classification of late acute and chronic GVHD. Blood. 2009;114(3):702–708.
73. Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–956.
74. Lee SJ, Klein JP, Barrett AJ, et al. Severity of chronic graft-versus-host disease: Association with treatment-related mortality and relapse. Blood. 2002;100(2):406–414.
75. Poyrazoglu OK, Bahcecioglu IH, Dagli AF, et al. Heterotopic gastric mucosa (inlet patch): Endoscopic prevalence, histopathological, demographical and clinical characteristics. Int J Clin Pract.2009;63(2):287–291.
76. von Rahden BH, Stein HJ, Becker K, et al. Heterotopic gastric mucosa of the esophagus: Literature-review and proposal of a clinicopathologic classification. Am J Gastroenterol. 2004;99(3):543–551.
77. Neumann WL, Luján GM, Genta RM. Gastric heterotopia in the proximal oesophagus (“inlet patch”): Association with adenocarcinomas arising in Barrett mucosa. Dig Liver Dis. 2012;44(4):292–296.
78. Hizawa K, Iida M, Matsumoto T, et al. Gastrointestinal manifestations of Cowden’s disease. Report of four cases. J Clin Gastroenterol. 1994;18(1):13–18.
79. McGarrity TJ, Wagner Baker MJ, Ruggiero FM, et al. GI polyposis and glycogenic acanthosis of the esophagus associated with PTEN mutation positive Cowden syndrome in the absence of cutaneous manifestations. Am J Gastroenterol. 2003;98(6):1429–1434.
80. Rywlin AM, Ortega R. Glycogenic acanthosis of the esophagus. Arch Pathol. 1970;90(5):439–443.
81. Stern Z, Sharon P, Ligumsky M, et al. Glycogenic acanthosis of the esophagus. A benign but confusing endoscopic lesion. Am J Gastroenterol. 1980;74(3):261–263.
82. Bender MD, Allison J, Cuartas F, et al. Glycogenic acanthosis of the esophagus: A form of benign epithelial hyperplasia. Gastroenterology. 1973;65(3):373–380.
83. Suoglu OD, Emiroglu HH, Sokucu S, et al. Celiac disease and glycogenic acanthosis: A new association? Acta Paediatr. 2004;93(4):568–570.
84. Attila T, Fu A, Gopinath N, et al. Esophageal papillomatosis complicated by squamous cell carcinoma. Can J Gastroenterol. 2009;23(6):415–419.
85. Fernández-Rodríguez CM, Badia-Figuerola N, Ruiz del Arbol L, et al. Squamous papilloma of the esophagus: Report of six cases with long-term follow-up in four patients. Am J Gastroenterol.1986;81(11):1059–1062.
86. Mosca S, Manes G, Monaco R, et al. Squamous papilloma of the esophagus: Long-term follow up. J Gastroenterol Hepatol. 2001;16(8):857–861.
87. Politoske EJ. Squamous papilloma of the esophagus associated with the human papillomavirus. Gastroenterology. 1992;102(2):668–673.
88. Glickman JN, Chen YY, Wang HH, et al. Phenotypic characteristics of a distinctive multilayered epithelium suggests that it is a precursor in the development of Barrett’s esophagus. Am J Surg Pathol.2001;25(5):569–578.
89. Glickman JN, Spechler SJ, Souza RF, et al. Multilayered epithelium in mucosal biopsy specimens from the gastroesophageal junction region is a histologic marker of gastroesophageal reflux disease. Am J Surg Pathol.2009;33(6):818–825.
90. Upton MP, Nishioka NS, Ransil BJ, et al. Multilayered epithelium may be found in patients with Barrett’s epithelium and dysplasia or adenocarcinoma. Dig Dis Sci. 2006;51(10):1783–1790.
91. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, et al. Malignant granular cell tumor of soft tissue: Diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22(7):779–794.
92. Wang J, Zhu XZ, Zhang RY. [Malignant granular cell tumor: A clinicopathologic analysis of 10 cases with review of literature]. Zhonghua Bing Li Xue Za Zhi. 2004;33(6):497–502.
93. Snover DC, Weisdorf SA, Vercellotti GM, et al. A histopathologic study of gastric and small intestinal graft-versus-host disease following allogeneic bone marrow transplantation. Hum Pathol.1985;16(4):387–392.
94. Fecker LF, Stockfleth E, Nindl I, et al. The role of apoptosis in therapy and prophylaxis of epithelial tumours by nonsteroidal anti-inflammatory drugs (NSAIDs). Br J Dermatol. 2007;156 (suppl 3):25–33.
95. Jana NR. NSAIDs and apoptosis. Cell Mol Life Sci. 2008;65(9):1295–1301.
96. Nguyen T, Park JY, Scudiere JR, et al. Mycophenolic acid (cellcept and myofortic) induced injury of the upper GI tract. Am J Surg Pathol. 2009;33(9):1355–1363.
97. Snover DC. Mucosal damage simulating acute graft-versus-host reaction in cytomegalovirus colitis. Transplantation. 1985;39(6):669–670.
98. Daniels JA, Gibson MK, Xu L, et al. Gastrointestinal tract epithelial changes associated with taxanes: Marker of drug toxicity versus effect. Am J Surg Pathol. 2008;32(3):473–477.
99. Iacobuzio-Donahue CA, Lee EL, Abraham SC, et al. Colchicine toxicity: Distinct morphologic findings in gastrointestinal biopsies. Am J Surg Pathol. 2001;25(8):1067–1073.