Douglas C. Tkachuk MD, FRCPC
Kathy Chun PhD, FCCMG
Jan V. Hirschmann MD
The myelodysplastic syndromes (MDSs) are disorders caused by a clonal expansion of hematopoietic stem cells in which maturation is abnormal (dysplastic) and production ineffective, resulting in many cells being destroyed before they reach the systemic circulation. Anemia typically occurs, often accompanied by thrombocytopenia and/or neutropenia. Some cases develop from exposure to ionizing radiation or cytotoxic chemotherapy, usually with alkylating agents, and in these circumstances the bone marrow is characteristically hypocellular and partially fibrotic. More frequently, these diseases occur as a primary problem in older adults, with a median age of about 70 when diagnosed. In them, the bone marrow is usually hypercellular.
Blasts may be increased in the myelodysplastic syndromes, but they do not exceed 20% of the differential count of at least 200 leukocytes in the peripheral blood and 500 in the bone marrow. Dysplasia may involve one or more hematopoietic lines; to be significant it should affect at least 10% of that line's cells in the bone marrow, but evidence for dysplasia may also be present on the peripheral smear. In erythrocytes the smear may show macrocytosis, anisocytosis, basophilic stippling, and Pappenheimer bodies. Poikilocytosis is usual and includes target cells, acanthocytes, elliptocytes, stomatocytes, red-cell fragments, and teardrop cells. Bone marrow findings in the erythrocyte precursors comprise nuclear and cytoplasmic abnormalities. The former consist of budding, internuclear bridging, the presence of more than one nucleus per cell, karyorrhexis (fragmentation), abnormal chromatin (either fine or dense) and megaloblastic changes, in which the nucleus is enlarged and less mature than is the cytoplasm. Cytoplasmic abnormalities include vacuolization and ringed sideroblasts, which are erythroblasts that, on iron stain, contain ≥10 ferritin granules encircling at least one-third of the nucleus.
Evidence of abnormal granulopoiesis on peripheral smear includes neutropenia, hypersegmented neutrophils, Döhle bodies, decreased or absent cytoplasmic granules, and the presence of immature cells, including blasts. The nuclei may have dense chromatin clumping, and many are hypolobulated, with a single lobe or two joined by a thin band of chromatin, resembling the congenital disorder, Pelger-Hüet anomaly. The presence of these pseudo-Pelger-Hüet cells on a blood smear strongly suggests an underlying myelodysplastic syndrome. Eosinophils and basophils may have diminished granules and decreased nuclear lobulation. These abnormalities also are apparent in the bone marrow, along with the small size of the granulocyte precursors, which may be present centrally rather than in their accustomed paratrabecular location, a finding labeled atypical localization of immature precursors (ALIP) when at least three of such foci occur in a bone marrow section.
Abnormal thrombopoiesis on peripheral smear is manifested by thrombocytopenia, giant platelets, and those with decreased or absent granules. In bone marrow specimens, dysplastic megakaryocytes are small (micromegakaryocytes), and possess abnormal nuclei that are multiple and widely separated or have decreased or absent lobulation.
Cytogenetic abnormalities are common in the myelodysplastic syndromes and all types are at varying risk for developing acute leukemia, which is almost always myelogenous. The World Health Organization (WHO) has defined eight types of myelodysplasia based primarily on bone marrow findings (Table 3.1).
Refractory Anemia (RA)
This entity accounts for about 5% to 10% of cases of MDS, the median survival is about 5 years, and acute leukemia eventuates in approximately 5% of patients. Dysplasia occurs in the erythroid precursors alone, ranges from mild to pronounced, and consists of the findings described in the first section. On peripheral blood smear the red cells are normocytic or macrocytic. Nonspecific cytogenetic abnormalities occur in about 25% of cases.
Refractory Anemia with Ringed Sideroblasts (RARS)
This disorder is responsible for about 10% of cases of MDS, has a median survival of about 6 years, and has about a 1% chance of evolving into acute leukemia. Dysplasia occurs only in the erythroid line, and at least 15% of the red cell precursors are ringed sideroblasts. Cytogenetic abnormalities occur in <10% of cases.
Refractory Cytopenia with Multilineage Dysplasia (RCMD)
This disorder accounts for about 25% of MDS, and the diagnosis requires cytopenias and dysplastic changes in at least two lines. When, in addition, ringed sideroblasts constitute >15% of the erythroid precursors, the diagnosis is the subtype refractory cytopenia with multilineage dysplasia and ringed sideroblasts(RCMD-RS), which accounts for about 15% of cases of MDS. The median survival for both is about 3 years, and the risk of leukemia is approximately 10%. Cytogenetic abnormalities occur in up to 50% of cases.
Refractory Anemia with Excess Blasts (RAEB)
In this MDS, the blasts are increased above normal, but not sufficiently to meet the criteria for leukemia, which is at least 20% of nucleated cells in the blood or bone marrow. Two subtypes exist: RAEB-1 has 5% to 9% blasts in the bone marrow and <5% in the blood; RAEB-2 has 10% to 19% blasts in the bone marrow and/or 5% to 19% blasts in the blood. Those with Auer rods are also considered RAEB-2. These two diseases account for approximately 40% of cases of MDS. About 25% of RAEB-1 and 33% of RAEB-2 develop acute leukemia, and their respective median survivals are 18 and 10 months. Approximately 33% to 50% of these patients have cytogenetic abnormalities.
Myelodysplastic Syndrome, Unclassifiable (MDS-U)
Patients are put in this category when they have dysplasia restricted to either the neutrophil or megakaryocytic lines. They fail to meet the criteria for the other MDSs. The number of patients who belong in this group, their median survival, and the risk of developing leukemia are uncertain.
Myelodysplastic Syndrome Associated with Isolated del(5q) Chromosome Abnormality (5q- Syndrome)
Unlike the other MDSs, this entity is primarily defined not by hematologic findings but by a cytogenetic abnormality, a deletion between bands q31 and 33 on chromosome 5, with variability in the actual break points and the size of the deletion. Most patients are middle-aged to older women, whose major problem is refractory macrocytic anemia. Some patients have thrombocytosis. The bone marrow is usually hypercellular, dysplasia is present in the erythroid precursors, many megakaryocytes have hypolobulated nuclei, and blasts are <5%. Patients typically have a long survival, and progression to acute leukemia occurs in <25% of cases.
|
Table 3.1 World Health Organization classification of the myelodysplastic syndromes |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
Table 3.2 Morphologic abnormalities in myelodysplastic syndromes |
|||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||
|
Table 3.3 Predisposing factors and epidemiologic associations |
|||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||
|
|
|
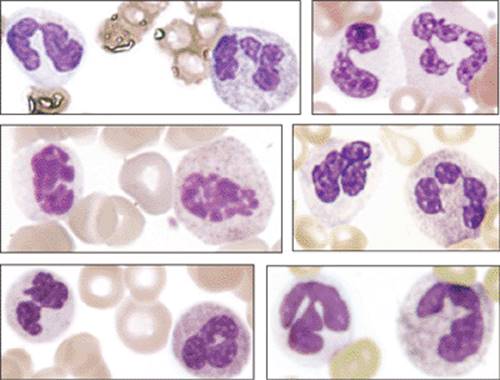
Figure 3.1 Myeloid dysplasia, blood smear. Dysplastic cytoplasmic and nuclear features in neutrophils from four cases of MDS are illustrated here. |
|
|
|
Figure 3.2 Dysplastic hypogranular neutrophils. Several examples of dysplastic, hypogranular neutrophils are shown here. In MDS, dysplastic features are seen usually only in a subpopulation of the affected lineage, whereas staining artifacts usually cause all granulocytes to appear hypogranular in the smear. In the blood smears displayed here, the dysplastic hypogranular neutrophils are all depicted on the left side of each panel. |
|
|
|
Figure 3.3 Dysplastic nuclear features in circulating neutrophils. Hypolobulation, “stringy” chromatin, and pseudo-Barr bodies are included in the spectrum of the abnormal nuclear features seen in MDS. |
|
|
|
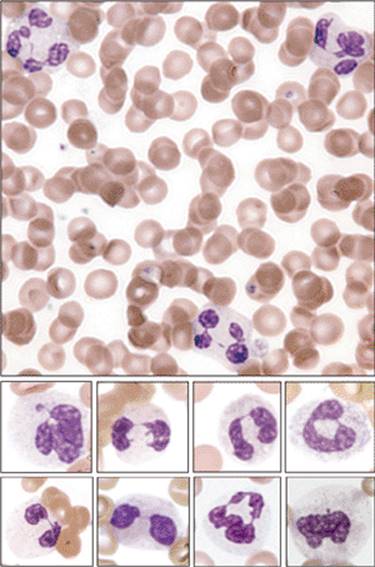
Figure 3.4 Inherited Pelger-Hüet anomaly. Low-power view of peripheral blood showing only hypolobulated neutrophils with very condensed chromatin from a case of inherited Pelger-Hüet anomaly. In myelodysplastic syndromes, hypolobulated neutrophils are usually seen as subpopulations mixed with normal appearing cells. |
|
|
|
Figure 3.5 Dysplastic nuclear features in circulating cells. Composite image taken from several cases of myelodysplastic syndrome showing dysplastic nuclear features seen in circulating granulocytes and nucleated RBCs. The right lower figure shows numerous Pappenheimer bodies. |
|
|
|
Figure 3.6 Dysplastic megakaryocytes. This low-power view of an aspirate smear from a case of MDS shows numerous dysplastic megakaryocytes that include micromegakaryocytes and forms displaying separate nuclear lobulations. Small dysplastic megakaryocytes (micromegakaryocytes) can be difficult to detect during low-power examination of aspirate smears. |
|
|
|
Figure 3.7 Dysplastic megakaryocytes. This low-power view of an aspirate smear from a case of RAEB-1 shows numerous dysplastic megakaryocytes displaying separate nuclear lobulations (arrows). |
|
|
|
Figure 3.8 Normocytic, megaloblastic, and dysplastic features of the erythroid lineage. Composite figure showing several examples of normal (normocytic) versus megaloblastic and dysplastic erythroid precursors at different stages of maturation. Megaloblastic precursors are typically larger in size than normal precursors and exhibit asynchronous nuclear and cytoplasmic maturation. The latter features are best appreciated in more mature forms, where cytoplasmic maturation proceeds in the form of hemoglobin production while nuclear maturation is delayed. Dyserythropoiesis is manifested primarily by nuclear contour abnormalities such as budding, irregularity (“cookie cutter” appearance), and asymmetric multinucleation. |
|
|
|
Figure 3.9 Dysplastic erythroids, iron stain. Low-power view of a Prussian blue–stained aspirate from a case of refractory anemia with ringed sideroblasts. More than 15% of the nucleated erythroid precursors display perinuclear necklaces of iron-laden mitochondria that encircle at least one-third of the circumference of the nucleus (ringed sideroblasts). |
|
|
|
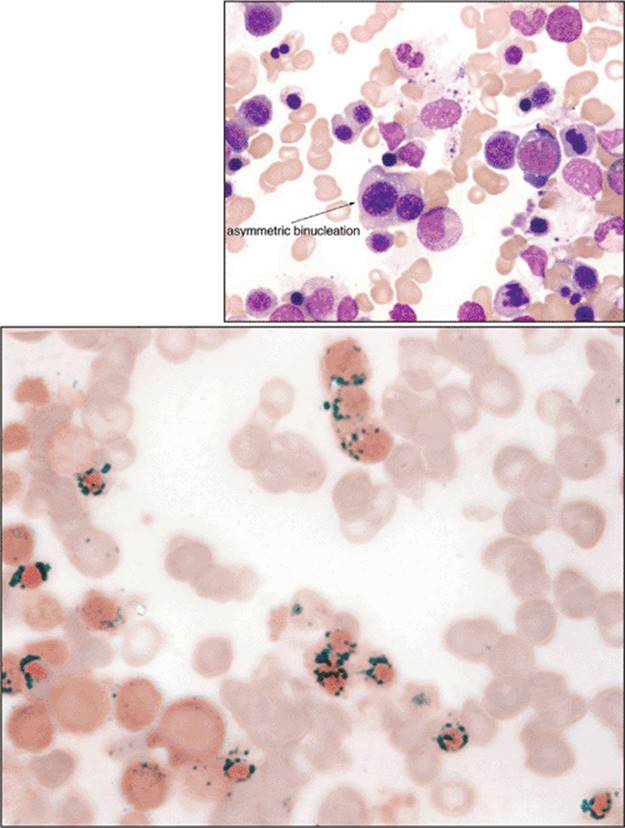
Figure 3.10 Dysplastic erythropoiesis. Hyperplastic megaloblastic dyserythropoiesis in an aspirate smear (top panel). The bottom panel is an iron-stained aspirate smear showing numerous ringed sideroblasts with perinuclear “necklaces” made of siderotic granules. |
|
|
|
Figure 3.11 Dysplastic megakaryocytic (A–E), erythroid (F–J), and myeloid (K–O) precursors in aspirate smears. A. Bizarre megakaryoblasts. B. andC. Unilobular micromegakaryocytes. D. andE. Megakaryocytes with separate nuclear lobulations. F. Dysplastic vacuolated pronormoblast. G. Asymmetric binucleation in mature erythroid. H. Trinucleate mature erythroid. I. Ringed siderocyte (iron stain). J. Mature erythroid with “nuclear budding.” K. Promyelocyte with dysplastic nucleus. L. Hyposegmented neutrophil. M. Hypersegmented neutrophil. N. Hypogranular neutrophil. O. Abnormal eosinobasophilic precursor. |
|
|
|
Figure 3.12 Bone marrow biopsy interpretation in MDS. Hypercellular hematoxylin and eosin (H&E)-stained bone marrow biopsies and CD34 immunostains are shown above and below, respectively, from cases of low- and high-grade MDS. Arrows delineate blasts. Positive-staining endothelial cells serve as built-in controls for CD34 immunostains. |
|
|
|
Figure 3.13 Bone marrow biopsy interpretation in MDS, ALIPS. Maturing granulopoiesis in normal biopsies usually appears as indiscrete, poorly circumscribed foci, centered primarily, but not exclusively, in paratrabecular and perivascular locations. These normal foci of granulopoiesis are made up of a mixture of maturing myeloid precursors with mature forms predominating. In MDS, abnormal localization of immature precursors (ALIPS) occurs, in which small clusters of immature myeloid forms are found away from bony trabeculae and vascular structures (arrows). |
|
|
|
Figure 3.14 Bone marrow biopsy interpretation in MDS. Dysplastic small, unilobular megakaryocytes are readily seen in this case of secondary MDS occurring following unsuccessful treatment for myeloma. The upper panel shows numerous small dysplastic megakarocytes. CD138 immunostains show increased numbers of plasma cells admixed with numerous dysplastic megakaryocytes (lower panel). |
|
|
|
Figure 3.15 Refractory anemia with excess blasts, type 2 (RAEB-2). Aspirate smear from a case of RAEB-2 showing dysplastic small megakaryocytes (micromegakaryocytes), a dysplastic hypogranular/hypolobulated neutrophil, and increased numbers of blasts (open arrows). |
|
|
|
Figure 3.16 5q-syndrome. The top panel is a blood smear showing macrocytic anemia and thrombocythemia. Macrocytic RBCs with cellular diameters that exceed the nucleus of a small mature lymphocyte are seen. Aspirate smear and biopsy in the left and right bottom panels, respectively, show increased numbers of the characteristic unilobular megakaryocytes. The isolated del(5q) cytogenetic abnormality is part of this syndrome or it may be found with or without other cytogenetic abnormalities in other MDS subtypes (see Fig. 3.18). |
|
|
|
Figure 3.17 45,X,–Y. Karyotype with a missing Y chromosome (upper panel). Fluorescent in situ hybridization (FISH) of chromosome X/Y (lower panel). The α-satellite region on the X chromosome is labeled with a green fluor, whereas the α-satellite region on the Y chromosome is labeled with a red fluor. When the Y chromosome is missing, only the green signal is present. |
|
|
|
Figure 3.18 del(5q) cytogenetic abnormality. Upper panel: Ideograms of the normal chromosome 5 with breakpoints shown by arrows and the del(5q) are shown to the left. The corresponding G-banded chromosomes are shown to the right. The bottom panels show the corresponding FISH results. The EGR-I gene at 5q31, labeled with a red fluor, is usually deleted (arrow). The loci at 5p15.2, including D55721 and D5523, are labeled with a green fluor and serve as intrachromosomal controls. |
|
|
|
Figure 3.19 Complex karyotype of an MDS patient. This karyotype from a case of RAEB-2 includes, among other aberrations, a del(5q) and monosomy 7. |