This chapter deals primarily with APGO Educational Topic Area:
TOPIC 35 VULVAR AND VAGINAL DISEASE
Students should be able to outline a basic approach to evaluation and management of vulvar and vaginal complaints, including defining the role of the wet mount preparation.
Clinical Case
A 20-year-old virginal woman presents to the office with a 2-day history of thick white discharge, redness of her “bottom,” and intense vaginal itching. She had a course of oral antibiotics the prior week for sinusitis. She denies ever having anything like this in the past. Her symptoms are confirmed on physical examination.
Vulvovaginitis is the spectrum of conditions that cause vaginal or vulvar symptoms such as itching, burning, irritation, and abnormal discharge. Vaginal and vulvar symptoms are among the most common reasons for patient visits to obstetrician–gynecologists. Symptoms may be acute, subacute, or chronic and may range in intensity from mild to severe. Vulvovaginitis may have important consequences in terms of discomfort and pain, days lost from school or work, sexual functioning, and self-image. Depending on the etiology, vulvovaginitis may also be associated with adverse reproductive outcomes in pregnant and nonpregnant women.
![]() VULVOVAGINITIS
VULVOVAGINITIS
Vulvovaginitis has a broad differential diagnosis, and successful treatment typically depends on accurately identifying its cause. The most common causes of vaginitis are bacterial vaginosis ([BV] 22%–50% of symptomatic women), vulvovaginal candidiasis (17%–39%), and trichomoniasis (4%–35%). These common vaginal infections often present with characteristic patterns (Table 28.1). The vulva and vagina are also sites of symptoms and lesions of several sexually transmitted infections, such as herpes genitalis, human papillomavirus, syphilis, chancroid, granuloma inguinale, lymphogranuloma venereum, and molluscum contagiosum (see Chapter 29). It is estimated that up to 70% of women with vaginitis remain undiagnosed. In this undiagnosed group, symptoms may be caused by a broad array of conditions, including atrophic vaginitis, various vulvar dermatologic conditions, and vulvodynia.
Although sexually transmitted and other infections are common etiologies of vulvovaginitis, the patient’s history and symptoms may point to chemical, allergic, or other noninfectious causes. Evaluation of women with vulvovaginitis should include a focused history about the entire spectrum of vaginal symptoms, including change in discharge, vaginal malodor, itching, irritation, burning, swelling, dyspareunia, and dysuria. Questions about the location of symptoms (vulva, vagina, and anus), duration, the relation to the menstrual cycle, the response to prior treatment including self-treatment and douching, and a sexual history can yield important insights into the likely etiology. In patients with vulvar symptoms, the physical examination should begin with a thorough evaluation of the vulva; however, evaluation may be compromised by patient self-treatment with nonprescription medications.
Easily performed office tests available to aid in diagnosing the cause of vulvovaginitis include vaginal pH testing, the amine (“whiff”) test, as well as microscopic examination of discharge mixed in normal saline or 10% potassium hydroxide (KOH). Laboratory tests such as rapid tests for enzyme activity from BV-associated organisms, Trichomonas vaginalis antigen, and point-of-care testing for DNA of Gardnerella vaginalis, T. vaginalis, and Candidaspecies are also available, although the role of these tests in the proper management of patients with vulvovaginitis is unclear. Depending on the risk factors, DNA amplification tests can be obtained for Neisseria gonorrhoeae and Chlamydia trachomatis.
![]() NORMAL VULVOVAGINAL ECOSYSTEM
NORMAL VULVOVAGINAL ECOSYSTEM
The vulva and vagina are covered by stratified squamous epithelium. The vulva contains hair follicles and sebaceous, sweat, and apocrine glands, whereas the epithelium of the vagina is nonkeratinized and lacks these specialized elements. At puberty, with maturation of the epithelial cells that occurs with estrogen stimulation, increased levels of glycogen in the vaginal tissues favor the growth of lactobacilli in the genital tract. These bacteria break down glycogen to lactic acid, lowering the pH from the 6 to 8 range, which is common before puberty and after menopause, to the normal vaginal pH range of 3.5 to 4.7 in the reproductive-aged woman. In addition to lactobacilli, a wide range of other aerobic and anaerobic bacteria are normally found in the vagina at concentrations of 108 to 109 colonies per mL of vaginal fluid. Because the vagina is a potential space, not an open tube, a ratio of 5:1 anaerobic to aerobic bacteria is normal.

Discharge from the vagina is normal; therefore, not all discharges from the vagina indicate infection. This distinction is important to the diagnostic process. Vaginal secretions arise from several sources. The majority of the liquid portion consists of mucus from the cervix. A small amount of moisture is contributed by endometrial fluid; exudates from accessory glands, such as the Skene and Bartholin glands; and from vaginal transudate. Exfoliated squamous cells from the vaginal wall give the secretions a white to off-white color and provide some increase in consistency. The action of the indigenous vaginal flora also can contribute to the secretion. These components form vaginal secretions that provide a physiologic moisture, which prevents symptoms of dryness and irritation. The amount and character of this normal wetness may vary under the influence of factors such as hormonal and fluid status, pregnancy, immunosuppression, douching, and coital activity. Asymptomatic women produce approximately 1.5 g of odorless vaginal fluid each day.
![]() BACTERIAL VAGINOSIS
BACTERIAL VAGINOSIS
BV is a polymicrobial infection characterized by a lack of normal hydrogen peroxide–producing lactobacilli and an overgrowth of facultative anaerobic organisms including G. vaginalis, Mycoplasma hominis, Bacteroides species, Peptostreptococcus species, Fusobacterium species, Prevotella species, and Atopobium vaginae.
Women with BV generally complain of a “musty” or “fishy” odor with an increased thin gray-white to yellow discharge. The discharge may cause mild vulvar irritation in approximately 25% of the cases. The vaginal discharge is mildly adherent to the vaginal wall and has a pH greater than 4.5. Adding a few drops of KOH to the vaginal discharge produces an “amine” or “fishy” odor, commonly referred to as a “positive whiff test.”
Microscopic examination made under saline wet mount shows a slight increase in white blood cells (WBCs), clumps of bacteria, loss of normal lactobacilli, and characteristic “clue cells” (Fig. 28.1). These are epithelial cells with numerous coccoid bacteria attached to their surface, which makes their borders appear indistinct and their cytoplasm resemble “ground glass.” Because the bacteria that cause BV are part of the normal vaginal flora, the mere presence of these organisms is not diagnostic. The “gold standard” for laboratory diagnosis of BV is the Gram stain, but, more commonly, the diagnosis is made clinically and is defined by any three of the following four criteria: 1) abnormal gray discharge, 2) pH greater than 4.5, 3) positive whiff test, and 4) the presence of clue cells. Neither Pap smear nor cultures for G. vaginalis is helpful in the diagnosis of BV.

FIGURE 28.1. Clue cells. Clue cells are epithelial cells with clumps of bacteria clustered on their surfaces. Clue cells indicate the presence of a vaginal bacterial infection. CDC/M. Rein.
Treatment
BV may be treated with oral or topical metronidazole as well as topical clindamycin. Treatment with oral tinidazole, oral clindamycin, or clindamycin intravaginal ovules are effective alternatives. Symptomatic pregnant women can be treated with either metronidazole or clindamycin, insofar as neither drug has been shown to have teratogenic effects. There are data suggesting that treatment of BV in women with high-risk pregnancies may reduce the incidence of premature rupture of membranes (PROM) and preterm delivery; however, there is no apparent benefit to either universal BV screening or treatment of asymptomatic pregnant women. In nonpregnant women, BV has been associated with both pelvic inflammatory disease (PID) and postoperative infections. It has also been associated with an increased risk of acquisition of human immunodeficiency virus (HIV) and herpes simplex virus (HSV). Although preoperative BV treatment may help prevent postoperative infections, treatment for BV has not been shown to decrease the risk of the HIV or HSV infection. Treatment of partners of patients with BV does not help prevent recurrence.
![]() VULVOVAGINAL CANDIDIASIS
VULVOVAGINAL CANDIDIASIS
Vulvovaginal candidiasis is caused by ubiquitous airborne fungi. Approximately 90% of these infections are caused by Candida albicans (Fig. 28.2). The remaining cases are caused by Candida glabrata, Candida tropicalis, or Torulopsis glabrata. Candida infections generally do not coexist with other infections and are not considered to be sexually transmitted, although 10% of male partners have concomitant penile infections. Candidiasis is more likely to occur in women who are pregnant, diabetic, obese, immunosuppressed, on oral contraceptives or corticosteroids, or have had broad-spectrum antibiotic therapy. Practices that keep the vaginal area warm and moist, such as wearing tight clothing or the habitual use of panty liners, may also increase the risk of Candida infections. Because Candida species typically require estrogenized tissue, vulvovaginal candidiasis is more common during reproductive years and less so before men arche or after menopause.

FIGURE 28.2. Candida albicans. Branching hyphae are present among epithelial cells in this Gram stain of a vaginal smear. CDC/ Dr. Stuart Brown.
Signs and Symptoms
The most common presenting complaint for women with candidiasis is itching, although up to 20% of women may be asymptomatic. Burning, external dysuria, and dyspareunia are also common. The vulva and vaginal tissues are often bright red in color, and excoriation is not uncommon in severe cases. A thick, odorless, adherent “cottage cheese” discharge with a pH of 4 to 5 is generally found.
Diagnosis
A reliable diagnosis cannot be made on the basis of history and physical examination alone. Over-the-counter (OTC) treatments are safe and effective, but any woman who does not respond to OTC treatment or who has a recurrence soon after treatment should be seen by a physician for a definitive diagnosis. Patients who have self-administered OTC medications should be advised to stop treatment 3 days before their office visit. Diagnosis requires either visualization of blastospores or pseudohyphae on saline or 10% KOH microscopy or a positive culture in a symptomatic woman. The diagnosis can be further classified as uncomplicated or complicated vulvovaginal candidiasis (Box 28.1). Latex agglutination tests may be of particular use for non–C. albicans strains, because they do not demonstrate the pseudohyphae on wet prep.
BOX 28.1 Classification of Vulvovaginal Candidiasis
Uncomplicated
Sporadic or infrequent episodes OR
Mild to moderate symptoms or findings OR
Likely instead of suspected Candida albicans infection OR
Nonimmunocompromised women
Complicated
Recurrent episodes (four or more per year) OR
Severe symptoms or findings OR
Suspected or proven non–C. albicans infection OR
Women with diabetes, severe medical illness, or immunosuppression
Modified from Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, 2010. MMWR Recomm Rep. 2002;51(RR-6):1–78.
Treatment
Treatment of Candida infections is primarily with the vaginal application of one of the synthetic imidazoles, such as miconazole, clotrimazole, butoconazole, tioconazole, and terconazole in cream or suppository form. Single-dose oral therapy with fluconazole 150 mg has become widely used. This same low dose is safe for pregnant women despite findings that there is an increased risk of birth defects associated with high daily doses (400–800 mg) of fluconazole. The antifungal nystatin is also used in pregnant women.
Although these agents are associated with high cure rates, approximately 20% to 30% of patients experience recurrences 1 month after treatment. Weekly therapy with oral fluconazole for 6 months has been shown to be effective in preventing recurrent candidiasis in 50% of women. Weekly or twice weekly topical therapy can also be used for prevention. T. glabrata is resistant to all azoles and may respond to therapy with intravaginal boric acid capsules or gentian violet. Patients with frequent recurrences should be carefully evaluated for possible risk factors such as diabetes and autoimmune disease. Prophylactic local therapy with an antifungal agent should be considered when systemic antibiotics are prescribed. Because it is not considered a sexually transmitted disease (STD), the Centers for Disease Control does not recommend routine treatment of sexual partners.
![]() TRICHOMONAL VULVOVAGINITIS
TRICHOMONAL VULVOVAGINITIS
T. vaginalis is a flagellate protozoan that lives only in the vagina, Skene ducts, and male or female urethra. The infection can be transmitted by sexual contact, but can also occur via fomites, and the organism has been known to survive in swimming pools and hot tubs. Trichomoniasis is associated with PID, endometritis, infertility, ectopic pregnancy, and preterm birth. It often coexists with other STDs as well as BV and has also been shown to facilitate HIV transmission.
Symptoms
Symptoms of Trichomonas infection vary from mild to severe and may include vulvar itching or burning, copious discharge with rancid odor, dysuria, and dyspareunia. Although not present in all women, the discharge associated with Trichomonas infections is generally “frothy,” thin, and yellow-green to gray in color, with a pH above 4.5. Examination may reveal edema or erythema of the vulva. Petechiae, or strawberry patches, are classically described as present in the upper vagina or on the cervix but are actually found in only about 10% of affected patients. A significant number of women with trichomoniasis are asymptomatic.
Diagnosis
The diagnosis is confirmed by microscopic examination of vaginal secretions suspended in normal saline. This wet smear will show large numbers of mature epithelial cells, WBCs, and the Trichomonasorganism (Fig. 28.3). Point-of-care tests include the OSOM Trichomonas Rapid Test, which uses an immunochromatographic capillary flow dipstick technology, and the Affirm VP III, a nucleic acid probe test that can identify T. vaginalis, G. vaginalis, and C. albicans. Other options include culture and amplification testing such as polymerase chain reaction testing. Women diagnosed with trichomoniasis should also undergo screening for other STDs, especially gon-orrhea and chlamydia.
Treatment
Treatment of Trichomonas infections is with oral metronidazole or tinidazole. Treating sexual partners of women with trichomoniasis is recommended. An individual undergoing treatment should avoid intercourse until she and her partner have completed the prescribed medication and are asymptomatic. Abstinence from alcohol use when taking metronidazole is necessary to avoid a possible disulfiram-like reaction. Trichomoniasis has been associated with preterm delivery, PROM, and low birth weight. Pregnant patients should be treated, and metronidazole is considered safe for use during pregnancy; however, treatment may not prevent these pregnancy complications.
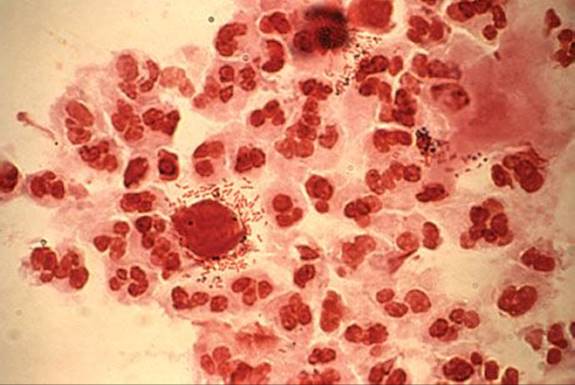
FIGURE 28.3. Trichomonads. The flagella of this parasite can be clearly seen in this image. CDC.
Although follow-up examination of patients with trichomoniasis for test of cure is often advocated, it is usually not cost effective, except in the rare patient with a history of frequent recurrences. In these patients, reinfection or poor compliance must be considered as well as the possibility of infection with more than one agent or other underlying disease. Infections with metronidazole-resistant T. vaginalishave been reported. Although absolute resistance is rare, relative resistance may be as high as 5%. These infections are treated with high doses of tinidazole.
![]() OTHER CAUSES
OTHER CAUSES
Atrophic Vaginitis
Atrophic vaginitis is defined as atrophy of the vaginal epithelium due to diminished estrogen levels. Although more common in postmenopausal women, atrophic vaginitis can be observed in younger premenopausal women. Estrogen status plays a crucial role in determining the normal state of the vagina. When estrogen levels decrease, there is loss of cellular glycogen with resulting loss of lactic acid. In the prepubertal and postmenopausal states, the vaginal epithelium is thinned, and the pH of the vagina is usually elevated (4.7 or greater). Loss of elasticity in the connective tissue may also occur, resulting in shortening and narrowing of the vagina. The urinary tract may also be affected and may demonstrate atrophic changes. Patients with atrophic vaginitis may have an abnormal (decreased) vaginal discharge, dryness, itching, burning, or dyspareunia. Typical urinary symptoms include urgency, frequency, recurrent urinary tract infections, and incontinence. Atrophic vaginitis is treated with local water-based moisturizing preparations or topical or oral estrogen therapy.
Desquamative inflammatory vaginitis is generally seen in perimenopausal and postmenopausal women and is characterized by purulent discharge, exfoliation of epithelial cells with vulvovaginal burning and erythema, relatively little lactobacilli, and overgrowth of Gram-positive cocci; usually streptococci are seen. Vaginal pH is greater than 4.5. Initial therapy is clindamycin cream 2%, applied daily for 14 days.
Clinical Follow-Up
The patient’s presentation strongly suggests candidal vulvovaginitis. The course of broad-spectrum antibiotics is a likely predisposing factor. The potassium hydroxide prep confirms the diagnosis, and the normal saline prep is negative for bacterial vaginosis and trichomoniasis. A culture is not necessary in relatively straightforward cases, as this one appears to be, and surveillance for sexually transmitted disease is not needed because she denies sexual activity. A single dose of oral fluconazole successfully treats this patient’s symptoms.
the Point Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!