Vincent Di Marino1 and Hubert Lepidi1
(1)
UER Médecine, Aix-Marseille Université, Marseille, France
Abstract
The tissue of the corpora cavernosa clitoridis, or cavernous tissue, is erectile tissue, meaning its histological structure enables these bodies to fill with blood, increase in size and harden. This tissue is made up of a complex network of venous sinuses that appear as intercommunicating anfractuous cavities (cavernous labyrinth) and of a thick fibrous envelope, the albuginea, which was long believed, erroneously, to be inextensible. The sinusoid cavities, or sinuses of the corpora cavernosa, most often have wide-open lumina (though sometimes collapsed) that are very irregular. Their dimensions vary greatly. Their shapes are more often polyhedral or narrow and elongated rather than circular or oval. These sinuses present numerous recesses. The inter-sinus communications are clearly visible and the main characteristic of the sinuses is that they are richly anastomotic (Fig. 6.1). The wall of the sinuses is indeed a vessel wall, comprising an endothelial layer and a conjunctive axis made of collagenous bundles in which smooth muscle fibres may be seen. Specific stains (orcein) demonstrate the existence of a rich network of elastic fibres (Fig. 6.2). It should be noted that the walls of the sinuses are thin, especially if compared to the size of the vessel lumina. The endothelial cells, made apparent by the immunolabelling with an anti-factor VIII antibody, have junctions of varying tightness and rest on a basal lamina. Extensions originate from the sinus walls and float in the vessel lumina. Their role is probably to direct blood flow during filling. Most of these extensions appear as fingers that are curved to varying degrees (like a bent index finger). They may also take the shape of small mounts, pyramids, bull horns, points, hooks or clubs. There are also complete or incomplete bridges between two opposite sinus banks, the sinus septa, which contribute to making the sinus labyrinth even more complex. Numerous small vessels (arterioles or venules) are also housed in the sinus walls. These small vessels are very sinuous and their walls are often thick. The arterioles and their branches are called “helicine” due to their often helicoidal arrangement (see Chap. 10). The larger vessels are located at intersections in the inter-sinus connective tissue. Otherwise, a fair number of nerve endings are found in the sinus walls themselves and in the inter-sinus connective tissue (Fig. 7.2).
6.1 Cavernous and Spongy Tissue
6.1.1 Cavernous Tissue
The tissue of the corpora cavernosa clitoridis, or cavernous tissue, is erectile tissue, meaning its histological structure enables these bodies to fill with blood, increase in size and harden. This tissue is made up of a complex network of venous sinuses that appear as intercommunicating anfractuous cavities (cavernous labyrinth) and of a thick fibrous envelope, the albuginea, which was long believed, erroneously, to be inextensible. The sinusoid cavities, or sinuses of the corpora cavernosa, most often have wide-open lumina (though sometimes collapsed) that are very irregular. Their dimensions vary greatly. Their shapes are more often polyhedral or narrow and elongated rather than circular or oval. These sinuses present numerous recesses. The inter-sinus communications are clearly visible and the main characteristic of the sinuses is that they are richly anastomotic (Fig. 6.1). The wall of the sinuses is indeed a vessel wall, comprising an endothelial layer and a conjunctive axis made of collagenous bundles in which smooth muscle fibres may be seen. Specific stains (orcein) demonstrate the existence of a rich network of elastic fibres (Fig. 6.2). It should be noted that the walls of the sinuses are thin, especially if compared to the size of the vessel lumina. The endothelial cells, made apparent by the immunolabelling with an anti-factor VIII antibody, have junctions of varying tightness and rest on a basal lamina. Extensions originate from the sinus walls and float in the vessel lumina. Their role is probably to direct blood flow during filling. Most of these extensions appear as fingers that are curved to varying degrees (like a bent index finger). They may also take the shape of small mounts, pyramids, bull horns, points, hooks or clubs. There are also complete or incomplete bridges between two opposite sinus banks, the sinus septa, which contribute to making the sinus labyrinth even more complex. Numerous small vessels (arterioles or venules) are also housed in the sinus walls. These small vessels are very sinuous and their walls are often thick. The arterioles and their branches are called “helicine” due to their often helicoidal arrangement (see Chap. 10). The larger vessels are located at intersections in the inter-sinus connective tissue. Otherwise, a fair number of nerve endings are found in the sinus walls themselves and in the inter-sinus connective tissue (Fig. 7.1).
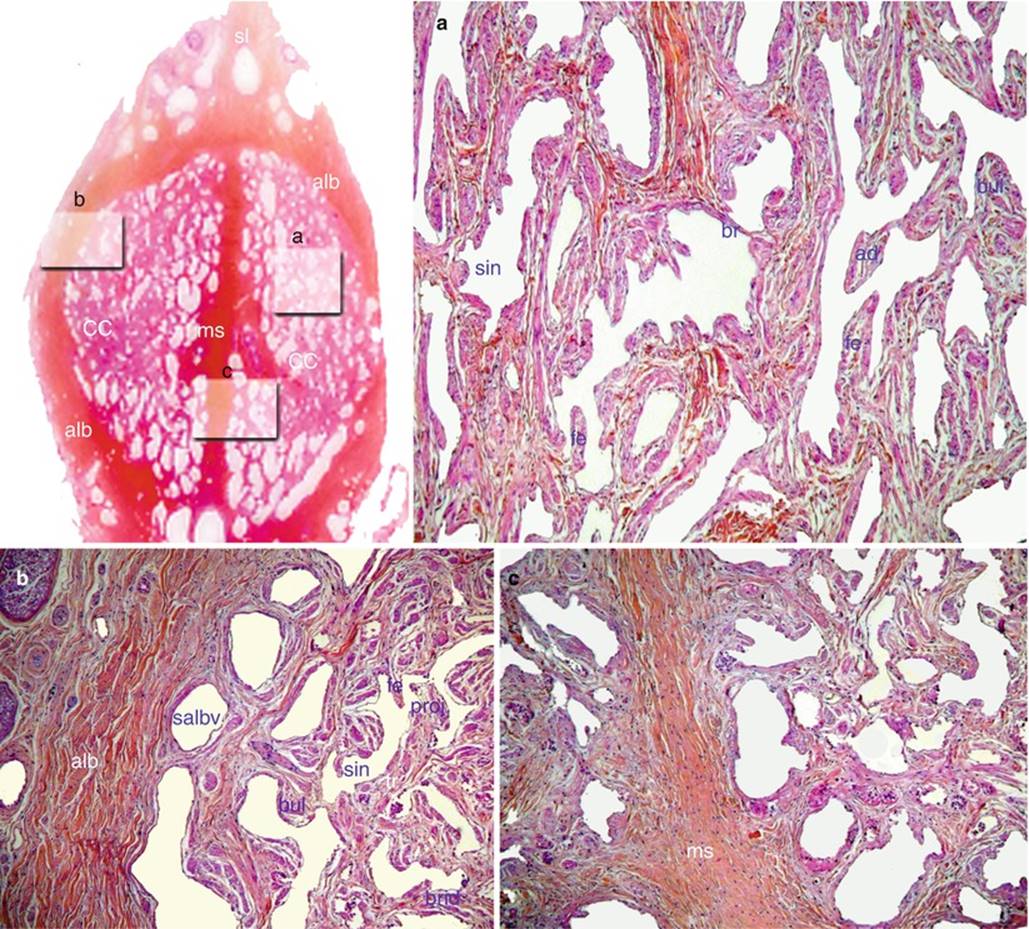
Fig. 6.1
Details of a frontal section through the descending part of the clitoral body showing the organisation of the corpora cavernosa. Part (a) of the section: the cavernous labyrinth; part (b) of the section: tunica albuginea and corpus cavernosum; part (c) of the section: the median septum and the corpora cavernosa. ad advance, alb tunica albuginea, brid bridge, bul bulge, cc corpus cavernosum, fe finger-like extension, ms median septum, proj projection, sin sinus, sl suspensory ligament, salbv sub-albugineous vein
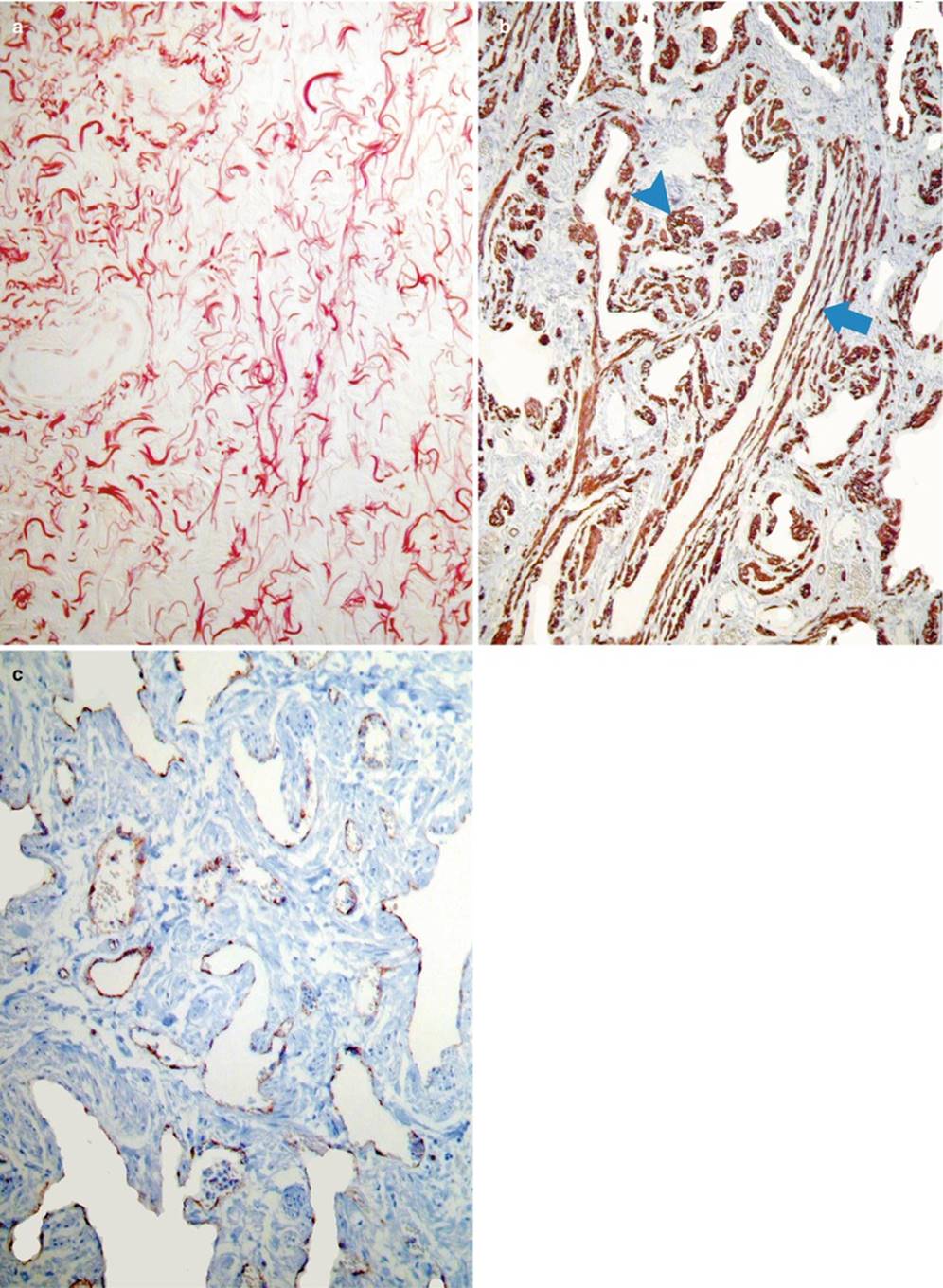
Fig. 6.2
Microarchitecture of the clitoral corpora cavernosa (histochemical study by specific staining of frontal sections of the clitoral body). (a) Staining by orceine: highlighting the elastic fibres. (b) Staining by smooth actin: highlighting the bundles of smooth muscle fibres (wine coloured) oriented in all directions, transversely (blue arrow) or longitudinally (blue arrowhead). (c) Staining by factor VIII: highlighting the endothelial cells: brown colour of the endothelia of the cavernosus maze and of the vascular endothelia. These endothelial cells secrete NO!
It is now proven that the work on corpora cavernosa of the penis can be transposed to the clitoral corpora cavernosa (A. Toesca et al.). Without negating the previous description, this work, notably that of A.M.B. Goldstein et al., demonstrates that instead of viewing the cavernous tissue as a labyrinth of sinuses with walls made of collagenous fibres and smooth muscle fibres, it should be considered as a fibrous collagenous tissue, rich in smooth muscle fibres, in which a network of intercommunicating vascular spaces are housed.
The inter-sinus connective tissue is made up of collagenous fibrous bundles which have the morphological characteristic of being wavy when in a state of rest (Fig. 6.3). According to E. Wespes, who for the most part, studied the penis corpora cavernosa, it is the presence of elastic fibres arranged in a bridge in contact with the collagenous bundles that enables the collagenous fibres to maintain this pleated appearance when in the flaccid phase and, most of all, to return to it as sexual arousal wanes.
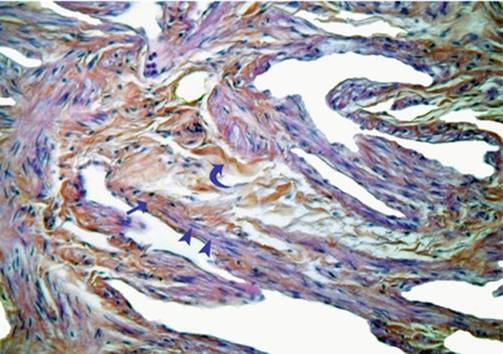
Fig. 6.3
Microarchitecture of the clitoral corpora cavernosa (Details of the cavernous network on a section of the clitoral body). The collagen fibres and the fibroblasts have an orange colour. The smooth muscular cells have a mauve colour. Note: At rest, the collagen fibres have an undulating shape (curved blue arrow). The smooth muscular cells, with flat and elongated nuclei (blue arrowheads), settle on the bundles of collagen fibres (right blue arrow)
The smooth muscle fibres of the clitoral corpora cavernosa were clearly identified using immunohistochemistry methods as the anti-desmin antibody affixes to them specifically. Alpha-smooth actin staining may also be used (Fig. 6.2). These muscle fibres have a longitudinal or transversal orientation within the inter-sinus connective tissue (A. Toesca). They are arranged as bundles or packets and end on collagenous fibres (Fig. 6.3) from which they will eliminate the folds to enable clitoral tumescence. These smooth muscle fibres are also present at the large arteriole and venule adventitia and then disappear on the small vessels. All of these smooth muscle fibres are interconnected. They therefore play a manifest contractile role in the regulation of sinus blood flow, as indicated by the author cited above. Their spontaneous myogenic activity corresponds to the flaccid state and their release only occurs during sexual arousal when the NO neurotransmitter is produced (see Chap. 7). Studied by electron microscopy (E. Wespes), these smooth muscle fibres demonstrate all characteristics of myogenic cells: uniform nucleus, fine basement membrane and above all, in the cytoplasm, mitochondria, contractile filaments and glycogen granules (energy nutrient).
Our microscopic observations demonstrated the existence of a sub-albugineal venous plexus in the clitoral corpora cavernosa, analogous to its well-known counterpart of the corpora cavernosa penis (Fig. 6.4). It is therefore surprising that certain authors negate the existence of this plexus (including A. Toesca). It is the compression of the veins of this plexus against the albuginea by the dilated cavernous sinusoids that prevents blood from leaving the corpora cavernosa and causes rigidity. Therefore, if this venous plexus did not exist, the clitoris would not have erectile capacity during sexual arousal.
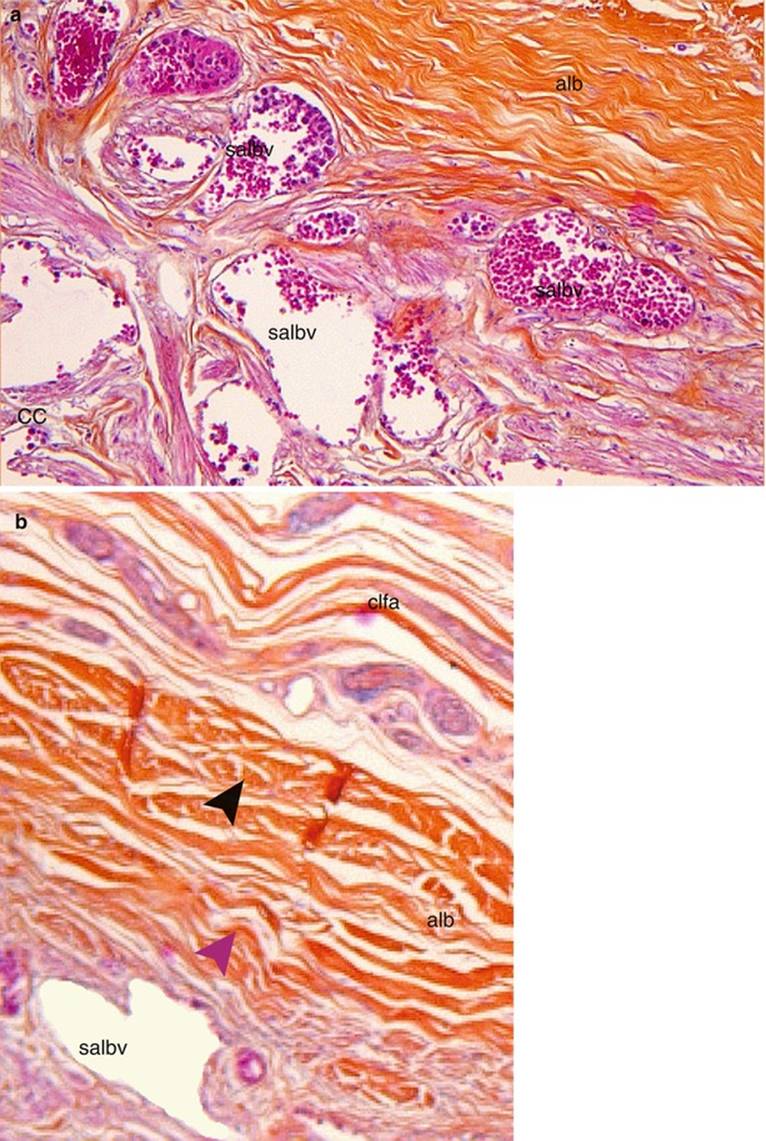
Fig. 6.4
Microscopic anatomy of the clitoral tunica albuginea. (a) Low magnification (x50) showing the layer of sub-albugineal veins (when these veins will be compressed by the dilated sinuses expanding against the tunica albuginea, the evacuation of the blood emptying the corpora cavernosa will stop, making the clitoris rigid). (b) High magnification (x100), showing the two layers of collagen fibres in the tunica albuginea: black arrowhead locating the longitudinal bundles of the outer layer and mauve arrowhead locating the circulary oriented fibres of the inner layer. alb tunica albuginea, clfa clitoral fascia, CC erectile tissue of corpora cavernosa, salbv sub-albugineal veins
At the body of the clitoris, the corpora cavernosa are surrounded by a single thick peripheral envelope of connective tissue, the albuginea of the clitoral body’s corpus cavernosum. A fibrous sagittal partition, resulting from the median junction area of the crura’s corpora cavernosa (the clitoral septum or median septum) originates from this albuginea.
The existence of the albuginea is essential because it conditions the phenomena of intumescence and rigidity by providing resistance to the sudden filling of the clitoral vascular labyrinth. Studied by numerous authors, the clitoral albuginea is now better known. The measurements we took on sections perpendicular to the clitoral axis (in the middle part of the descending portion of the body) demonstrate an average thickness of 300 μm. Several characteristics are now known:
· The albuginea is not a rigid, nondeformable structure: Its thickness increases and decreases during clitoral tumescence (even if these variations are very limited). However, the albuginea cannot expand beyond a certain increase in its dimensions. It therefore opposes the pressure of blood flow and the increase of the sinus diameter, thus limiting tumescence, i.e. the swelling of the clitoral body.
· The albuginea includes two layers (Fig. 6.4), like that of the penis corpora cavernosa: an external layer of longitudinal collagenous fibre bundles and an internal layer of circularly oriented bundles. However, only the internal circular layer is clearly visible on the clitoris. The external longitudinal bundles are sometimes sparse in the external most part of the circular layer or even absent in certain quadrants. This is perfectly understandable given that the elongation of the clitoris remains very moderate and certainly does not have the same purpose as penile elongation for coitus.
· The collagen bundles of the albuginea are made up of fibres that are indeed inextensible, but they are pleated, wavy and therefore have a capacity for elongation. The significant size of the circular layer of this albuginea therefore demonstrates the relative expansion of the clitoral diameter in the sexual arousal phase. It is the smoothing of the waves in the collagenous fibres that enables this expansion; the albuginea also thins at the same time. During detumescence and return to flaccidity, the wavy morphology of the collagenous fibres is acquired once again (resting morphology) due to elastic fibres along with the collagen bundles.
· The fibrous columns of the sinus trabeculae originate from the deep surface of the albuginea. A.M.B. Goldstein et al. are to be credited for having demonstrated that a sort of fibrous frame exists within the cavernous tissue, creating a true “fibrous skeleton” of the corpora cavernosa and preventing them from rupturing. The columns of this frame elongate during tumescence, enabling an increase in the diameter of the sinus lumina. The fibrous frame also surrounds the vessels and nerves (Fig. 10.1), which are then completely protected in true fibrous tunnels when the intra-cavernous pressure becomes very high and erection occurs.
· The tunica albuginea makes a complete crown around the corpora cavernosa but it continues above the clitoral body, with collagenous bundles of the suspensory ligament (“noon” position on the crown) and below the body with the collagenous bundles of the intermediate part (6:00 on the crown). A fibrous partition originates from the albuginea at this last position: the clitoral septum (septum cavernosum of clitoral body) or median septum.
This septum is a thick, sagittal, median partition that is part of the cavernous skeleton (the sinus partitions are attached to it, as well as to the albuginea). Its base has a width close to the thickness of the albuginea. It thins to a point at its anterior end (noon position!). More often than not it forms an incomplete partition such that the two corpora cavernosa meet well above the end or tip. The sinuses of the left and right corpora cavernosa have oblique axes converging at the communication zone which is therefore essential for inter-cavernous drainage. The arteries of the corpora cavernosa are located on either side of the middle part of this median septum and are attached to it by their fibrous sheaths.
Other septa (paramedian or lateral) may exist. They always originate from the albuginea but are thus arranged obliquely and are often very short.
Some variants exist in the microscopic anatomy of the cavernous formations, depending on the levels:
· The size and number of sinus lacunae vary, depending on the cavernous segment considered (Figs. 5.6 and 5.10): These elements vary in an inversely proportional manner. The largest and most sparse sinuses, with equal surface area or volume of cavernous tissue, are located at the crura or ascending portion of the body. The smallest and most abundant sinuses are located at the descending portion where they are very tightly and densely packed. At the crura, the sinus lumina are larger towards the centre than at the periphery.
· The albuginea evidently surrounds the crura and body of the clitoris. However, the albuginea of the crura is thinner and cannot be seen without dissection. Each crus is completely covered by the ischiocavernosus muscle (see the Chap. 11) which truly sheathes it.
· The form of the corpora cavernosa varies depending on the levels considered; more or less cylindrical at the crura and the ascending portion of the body, the corpora cavernosa take on a semilunar shape at the descending part (Fig. 6.1). At this level, the two corpora cavernosa face one another by their medial plane surface, and the former centre parts of the albugineae merge in a median septum, whereas the remaining parts of the two primitive albugineae merge as one single albuginea: the clitoral body albuginea (Fig. 6.1).
It should be recalled that the corpora cavernosa are richly innervated, which will be covered in the “Innervation” chapter (Chap. 8).
6.1.2 Spongy Tissue
While it belongs to the same bulbo-clitoral organ and extensively communicates with the cavernous tissue, the spongy tissue is quite different from the latter. It does not have an erectile property in the true sense of the word (as is true for spongy tissue in men), even if it does contribute to achievement of tumescence and rigidity from a vascular point of view.
Observation of the slides demonstrates these differences immediately:
· The spongy tissue, to be filled with blood upon sexual arousal, like the cavernous tissue, is made up of intercommunicating cavities; but here the cavities or lacunae are of a less aberrant shape, rounded or oval for the most part and of irregular dimensions, but always much bigger than those of the cavernous tissue sinuses (Fig. 6.5). The tissue really does resemble a sponge, hence its name. The trabeculae that separate the lacunae are finer than those in the cavernous tissue, especially when compared to the dimensions of the lacunae themselves. The lumen of the lacunae is bordered by an endothelium that at first appears to be identical to that of the cavernous lacunae but for which the anti-factor VIII antibody immunolabelling is very weak (Fig. 6.6). The functions of these endothelial cells are most definitely different than those of the cavernous endothelium cells (different antithrombotic properties?1).
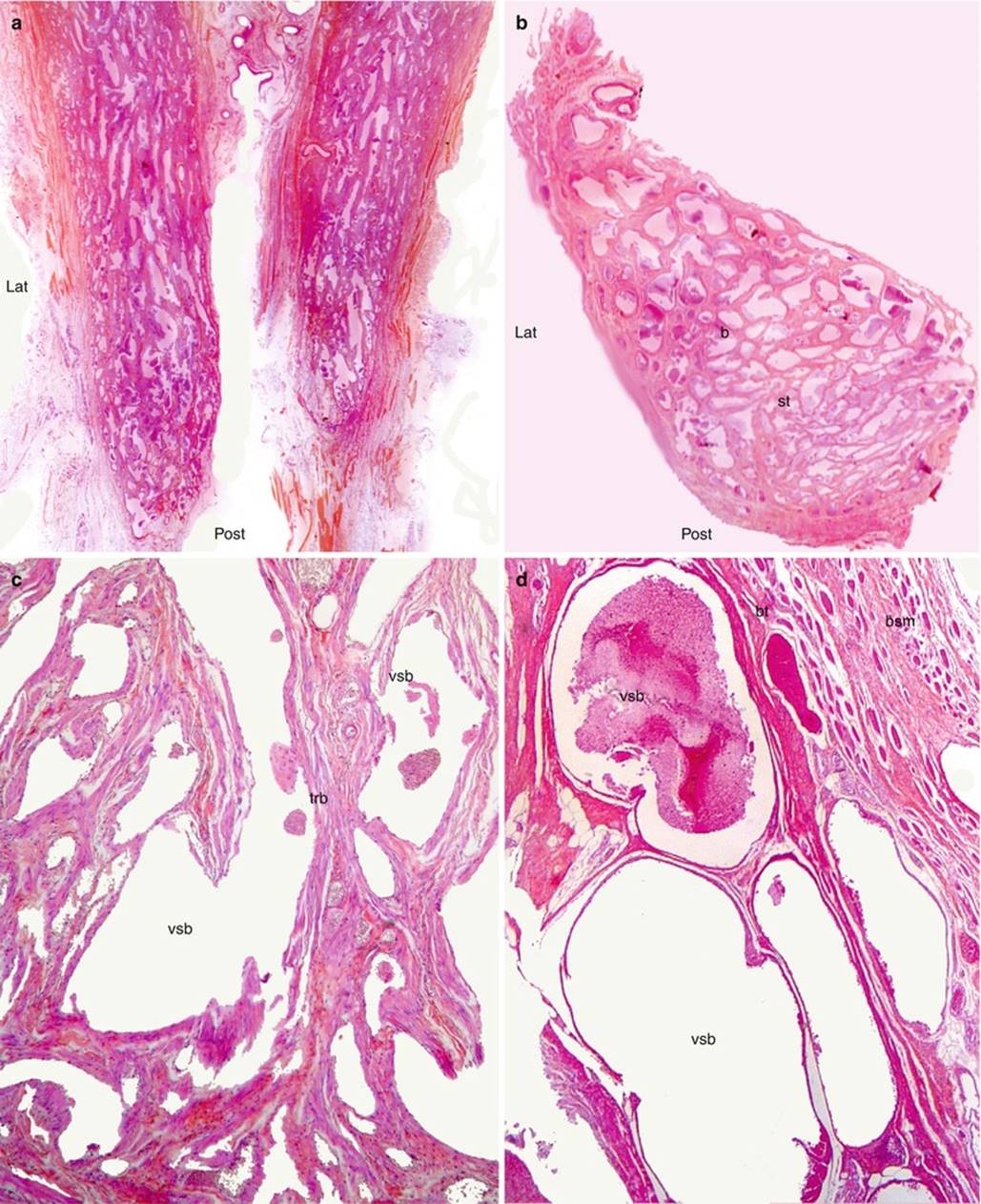
Fig. 6.5
The spongy tissue of the bulbs (bulbo-clitoral organ). (a) Photomicrograph of two bulbs in collapsed state; (b) photomicrograph of an isolated fig-shaped bulb; (c) microscopic view of the spongy tissue (low magnification); (d) microscopic view (strong magnification) showing the rounded vascular spaces. b bulb, bsm bulbo-spongiosus muscle, bt (fibrous) bulb tunica, st spongy tissue, trb trabeculae of the bulb, vsb vascular spaces of the bulb (spongy sinus). Note: The frequent presence of residual blood in the vascular spaces of the bulbs
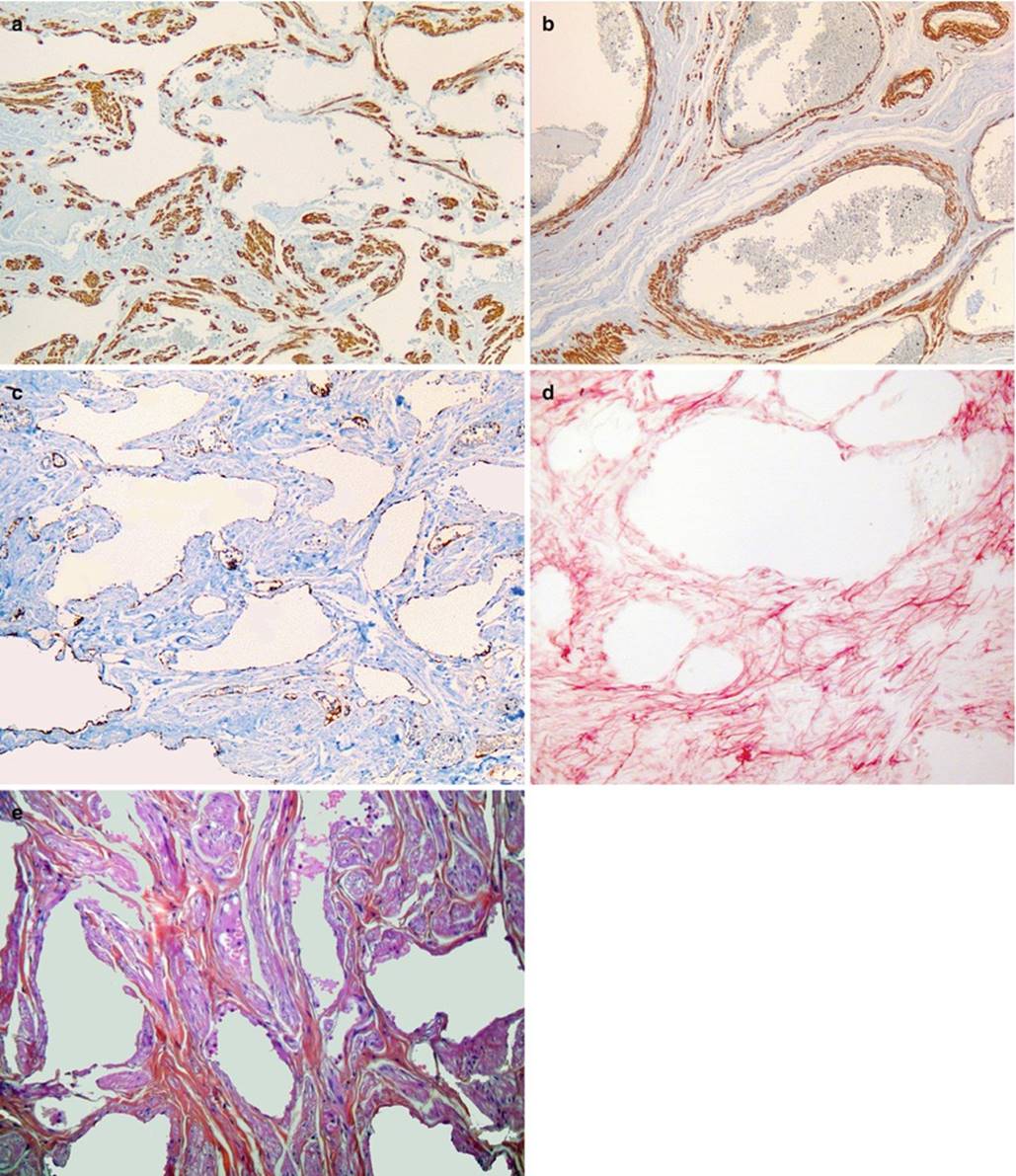
Fig. 6.6
Microarchitecture of the bulbo-clitoral organ’s corpus spongiosum (histochemical study by specific staining of the bulb’s sections). (a, b) Immuno histochemical staining by alpha-smooth actin: highlighting the bundles of smooth muscular fibers (wine-coloured). (c) Immuno histochemical staining by Factor VIII: highlighting the endothelial cells. (d) Staining by orcein: highlighting the elastic fibers. (e) Classical histological staining (HEAS). (a, b): The smooth muscular fibers are abundant into the spongy stroma (a), and around the vessels (b). (c) The impregnation of the spongious tissue’s endothelial cells is poor. (d) The red elastic fibers draw a sort of reticulum around the rounded spongy cavities. (e) The collagen fibers and the fibroblasts have an orange colour. The smooth muscular fibers have a purple colour and their elongated nuclei are dark blue
· Observation under greater magnification shows that the intermediate connective tissue is less abundant than in the corpora cavernosa. Here it is also made up of wavy, collagenous fibre bundles, demonstrating potential capacity for elongation. In the spongy tissue, near the collagenous fibres, we can see smooth muscle fibres which also go to prove the possibility of filling or emptying the lacunae by action on the trabecula collagenous fibres. Specific staining of the elastic fibres using orcein shows, however, that the spongy tissue is richer in elastic fibres than the cavernous tissue (A. W.M. Van Turnhout); once again recalling the comparison to the sponge which returns to its initial shape after being pressed to empty it of the liquid absorbed.
· The peripheral fibrous layer that surrounds the spongy tissue is much thinner than the albuginea of the corpora cavernosa, such that we cannot really call it a spongy albuginea but rather a fibrous peripheral envelope or tunic. However, a fibrous architecture exists which is similar to that of the cavernous frame, and the lacunae trabeculae are in continuity with the fibrous peripheral envelope. The thickness of this envelope exceeds that of the trabeculae by very little.
· If we consider the large size of the spongy lacunae, the relative thinness of the trabeculae separating these mega-lacunae and the fineness of the peripheral envelope of the bulbs, it is understood that the spongy tissue, especially at the bulbs (where it is particularly exposed) is very fragile. This explains the large perineal haematomas that may occur during labour when the foetus is expelled or the development of centro-bulbar haemorrhagic cysts (see Fig. 5.18).
The spongy tissue presents specific traits depending on its topography:
· At each of the two bulbs, the fibrous peripheral envelope is covered on its outer surface by bundles of striated muscles of the homolateral bulbospongiosus muscle (Figs. 6.7 and 11.4) (see the Chap. 11). To visualise the fibrous envelope, the muscle must be resected. We can then see the blue-grey appearance of this envelope, semitransparent due to its thinness. Upon sectioning, the bulbar lacunae demonstrate a variable general direction: parallel to the longitudinal axis of the bulb (obliqueness in front and inside) for elongated bulbs with a leech-like appearance. The direction is perpendicular to the longitudinal axis for bulbs in the form of small pouches (Fig. 6.5). It should also be noted that the vascular lacunae with the largest diameters are observed at the large posterior end of the bulbs.
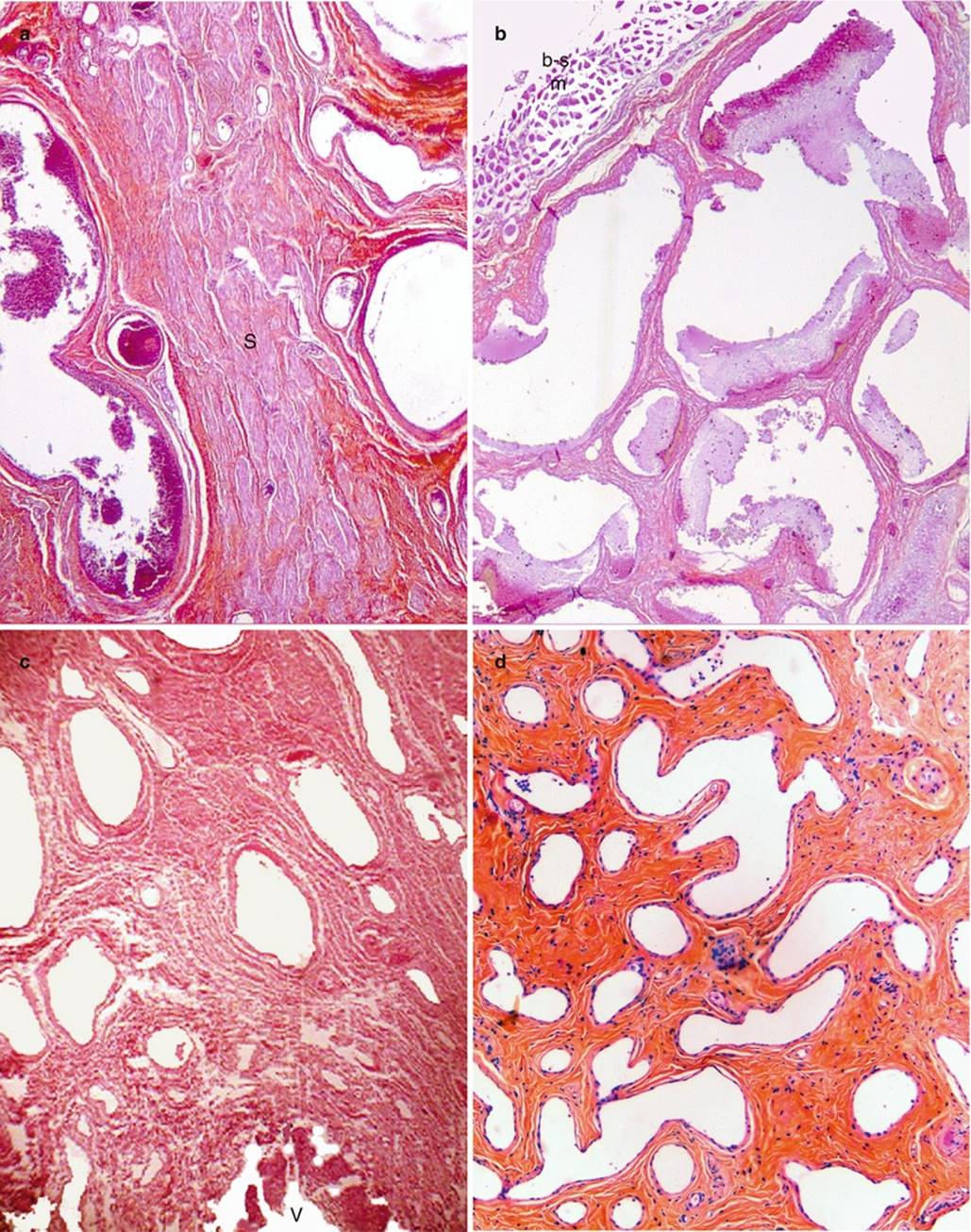
Fig. 6.7
The four different aspects of spongy tissue according to its location. (a) Spongy tissue of the pars intermedia; double row of closely set venous canals separated by a large septum (S) rich in smooth muscle fibres (purple coloured). (b) Spongy tissue of the bulbs, large rounded or polyhedric vascular spaces containing many red cells; striated muscle fibres are those of the bulbospongiosus muscle (b-s m). (c) Spongy tissue of the residual spongy part (rsp), above the vestibular roof (V). (d) Spongy tissue of the glans clitoridis (lower half)
· At the commissure of the bulbs (commissura bulborum) (Fig. 5.17), the lacunae have a tendency to become horizontal and follow the general arc form of a supra-urethral circle. In addition, these lacunae are transversally very flat and elongated. The lacunae of the two bulbs extend into these commissural lacunae and the septum of the overlying pars intermedia does not always descend to the bulbar commissure (see Fig. 5.13). The fibrous envelope now only exists on the posterior surface (supra-urethral concavity) of the bulbar commissure. The anterior surface (back) of the commissure continues with the vascular lacunae of the pars intermedia.
· At the pars intermedia, the vessels are sinuous with a large parallel axis in a comb-tooth pattern. Upon sectioning, they appear as lacunae with a greater diameter than the bulbar lacunae, arranged one on top of the other in a “stack of plates” (see Figs. 6.7 and 5.17). They often have a tendency to form two vertical columns, left and right, parallel to the median septum that separates them. This septum of the intermediate part is a thick, fibrous septum located in line with the median septum of the clitoral body which it follows, becoming progressively enlarged (Fig. 5.17). This septum is usually interrupted at the commissure of the bulbs. The pars intermedia lacunae communicate with the sinusoids of the posterior part of the elbow and of the clitoral body, and we can even see the spongy lacunae going through the albuginea, erupting into the homolateral cavernous tissue (Fig. 6.8)! The vascular rows of the pars intermedia are well protected because they are located within the thick network of collagenous fibres in connection with the overlying clitoral albuginea.
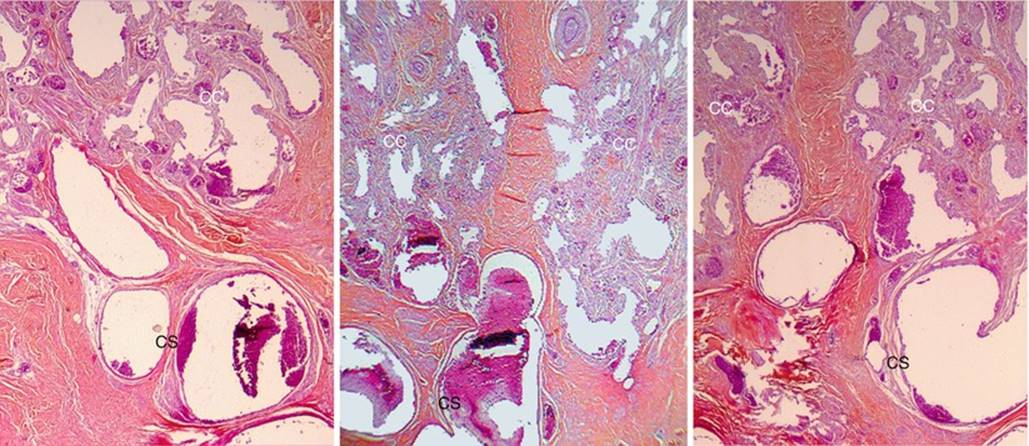
Fig. 6.8
Three examples of interpenetration of spongy and cavernous tissues. CC corpus cavernosum, CS corpus spongiosum
· The infra-clitoral residual spongy part (icrsp) extends from the commissure of the bulbs, as shown previously, and is positioned below the descending part of the clitoral body. Obscured or even refuted by some authors, the “icrsp” is on the contrary, a significant part of the spongy tissue of the bulbo-clitoral organ in which we can observe the presence of large vascular lacunae with large vertical axes. The diameters of these lacunae tend to decrease as we approach the glans. This icrsp is connected to the clitoral body by the pars intermedia previously studied. Below the icrsp, the spongy lacunae are divided into two contingents, right and left, which reach the lateral walls of the vestibule to anastomose with the veins present in these walls (Figs. 6.7 and 5.15). The visible turgescence of these veins during sexual arousal can be explained by the fact that these vestibular veins are in continuity with those of the labia minora (turgescence transmitted by blood engorgement of the erectile bodies).
· As we saw previously, the spongy tissue continues from the icrsp up to the free part of the glans. But this spongy tissue becomes very involutive as it approaches the glans (spongy tissue in which a terminal urethra did not form, as it does in the male glans penis), such that at the glans (especially in the “lower half”, we only find scattered, rounded vascular lacunae of varying diameters, arranged more towards the centre than at the periphery, within interlacunar connective tissue that is more abundant and more dense (slightly wavy, collagenous fibres, arranged with a nice microscopic architecture (Fig. 5.20)). In this stroma, we also find elastic fibres and some smooth muscle fibres. In the “upper half” of the glans, the presence of Forster’s ligament and its tree structure causes the spongy residues to be dispersed within the connective frame thus constructed (Fig. 5.12).
Footnotes
1
1Note that on histological sections, the spongy lacunae are always filled with erythrocytes (Fig. 6.7)!