GENERAL PRINCIPLES
Supportive care addresses the physical, mental, and spiritual needs of the cancer patient. Physical symptoms can arise from the cancer itself, the side effects of therapy, medications, or comorbid medical conditions. This chapter focuses on symptom control as an important element of oncology practice, including pain management, nausea and vomiting, mucositis, diarrhea, anorexia, and dyspnea. It also addresses the emotional issues of depression, anxiety, and delirium, and presents an approach to addressing spiritual needs of the cancer patient.
MANAGEMENT BY PHYSICAL SYMPTOM PAIN MANAGEMENT
GENERAL PRINCIPLES
Pain is a prevalent complaint in cancer patients, occurring in 50% to 70% of all patients with cancer. More than one half of cancer patients experience moderate to severe pain, and 50% to 80% of cancer patients are not satisfied with their pain relief. The under treatment of cancer pain can be attributed to multiple barriers, including physician, patient, and societal factors. A physician must remember that each person’s pain is different and must be treated as such.1
Definition
Pain is always subjective. The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Each individual learns the application of the word through experiences related to injury early in life.” Acute pain may be associated with physical signs, including tachycardia, hypertension, hyperventilation, facial grimacing, and verbalizations. However, patients with chronic pain may not exhibit any of these overt physical signs and may not “appear in pain.” It is important to remember that pain is always subjective, and the patient’s self-reporting is a key element to an accurate pain assessment.1
DIAGNOSIS
![]() The first step in the management of pain depends on a comprehensive pain assessment gathered through history, physical exam, and review of laboratory and radiology studies. Important pain characteristics to elicit from the patient should be descriptions of the pain with regard to onset, duration, intensity, quality, and exacerbating or relieving factors. The physician can use each of these characteristics to identify potential etiologies and institute the appropriate pain management plan.
The first step in the management of pain depends on a comprehensive pain assessment gathered through history, physical exam, and review of laboratory and radiology studies. Important pain characteristics to elicit from the patient should be descriptions of the pain with regard to onset, duration, intensity, quality, and exacerbating or relieving factors. The physician can use each of these characteristics to identify potential etiologies and institute the appropriate pain management plan.
![]() Simple tools can reliably aid in the measurement of pain. The most common clinical assessment tools are verbal rating scales and visual analog scales. A verbal rating scale uses words to describe pain such as none, mild, moderate, severe, or excruciating. A visual analog scale uses a line with or without verbal clues or numbers and asks patients to place their pain rating on this scale. The specific scale used to measure pain is less important than the consistent use of a scale over time. For illiterate or pediatric patients, a visual analog scale can be used with pictures to describe the levels of pain as a better pain assessment tool.
Simple tools can reliably aid in the measurement of pain. The most common clinical assessment tools are verbal rating scales and visual analog scales. A verbal rating scale uses words to describe pain such as none, mild, moderate, severe, or excruciating. A visual analog scale uses a line with or without verbal clues or numbers and asks patients to place their pain rating on this scale. The specific scale used to measure pain is less important than the consistent use of a scale over time. For illiterate or pediatric patients, a visual analog scale can be used with pictures to describe the levels of pain as a better pain assessment tool.
TREATMENT1–4
![]() The World Health Organization (WHO) recommends the use of an analgesic ladder in the approach to the selection of opioids to treat cancer pain. Analgesic selection should be guided by the severity of cancer pain. Patients with mild to moderate pain are usually started on acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs). Patients with moderate to severe pain, or those who had insufficient relief after a trial of acetaminophen or NSAIDs, are treated with an opioid used for moderate pain, such as codeine, hydrocodone, dihydrocodeine, and oxycodone. This opioid may be combined with acetaminophen or an NSAID or an alternative adjuvant drug (tricyclic antidepressant, anticonvulsant, or topical anesthetic). Many of the drugs used for moderate to severe cancer pain are available in the United States as a combination of the opioid and acetaminophen or aspirin (ASA). The drug can be titrated until the maximum safe dose of acetaminophen (4 g/d) or ASA is reached.
The World Health Organization (WHO) recommends the use of an analgesic ladder in the approach to the selection of opioids to treat cancer pain. Analgesic selection should be guided by the severity of cancer pain. Patients with mild to moderate pain are usually started on acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs). Patients with moderate to severe pain, or those who had insufficient relief after a trial of acetaminophen or NSAIDs, are treated with an opioid used for moderate pain, such as codeine, hydrocodone, dihydrocodeine, and oxycodone. This opioid may be combined with acetaminophen or an NSAID or an alternative adjuvant drug (tricyclic antidepressant, anticonvulsant, or topical anesthetic). Many of the drugs used for moderate to severe cancer pain are available in the United States as a combination of the opioid and acetaminophen or aspirin (ASA). The drug can be titrated until the maximum safe dose of acetaminophen (4 g/d) or ASA is reached.
![]() Patients with severe pain, including those who fail to reach adequate pain relief with drugs from the second step on the WHO ladder should receive an opioid that is useful in the treatment of severe cancer pain. The drugs useful in the treatment of severe cancer pain include morphine, hydromorphone, fentanyl, oxycodone, and methadone. These opioids may also be combined with acetaminophen or an NSAID or an adjuvant drug when needed. Patients can experience a variation of analgesia and side effects between the different opioids. A clinician may need to rotate among the various opioids to identify the drugs that have the correct balance between pain control and side effects. These drugs should be titrated to analgesic effect or intolerable side effects. There is no maximum dose limitation on the opioid medication itself.
Patients with severe pain, including those who fail to reach adequate pain relief with drugs from the second step on the WHO ladder should receive an opioid that is useful in the treatment of severe cancer pain. The drugs useful in the treatment of severe cancer pain include morphine, hydromorphone, fentanyl, oxycodone, and methadone. These opioids may also be combined with acetaminophen or an NSAID or an adjuvant drug when needed. Patients can experience a variation of analgesia and side effects between the different opioids. A clinician may need to rotate among the various opioids to identify the drugs that have the correct balance between pain control and side effects. These drugs should be titrated to analgesic effect or intolerable side effects. There is no maximum dose limitation on the opioid medication itself.
![]() In the treatment of cancer pain, it is important to distinguish between acute and chronic pain, as the goals of treatment are slightly different. Acute pain is a linear event; the pain starts, and, with relief of the offending event, the pain stops. Chronic pain is cyclical in nature, repeating itself over time. For acute pain, the goal of treatment is pain relief. To accomplish pain relief, the drugs administered should have a rapid onset of action, with the desired duration of action (e.g., 2 to 4 hours). These drugs are given as needed. Common side effects, such as sedation, are usually acceptable and well tolerated by the patient. An example of an acute pain scenario is the patient who falls and suffers a hip fracture at the site of a previous bone metastasis. The patient is treated with short-acting IV narcotics until surgery can be performed to stabilize the fracture.
In the treatment of cancer pain, it is important to distinguish between acute and chronic pain, as the goals of treatment are slightly different. Acute pain is a linear event; the pain starts, and, with relief of the offending event, the pain stops. Chronic pain is cyclical in nature, repeating itself over time. For acute pain, the goal of treatment is pain relief. To accomplish pain relief, the drugs administered should have a rapid onset of action, with the desired duration of action (e.g., 2 to 4 hours). These drugs are given as needed. Common side effects, such as sedation, are usually acceptable and well tolerated by the patient. An example of an acute pain scenario is the patient who falls and suffers a hip fracture at the site of a previous bone metastasis. The patient is treated with short-acting IV narcotics until surgery can be performed to stabilize the fracture.
![]() Chronic pain management has a different focus. The overall goal is pain prevention and the avoidance of undesirable side effects, such as sedation. The analgesic regimen should include long-acting narcotics administered on a regular schedule and should be individualized for the patient based on side effects. Patients with chronic pain also need to have the understanding of how to manage acute exacerbations with short-acting, rapid-onset analgesics, most commonly referred to as breakthrough pain relief. Many cancer patients have chronic pain. Chronic pain is ineffectively managed when the clinician focuses on acute control of the pain in this setting.
Chronic pain management has a different focus. The overall goal is pain prevention and the avoidance of undesirable side effects, such as sedation. The analgesic regimen should include long-acting narcotics administered on a regular schedule and should be individualized for the patient based on side effects. Patients with chronic pain also need to have the understanding of how to manage acute exacerbations with short-acting, rapid-onset analgesics, most commonly referred to as breakthrough pain relief. Many cancer patients have chronic pain. Chronic pain is ineffectively managed when the clinician focuses on acute control of the pain in this setting.
Medications 1–4
![]() Opioid therapy can provide effective pain relief to the majority of patients with cancer pain. Opioids can be classified as pure agonists or agonist antagonists, based on their interactions with opioid receptors in the body. The drugs that are included in the agonist–antagonist subclass include butorphanol (Stadol), nalbuphine (Nubain), pentazocine (Talwin), and buprenorphine (Buprenex). Drugs in this subclass have a ceiling effect for analgesia and may reverse the effects of pure agonists. For these reasons, use of the mixed agonist–antagonist subclass is not recommended in the treatment of cancer pain.
Opioid therapy can provide effective pain relief to the majority of patients with cancer pain. Opioids can be classified as pure agonists or agonist antagonists, based on their interactions with opioid receptors in the body. The drugs that are included in the agonist–antagonist subclass include butorphanol (Stadol), nalbuphine (Nubain), pentazocine (Talwin), and buprenorphine (Buprenex). Drugs in this subclass have a ceiling effect for analgesia and may reverse the effects of pure agonists. For these reasons, use of the mixed agonist–antagonist subclass is not recommended in the treatment of cancer pain.
![]() When managing chronic pain, it is important to remember that there are wide variations in dose requirements. This variation is not based on the size or age of the patient or the amount of disease present. The analgesic dose required to keep a patient out of pain cannot be predicted, but rather, must be determined by educated trial and error. The following are guidelines for opioid use in chronic pain patients.
When managing chronic pain, it is important to remember that there are wide variations in dose requirements. This variation is not based on the size or age of the patient or the amount of disease present. The analgesic dose required to keep a patient out of pain cannot be predicted, but rather, must be determined by educated trial and error. The following are guidelines for opioid use in chronic pain patients.
![]() Start with one drug at the lowest effective dose. Titrate the drug to pain relief or intolerable side effects. If the patient is unable to tolerate one narcotic due to undesirable side effects, switch to an alternative agent.
Start with one drug at the lowest effective dose. Titrate the drug to pain relief or intolerable side effects. If the patient is unable to tolerate one narcotic due to undesirable side effects, switch to an alternative agent.
![]() Use around-the-clock dosing schedules to avoid peaks and valleys in serum analgesic levels.
Use around-the-clock dosing schedules to avoid peaks and valleys in serum analgesic levels.
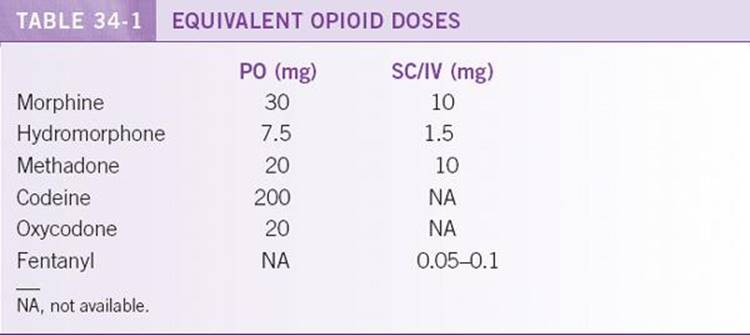
![]() Sustained or long-acting release preparations of narcotics are very useful in this population. When converting between modes of administration or drugs, calculate the equianalgesic dosages to avoid undermedicating a patient. See Table 34-1.
Sustained or long-acting release preparations of narcotics are very useful in this population. When converting between modes of administration or drugs, calculate the equianalgesic dosages to avoid undermedicating a patient. See Table 34-1.
![]() Breakthrough pain medications should be the same or a similar drug used for long-acting pain relief. The minimum effective breakthrough pain medication dose should be equivalent to 12.5% of the patient’s total daily narcotic requirements, or 25% of a single BID dose.
Breakthrough pain medications should be the same or a similar drug used for long-acting pain relief. The minimum effective breakthrough pain medication dose should be equivalent to 12.5% of the patient’s total daily narcotic requirements, or 25% of a single BID dose.
![]() Keep the regimen as simple as possible. Avoid mixing a variety of analgesic regimens.
Keep the regimen as simple as possible. Avoid mixing a variety of analgesic regimens.
![]() Always start a bowel regimen when placing a patient on narcotics, as constipation is a side effect of all narcotics.
Always start a bowel regimen when placing a patient on narcotics, as constipation is a side effect of all narcotics.
![]() Educate the patient and family about dosing and side effects. Discuss and reassure the patient and family about addiction, tolerance, and physical dependence.
Educate the patient and family about dosing and side effects. Discuss and reassure the patient and family about addiction, tolerance, and physical dependence.
![]() Morphine is the drug of choice for moderate to severe cancer pain. It has a wide range of doses available and flexible methods of delivery. Morphine is available as sustained-release, immediate-release, liquid/sublingual, and parenteral preparations. The sustained-release tablets may be given per rectum or sublingually in patients unable to swallow. Oxycodone is available orally as immediate- and sustained-release preparations. Fentanyl is available in the parenteral route, as well as the fentanyl (Duragesic) patch for patients unable to swallow or who cannot tolerate morphine or oxycodone. The patches are applied to the chest wall or back and changed every 48 to 72 hours. The onset of action in these long-acting preparations is 12 hours. When starting a patient on long-acting agents, the clinician needs to provide the patient with immediate-relief preparations for use in the interim, until the long-acting narcotic can achieve adequate serum levels for analgesia.
Morphine is the drug of choice for moderate to severe cancer pain. It has a wide range of doses available and flexible methods of delivery. Morphine is available as sustained-release, immediate-release, liquid/sublingual, and parenteral preparations. The sustained-release tablets may be given per rectum or sublingually in patients unable to swallow. Oxycodone is available orally as immediate- and sustained-release preparations. Fentanyl is available in the parenteral route, as well as the fentanyl (Duragesic) patch for patients unable to swallow or who cannot tolerate morphine or oxycodone. The patches are applied to the chest wall or back and changed every 48 to 72 hours. The onset of action in these long-acting preparations is 12 hours. When starting a patient on long-acting agents, the clinician needs to provide the patient with immediate-relief preparations for use in the interim, until the long-acting narcotic can achieve adequate serum levels for analgesia.
![]() Meperidine (Demerol) should be avoided in the treatment of chronic pain. Meperidine has the very short half-life of 2 to 3 hours. This is ineffective in the management of chronic pain. Meperidine has a toxic metabolite, normeperidine, which is a weaker analgesic but a potent CNS stimulant. Normeperidine has a half-life of ≥25 to 30 hours in the setting of renal failure. This can rapidly lead to accumulation of the drug when used for more than 48 to 72 hours. CNS toxicity can include irritability, tremors, myoclonus, agitation, and seizures. When CNS toxicity occurs, it is important to stop the drug. Naloxone (Narcan) should not be administered, as the effects of normeperidine are not reversed with naloxone and can precipitate worsening CNS toxicity.
Meperidine (Demerol) should be avoided in the treatment of chronic pain. Meperidine has the very short half-life of 2 to 3 hours. This is ineffective in the management of chronic pain. Meperidine has a toxic metabolite, normeperidine, which is a weaker analgesic but a potent CNS stimulant. Normeperidine has a half-life of ≥25 to 30 hours in the setting of renal failure. This can rapidly lead to accumulation of the drug when used for more than 48 to 72 hours. CNS toxicity can include irritability, tremors, myoclonus, agitation, and seizures. When CNS toxicity occurs, it is important to stop the drug. Naloxone (Narcan) should not be administered, as the effects of normeperidine are not reversed with naloxone and can precipitate worsening CNS toxicity.
![]() Propoxyphene (Darvon-N) is another narcotic agent that is ineffective in the treatment of chronic pain. Despite its widespread use, the drug has no more analgesic properties than ASA (650 mg). Propoxyphene has the long half-life of 6 to 12 hours. It also has a toxic metabolite, norpropoxyphene, with a half-life of 30 to 36 hours. Norpropoxyphene has been associated with pulmonary edema, cardiotoxicity, and cardiac arrest.
Propoxyphene (Darvon-N) is another narcotic agent that is ineffective in the treatment of chronic pain. Despite its widespread use, the drug has no more analgesic properties than ASA (650 mg). Propoxyphene has the long half-life of 6 to 12 hours. It also has a toxic metabolite, norpropoxyphene, with a half-life of 30 to 36 hours. Norpropoxyphene has been associated with pulmonary edema, cardiotoxicity, and cardiac arrest.
![]() IM injections should be avoided for the management of cancer pain. The use of IM injections is painful, and absorption is unreliable. The onset of action can be 30 to 60 minutes, and this is not acceptable in the acute pain setting. IV or transmucosal (sublingual or rectal) routes are much more efficacious at getting rapid onset of action in the acute pain setting.
IM injections should be avoided for the management of cancer pain. The use of IM injections is painful, and absorption is unreliable. The onset of action can be 30 to 60 minutes, and this is not acceptable in the acute pain setting. IV or transmucosal (sublingual or rectal) routes are much more efficacious at getting rapid onset of action in the acute pain setting.
![]() The perception that the administration of opioid analgesics for chronic pain management causes addiction is prevalent and is a barrier to adequate pain control. Confusion about the differences among addiction, tolerance, and physical dependence is in part responsible.
The perception that the administration of opioid analgesics for chronic pain management causes addiction is prevalent and is a barrier to adequate pain control. Confusion about the differences among addiction, tolerance, and physical dependence is in part responsible.
![]() Addiction is a pattern of drug abuse characterized by drug craving and overwhelming behaviors that are used to obtain a drug.
Addiction is a pattern of drug abuse characterized by drug craving and overwhelming behaviors that are used to obtain a drug.
![]() Tolerance is a state in which escalating doses of opioids are needed to achieve pain control as the drug effectiveness reduces over time. Tolerance occurs with all of the side effects of narcotics, with the exception of constipation. It is important to educate patients and family members that tolerance too many of the common side effects, such as itching or sedation, will develop, and that the drug should not be abruptly discontinued.
Tolerance is a state in which escalating doses of opioids are needed to achieve pain control as the drug effectiveness reduces over time. Tolerance occurs with all of the side effects of narcotics, with the exception of constipation. It is important to educate patients and family members that tolerance too many of the common side effects, such as itching or sedation, will develop, and that the drug should not be abruptly discontinued.
![]() Physical dependence is the onset of signs and symptoms of withdrawal with abrupt discontinuation of the opioid. Abrupt withdrawal may result in tachycardia, hypertension, diaphoresis, nausea, vomiting, abdominal pain, psychosis, and hallucinations. This is not the same as addiction. Physical dependence and addiction are not synonymous. When stopping chronic opioid medications, the dose should be reduced in increments of 20% every 2 to 3 days to avoid the risk of withdrawal symptoms. Finally, it should be remembered that patients experiencing inadequately controlled pain may engage in what appears to be drug-seeking behavior, which is easy to confuse with addiction.
Physical dependence is the onset of signs and symptoms of withdrawal with abrupt discontinuation of the opioid. Abrupt withdrawal may result in tachycardia, hypertension, diaphoresis, nausea, vomiting, abdominal pain, psychosis, and hallucinations. This is not the same as addiction. Physical dependence and addiction are not synonymous. When stopping chronic opioid medications, the dose should be reduced in increments of 20% every 2 to 3 days to avoid the risk of withdrawal symptoms. Finally, it should be remembered that patients experiencing inadequately controlled pain may engage in what appears to be drug-seeking behavior, which is easy to confuse with addiction.
![]() Adjuvant analgesics can be important in the treatment of cancer pain. Adjuvant analgesics include antidepressants, anticonvulsants, corticosteroids, and local anesthetics. Within the antidepressants, tricyclics are the most effective as an adjunctive therapy for neuropathic pain. Common side effects from the tricyclics include orthostatic hypotension, sedation, urinary retention, confusion, and sexual dysfunction. Doses of the tricyclic antidepressants should be started low and titrated for analgesia. Anticonvulsants are also helpful adjunctive therapies in the treatment of neuropathic pain syndromes. These drugs include carbamazepine (Tegretol), phenytoin (Dilantin), gabapentin (Neurontin), and pregabalin (Lyrica). The usual initiating dose of gabapentin is 100 mg TID titrated up to a maximum of 3600 mg/d. Side effects of these drugs can be self-limiting, including sedation, confusion, and dizziness.
Adjuvant analgesics can be important in the treatment of cancer pain. Adjuvant analgesics include antidepressants, anticonvulsants, corticosteroids, and local anesthetics. Within the antidepressants, tricyclics are the most effective as an adjunctive therapy for neuropathic pain. Common side effects from the tricyclics include orthostatic hypotension, sedation, urinary retention, confusion, and sexual dysfunction. Doses of the tricyclic antidepressants should be started low and titrated for analgesia. Anticonvulsants are also helpful adjunctive therapies in the treatment of neuropathic pain syndromes. These drugs include carbamazepine (Tegretol), phenytoin (Dilantin), gabapentin (Neurontin), and pregabalin (Lyrica). The usual initiating dose of gabapentin is 100 mg TID titrated up to a maximum of 3600 mg/d. Side effects of these drugs can be self-limiting, including sedation, confusion, and dizziness.
![]() Corticosteroids can be useful in the management of bone metastases, nerve compression, elevated intracranial pressure, and obstruction of a hollow viscus. Local anesthetics, such as nerve blocks, lidocaine patches, and eutectic mixture of local anesthetics (EMLA) cream, can aid in the treatment of cancer pain. In extreme cases, IV administration of anesthetics can be used in conjunction with IV or intraspinal narcotics to allow the clinician to administer lower doses of narcotics and spare the patient the complications of sedation seen with high doses of narcotics.
Corticosteroids can be useful in the management of bone metastases, nerve compression, elevated intracranial pressure, and obstruction of a hollow viscus. Local anesthetics, such as nerve blocks, lidocaine patches, and eutectic mixture of local anesthetics (EMLA) cream, can aid in the treatment of cancer pain. In extreme cases, IV administration of anesthetics can be used in conjunction with IV or intraspinal narcotics to allow the clinician to administer lower doses of narcotics and spare the patient the complications of sedation seen with high doses of narcotics.
![]() Bisphosphonates (pamidronate, zoledronic acid) and calcitonin have been used to treat pain from bony metastases. Clinical trials have failed to demonstrate clear evidence for the ability of bisphosphonates to deliver an analgesic benefit over placebo. Calcitonin provides no benefit in metastatic bone pain over placebo, but some studies suggest that it may reduce the intensity and frequency ofneuropathicpain.
Bisphosphonates (pamidronate, zoledronic acid) and calcitonin have been used to treat pain from bony metastases. Clinical trials have failed to demonstrate clear evidence for the ability of bisphosphonates to deliver an analgesic benefit over placebo. Calcitonin provides no benefit in metastatic bone pain over placebo, but some studies suggest that it may reduce the intensity and frequency ofneuropathicpain.
CONSTIPATION5
GENERAL PRINCIPLES
Most constipation in cancer comes from opioid pain management, but the differential diagnosis of constipation is broad.
DIAGNOSIS
![]() Before assuming that all constipation is pain medicine related in the cancer patient, one must remember to consider bowel obstruction, spinal cord compression, hypercalcemia, hypokalemia, diabetes mellitus, hypothyroidism, timing of chemotherapy, uremia, etc., as these must be treated differently. Other possible considerations are different classes of drugs, such as: antacids, anticholinergics, antidepressants, calcium channel blockers, cholestyramine, clonidine, diuretics, levodopa, NSAIDs, psychotropics, and sympathomimetics.
Before assuming that all constipation is pain medicine related in the cancer patient, one must remember to consider bowel obstruction, spinal cord compression, hypercalcemia, hypokalemia, diabetes mellitus, hypothyroidism, timing of chemotherapy, uremia, etc., as these must be treated differently. Other possible considerations are different classes of drugs, such as: antacids, anticholinergics, antidepressants, calcium channel blockers, cholestyramine, clonidine, diuretics, levodopa, NSAIDs, psychotropics, and sympathomimetics.
![]() During opioid treatment, constipation should be expected. Prophylactic measures should always be initiated with the start of opioid therapy. Constipation occurs with all opioids, and pharmacologic tolerance rarely develops. Symptoms from constipation may become so severe that patients may decide to discontinue pain medications. This is preventable with the use of an aggressive laxative regimen.
During opioid treatment, constipation should be expected. Prophylactic measures should always be initiated with the start of opioid therapy. Constipation occurs with all opioids, and pharmacologic tolerance rarely develops. Symptoms from constipation may become so severe that patients may decide to discontinue pain medications. This is preventable with the use of an aggressive laxative regimen.
TREATMENT5
![]() Dietary interventions are almost never sufficient to prevent constipation. Combinations of agents are often necessary. Clinicians should also avoid the use of bulk-forming agents in the absence of a motility agent, especially in debilitated or anorectic patients. When using these agents, it should be remembered that stool softeners and bulking agents do little to relieve constipation but may make stools more comfortable to pass. Their sole use will only lead to constipation with soft stools, and another agent is necessary for adequate treatment. Also, it should be remembered that the onset of abdominal pain or nausea in a patient taking opioids may be due to unrecognized constipation.
Dietary interventions are almost never sufficient to prevent constipation. Combinations of agents are often necessary. Clinicians should also avoid the use of bulk-forming agents in the absence of a motility agent, especially in debilitated or anorectic patients. When using these agents, it should be remembered that stool softeners and bulking agents do little to relieve constipation but may make stools more comfortable to pass. Their sole use will only lead to constipation with soft stools, and another agent is necessary for adequate treatment. Also, it should be remembered that the onset of abdominal pain or nausea in a patient taking opioids may be due to unrecognized constipation.
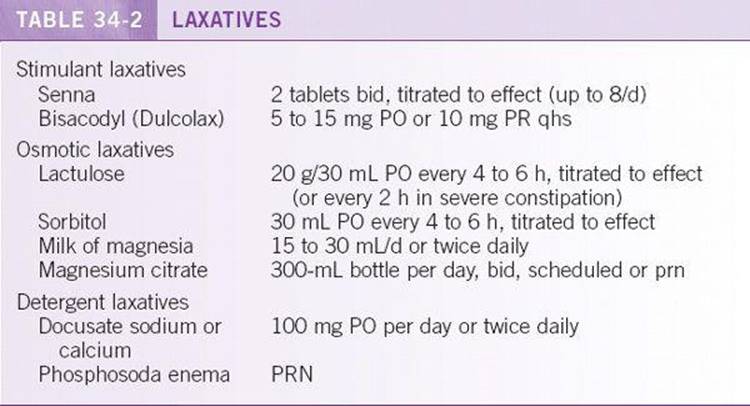
![]() Laxatives can be classified into three categories: stimulant, osmotic, and detergent agents (Table 34-2). Stimulant laxatives irritate the bowel, leading to increased peristaltic activity. Osmotic laxatives draw water into the bowel lumen and increase the moisture content of the stool. In addition, they add to overall stool volume. Detergent laxatives facilitate the dissolution of fat in water and increase the water content of stool. Laxatives can be titrated to a maximal therapeutic dose. Clinicians should try to simplify the bowel regimen, as this will improve patient compliance. Combinations of stimulant and detergent laxatives such as docusate/senna (Senokot-S) are ideal for preventing opioid-induced constipation.
Laxatives can be classified into three categories: stimulant, osmotic, and detergent agents (Table 34-2). Stimulant laxatives irritate the bowel, leading to increased peristaltic activity. Osmotic laxatives draw water into the bowel lumen and increase the moisture content of the stool. In addition, they add to overall stool volume. Detergent laxatives facilitate the dissolution of fat in water and increase the water content of stool. Laxatives can be titrated to a maximal therapeutic dose. Clinicians should try to simplify the bowel regimen, as this will improve patient compliance. Combinations of stimulant and detergent laxatives such as docusate/senna (Senokot-S) are ideal for preventing opioid-induced constipation.
![]() Prokinetic agents such as metoclopramide (Reglan) can increase peristaltic activity and facilitate stool movement. This agent can be used in combination with other laxative agents. Lubricant stimulants and large-volume enemas can also be used but are not recommended for daily use and prophylaxis of opioid-related constipation. The use of these agents is effective while titrating other laxatives to ensure that the patient is having regular bowel movements.
Prokinetic agents such as metoclopramide (Reglan) can increase peristaltic activity and facilitate stool movement. This agent can be used in combination with other laxative agents. Lubricant stimulants and large-volume enemas can also be used but are not recommended for daily use and prophylaxis of opioid-related constipation. The use of these agents is effective while titrating other laxatives to ensure that the patient is having regular bowel movements.
![]() Often patients present with constipation from narcotics of the order of days to weeks in duration. It is important to identify this immediately and treat it aggressively. One can use enemas or suppositories per rectum, or oral regimens such as lactulose, 20 g every 2 hours, until the bowels move. Patients should be instructed to inform their physician if they do not have a bowel movement within any 48-hour time period while they are on narcotics to avoid potentially life-threatening complications.
Often patients present with constipation from narcotics of the order of days to weeks in duration. It is important to identify this immediately and treat it aggressively. One can use enemas or suppositories per rectum, or oral regimens such as lactulose, 20 g every 2 hours, until the bowels move. Patients should be instructed to inform their physician if they do not have a bowel movement within any 48-hour time period while they are on narcotics to avoid potentially life-threatening complications.
DIARRHEA5
GENERAL PRINCIPLES
Diarrhea can be defined as stools that are looser than normal and that may be increased in number over baseline. The definition is based on the frequency, volume, and consistency of stools. In cancer patients, getting up to go to the bathroom multiple times day and night can be exhausting. If persistent, diarrhea can lead to dehydration and electrolyte abnormalities that can lead to the need for a hospital admission.
DIAGNOSIS
Potential causes of diarrhea in the cancer patient can include infections, malabsorption, gastrointestinal bleeding, medications, chemotherapy (particularly 5-FU), radiation to the abdomen or pelvis, and overflow incontinence. It is important to remember that herbals such as ginkgo biloba, ginseng, and licorice may also cause diarrhea.
TREATMENT
![]() Patients should be instructed on the establishment of normal bowel habits. Any change from the normal baseline should be reported to the physician to avoid severe dehydration or electrolyte imbalances. Patients should be counseled on the avoidance of foods containing lactose or other gas-forming foods that can increase abdominal cramping and pain. Another general approach to diarrhea is to increase the bulk of the stools with the addition of psyllium, bran, or pectin. However, sometimes bulk-forming agents can worsen abdominal cramping and bloating.
Patients should be instructed on the establishment of normal bowel habits. Any change from the normal baseline should be reported to the physician to avoid severe dehydration or electrolyte imbalances. Patients should be counseled on the avoidance of foods containing lactose or other gas-forming foods that can increase abdominal cramping and pain. Another general approach to diarrhea is to increase the bulk of the stools with the addition of psyllium, bran, or pectin. However, sometimes bulk-forming agents can worsen abdominal cramping and bloating.
![]() For the medical management of transient or mild diarrhea, the use of attapulgite (Kaopectate) or bismuth salts (Pepto-Bismol) can be useful. Care should be taken to rule out infection by checking Clostridium difficile toxin before using antiperistaltic medications in the setting of recent antibiotic use. Potential infectious workup may include checking for fecal leukocytes, ova, and parasites and stool culture. For more persistent and severe diarrhea, agents that slow down peristalsis are more useful, including the following:
For the medical management of transient or mild diarrhea, the use of attapulgite (Kaopectate) or bismuth salts (Pepto-Bismol) can be useful. Care should be taken to rule out infection by checking Clostridium difficile toxin before using antiperistaltic medications in the setting of recent antibiotic use. Potential infectious workup may include checking for fecal leukocytes, ova, and parasites and stool culture. For more persistent and severe diarrhea, agents that slow down peristalsis are more useful, including the following:
![]() Loperamide (Imodium), 2 to 4 mg PO every 6 hours (maximum, 8 tablets/ day)
Loperamide (Imodium), 2 to 4 mg PO every 6 hours (maximum, 8 tablets/ day)
![]() Diphenoxylate/atropine (Lomotil), 2.5 to 5 mg PO every 6 hours (maximum, 8 tablets/day)
Diphenoxylate/atropine (Lomotil), 2.5 to 5 mg PO every 6 hours (maximum, 8 tablets/day)
![]() Tincture of opium, 0.7 mL PO every 4 hours and titrated as needed (Belladonna can be added as an antispasmodic agent.)
Tincture of opium, 0.7 mL PO every 4 hours and titrated as needed (Belladonna can be added as an antispasmodic agent.)
![]() Octreotide (Dandostatin LAR Depot), 10 to 20 mg IM every 4 weeks
Octreotide (Dandostatin LAR Depot), 10 to 20 mg IM every 4 weeks
![]() For persistent, severe secretory diarrhea, the patient should be admitted for parenteral fluid support and the initiation of octreotide.
For persistent, severe secretory diarrhea, the patient should be admitted for parenteral fluid support and the initiation of octreotide.
![]() Octreotide (Sandostatin), 50 to 500 μg SC/IV every 8 to 12 hours. Begin at 50 μg SC/IV, then titrated up 100 μg per dose every 48 hours to a maximum of 500 μg SC every 8 hours, with titration based on response; may also be given as a continuous IV infusion, 10 to 80 μg/h.
Octreotide (Sandostatin), 50 to 500 μg SC/IV every 8 to 12 hours. Begin at 50 μg SC/IV, then titrated up 100 μg per dose every 48 hours to a maximum of 500 μg SC every 8 hours, with titration based on response; may also be given as a continuous IV infusion, 10 to 80 μg/h.
NAUSEA AND VOMITING5,6
GENERAL PRINCIPLES
Nausea and vomiting are commonly associated with advanced malignancies as a direct result of the disease or as side effects of chemotherapy or other medications. There are multiple potential causes of nausea and vomiting in the cancer patient. Different etiologies for nausea and vomiting may require different interventions for control of the symptoms.
DIAGNOSIS
![]() The three most common forms of chemotherapy-associated nausea are acute, which begins within 1 to 2 hours of chemotherapy; delayed, which occurs 24 hours to 5 days after chemotherapy; and anticipatory, which is a conditioned response from prior occurrences of chemotherapy.
The three most common forms of chemotherapy-associated nausea are acute, which begins within 1 to 2 hours of chemotherapy; delayed, which occurs 24 hours to 5 days after chemotherapy; and anticipatory, which is a conditioned response from prior occurrences of chemotherapy.
![]() A thorough assessment of nausea and vomiting is important to gain an understanding of potential etiologies and to allow for an appropriate choice of antiemetics. A common mnemonic for potential etiologies is the “11 M’s of emesis”: metastases, meningeal irritation, movement, mental (anxiety), medications, mucosal irritation, mechanical obstruction, motility, metabolic, microbes, and myocardial (ischemia, congestive heart failure). Identification of the source of nausea and vomiting dictates treatment.
A thorough assessment of nausea and vomiting is important to gain an understanding of potential etiologies and to allow for an appropriate choice of antiemetics. A common mnemonic for potential etiologies is the “11 M’s of emesis”: metastases, meningeal irritation, movement, mental (anxiety), medications, mucosal irritation, mechanical obstruction, motility, metabolic, microbes, and myocardial (ischemia, congestive heart failure). Identification of the source of nausea and vomiting dictates treatment.
TREATMENT
![]() For prevention of chemotherapy-associated acute nausea, the three classes of drugs with the highest efficacy are corticosteroids (dexamethasone), 5-HT3 receptor antagonists (dolasetron, granisetron, ondansetron, palonosetron), and the neurokinin-1 (NK1) receptor antagonist aprepitant (Emend). Treatment recommendations for acute nausea and vomiting are dependent of the emetogenic potential of the chemotherapy.
For prevention of chemotherapy-associated acute nausea, the three classes of drugs with the highest efficacy are corticosteroids (dexamethasone), 5-HT3 receptor antagonists (dolasetron, granisetron, ondansetron, palonosetron), and the neurokinin-1 (NK1) receptor antagonist aprepitant (Emend). Treatment recommendations for acute nausea and vomiting are dependent of the emetogenic potential of the chemotherapy.
![]() For low-emetogenic therapies, dexamethasone or metoclopramide (a dopa-mine antagonist) is used. For moderately emetogenic therapies, a 5-HT 3 is combined with dexamethasone.
For low-emetogenic therapies, dexamethasone or metoclopramide (a dopa-mine antagonist) is used. For moderately emetogenic therapies, a 5-HT 3 is combined with dexamethasone.
![]() For highly emetogenic chemotherapies, such as platinum-based regimens, aprepitant is combined with a 5-HT3 and dexamethasone.
For highly emetogenic chemotherapies, such as platinum-based regimens, aprepitant is combined with a 5-HT3 and dexamethasone.
![]() For delayed nausea, either single-agent dexamethasone or dexamethasone plus metoclopramide is recommended. If the combination treatment does not work, aprepitant should be considered.
For delayed nausea, either single-agent dexamethasone or dexamethasone plus metoclopramide is recommended. If the combination treatment does not work, aprepitant should be considered.
![]() Anticipatory emesis is a conditioned response from prior cycles of chemotherapy. Patients benefit from benzodiazepines and behavioral therapy (hypnosis, desensitization, relaxation, etc.). The best way to prevent anticipatory emesis is good control of acute and delayed emesis in prior cycles of chemotherapy.
Anticipatory emesis is a conditioned response from prior cycles of chemotherapy. Patients benefit from benzodiazepines and behavioral therapy (hypnosis, desensitization, relaxation, etc.). The best way to prevent anticipatory emesis is good control of acute and delayed emesis in prior cycles of chemotherapy.
![]() Nausea and vomiting from a bowel obstruction can be a challenge to treat, especially when surgery is not an option. Octreotide has been shown to effectively inhibit the secretion of fluid into the intestinal lumen and decrease bloating and abdominal pain, as well as nausea and vomiting. It may be started by continuous infusion or intermittent SC injection at a dose of 100 μg every 8 to 12 hours and titrated every 24 to 48 hours for effect.
Nausea and vomiting from a bowel obstruction can be a challenge to treat, especially when surgery is not an option. Octreotide has been shown to effectively inhibit the secretion of fluid into the intestinal lumen and decrease bloating and abdominal pain, as well as nausea and vomiting. It may be started by continuous infusion or intermittent SC injection at a dose of 100 μg every 8 to 12 hours and titrated every 24 to 48 hours for effect.
![]() Dopamine antagonists are one of the most frequently used antiemetics. These medications have the potential to cause sedation and extrapyramidal symptoms. Medication options include the following.
Dopamine antagonists are one of the most frequently used antiemetics. These medications have the potential to cause sedation and extrapyramidal symptoms. Medication options include the following.
![]() Haloperidol(Haldol), PO, IV, SC
Haloperidol(Haldol), PO, IV, SC
![]() Prochlorperazine(Compazine), PO, PR, IV
Prochlorperazine(Compazine), PO, PR, IV
![]() Droperidol(Inapsine), IV
Droperidol(Inapsine), IV
![]() Promethazine(Phenergan), PO
Promethazine(Phenergan), PO
![]() Perphenazine(Trilafon), PO, IV
Perphenazine(Trilafon), PO, IV
![]() Trimethobenzamide(Tigan), PO, PR
Trimethobenzamide(Tigan), PO, PR
![]() Metoclopramide(Reglan), PO, IV
Metoclopramide(Reglan), PO, IV
![]() Histamine antagonists may also cause sedation and can have a beneficial effect in some patients. The antihistamines also have the added benefit of anticholinergic properties, which can also be beneficial in patients with dual etiologies of nausea. These drugs include the following:
Histamine antagonists may also cause sedation and can have a beneficial effect in some patients. The antihistamines also have the added benefit of anticholinergic properties, which can also be beneficial in patients with dual etiologies of nausea. These drugs include the following:
![]() Diphenhydramine(Benadryl), PO, IV
Diphenhydramine(Benadryl), PO, IV
![]() Meclizine(Antivert), PO
Meclizine(Antivert), PO
![]() Hydroxyzine(Atarax), PO, IV
Hydroxyzine(Atarax), PO, IV
![]() Scopolamine is an anticholinergic agent that is useful in treating nausea induced by the vestibular apparatus. It can also be used adjunctively with other antiemetics in empiric therapy. Scopolamine can be given as an IV or SC scheduled or continuous infusion but is also conveniently available as a transdermal patch.
Scopolamine is an anticholinergic agent that is useful in treating nausea induced by the vestibular apparatus. It can also be used adjunctively with other antiemetics in empiric therapy. Scopolamine can be given as an IV or SC scheduled or continuous infusion but is also conveniently available as a transdermal patch.
![]() Serotonin antagonists have been effective in the treatment of chemotherapy-associated nausea and vomiting. They are also useful for refractory nausea but are typically tried when other medications have failed. The medications available are as follows:
Serotonin antagonists have been effective in the treatment of chemotherapy-associated nausea and vomiting. They are also useful for refractory nausea but are typically tried when other medications have failed. The medications available are as follows:
![]() Ondansetron(Zofran), PO, IV
Ondansetron(Zofran), PO, IV
![]() Granisetron(Kytril), PO, IV
Granisetron(Kytril), PO, IV
![]() Dolasetron(Anzemet), PO, IV
Dolasetron(Anzemet), PO, IV
![]() Palonosetron(Aloxi), IV
Palonosetron(Aloxi), IV
![]() The NK1receptor antagonist aprepitant (Emend) has become first-line therapy on day 1 for highly emetogenic chemotherapies.
The NK1receptor antagonist aprepitant (Emend) has become first-line therapy on day 1 for highly emetogenic chemotherapies.
![]() The use of dronabinol (Marinol) and benzodiazepines is beneficial in some patients, but the mechanism of action remains unclear. Benzodiazepines (i.e., lorazepam [Ativan] at a 1-mg dose) often are useful in conjunction with other classes of antiemetics and may have a synergistic effect.
The use of dronabinol (Marinol) and benzodiazepines is beneficial in some patients, but the mechanism of action remains unclear. Benzodiazepines (i.e., lorazepam [Ativan] at a 1-mg dose) often are useful in conjunction with other classes of antiemetics and may have a synergistic effect.
MUCOSITIS5
GENERAL PRINCIPLES
Mucositis refers to painful inflammation and ulceration of the oral mucosa. Mucositis can result from chemotherapy or radiation therapy. Chemotherapeutic agents that are associated commonly with mucositis include bleomycin, cytarabine, doxorubicin, melphalan, methotrexate, etoposide, and 5-FU. Radiation to the head and neck may also cause mucositis. Patient factors that can contribute to worsening symptoms include poor-fitting oral prostheses, periodontal disease, and overall poor oral hygiene. Patients should undergo repair of ill-fitting prostheses, tooth extraction, and repair of periodontal disease before the initiation of chemotherapy. In the event that repair cannot be done before chemotherapy, the physician should make a referral to an oral surgeon once the patient’s peripheral blood counts have returned to baseline.
DIAGNOSIS
A mucositis grading system established by the National Cancer Institute allows the physician to assess mucositis severity in terms of both pain and the patient’s ability to continue to eat or drink, graded on a scale from 0 to 4. A score of 0 is given when there is no evidence of mucositis. When a patient develops nonpainful erythema or ulcers, but is able to eat or drink, a score of 1 is given. A score of 2 is given when there are mildly to moderately painful erythema or ulcers, but the patient is still able to eat or drink without difficulty. This may require intermittent analgesia. Severe erythema, painful ulcers that cause interference with eating and drinking requiring constant analgesia, scores a 3. Finally, a score of 4 is given when the severity of symptoms requires parenteral analgesia and/or nutritional support.
TREATMENT
A standardized approach to the prevention and treatment of mucositis is essential to quality care in the oncology patient. The prophylactic measures usually used include mouth rinses with sodium chloride, sodium bicarbonate, chlorhexidine (Peridex) or calcium phosphate (Caphosol). Regimens commonly used for the treatment of mucositis and the associated pain include a local anesthetic such as lidocaine, magnesium-based antacids (Maalox, Mylanta), diphenhydramine (Benadryl), and an antifungal such as nystatin (Mycostatin) or Mycelex. These agents are used either alone or at equal concentrations in a mouthwash. The patient can use the mouthwash up to five times per day for relief. In the treatment of severe mucositis, narcotics may need to be used in addition to the agents mentioned earlier.
ANOREXIA AND CACHEXIA7
GENERAL PRINCIPLES
Anorexia and cachexia frequently occur with advanced malignancies and are characterized by a loss of muscle mass and adipose tissue. The increased catabolism of cancer and the anorexia that accompanies it result in increased muscle protein breakdown and lipolysis. These symptoms typically represent progression of disease and are not reversible with parenteral or enteral nutrition. Anorexia and cachexia are significant causes of distress to the patient and their family members.
DIAGNOSIS
Weight loss of more than 5%, decreased appetite and deceased food intake are the hallmarks of cancer related anorexia and cachexia. The specific etiologies of these symptoms are not well understood. The clinician should always assess for other potential etiologies underlying the loss of appetite and weight such as dysphagia, odynophagia, infections, and side effects of medications.
TREATMENT
There are several approaches to the general management of anorexia and cachexia.
![]() Patients should be offered their favorite foods and nutritional supplements if the patients enjoy them. Any dietary restrictions should be eliminated. Portion sizes can be reduced, and food should be made to look appetizing. Foods that have potent odors should be avoided.
Patients should be offered their favorite foods and nutritional supplements if the patients enjoy them. Any dietary restrictions should be eliminated. Portion sizes can be reduced, and food should be made to look appetizing. Foods that have potent odors should be avoided.
![]() There is a variety of pharmacologic approaches for improving appetite. Corticosteroids have an appetite-stimulating effect, as well as effects on the patient’s mood and energy level. Dexamethasone (Decadron) at doses of ≥4 mg/d is recommended. Dexamethasone is preferred because of the relative lack of mineralocorticoid effects, but any steroid will be efficacious such as Prednisone 20 mg/d. Steroids are considered only for short-term treatment, as they lose their efficacy over days to weeks. If longer treatment is anticipated, megestrol (Megace) has also been shown to improve appetite in cancer patients. There is a large variation in the effective dose of megestrol between individual patients. One should begin with 200 mg PO every 6 to 8 hours and titrate up to 400 to 800 mg/d or Megace ES, 650 mg PO daily. The cannabinoids, such as dronabinol (Marinol), have been shown to promote weight gain in cancer patients.
There is a variety of pharmacologic approaches for improving appetite. Corticosteroids have an appetite-stimulating effect, as well as effects on the patient’s mood and energy level. Dexamethasone (Decadron) at doses of ≥4 mg/d is recommended. Dexamethasone is preferred because of the relative lack of mineralocorticoid effects, but any steroid will be efficacious such as Prednisone 20 mg/d. Steroids are considered only for short-term treatment, as they lose their efficacy over days to weeks. If longer treatment is anticipated, megestrol (Megace) has also been shown to improve appetite in cancer patients. There is a large variation in the effective dose of megestrol between individual patients. One should begin with 200 mg PO every 6 to 8 hours and titrate up to 400 to 800 mg/d or Megace ES, 650 mg PO daily. The cannabinoids, such as dronabinol (Marinol), have been shown to promote weight gain in cancer patients.
![]() It should be understood that clinical studies have demonstrated no impact on overall survival or improvement in quality of life when anorexia and cachexia are pharmacologically managed. Thus, treatment of anorexia and weight loss is done primarily because anorexia is distressing to the patients and their families.
It should be understood that clinical studies have demonstrated no impact on overall survival or improvement in quality of life when anorexia and cachexia are pharmacologically managed. Thus, treatment of anorexia and weight loss is done primarily because anorexia is distressing to the patients and their families.
DYSPNEA7
GENERAL PRINCIPLES
Dyspnea can be one of the most frightening symptoms to patients and their family members. Some patients with severe tachypnea will not complain of dyspnea, while others who are not tachypneic report severe dyspnea. For the majority of patients, relief of dyspnea can be achieved with simple interventions.
DIAGNOSIS
Respiratory rate, oxygen saturation, and blood gas levels often do not correlate with the patient’s subjective report. The clinician must accept the patient’s self-report and try to identify and/or correct the underlying etiology of the symptom. In patients with known advanced disease, the burden of investigating the etiology of the dyspnea must be weighed against the limited potential benefit from therapeutic interventions.
TREATMENT
There are three widely used medical approaches for symptomatic breathlessness: supplemental oxygen, opioids, and anxiolytics.
![]() A therapeutic trial of supplemental oxygen may be beneficial; it has been suggested that there is a placebo effect in nonhypoxemic patients. In addition, the cool air moving across the patient’s face from the supplemental oxygen can also have a calming effect and help to relieve the feelings of air hunger. Studies have reported that stimulation of the trigeminal nerve with oxygen can cause a central inhibitory effect and relieve dyspnea. A fan in the room can also help achieve this effect.
A therapeutic trial of supplemental oxygen may be beneficial; it has been suggested that there is a placebo effect in nonhypoxemic patients. In addition, the cool air moving across the patient’s face from the supplemental oxygen can also have a calming effect and help to relieve the feelings of air hunger. Studies have reported that stimulation of the trigeminal nerve with oxygen can cause a central inhibitory effect and relieve dyspnea. A fan in the room can also help achieve this effect.
![]() Opioids can provide relief in dyspnea without any measurable effect on respiratory rate or blood gas measurements. The precise mechanism by which opioids exert this effect is not known. In an opioid-naïve patient, doses lower than those used to achieve analgesia may be effective. Doses of hydrocodone, 5 mg PO every 4 hours, or codeine, 30 mg PO every 2 hours, can be beneficial in these patients. Other opioids can be useful and administered IV for urgent situations or when the PO route is not available. Patients can be maintained on a fixed schedule of opioid IV every 4 to 6 hours. An additional dose of a short-acting opioid, equivalent to 25% to 50% of the amount of baseline opioid taken every 4 hours can be used hourly for intermittent periods of worsening dyspnea. Sublingual morphine can also be helpful in the terminal dyspneic patient.
Opioids can provide relief in dyspnea without any measurable effect on respiratory rate or blood gas measurements. The precise mechanism by which opioids exert this effect is not known. In an opioid-naïve patient, doses lower than those used to achieve analgesia may be effective. Doses of hydrocodone, 5 mg PO every 4 hours, or codeine, 30 mg PO every 2 hours, can be beneficial in these patients. Other opioids can be useful and administered IV for urgent situations or when the PO route is not available. Patients can be maintained on a fixed schedule of opioid IV every 4 to 6 hours. An additional dose of a short-acting opioid, equivalent to 25% to 50% of the amount of baseline opioid taken every 4 hours can be used hourly for intermittent periods of worsening dyspnea. Sublingual morphine can also be helpful in the terminal dyspneic patient.
![]() Dyspnea may cause severe anxiety. Some patients with dyspnea may need more effective treatment for their anxiety. Benzodiazepines can be used in addition to opioids and other nondrug therapies to reduce dyspnea. The clinician should begin with low doses and titrate for desired effects. Sublingual lorazepam has been shown to be quite effective if there is no IV access.
Dyspnea may cause severe anxiety. Some patients with dyspnea may need more effective treatment for their anxiety. Benzodiazepines can be used in addition to opioids and other nondrug therapies to reduce dyspnea. The clinician should begin with low doses and titrate for desired effects. Sublingual lorazepam has been shown to be quite effective if there is no IV access.
ANEMIA8
GENERAL PRINCIPLES
Anemia in cancer patients may be due to the effects of their underlying malignancy (particularly when there is bone marrow involvement) and/or treatment. The basic mechanisms involved are decreased erythropoiesis, impaired iron metabolism, and decreased survival time for RBCs. In addition, erythropoietin production may be impaired.
DIAGNOSIS
Diagnosis is made by CBC, with a hemoglobin and hematocrit that are less than normal.
TREATMENT
Current treatment approaches are aimed at treating the underlying malignancy and boosting red cell mass. Transfusions offer only transient effects and have side effects such as transfusion reactions, iron overload, volume overload, and cardiac congestion. It is recommended that transfusions be administered only to those patients who are suffering from symptoms of anemia with hemoglobin <8 g/dL. Recombinant erythropoietin has been shown to reduce transfusion requirements and improve outcomes in terms of quality of life and response to treatment. ESAs have also been associated with tumor growth and shorter overall survival. Strict guidelines for the use of ESAs of erythropoiesis-stimulating agents (ESAs) have been published by the FDA and can be viewed at http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm200297.htm. ESAs can now only be prescribed by registered users for cancer patients.
EMOTIONAL SYMPTOM MANAGEMENT9
GENERAL PRINCIPLES
Depression occurs in approximately half of cancer patients, though it is often under-diagnosed and undertreated. Specific problems facing these patients include pain, medication side effects, and changes in functional status.
DIAGNOSIS
Typical features of major depression may be present, such as depressed mood for at least 2 weeks, feelings of guilt or worthlessness, inability to concentrate, decreased energy, preoccupation with death or suicide, anhedonia, and changes in eating or sleeping habits. In the cancer patient, one must be aware that drugs such as prednisone, dexamethasone, procarbazine, vincristine, and vinblastine can also cause depression like symptoms. Loss of appetite, fatigue, or insomnia may be secondary to chemotherapy, the cancer itself, or pain, making it difficult to diagnose depression. Excessive guilt, low self-esteem, the wish to die, and hopelessness are most diagnostic of depression in the cancer patient. One must be careful to screen for suicidal ideation, as the incidence of suicide is higher in both men and women with cancer.
TREATMENT
![]() Depression should be screened for and treated in all cancer patients. In addition to counseling by oncologic psychologists, medications can by useful in the treatment of depression.
Depression should be screened for and treated in all cancer patients. In addition to counseling by oncologic psychologists, medications can by useful in the treatment of depression.
![]() Antidepressants may require up to 6 weeks before symptoms are alleviated. The selective serotonin reuptake inhibitors (e.g., citalopram, 20 to 80 mg PO daily), bupropion SR (200 to 400 mg PO daily), and mirtazapine (usual dosage range, 30 to 45 mg PO daily; mirtazapine has sedating effects but may aid those with insomnia) are all reasonable first-line agents. Tricyclic antidepressants have the ability to treat depression and potentiate the effects of opioids on neuropathic pain. Imipramine, amitriptyline, and doxepin are started at 25 mg PO at bedtime, then titrated up 25 to 50 mg every 24 to 48 hours until the desired effect is achieved.
Antidepressants may require up to 6 weeks before symptoms are alleviated. The selective serotonin reuptake inhibitors (e.g., citalopram, 20 to 80 mg PO daily), bupropion SR (200 to 400 mg PO daily), and mirtazapine (usual dosage range, 30 to 45 mg PO daily; mirtazapine has sedating effects but may aid those with insomnia) are all reasonable first-line agents. Tricyclic antidepressants have the ability to treat depression and potentiate the effects of opioids on neuropathic pain. Imipramine, amitriptyline, and doxepin are started at 25 mg PO at bedtime, then titrated up 25 to 50 mg every 24 to 48 hours until the desired effect is achieved.
![]() The psychostimulants methylphenidate, dextroamphetamine, and modafinil are an alternative for depressed patients with cancer (e.g., methylphenidate, 5 mg PO at 9:00 a.m. and noon daily). They begin to work within a short period of time, provide relief from the sedating effects of opioids, and give the patient improved energy. Tolerance can develop to stimulants, and dosages may have to be adjusted over time.
The psychostimulants methylphenidate, dextroamphetamine, and modafinil are an alternative for depressed patients with cancer (e.g., methylphenidate, 5 mg PO at 9:00 a.m. and noon daily). They begin to work within a short period of time, provide relief from the sedating effects of opioids, and give the patient improved energy. Tolerance can develop to stimulants, and dosages may have to be adjusted over time.
ANXIETY9
DIAGNOSIS
The diagnosis and recognition of anxiety can be challenging. Patients often complain of physical and somatic manifestations of anxiety. The patient’s subjective level of distress from fear, isolation, estrangement, or other common stressors is often the impetus for treatment.
TREATMENT
Anxiety is usually treated with benzodiazepines, neuroleptics, antihistamines, or nonpharmacologic psychotherapies. Benzodiazepines are first-line therapy for the treatment of anxiety disorders.
![]() Lorazepam, 0.5 to 2.0 mg PO, IV, or IM, every 3 to 6 hours
Lorazepam, 0.5 to 2.0 mg PO, IV, or IM, every 3 to 6 hours
![]() Alprazolam, 0.25 to 1.0 mg PO, every 6 to 8 hours
Alprazolam, 0.25 to 1.0 mg PO, every 6 to 8 hours
![]() Diazepam, 2.5 to 10 mg PO, PR, IM, or IV every 3 to 6 hours
Diazepam, 2.5 to 10 mg PO, PR, IM, or IV every 3 to 6 hours
![]() Clonazepam, 1 to 2 mg PO, every 8 to 12 hours
Clonazepam, 1 to 2 mg PO, every 8 to 12 hours
Other anxiolytics include the following.
![]() Haloperidol (0.5 to 5 mg PO, IV, or SC every 2 to 12 hours), if there is concern about respiratory depression
Haloperidol (0.5 to 5 mg PO, IV, or SC every 2 to 12 hours), if there is concern about respiratory depression
![]() Thioridazine (10 to 25 mg PO tid), if insomnia and agitation are also present
Thioridazine (10 to 25 mg PO tid), if insomnia and agitation are also present
![]() Hydroxyzine (25 to 50 mg every 4 to 6 hours PO, IV, or SC), which has mild anxiolytic, sedative, and analgesic properties
Hydroxyzine (25 to 50 mg every 4 to 6 hours PO, IV, or SC), which has mild anxiolytic, sedative, and analgesic properties
![]() Buspirone (10 mg PO tid), a nonbenzodiazepine anxiolytic that is useful in patients with chronic anxiety or anxiety related to adjustment disorders
Buspirone (10 mg PO tid), a nonbenzodiazepine anxiolytic that is useful in patients with chronic anxiety or anxiety related to adjustment disorders
Nonpharmacologic interventions for anxiety and distress include supportive psychotherapy and behavioral interventions used alone or in combination, relaxation, guided imagery, and hypnosis.
DELIRIUM9
GENERAL PRINCIPLES
Delirium is common in advanced cancer and is strongly associated with mortality. The differential diagnosis for delirium in the cancer patient includes dehydration, hypo- and hypernatremia, hypocalcemia, uremia, liver failure, drugs (opiates, radiation, chemotherapeutics, benzodiazepines, tricyclic antidepressants, etc.), brain metastases, paraneoplastic syndrome, and infection.
DIAGNOSIS
One must identify the underlying cause so that supportive therapies can be given. Many scales exist for the diagnosis of delirium, including the Mini Mental Status Exam and Memorial Delirium Assessment Scale, and these should be used to both diagnose and follow delirium.
TREATMENT
If supportive techniques do not work, treatment with neuroleptics or sedative medications can be tried.
![]() Haloperidol (Haldol), 0.5 to 1 mg every 1 to 2 hours PO, IV, or SC is the first drug of choice for treatment of delirium and is usually effective for agitation, paranoia, and fear.
Haloperidol (Haldol), 0.5 to 1 mg every 1 to 2 hours PO, IV, or SC is the first drug of choice for treatment of delirium and is usually effective for agitation, paranoia, and fear.
![]() Zyprexa, 5 to 10 mg PO, sublingually, is another possible first-line agent, as it can be given under the tongue.
Zyprexa, 5 to 10 mg PO, sublingually, is another possible first-line agent, as it can be given under the tongue.
![]() Lorazepam, 0.5 to 1.0 mg PO or IV, plus haloperidol (but not lorazepam alone) can be tried next.
Lorazepam, 0.5 to 1.0 mg PO or IV, plus haloperidol (but not lorazepam alone) can be tried next.
![]() Chlorpromazine can be used if no response to antipsychotics is observed within 24 to 48 hours, as it is much more sedating.
Chlorpromazine can be used if no response to antipsychotics is observed within 24 to 48 hours, as it is much more sedating.
INSOMNIA7
DIAGNOSIS
Insomnia, or inability to sleep, is often a result of pain, medications, anxiety, or a mood disorder. Poor sleep can be distressing in the cancer patient, as it can make pain, anxiety, and delirium worse. Proper sleep hygiene and adequate management of pain and other symptoms are beneficial.
TREATMENT
Benzodiazepines (e.g., lorazepam, 0.5 to 2 mg PO qhs) or antidepressants with sedating effects (e.g., trazodone, 50 mg PO qhs, or amitriptyline, 25 to 50 mg PO qhs) may be used in conjunction with the nonpharmacologic measures. Newer agents such as Ambien/Ambien CR (5 to 10 mg/6.25 to 12.5 mg PO qpm), Lunesta (2 to 3 mg PO qpm), and Rozerem (8 mg PO qpm) can be tried. One should be careful when treating insomnia in terminally ill patients, as these can be hypnotic drugs. For some patients, improved cognition may be achieved by discontinuing the medications without an effect on insomnia.
ADDRESSING SPIRITUAL CARE10
![]() When a person has a malignancy, suffering occurs at many levels. Religion or spiritual belief can be a source of great strength or considerable pain to a patient. Some find new faith during a cancer experience, while others find great turmoil. Spiritual care for the oncology patient can be either uncomfortable for the physician or, if the physician is overzealous, uncomfortable for the patient. Many doctors and nurses are appropriately uneasy when it comes to talking about religion because they fear they might be imposing their religious beliefs on others. The role of the physician is to advocate and try to connect a patient with chaplains, the patient’s own religious community, or nonreligious groups that might help to provide solace.
When a person has a malignancy, suffering occurs at many levels. Religion or spiritual belief can be a source of great strength or considerable pain to a patient. Some find new faith during a cancer experience, while others find great turmoil. Spiritual care for the oncology patient can be either uncomfortable for the physician or, if the physician is overzealous, uncomfortable for the patient. Many doctors and nurses are appropriately uneasy when it comes to talking about religion because they fear they might be imposing their religious beliefs on others. The role of the physician is to advocate and try to connect a patient with chaplains, the patient’s own religious community, or nonreligious groups that might help to provide solace.
![]() The role of the oncologic chaplain can greatly aid in the spiritual journey of a patient, both as an inpatient and as an outpatient. Chaplains can help identify patients in spiritual distress and address the religious or spiritual issues raised by their illness. Those who have never had strong religious beliefs may not feel an urge to turn to religion, but as trained listeners, chaplains can help patients identify core beliefs, recognize coping skills, and, potentially, help patients to find sources of strength within or beyond themselves.
The role of the oncologic chaplain can greatly aid in the spiritual journey of a patient, both as an inpatient and as an outpatient. Chaplains can help identify patients in spiritual distress and address the religious or spiritual issues raised by their illness. Those who have never had strong religious beliefs may not feel an urge to turn to religion, but as trained listeners, chaplains can help patients identify core beliefs, recognize coping skills, and, potentially, help patients to find sources of strength within or beyond themselves.
![]() Chaplains also help families identify spiritual resources to enhance their coping with the level of distress during a loved one’s illness. Often, chaplains are privy to information that may not be provided to the medical professional. This can, with permission, be shared for the benefit of the patient and improvement of care. Therefore, it is appropriate to involve chaplaincy in a patient’s care. It is not necessary to ask whether a patient would like a chaplain, as the patient may feel undue pressure based on distorted understandings of a professional chaplain’s role. A trained chaplain showing up at the bedside can lead to positive outcomes, even if the patient is enabled to say, “No, thank you” to spiritual care. Chaplains work to help people in crisis find a measure of control in the midst of what can feel like chaos.
Chaplains also help families identify spiritual resources to enhance their coping with the level of distress during a loved one’s illness. Often, chaplains are privy to information that may not be provided to the medical professional. This can, with permission, be shared for the benefit of the patient and improvement of care. Therefore, it is appropriate to involve chaplaincy in a patient’s care. It is not necessary to ask whether a patient would like a chaplain, as the patient may feel undue pressure based on distorted understandings of a professional chaplain’s role. A trained chaplain showing up at the bedside can lead to positive outcomes, even if the patient is enabled to say, “No, thank you” to spiritual care. Chaplains work to help people in crisis find a measure of control in the midst of what can feel like chaos.
REFERENCES
1. National Comprehensive Cancer Network. Cancer pain treatment guidelines for patients. Version I, 2011. Adult cancer pain. In: National Comprehensive Cancer Network Practice Guidelines in Oncology, 2011:1. Last accessed: 2/14/2011 <http://www.nccn.org/professionals/physician_gls/pdf/pain.pdf>.
2. Pharo GH, Zhou L. Pharmacologic management of cancer pain. J Am Osteopath Assoc. 2005; 105(11 Suppl 5):S21–S28.
3. Levy MH. Drug therapy: pharmacologic treatment of cancer pain. N Engl J Med. 1996; 335:1124–1132.
4. Bonica JJ, Ventafridda V, Twycross RG. Cancer pain. In: Bonica JJ, ed. The Management of Pain. 2nd ed. Phila delphia: Lea& Febiger; 1990:400–460.
5. Ludwig H, Zojer N. Supportive care. Ann Oncol. 2007;18(Suppl1):i37–i44.
6. National Comprehensive Cancer Network. Antiemesis. Version 3, June 2011. In: National Comprehensive Cancer Network Practice Guidelines in Oncology. Last accessed 2/14/2011 <http://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf>.
7. National Comprehensive Cancer Network. Palliative Care. Version 3, June 2011. In: National Comprehensive Cancer Network Practice Guidelines in Oncology. Last accessed 4/03/2011 <http://www.nccn.org/professionals/physician_gls/pdf/palliative.pdf>.
8. National Comprehensive Cancer Network. Cancer- and Chemotherapy-Induced Anemia, Version 2, 2011. In: National Comprehensive Cancer Network Practice Guidelines in Oncology, 2011. Last accessed 4/03/2011 <http://guidelines.nccn.org/epc-guideline/guideline/id/EDDAC6A8-9CDE-B334-F2EB-B9C9062EB883?jumpTo=false#;history=1_EDDAC6A8-9CDE-B334-F2EB-B9C9062EB883_empty_-1>.
9. National Comprehensive Cancer Network. Distress Management. Version I, 2011. Adult cancer pain. In: National Comprehensive Cancer Network Practice Guidelines in Oncology, 2011:1. Last accessed 4/3/2011 <http://www.nccn.org/professionals/physician_gls/pdf/distress.pdf>.
10. Berger J. Identifying spiritual land scapes amongon cologypatients. Chaplaincy Today. 1998; 4(2):15–21.