Time Recommended to Complete: 1 day
Sankar Swaminathan, M.D.
GUIDING QUESTIONS
1. Who is likely to become ill with one of these serious adult viral illnesses?
2. What are the presenting features and laboratory tests that are useful in making a diagnosis?
3. What are the major complications of each of these diseases?
4. What are the treatments available for each viral illness?
5. Which patients should be treated?
6. What are the preventive measures that are available?
7. How does the avian influenza virus differ from other influenza viruses, and why should we worry?
VARICELLA IN THE ADULT
Varicella virus [also called varicella–zoster virus (VZV)] is a double-stranded DNA herpesvirus that causes two diseases: varicella (chickenpox) and zoster (shingles). Chickenpox is a manifestation of primary infection; zoster is caused by reactivation of latent infection.
Epidemiology
The epidemiology of VZV infection has been drastically altered by the introduction of universal vaccination against chickenpox. Approximately 3–4 million cases of chickenpox and 500,000 cases of zoster occurred each year in the United States before the introduction of the single-dose VZV vaccine in 1995. By 2005, dramatic reductions in chickenpox occurred, with the incidence declining by approximately 85%. Two-dose vaccination was instituted in 2006. By 2007, there were only 14 deaths attributed to varicella. Of these only one was in a child and 11 were in elderly patients.
Chickenpox is primarily a disease of childhood. Nevertheless, 10% of the adult population is estimated to be at risk of infection, and the majority of cases in the United States now occur in adults. The virus circulates exclusively in humans, and no other reservoirs of infection are known. The disease becomes epidemic in the susceptible population in winter and early spring, affecting both sexes and all races equally. Transmission occurs via the respiratory route and requires close contact even though the virus is highly infectious, with attack rates of 70–90% in susceptible family members.
In contrast, zoster affects primarily elderly people. Zoster is caused by reactivation of latent VZV in people who previously had chickenpox. Zoster occurs in up to 1% of people over 60 years of age, and 75% of cases occur in those over the age of 45 years. The development of zoster is not associated with exposure to other people with chickenpox or zoster, although patients with zoster may themselves be capable of transmitting the virus to susceptible individuals. Zoster occasionally occurs in younger individuals, particularly those who are immunosuppressed.
CASE 14.1
A 36-year-old mother of two presented to the emergency room with complaints of shortness of breath. She had noted the onset of the skin lesions and low-grade fever 2 days before admission. Her son was recovering from a recent bout of chickenpox. Aside from the rash, she had been feeling well until the day of admission, when she began experiencing a dry cough and increasing shortness of breath.
On examination, this woman had a temperature of 38.5°C and a respiratory rate of 30 breaths per minute. She appeared in moderate respiratory distress. Her extensive skin rash primarily involved the trunk and face. Lesions varied in character, some being papular, vesicular, or pustular. A few crusted lesions were also noted. Pulmonary examination revealed a few rales. A chest X-ray revealed bilateral lower lobe infiltrates with a fine reticulonodular pattern. Arterial blood gas registered a pH of 7.45, a Paco2 of 35 mmHg, and a Pao2 of 70 mmHg on room air.
Intravenous acyclovir was begun. New crops of skin lesions were noted over the first 24 hours; however, the patient then defervesced, and her respiratory status slowly improved. She did not require intubation, and she was discharged on oral acyclovir.
Pathophysiology and Clinical Manifestations
Chickenpox is popularly felt to be a benign childhood rite of passage. Nevertheless, from 1990 to 1994, approximately 100 deaths each year in the United States were attributed to chickenpox and its complications. Deaths continue to occur in healthy adults despite the availability of a vaccine. The overall risk of death is about 15 times higher in adults than in children, being estimated at more than 3 per 10,000 cases. Most deaths in adults are a result of the development of visceral complications as discussed later in this subsection.
The disease begins with infection by the respiratory route. The virus then replicates at local sites (which have not been clearly identified) and infects the reticuloendothelial system. Viremia ensues, followed by diffuse seeding of the skin, internal organs, and nervous system. Replication of the virus occurs in the dermis, leading to degenerative changes and the formation of multinucleated giant cells, producing the characteristic diffuse vesicular rash. A mild prodrome of fever and malaise of 3–5 days usually precedes the rash.
The rash initially appears on the face and trunk and spreads outward. It may also be present on the oral mucosa. It begins as small erythematous papules less than a centimeter in diameter that rapidly evolve into vesicles. As viral replication proceeds and infiltration by polymorphonuclear leukocytes occurs, the lesions appear purulent. A hallmark of chickenpox is that lesions at all stages of development—maculopapules, vesicles, and scabs—are all found together. As they evolve, the lesions appear umbilicated in the center. Successive crops of lesions occur over several days, with complete healing by 10-14 days in uncomplicated cases. The virus establishes lifelong latent infection in the dorsal root ganglia.
Reactivation of VZV can result in zoster, also known as herpes zoster and shingles. Zoster presents as a localized eruption along the course of one or more dermatomes, most commonly the thoracic or lumbar. The rash, which is often preceded by localized pain, begins as erythematous papules that evolve into vesicles. The vesicles may coalesce into large, confluent blisters with a hemorrhagic component. Healing occurs over the course of 2 weeks, although permanent skin changes such as discoloration and scarring may occur.
When zoster affects the first branch of the trigeminal nerve, herpes zoster ophthalmicus may occur, with involvement of the cornea and potentiallysightthreatening complications. Involvement of other branches of the trigeminal or facial nerves may result in unusual presentations with intra-oral vesicles. The constellation of lesions in the external auditory canal, loss of taste, and facial palsy is termed Ramsay Hunt syndrome.
Diagnosis
The diagnosis of chickenpox can usually be made on clinical grounds, based on the characteristics described earlier. Since the eradication of all known natural human reservoirs of smallpox and the discontinuation of universal smallpox vaccination, the clinical diagnosis of chickenpox has been relatively straightforward. Nevertheless, the possibility of smallpox as a biologic weapon and resumption of vaccination of larger segments of the population may necessitate considering smallpox (see below) or disseminated Vaccinia in the differential diagnosis of a diffuse vesicular rash in an adult.
A diffuse vesicular eruption, Kaposi varicelliform eruption, occasionally occurs in patients with eczema. This syndrome may be caused either by vaccination with Vaccinia virus or by herpes simplex virus (HSV). The diagnosis can be made on the basis of the history and identification of the virus in vesicle fluid. Occasionally, enteroviral infection may cause diffuse cutaneous vesicular lesions that mimic early chickenpox. These lesions are often found on the palms, soles, and oral mucosa and do not progress like those of chickenpox.
KEY POINTS
About the Epidemiology, Pathogenesis, and Clinical Manifestation of Chickenpox
1. Chickenpox infected 3–4 million people annually (10% adults) in the United States before vaccine availability; zoster, 500,000 annually.
2. Highly infectious, spreads person to person by air droplets; zoster represents reactivation.
3. Double-stranded DNA virus; enters via the respiratory tract, and then disseminates.
4. Chickenpox primarily infects the skin:
a) Preceded by a mild prodrome.
b) Lesions have a centripetal distribution beginning on the trunk and later spreading to the extremities.
c) Lesions at all stages (maculopapules, vesicles, scabs) are present at the same time.
d) Lesions are pruritic.
5. Zoster is the result of viral reactivation from the nerve ganglion.
a) Involves a single dermatome.
b) Pain precedes the rash.
c) Zoster ophthalmicus involves the cornea; can be sight threatening.
d) Combination of facial palsy, loss of taste, and lesions in external auditory canal is called Ramsay hunt syndrome.
The diagnosis of zoster may sometimes be more difficult, with the primary alternative diagnosis being HSV. Culture of the virus from unroofed vesicles remains a reliable method of differentiating viral agents in this situation, although polymerase chain reaction (PCR)-based tests are more rapid and are also highly specific and sensitive. Antibody-based assays performed on lesion scrapings or vesicle fluid may also be useful if available. PCR testing of cerebrospinal fluid (CSF) may be useful in cases of central nervous system (CNS) involvement.
Complications
The major complications of varicella result from involvement of the pulmonary and nervous systems. Varicella pneumonitis is more common in adults and immunocompromised patients than in children. It has been estimated that as many as 1 in 400 adults with chickenpox have some pulmonary involvement, although most cases appear to be subclinical. When clinical varicella pneumonitis occurs in adults, it may be associated with high morbidity and mortality. The disease can be particularly severe in pregnant women during the later stages of pregnancy, possibly because of both the respiratory impairment resulting from a gravid uterus and the immunologic changes associated with pregnancy. Smoking and the presence of a large number of skin lesions have been identified as risk factors for the development of varicella pneumonia. Tachypnea, dyspnea, and fever with nodular or interstitial markings on chest X-ray are typically observed. Development of encephalitis in association with chickenpox in adults is relatively uncommon, occurring in up to 0.1–0.2% of patients, with mortality being as high as 20%. Seizures are common and are accompanied by headache, fever, and progressive obtundation.
The major complications of zoster are also neurologic. Involvement of the CNS can almost always be demonstrated in relatively asymptomatic patients with zoster when the CSF is examined. The most common complication is postherpetic neuralgia, especially in people over 50 years of age. As many as half of these patients will have persistent severe pain in the area where the lesions appeared. Encephalitis, transverse myelitis, and Guillain–Barré syndrome can also occur in association with an episode of zoster. A specific complication, particularly of ophthalmic zoster, is the subsequent development of granulomatous cerebral angiitis, which may result in stroke. Ophthalmic zoster may also result in keratitis, iridocyclitis, and (in severe cases) loss of vision.
KEY POINTS
About the Complications Associated with Varicella Infection
1. Pneumonia in adults can be fatal.
a) Severity is increased in pregnant women and smokers.
b) Severity often correlates with extent of the skin lesions.
2. Encephalitis is a rare complication associated with seizures, headache, obtundation, and 20% mortality.
3. Zoster is associated with multiple complications:
a) Postherpetic neuralgia occurs in up to 50% of cases. More common in patients over 50 years of age.
b) Guillain–Barré syndrome, transverse myelitis, and encephalitis are occasionally seen.
c) Keratitis, iridocyclitis, blindness, and granulomatous cerebral angiitis are also possible.
4. Dissemination in immunosuppressed patients is often fatal.
Chickenpox and zoster are often more severe in the immunosuppressed patient. Bone marrow transplant recipients and children with hematologic malignancies are especially prone to visceral dissemination, with associated high mortality, and they require early and aggressive antiviral therapy.
Treatment
The mainstay of treatment for VZV is acyclovir and related nucleoside analogs that inhibit the viral DNA polymerase. Oral acyclovir therapy is recommended for adults and adolescents with chickenpox. Treatment reduces the total number of lesions and shortens the duration of lesion formation by about 1 day. Whether treatment reduces the likelihood of the serious complications described earlier in adults is unknown. The recommended adult dosage is 800 mg five times daily.
The minimum inhibitory concentration of acyclovir for VZV is 2–6 mmol/L, which is difficult to achieve by oral administration. Intravenous treatment is indicated in cases of varicella pneumonia and should be considered in other cases of visceral or CNS involvement. The usual dosage is 5–10 mg/kg every 8 hours. Prompt infectious disease consultation should be obtained in all cases of complicated varicella or varicella in the immunocompromised patient.
Oral treatment of chickenpox and zoster is recommended for adults and children within 24 hours of onset of symptoms. Treatment of chickenpox reduces constitutional symptoms and the number of lesions shortens the duration of symptoms by about 1 day. In children, the oral dosage is 20 mg/kg four times daily for 5 days (maximum of 800 mg daily). Adolescents and adults dosage is up to 800 mg five times a day. Antiviral treatment of zoster reduces acute neuritis and accelerates healing. Treatment in the immunosuppressed patient prevents dissemination. Ophthalmic zoster is usually treated with oral acyclovir or with the more bioavailable agents, valacyclovir and famciclovir. Treatment of cutaneous zoster may also reduce the incidence or duration of postherpetic neuralgia, but the data supporting these effects has been questioned. Nevertheless, oral famciclovir and valacyclovir are approved for this indication and are more convenient than acyclovir because they are administered less frequently. Concurrent administration of corticosteroids to treat postherpetic neuralgia is also controversial, but some studies claim improvement in quality of life when steroids are added to antiviral therapy.
Prevention
A live attenuated varicella vaccine has been available since 1995. It is close to 100% effective in preventing serious disease, and it has a low incidence of side effects. Immunity has been persistent over the period since initial licensure. Varicella vaccination is recommended for all susceptible individuals over the age of 12 months. Although rates of zoster are lower in vaccines, the vaccine strain may actually reactivate more frequently, but sub-clinically. Vaccination becomes more important as its acceptance rate increases, because the likelihood of infection during childhood decreases, increasing the risk of adult disease. The most recent recommendations are that all children receive two doses of varicella vaccine before the age of 4–6 years, with the first dose at 12–15 months of age. Adults without evidence of prior infection should also be vaccinated, and children and adults who have received only one dose in the past should receive a second catch-up dose. The vaccine should not be administered to pregnant women or immunocompromised individuals.
KEY POINTS
About the Treatment and Prevention of Varicella and Zoster Infections
1. Acyclovir is recommended for adolescents and adults with chickenpox. Those with serious infection should receive high-dose intravenous therapy.
2. Antiviral treatment (acyclovir, famciclovir, or valacyclovir) is recommended for all cases of zoster.
a) Reduces acute neuritis and accelerates healing.
b) Prevents dissemination in the immunocompromised host.
c) May reduce postherpetic neuralgia.
d) Efficacy of concurrent treatment with corticosteroids to reduce postherpetic neuralgia is controversial.
3. Live attenuated vaccine is highly efficacious for chickenpox.
a) Recommended for all susceptible individuals over the age of 12 months.
b) Has essentially eliminated childhood illness and death from chickenpox in the United States.
4. Zoster vaccine was released in 2006.
a) It reduces the attack rate by 50%
b) It reduces postherpetic neuralgia.
5. Varicella–zoster immunoglobulin is effective at preventing active disease.
a) Give within 96 hours of exposure.
b) Recommended for all exposed pregnant women and immunocompromised patients.
In 2006, a zoster vaccine was approved for use in patients over 60 years of age who have not previously had zoster. The vaccine achieved an approximately 50% reduction in the incidence of zoster and a 67% reduction in postherpetic neuralgia, suggesting that the vaccine may lessen the likelihood of complications even if zoster occurs. The zoster vaccine, which has a larger dose of the attenuated virus than the chickenpox vaccine, has now been approved for use in all patients over the age of 50.
Varicella–zoster immunoglobulin (VZIG) is effective in preventing disease in susceptible individuals when administered within 96 hours of exposure. Its use should be considered in all immunocompromised patients and in susceptible pregnant women who have been exposed. Significant exposure is defined as contact in the household or hospital room for more than 1 hour. VZIG should also be administered to newborn infants whose mothers have onset of chickenpox less than 5 days before delivery or up to 48 hours postpartum.
SMALLPOX
Endemic smallpox was eradicated in 1977. As a result, smallpox vaccinations were discontinued for civilians in 1980 and for military recruits in 1989, leaving a high percentage of the world’s population without immunity to this deadly virus. Although only two repositories of the Variola virus are known (the U.S. Centers for Disease Control and Prevention, CDC, in Atlanta and the Research Institute of Viral Preparations in Moscow), stockpiles of the virus may be in the hands of others.
Epidemiology
Smallpox is spread person to person and has no other animal reservoirs. The incubation period before symptomatic illness is 7–17 days (average: 12 days). The period of communicability begins with the onset of rash and continues until all scabs separate from the skin, 3–4 weeks after the onset of illness. The virus is shed from lesions in the oropharynx and on the skin, producing airborne droplets and skin fragments that can be inhaled. Patients are most infectious if they are coughing or have the hemorrhagic form of disease. The communicability of smallpox is low as compared with chickenpox and measles; secondary cases occur most commonly in household contacts and hospital personnel. The virions are relatively resistant to drying and to many disinfectants; they can remain infectious for months at room temperature. Autoclaving, chlorine preparations, iodophors, and ammonia inactivate them.
KEY POINTS
About the Epidemiology of Smallpox
1. Humans are the only reservoir for the disease.
2. Incubation period is 7–17 days.
3. Patients are infectious from the onset of rash until scabs separate from the skin.
a) Person-to-person transmission occurs by inhalation of droplets or skin particles shed by a patient.
b) Spread within households and to hospital personnel.
c) Virions can survive in the environment, but are inactivated by chlorine, ammonia, iodine, and heat.
A number of factors make Variola a potentially dangerous biologic weapon:
• Infection can be aerosol-spread, and the virions can survive in the environment.
• Person-to-person transmission facilitates continued spread after an initial attack.
• Routine vaccination was discontinued, creating large susceptible civilian and military populations.
• The potency of stored vaccine may be declining.
• The disease causes severe morbidity and mortality.
• Health care personnel have no clinical experience with the disease, and delays in diagnosis, treatment, and prevention would therefore be expected.
Virology and Pathogenesis
Variola is a large, double-stranded DNA virus. It replicates in the cytoplasm of host cells that release new viral particles by bud formation on the cell surface. Virus-containing airborne droplets and dust particles are inhaled. The virus then spreads from the upper respiratory tract to the regional lymph nodes, where it enters the bloodstream, causing transient viremia before it invades virtually all body tissues. Epithelial cells are particularly susceptible, accounting for the prominent skin lesions.
Initially, edema develops at infected sites in the skin, accompanied by perivascular infiltration with mononuclear and plasma cells, causing the formation of macular skin lesions. Subsequently, the epithelial cells undergo ballooning degeneration, and spherical inclusion bodies containing clusters of virions (Guarnieri bodies) form in the cell cytoplasm. These changes are accompanied by the formation of papular skin lesions. Cell necrosis follows, accompanied by the formation of skin vesicles. Viral replication then ceases, and the skin lesions become crusted and dry, eventually healing and forming prominent scars.
KEY POINTS
About the Pathogenesis of Smallpox
1. Variola is a double-stranded DNA virus.
2. Replicates in the cytoplasm of host cells. Infectious particles bud from the cell surface.
3. The virus enters the lung in airborne droplets, spreads to regional lymph nodes, and then to the bloodstream.
4. Disseminates to all tissues.
5. Epithelial cells are particularly susceptible; skin develops perivascular infiltration.
6. Ballooning degeneration and inclusion body formation is followed by cell necrosis.
Clinical Manifestations
The first clinical manifestations of the disease are nonspecific and consist of the acute onset of fever, rigors, malaise, headache, backache, and vomiting. Delirium develops in approximately 15% of cases, and a transient erythematous rash may appear. This clinical prodrome lasts 2–4 days and is caused by high-level viremia. During this period, virus can be readily cultured from the blood.
KEY POINTS
About the Clinical Manifestations of Smallpox
1. Febrile prodrome over 2–4 days is associated with high-level viremia. (No prodrome with chickenpox.)
2. Skin lesions are centrifugal (begin on the extremities later moving to the trunk) with smallpox versus centripetal (begin on the trunk and later involve the extremities) with chickenpox.
3. Synchronous development with smallpox versus asynchronous development with chickenpox.
4. Lesions progress in unison from macular to papular to vesicular to crusting, feel shot-like, and leave scars; chickenpox lesions are softer and usually do not scar.
Next, the exanthem becomes apparent. Lesions begin on the face, hands, and forearms, subsequently spreading to the lower extremities and, over the following week, to the trunk [see Figure 14.1 (A)]. The distribution of skin lesions is centrifugal—that is, lesions are first seen on the distal extremities and face and then progress to the trunk. Initially, macules are seen that subsequently form papules, and then progress to pustular vesicles [see Figure 14.1(B)]. After about 2 weeks, the lesions form dry scabs that fall off, leaving scars. The skin lesions progress in a synchronous fashion—that is, at any one time, all skin lesions are at a similar stage.
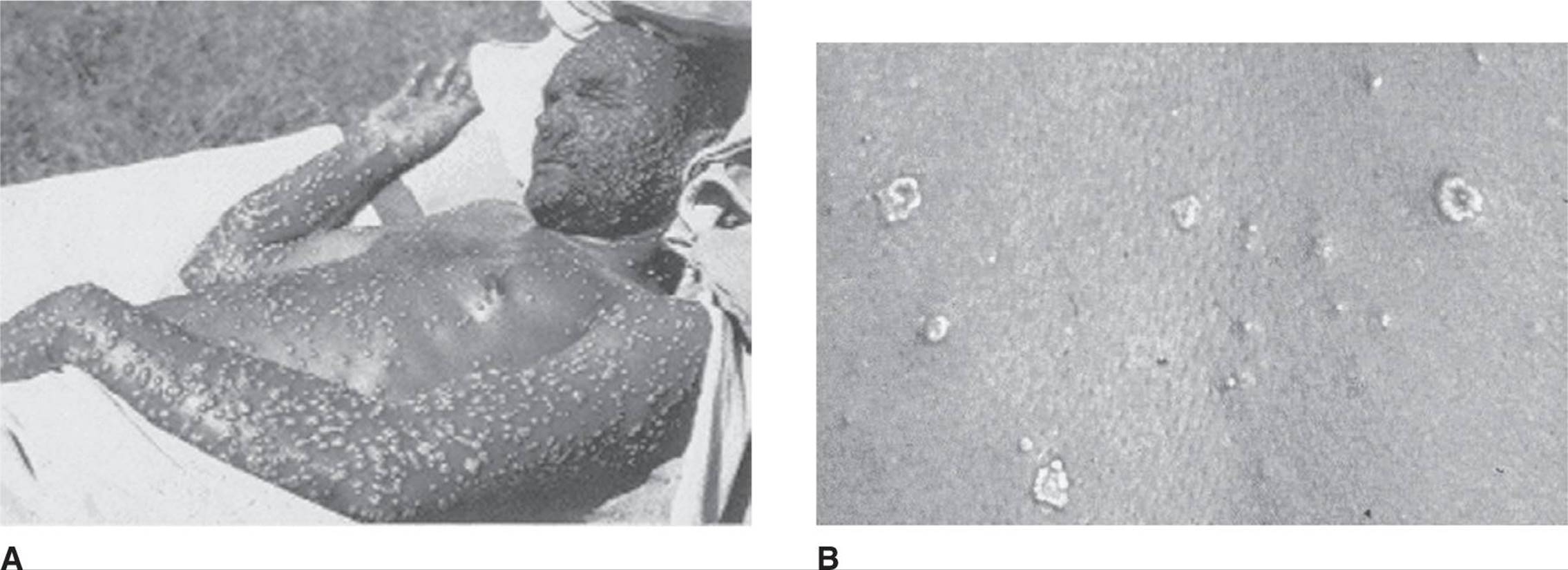
Figure 14.1. Smallpox. A. Adult with severe smallpox skin lesions. (Picture from www.coldcure.com.) B. View of individual raised skin lesions, all at a similar stage of progression. (Picture from Henderson DA. Smallpox: clinical and epidemiologic features. Emerg Infect Dis. 1999;5:537–539.) See color image on color plate 3.
The clinician must be able to differentiate smallpox from chickenpox (varicella virus), a common, naturally occurring infection. Three clinical characteristics are most helpful in differentiating the two diseases:
• First, chickenpox is usually not associated with a significant prodrome. Patients often feel well before the onset of skin lesions.
• Second, the lesions of chickenpox and smallpox begin in different locations. In chickenpox, lesions are first seen on the trunk, and they often spare the face. Subsequently, lesions spread to the arms and legs. That is, the distribution of chickenpox lesions is centripetal—that is, first seen on the central trunk and later on the distal extremities and face—rather than centrifugal (like smallpox).
• Third, the morphology of the skin lesions differs. Skin lesion development is asynchronous in chickenpox: macules, papules, vesicles, and scabs can all be seen at the same time on an individual patient. Chickenpox lesions are also irregular in shape and size, and are usually superficial. Smallpox lesions have smooth borders, are of similar size, and often extend to the dermis. The vesicles of smallpox feel shot-like; chickenpox vesicles are soft and collapse easily.
A series of criteria for the presumptive diagnosis of smallpox are available on the CDC Web site: http://www.bt.cdc.gov/agent/smallpox/diagnosis/evalposter.asp.
Diagnosis
Full-blown disease can be readily diagnosed clinically. The diagnosis can be confirmed by viral culture on chorioallantoic membrane. Diagnostic techniques using PCR are under development and will allow for more rapid diagnosis.
A particular problem from an epidemiologic standpoint is the potential for failure to recognize relatively mild cases of smallpox in people with partial immunity. These patients may shed virus from the oropharynx in the absence of skin lesions.
Treatment and Prognosis
Currently, no treatment of smallpox other than supportive care is available. Cidofovir is active against poxviruses and may be considered for treatment. In animal studies, the tyrosine kinase inhibitor imatinib has been shown to reduce the spread of the closely related Vaccinia virus. Imatinib blocks the Abl family of tyrosine kinases, whose activity is required for extracellular release of the virus. Two additional antiviral drugs are under development. One interferes with a specific host signal transduction pathway required for viral spread, and the other blocks synthesis of a vital poxvirus protein. The overall mortality for smallpox is 30% in unvaccinated and 3% in vaccinated patients. Mortality is highest in very young and very old patients.
Prevention
The identification of a smallpox case represents a public health emergency, and public health officials should be notified immediately. Vaccination of all exposed individuals is recommended as quickly as possible, and vaccination within 7 days is protective.
The vaccine contains Vaccinia virus (cowpox virus) and is administered by intradermal inoculation using a bifurcated needle. Successful vaccination should result in vesicle formation at the site of inoculation, followed by scarification. Immunity has recently been shown to be lifelong. Side effects include low-grade fever and axillary adenopathy. Disseminated Vaccinia occurs in approximately 3 in 10,000 vaccinations. The vaccine is contraindicated in people with HIV infection, immunosuppression, or a history or presence of eczema, or in people who are in close contact with individuals having one of the foregoing conditions. Other complications reported during the recent vaccination of 38,000 first responders included myocarditis or pericarditis, cardiac ischemic events, and postvaccinal encephalitis. Vaccinia immunoglobulin (VIG) may be protective, but the large volume required for intramuscular administration (0.6 mL/kg—for example, 42 mL in a 70-kg person) makes it an impractical tool for mass prophylaxis.
KEY POINTS
About the Diagnosis, Treatment, and Prevention of Smallpox
1. Disease can be readily diagnosed clinically and can be confirmed by viral culture.
2. Minimally symptomatic patients may spread disease; they need to be recognized and isolated.
3. Infected patients should be strictly isolated: use negative-pressure rooms and masks, gloves, and gowns.
4. Cidofovir may prove helpful; imatinib slows spread in animal studies.
5. Vaccine is protective if given within 7 days of exposure.
a) Live Vaccinia virus is given by intradermal inoculation.
b) Contraindicated in HIV infection, immunosuppression, history or presence of eczema.
c) Vaccinia immunoglobulin is protective, but impractical for large numbers of patients.
Infected patients must be strictly isolated. Placement in a negative air-pressure room, with the door closed, is recommended. Masks, gowns, and gloves must be worn when entering the room. Transport of the patient should be limited. All surfaces and supplies must be treated as contaminated. Large numbers of patients would quickly overwhelm isolation facilities and would necessitate separate temporary isolation facilities.
EPSTEIN–BARR VIRUS
Epidemiology
Infection with Epstein–Barr (EBV) is ubiquitous, with 90-95% of all adults displaying serologic evidence of a past infection. In the United States, approximately 50% of children are seropositive by 5 years of age, with a second period of seroconversion occurring in early adulthood. Infection occurs earlier in developing countries and in certain areas of the United States. Most cases of EBV infection are transmitted by the presence of virus in oropharyngeal secretions of asymptomatic shedders. Blood transfusions and transplantation of solid organs or bone marrow may also be associated with EBV transmission.
CASE 14.2
An 18-year-old college freshman presented to the student health office with fever and sore throat for 1 week. His temperature was 38.9°C, his tonsils were enlarged, and he had diffuse nontender lymphadenopathy. The possibility of mononucleosis was raised, and titers for viral capsid antigen (VCA), immunoglobulins G (IgG), and M (IgM) were 1:160 and 1:80, respectively, at that time. Over the next week, he became increasingly ill, developing scleral icterus and fever of 40°C.
On physical examination, the student was noted to have a tender, enlarged liver and palpable spleen. Multiple petechiae were noted on both lower legs.
Laboratory workup showed elevated liver transaminases: 550 IU/L aspartate aminotransferase, 1000 IU/L alanine transaminase, 4000 IU/L lactate dehydrogenase (LDH), and bilirubin 6.0 mg/dL (total) and 4.8 mg/dL (direct). His hematocrit was 30%, and his white blood cell (WBC) count was 2300/mm3, with 20% polymorphonuclear leukocytes (PMNs), 50% lymphocytes, 20% atypical lymphocytes, and 10% monocytes. Numerous atypical lymphocytes were seen on smear. Platelets measured 23,000/mm3, and his erythrocyte sedimentation rate was 12 mm/h. Repeat serology revealed a VCA IgM of 1:160 and a VCA IgG of 1:640. Glucocorticoid therapy was considered; however, over the next 2 weeks, the fever spontaneously resolved, liver function tests returned to normal, hematocrit increased to 35%, WBC count improved to 3000/mm3 (with 70% PMNs), and platelets rose to 100,000/mm3. The young man’s spleen remained enlarged, and he was warned to avoid contact sports for the next few months.
Pathophysiology and Clinical Manifestations
EBV is associated with a variety of clinical disorders arising from various pathogenic mechanisms. Infection during childhood is often asymptomatic or associated with nonspecific symptoms. Infection during adolescence or adulthood more commonly results in the syndrome of acute infectious mononucleosis, characterized by a vigorous humoral and cellular immune response to rapidly proliferating EBV-infected B cells. The most common signs and symptoms of mononucleosis include fever, sore throat, malaise, and lymphadenopathy. The pharyngitis may be exudative and severe. As noted in case 14.2, the enlarged lymph nodes are usually not tender. Other findings, in order of decreasing likelihood, include splenomegaly, hepatitis, palatal petechiae, jaundice, and rash. The rash, when seen, is nonspecific and may be transient. Administration of ampicillin during early EBV-associated mononucleosis very commonly results in a maculopapular rash.
Many aspects of the clinical syndrome of acute infectious mononucleosis—for example, fever, lymphadenopathy, splenomegaly, atypical lymphocytosis—are the result of vigorous T cell and natural killer (NK) cell proliferation and a cytokine response by the immune system rather than a result of direct viral infection, replication, and cytolysis. After resolution of primary infection, EBV persists for life as a latent infection in B cells and as a lytic infection in the oropharynx. Persistent EBV infection is controlled by a virus-specific immune response and most humans remain asymptomatic. However, immunosuppression associated with HIV infection, transplantation, or congenital immunodeficiency can result in uncontrolled oligoclonal or monoclonal B cell proliferation of latently infected cells. Uncontrolled lytic infection in the oropharynx is manifested as oral hairy leukoplakia (OHL) in immunosuppressed hosts.
Individuals with a rare, inherited immunodeficiency linked to the × chromosome and known as X-linked lymphoproliferative syndrome (XLP) or Duncan syndrome are prone to overwhelming lethal primary infection with EBV. Survivors are at risk of the subsequent development of lymphoma and agammaglobulinemia. The genetic defect in these patients has been mapped to a small cytoplasmic protein (SAP) that is implicated in regulation of T and NK cell signaling.
Since the original description of XLP, a spectrum of syndromes characterized by an inability to control EBV infection has been recognized. Most cases of chronic active EBV infection of this type have been described in Japan. Affected patients present with varying degrees of lymphoproliferation that usually culminate in frank lymphoma. Several specific immune deficits have been identified in such individuals and include defects in the genes encoding perforin and the magnesium transporter gene, MAGT1. These cases are characterized by fever, hepatic dysfunction, splenomegaly, lymphadenopathy, and thrombocytopenia.
KEY POINTS
About the Epidemiology, Pathogenesis, and Clinical Manifestation of Epstein-Barr Virus
1. Spread by oral secretions, with 95% of adults carrying the virus.
2. Infects B cells, and illness manifestations are the result of vigorous T cell and natural killer (NK) cell inflammatory response.
3. Fever, sore throat, and lymphadenopathy are the classic triad of mononucleosis.
4. Acute complications of the infection include splenic rupture, neurologic syndromes, and airway obstruction. Less commonly, hepatitis, hemolytic anemia, thrombocytopenia, and neutropenia may occur.
5. Diseases associated with Epstein–Barr virus (EBV) infection include post-transplant lympho-proliferative disease, B cell lymphoma, Hodgkin lymphoma, NK cell lymphoma, oral hairy leukoplakia and gastric carcinoma.
Persistent, latent EBV infection is also associated with development of Burkitt lymphoma, nasopharyngeal carcinoma, certain types of Hodgkin disease, gastric carcinoma, and leiomyosarcomas in immunosuppressed hosts. Infection of NK cells by EBV has been associated with hypersensitivity to mosquito bites and the development of NK cell leukemia. EBV infection of T and NK cells, with development of lymphoma and leukemia, is more common in the Far East than in the United States, where most EBV-associated lymphomas are of B cell origin.
Complications
Serious and life-threatening complications of EBV infection occasionally occur. These include autoimmune hemolytic anemia, erythrophagocytic syndrome, thrombocytopenia, splenic rupture, and neurologic syndromes. The neurologic syndromes, although rare, include encephalitis and Guillain–Barré syndrome. The most common causes of death from EBV-associated mononucleosis in healthy adults are neurologic complications, splenic rupture, and airway obstruction. It should be emphasized that mononucleosis-associated encephalitis is rare and usually benign. Nevertheless, any of these complications may be the presenting sign of mononucleosis and “atypical” cases are not unusual.
Diagnosis
Diagnosis of mononucleosis is usually based on clinical suspicion confirmed by laboratory testing. The clinical diagnosis in the typical adolescent or young adult is usually not too difficult. However, many cases occur in which few or none of the classic signs are evident at initial presentation.
Other causes of the infectious mononucleosis syndrome that should be considered in the young adult are cytomegalovirus (CMV), acute HIV infection, human herpesvirus 6, toxoplasmosis, cat scratch disease, and lymphoma. Laboratory confirmation of EBV infection is achieved primarily by serologic testing. Heterophil antibodies directed against sheep erythrocyte agglutinins are positive in about 90% of cases during the primary infection. Commercially available Monospot testing for heterophil antibodies is less sensitive in children, and sequential Monospot testing or determination of EBV-specific antibodies is indicated when clinical findings are suggestive of EBV infection, and the initial Monospot is negative. The presence of IgM antibodies to viral capsid antigen (VCA) is the most sensitive and specific indicator of acute infection. The antibodies are usually detectable at initial presentation, along with IgG VCA antibody (see Table 14.1). By 4–8 weeks, the IgM VCA antibodies decline and disappear, but IgG VCA antibodies persist for life. Antibodies to Epstein–Barr viral nuclear antigens (EBNAs) do not develop until approximately 4 weeks after onset of symptoms, but they persist for life. Seroconversion to anti-EBNA positivity is therefore indicative of recent EBV infection. Although antibodies to EBV early antigens are often elevated during acute infection, they may persist for variable periods. These antibodies are frequently detectable in healthy convalescent patients many years after infection, and they are therefore of limited utility in diagnosing acute infection.
Table 14.1. Typical Result Patterns in Serologic Testing for Epstein–Barr Virus During Various Stages of Infection
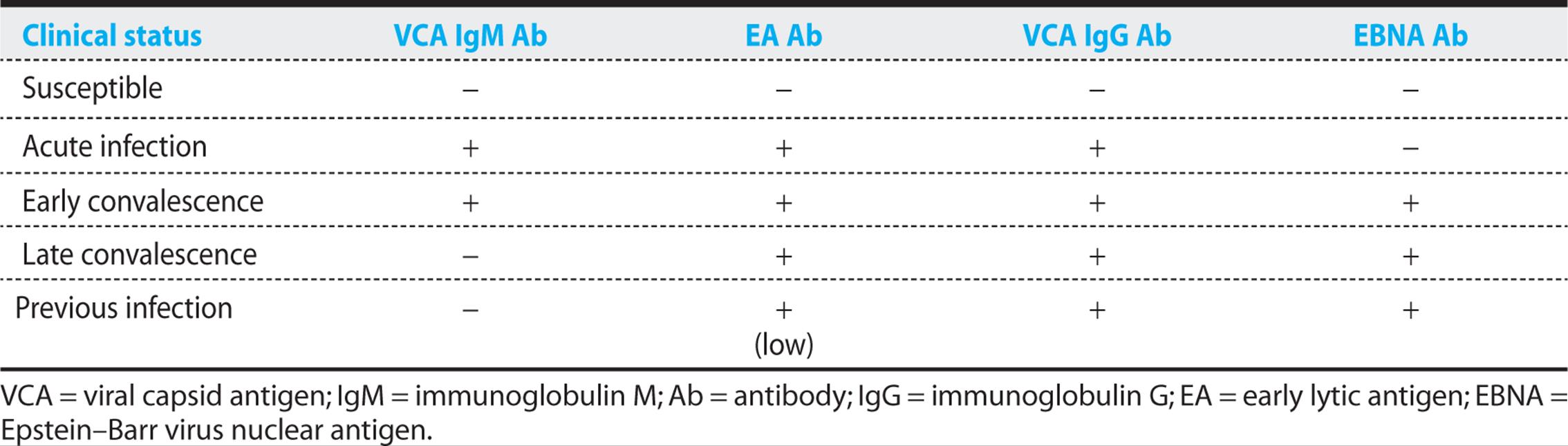
In summary, at the time of presentation, VCA IgM antibody is positive, and VCA IgG and early lytic antigen (EA) antibody are also usually positive. As convalescence proceeds, EBNA antibodies become detectable, and VCA IgM antibody disappears. The EBNA and VCA IgG antibodies remain detectable for life, and EA antibodies are also usually detectable, although at low titers.
Quantifying the EBV DNA load in peripheral blood by PCR identifies immunosuppressed patients who have or who are at high risk of developing EBV-associated B cell lymphomas. Although an elevated EBV DNA load in blood is clearly associated with the development of post-transplant lymphoproliferative disease (PTLD), the predictive value of such a finding is not uniformly high, given that only approximately 50% of bone marrow transplant patients with elevated EBV DNA develop PTLD. An increasing EBV DNA load may be predictive of the development of PTLD, underscoring the need for serial monitoring in high-risk patients. Testing to measure the EBV load in blood is not helpful and is not indicated for the diagnosis or management of primary EBV infection in normal hosts.
Therapy
Treatment of EBV-associated diseases is closely linked with the underlying pathogenesis of the disease. The usual treatment of EBV-associated malignancies involves chemotherapy and radiation therapy as opposed to antiviral strategies, and those options are not discussed here.
INFECTIOUS MONONUCLEOSIS
More than 95% of infectious mononucleosis cases resolve uneventfully without specific therapy, and so supportive treatment is generally indicated. Acetaminophen can be used to reduce fever. Use of concomitant antibiotics for possible bacterial pharyngitis should be judicious, with support from positive bacterial culture results, because a high incidence of allergic reactions to antibiotics such as ampicillin is observed during acute infectious mononucleosis.
The use of corticosteroids for uncomplicated infectious mononucleosis remains controversial. Corticosteroids have been shown to reduce fever and shorten the duration of constitutional symptoms. However, adverse drug complications can arise from even short courses of corticosteroids, and corticosteroid use is probably best avoided in routine infectious mononucleosis, given its self-limiting nature. Corticosteroids are generally reserved for infectious mononucleosis cases complicated by potential airway obstruction from enlarged tonsils, severe thrombocytopenia, or severe hemolytic anemia. These complications result from the excessive immune response rather than from uncontrolled viral infection, and a short course of corticosteroids (1 mg/kg prednisone daily) with tapering over 1–2 weeks can be effective for treating the excessive tonsillar proliferation or autoimmune symptoms. Corticosteroids might also be used for other autoimmune complications occasionally associated with infectious mononucleosis—for example, CNS involvement, myocarditis, or pericarditis. Unless contraindicated, administration of acyclovir concurrently with corticosteroids is the author’s general practice.
In general, acyclovir for uncomplicated infectious mononucleosis inhibits oral viral replication, but provides no clinical benefit. In rare, complicated cases of primary EBV infection and infectious mononucleosis in which the patient is immunosuppressed or severely ill, acyclovir or ganciclovir treatment may be rational, given the safety profile of these drugs, their ability to inhibit EBV replication in vitro and in vivo, and anecdotal reports of clinical response in unusual cases in which excessive EBV replication may have been pathogenic.
Splenic rupture is a rare, but a potentially fatal complication of infectious mononucleosis, occurring in approximately 0.1% of cases. Splenic rupture is more common in men, and approximately half of cases are spontaneous (not associated with trauma or other contributory factors). In one review of 55 cases of splenic rupture associated with infectious mononucleosis, all cases occurred within 3 weeks after the start of the illness. Another case–control study that combined physical, ultrasound, and laboratory examinations of patients with infectious mononucleosis found that physical examination was an insensitive method of detecting splenomegaly (17%), but that all patients were found to have splenomegaly for the first 20 days, and the severity of laboratory abnormalities did not correlate with splenic enlargement.
KEY POINTS
About the Diagnosis of Epstein-Barr Virus
1. The heterophil antibody agglutination test is positive in 90% of primary disease.
2. The Monospot test may be negative, especially early in the course of the disease.
3. The Monospot is also less sensitive in children and specific serologic testing is often necessary for diagnosis.
4. Titer of immunoglobulin M (IgM) antibody to viral capsid antigen (VCA) is the most sensitive and specific test.
a) Titer is often elevated at the time of presentation.
b) Declines quickly and disappears by 4–8 weeks; a positive titer indicates recent infection.
c) An elevated immunoglobulin IgG VCA titer persists for life.
5. The EpsteinBarr nuclear antigen becomes detectable after 4 weeks, and a positive titer indicates remote infection.
6. Antibodies to early Epstein–Barr viral antigens (EA) are usually not helpful.
7. The differential diagnosis includes CMV and acute HIV infection.
8. Serial quantitative PCR testing of the viral load may be helpful for predicting the risk of subsequent lymphoproliferative disease in transplant patients with Epstein–Barr virus infection.
Although various strategies to minimize the risk of splenic rupture have been advanced, incorporating the results of physical examination and ultrasound imaging, no studies have validated the utility of any approach. It therefore seems prudent to recommend that the patient avoid, for a minimum of 4 weeks after the onset of illness, contact sports or activities (such as weightlifting) that raise intra-abdominal pressure.
Patients recovering from infectious mononucleosis may shed virus in their saliva for a period of several months after recovery despite being clinically well (see “Epidemiology” earlier in this subsection). Furthermore, it is clear that all latently infected humans may intermittently shed EBV in saliva. It is therefore difficult for seronegative subjects to avoid the risk of acquiring EBV infection. It appears that intimate sexual contact is more likely to transmit EBV infection.
EBV-ASSOCIATED LYMPHOPROLIFERATIVE SYNDROMES
Some patients have an unusual clinical course following infectious mononucleosis with severe illness and evidence of uncontrolled active EBV infection. These patients typically have extremely high EBV viral loads in blood, and exhibit end-organ involvement with proliferating EBV-infected lymphocytes. Such patients, including those with XLP, frequently progress to develop aggressive lymphoma. Bone marrow transplantation may be curative in such cases.
Chronic Fatigue Syndrome
Infection with EBV has also been implicated as a cause of fatigue syndrome. However, seroepidemiologic studies have argued against a pathogenic role for EBV in chronic fatigue syndrome. In addition, a placebo-controlled study with acyclovir has shown no efficacy for patients with chronic fatigue syndrome.
Oral Hairy Leukoplakia
OHL is an unusual lesion of the tongue found in HIV-infected patients. Vigorous EBV lytic replication is present in the excessively proliferating epithelium. This is the only instance in which disease appears to be a direct consequence of lytic EBV replication, and oral acyclovir therapy (3.2 g daily) can temporarily reverse the lesions. However, because nucleoside analogs have no effect on persistent, latent EBV infection, lytic EBV replication and OHL frequently recur upon withdrawal of therapy. Successful control of HIV infection with highly active antiretroviral therapy (HAART) usually results in resolution of OHL.
KEY POINTS
About Therapy of Epstein-Barr Virus
1. Patients with acute mononucleosis are generally given supportive care.
a) Avoid antibiotics when possible.
b) Ampicillin almost always causes a rash.
c) Use prednisone for airway obstruction, thrombocytopenia, or hemolytic anemia.
d) Supportive care is all that is usually necessary even in severe cases.
2. Chronic active infection with Epstein–Barr virus (EBV)
a) Is usually due to a subtle innate immune deficiency;
b) presents as progressive and relapsing disease after primary mononucleosis;
c) produces severe end-organ involvement; and
d) usually results in lymphoma that may be curable with bone marrow transplantation.
3. In chronic fatigue syndrome, antiviral therapy is of no benefit.
4. Oral hairy leukoplakia can result from lytic EBV infection in HIV-infected patients.
a) Acyclovir can control the infection.
b) Relapse often occurs when treatment is discontinued.
HANTAVIRUS
CASE 14.3
In 1993, a 19-year-old male marathon runner who had been in excellent health presented to a local emergency room in New Mexico complaining of fever, myalgia, chills, headache, and malaise. He had no dyspnea or cough. His fiancée had died 2 days earlier of a respiratory illness that was not characterized. The patient had a temperature of 39.4°C, a blood pressure of 127/84 mmHg, a heart rate of 118 per minute, and a respiratory rate of 24 per minute. The remainder of his physical examination was normal.
Laboratory examination revealed a hematocrit of 49.6%; a WBC count of 7100/mm3, with 66% segmented neutrophils and 10% band forms; a platelet count of 195,000/mm3; a creatinine level of 1.1 mg/dL; a serum lactate dehydrogenase level of 195 IU/L; and an oxygen saturation of 91% on room air. Urinalysis and chest X-ray were both normal.
The patient was discharged after treatment with acetaminophen, antibiotics, and amantadine; but, 2 days later, he returned to a clinic complaining of persistent symptoms, now including vomiting and diarrhea. He was discharged with no change in diagnosis or therapy. Over the following day, a cough productive of blood-tinged sputum developed, and the young man’s respiratory distress worsened. He suffered cardiopulmonary arrest and could not be resuscitated.
A chest X-ray during the terminal illness revealed diffuse alveolar and interstitial infiltrates.
Case 14.3, which is taken from the description of the outbreak of hantavirus pulmonary syndrome (HPS) in the Four Corners region of New Mexico, Arizona, Colorado, and Utah in 1993, dramatically illustrates almost every characteristic of this devastating illness spread by rodents. Hantaviruses are members of the Bunyavirus family, and have a segmented single-stranded RNA viral genome.
Epidemiology
A number of hantavirus strains are found in a wide variety of rodents throughout the United States and Central and South America (see Table 14.2). Hantaviruses are carried by chronically infected rodents, which do not become ill but shed the virus in their saliva and urine freely. Humans become infected when they inhale aerosols of these infected fluids. Risk factors thus include cleaning or entering buildings that harbor rodents. Several species of mice and rats that harbor hantavirus strains readily enter human dwellings in many areas of the United States. Since 1993, cases of HPS have been reported in virtually all geographic areas of the United States and Central and South America. In United States, most infected people are thought to develop disease, as seropositivity in endemic areas is very low. Although relatively rare, dozens of cases have continued to occur annually in the United States since 1993, when the virus was first identified (see Figure 14.1). Incidence is probably affected by various factors, including seasonal variables, such as rainfall and temperature, which affect rodent populations. Most recently, in 2012, a cluster of cases occurred in Yosemite National Park, in campers who occupied cabins that had been entered by mice. Mortality remains high, ranging between 20% and 50% of reported cases (Figure 14.2). Many different hantaviruses have been found in various rodents across the United States, but have not been associated with human disease, raising the possibility of emerging hantavirus diseases in the future. The segmented nature of the hantavirus genome also raises the possibility of novel pathogenic strains arising through reassortment.
Table 14.2. Rodent Hosts and Hantaviruses Causing HPS in the United States

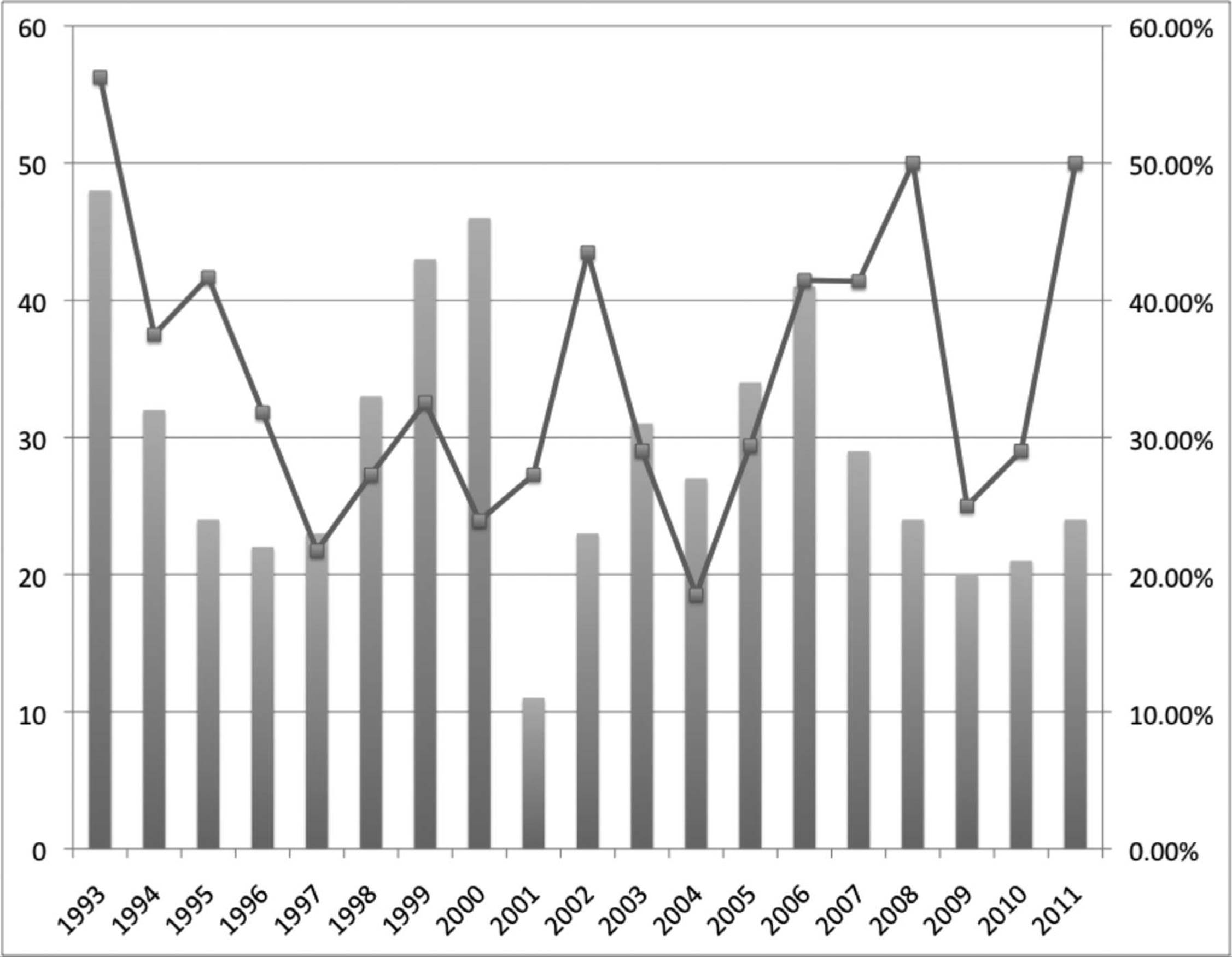
Figure 14.2. Annual incidence of hantavirus pulmonary syndrome (HPS) cases in the United States and case fatality (black line). The number of cases varies yearly probably due to environmental and ecological factors but mortality is invariably high. (Adapted from CDC (http://www.cdc.gov/hantavirus/surveillance/annual-cases.html)
Pathophysiology and Clinical Manifestations
The incubation period for HPS ranges from 1 to 6 weeks, with most cases occurring 2–4 weeks after exposure. As already described, HPS begins with fever and myalgias that may be associated with abdominal complaints. Initially, the patient does not appear extremely ill. Over the next few days, respiratory symptoms develop. These are initially mild, and cough and dyspnea may be minimal. Fever, tachycardia, mild hypotension, and hypoxia are usually present. Hemoconcentration, presence of immature white blood cells (WBCs), mild thrombocytopenia, increased partial thromboplastin time, and lactate dehydrogenase are all typical. A pulmonary vascular leak syndrome occurs, and hypoxia, shock, and pulmonary edema may develop rapidly. Little inflammation is seen in autopsies or biopsies of affected lung.
Diagnosis
Hantavirus serology is almost always positive in patients at the time of admission. An enzyme-linked immunosorbent assay (ELISA) is available from the CDC and some state health laboratories. A positive IgM in acute sera and IgG (fourfold rise) is diagnostic. Immunohistochemistry is also specific and can be used to identify hantavirus in infected tissue biopsies. Reverse transcriptase-polymerase chain reaction (RT-PCR) was very useful in the initial identification of the etiology, but is not the preferred diagnostic test for routine use. If HPS is suspected, infectious disease consultation should be obtained immediately, and the CDC should be notified.
Therapy and Prevention
If the patient can be supported through the period of hypoxia and shock, recovery can be complete. It is important to realize that in HPS the vascular permeability of the lung is abnormal; fluid administration should be performed with this fact in mind. Intravenous ribavirin has been used in experimental treatment protocols; however, it was neither effective in open-label use in 1993 nor in a subsequent placebo-controlled trial. It is not approved or available for use in treating HPS. Extracorporeal membrane oxygenation (ECMO) has been reported to be helpful in the management of severe cases.
KEY POINTS
About Hantavirus
1. Spread by rodents that shed the virus in their saliva and urine; virus is inhaled as an aerosol.
2. Found throughout the United States.
3. Starts as a febrile illness with prominent myalgia, and may proceed to fulminant respiratory failure.
a) Virus causes a pulmonary capillary leak syndrome with acute respiratory distress syndrome (ARDS).
b) Severe hypoxia, hemoconcentration, throm-bocytopenia and increased partial thromboplastin time, and lactate dehydrogenase (LDH) are typical.
4. Serologies, polymerase chain reaction, and immunohistochemical staining are all available for diagnosis.
5. If supportive care and cautious fluid administration assist the patient to survive the ARDS, full recovery is possible.
Prevention of HPS consists of personal precautions to avoid inhalation of aerosolized material contaminated by rodents, and general measures to reduce rodent infestation. No exposed health care workers have ever shown evidence of infection or illness. However, there has been documented human-to-human transmission of Andes virus, a related virus that causes HPS, in South America. Universal precautions are therefore advised for all those caring for patients with HPA.
SEVERE ACUTE RESPIRATORY SYNDROME
Epidemiology
In March 2003, the World Health Organization (WHO) orchestrated a worldwide effort to control a sudden outbreak of a progressive respiratory illness termed severe acute respiratory syndrome (SARS). Retrospectively, it was determined that the epidemic first arose in Guangdong Province, China, in 2002, where it affected at least 300 people. In February 2003, an infected business man traveling from China stayed in a hotel in Hong Kong and infected 10 other individuals staying on the same floor. These individuals in turn spread the illness to five different countries, including Hong Kong, Singapore, Vietnam, Thailand, and Canada. The illness was spread primarily through air droplets in closed spaces including airplanes. Family members and hospital personnel who failed to maintain respiratory precautions were primarily affected. The virus is also shed in the stool, and in one regional outbreak, infection spread through an apartment complex as consequence of a defective sewage system. In all, 8096 patients were identified worldwide, with a fatality rate of approximately 9.6%. Only eight cases were confirmed in the United States. Twenty percent of the cases were in health care workers. Several subsequent small clusters of infection occurred in 2004, originating from laboratory exposures. Since 2004, there have been no further documented cases of SARS. However, in 2012, two cases of severe respiratory illness associated with a coronavirus similar but distinct from SARS coronavirus-like virus (SCoV) occurred in two men from the Middle East. No human-to-human transmission of this novel coronavirus has been documented and the cases are currently under investigation.
Virologic and epidemiologic studies led to the isolation of SCoV-like viruses from Himalayan palm civets in a live-animal market in Guangdong, China. Infection of another small mammal, a raccoon dog, was also confirmed. However, these cases are thought to have been secondary infections and the most likely natural reservoir is the horseshoe bat.
Cause and Pathogenesis
The causative agent of SARS was quickly identified as a single-stranded RNA coronavirus. This virus, named SCoV has characteristics similar to those of the influenza and measles viruses. However, before the SARS outbreak, coronaviruses were known to be among the most common causes of adult viral upper respiratory infection (URI), producing clinical symptoms and signs identical to those caused by rhinoviruses. The SARS strain has a unique genomic sequence, being most closely related to bovine and avian coronaviruses and distantly related to other human coronaviruses. This enveloped virus does not withstand drying, but may remain infectious in a warmer, moist environment. On average, the virus survives on surfaces and hands for approximately 3 hours.
The virus attaches to cells in the respiratory tract and enters the cytoplasm, where it multiplies. It is then released from dead cells or extruded from living cells. The severe tissue damage associated with SARS infection is thought to be largely a result of the host’s overly vigorous immune response to the virus. Coronavirus is spread primarily by respiratory droplets produced by coughing. Epidemiologic studies suggested that a small subset of SARS patients were particularly efficient at spreading the virus to others; they have been called “super spreaders.” These individuals had severe infection and were suspected to be producing small droplets that more efficiently aerosolized and remained in the air for prolonged periods.
Clinical Manifestations
The infection attacks primarily adults aged 25–70 years who are healthy. Children are generally spared, although a few cases have been suspected in children under the age of 15 years. The incubation period typically lasts 2–14 days. Infectiousness is thought to begin at about day 5 and peak at about day 10 of illness. The illness usually begins with a severe febrile prodrome. This fever is often high and can be associated with chills and rigors. Fever is accompanied by headache, malaise, and myalgias. During this phase of the illness, respiratory symptoms are mild. Rash and neurologic symptoms and signs are usually absent. Gastrointestinal symptoms are also usually absent at this stage, although diarrhea has been reported in some cases. The lower respiratory phase of the illness begins 3–7 days after the onset of symptoms. Patients begin to experience a severe, dry, nonproductive cough, accompanied by dyspnea and hypoxemia. Respiratory distress is often severe, with 10–20% of patients requiring intubation and mechanical ventilation.
Laboratory findings may include a decreased absolute lymphocyte count. The total peripheral WBC count is usually normal or decreased. At the peak of the respiratory illness, 50% of patients develop leukopenia and thrombocytopenia (50,000–150,000/μ.L). Muscle and hepatic enzymes are often elevated early in the respiratory phase, reflecting the onset of rhabdomyolysis and hepatitis. Levels of creatine phosphokinase can be as high as 3000 IU/L, and hepatic transaminases usually are two to six times normal. Serum lactate dehydrogenase (LDH) is elevated in 70–80% of patients. Renal function usually remains normal.
Chest X-ray is usually normal during the febrile prodrome, but changes dramatically during the respiratory phase. The initial abnormalities seen are focal interstitial infiltrates that quickly progress to more generalized, patchy, interstitial infiltrates. In the late stages, these interstitial infiltrates develop into areas of dense consolidation. At autopsy, lung pathology may reveal pulmonary edema, hyaline membranes, and desquamation of type 2 pneumocytes. In later stages, fibroblast proliferation is observed in the interstitium and alveoli.
Diagnosis
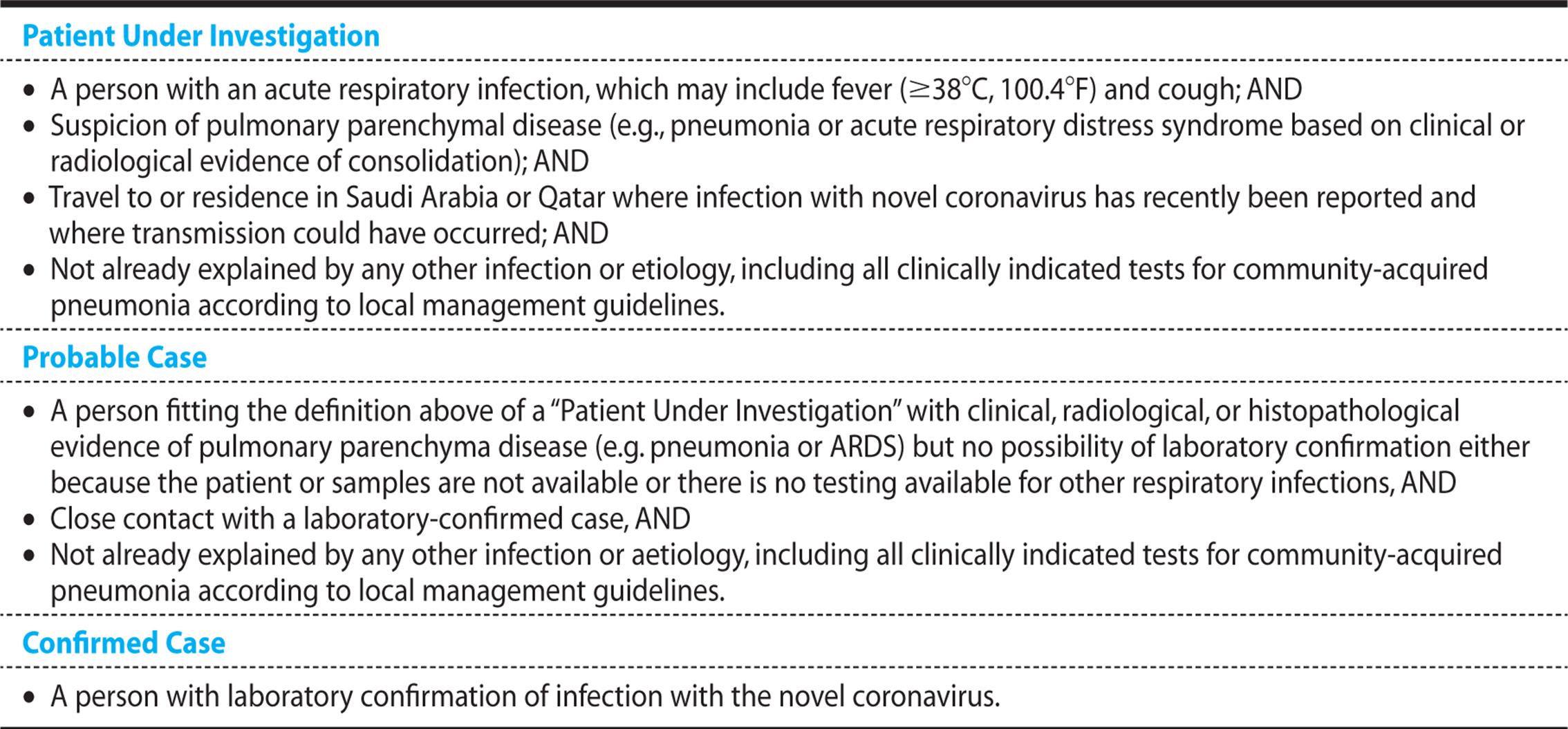
For epidemiologic purposes, the diagnosis must be made quickly based on clinical criteria. For this purpose, the CDC has created a series of case definitions (see Table 14.3).
Table 14.3. WHO Case Definitions for Severe Acute Respiratory Syndrome (SARS)
Real-time RT-PCR tests have been developed to rapidly and sensitively identify the SARS coronavirus in clinical samples. However, in the absence of ongoing worldwide SARS transmission, the probability that a positive test will be a false positive is high. Testing for the novel coronavirus identified in 2012 can also be performed by the CDC. In addition, sample collection technique is extremely important to maximize sensitivity and specificity. Therefore, testing should be ordered only after informed consent is obtained from the patient and preferably after consultation with state public health authorities and the CDC. A reliable ELISA has been developed to measure SARS antibody titers in patient serum. However, detectable antibody titers are generally not observed until the second week of the illness.
Treatment and Outcome
No specific treatment of SARS is available. At the present time, meticulous supportive care is all that medical science has to offer. A number of specific therapies have been attempted without clear benefit. Antibiotics may prevent bacterial superinfection and should be considered later in the disease course based on Gram stain findings (see Chapters 1 and 4). Oseltamivir, intravenous ribavirin, and combined ribavirin and corticosteroids have not been shown to be of benefit. Some patients have worsened as corticosteroids have been tapered.
In the 2003 outbreak, the overall fatality rate was 9.6% worldwide. A poorer prognosis was associated with older age: patients above the age of 60 years had a 43% mortality. A high serum LDH or high peripheral neutrophil count is also associated with a worse outcome.
Prevention
Given the unavailability of curative therapies, infection control practices are critical for preventing the spread of this deadly infection. All suspected cases must be placed in strict respiratory isolation. Hospitalized patients should be placed in negative pressure rooms. Respirator masks (N-95) should be worn in combination with gowns, gloves, and protective eyewear. Health care workers are at particularly high risk if present during intubation of an infected patient. In the Toronto outbreak, one case of SARS was mistakenly diagnosed as congestive heart failure, and respiratory precautions were not instituted.
KEY POINTS
About Severe Acute Respiratory Syndrome
1. Caused by a unique strain of coronavirus that is spread by aerosolized droplets and is excreted in stool.
2. Attacks mainly people over the age of 15 years. Most cases occur in people 25–70 years of age,
3. Incubation period is 2–14 days. Illness occurs in two stages:
a) Febrile prodrome
b) Respiratory phase with infiltrates and hypoxia
4. Diagnosis based on clinical criteria.
5. Only current treatment is meticulous supportive care.
6. Mortality is 9.6% overall, and 43% in people over 60 years of age.
7. Strict respiratory isolation and standard contact isolation are used to prevent transmission.
Possibly infected patients who do not require hospitalization should be instructed not leave home until they have been asymptomatic for 10 days. They should use separate utensils, towels, and sheets. Contacts may leave home as long as they are asymptomatic. Travel to areas where the WHO has determined the presence of multiple active cases of SARS should be avoided.
INFLUENZA
Virology and Epidemiology
Influenza virus is a major cause of morbidity and mortality worldwide. Influenza A and B both cause epidemic illnesses, and influenza A can cause pandemics such as the 1918–1919 pandemic in which at least 20 million people died (Some estimates suggest that the number may have even reached 100 million.). Influenza routinely causes epidemics every 1–3 years. The number of cases always increases in the winter months.
The influenza virus, an enveloped RNA virus, has eight gene segments that encode proteins. Two of these genes, the hemagglutinin (HA) and neuraminidase (NA) genes, are important mediators of pathogenicity and immunogenicity. Virus binding and infection requires HA, and virion release requires NA. The antibody responses to HA and NA are critical for protection against infection.
Influenza strain nomenclature consists of the type (A or B), the geographic source of the initial isolate, the isolate number, the year of isolation, and the HA and NA gene subtypes. Thus, a strain of influenza A virus that was isolated in Hong Kong in 1968 is designated A/Hong Kong/03/68[H3N2].
The influenza virus changes the structure of its HA and NA proteins by genetic mutation—a process known as antigenic drift. Antigenic drift produces variant strains against which human populations have less protective antibody. Occasionally, influenza A virus acquires a completely different set of antigens by a process known as antigenic shift. The unique strains produced by antigenic shift can infect large segments of the population, because cross-reactive or protective antibodies are lacking, thus leading to a pandemic. The virus is thought to undergo antigenic shift by reassortment (exchange of segments of genome with avian influenza species). The process of reassortment and production of virulent human influenza species may occur in pigs, which can be infected with human and avian species of influenza alike.
Influenza attack rates are highest in the very young, but the greatest morbidity and mortality are seen among elderly patients. Influenza is also particularly dangerous to people with underlying pulmonary disease or those who are immunocompromised. In the United States, influenza annually causes about 15 million excess cases of respiratory illnesses in young people and about 4 million cases in older adults. The virus is efficiently transmitted by aerosols of respiratory secretions generated by coughing, sneezing, and talking.
In 1997, direct transmission of avian influenza from birds to humans was documented in Hong Kong. Sporadic cases of bird-to-human transmission have been occurring since 2003, primarily in Southeast Asia. Although occasional human-to-human transmission has been reported, efficient spread of avian strains among humans has not yet occurred. Recent data derived from sequencing of isolates obtained from formalin-fixed, paraffin-embedded lung tissue from 1918 influenza cases and a frozen sample from a victim buried in permafrost since 1918 have shed light on the nature of the 1918 pandemic strain. The sequences suggest that the 1918 strain was derived from an avian strain by adaptation to a human host rather than by reassortment. Experiments in mice also suggest that the 1918 strain possesses strong and unique virulence determinants. These findings have raised the possibility that the H5N1 avian influenza strains sporadically infecting humans today could mutate to become more infectious and transmissible among humans while retaining a high level of lethality.
In 2009, a new strain of H1N1 influenza was first detected in humans in Mexico and rapidly spread to cause a pandemic with confirmed cases in over 75 countries. Fifty-nine million cases are estimated to have occurred in the United States by 2010, with 265,000 hospitalizations and 12,000 deaths. The novel strain, named swine-origin influenza virus (SOIV), arose from a reassortment between previously circulating swine influenza viruses and a Eurasian swine strain. Most cases occurred in children and younger adults, possibly reflecting a lack of immunity in the younger adults. Illness among hospitalized patients was relatively severe, with mortality ranging from 14% to 46%. Pregnant women and the immunosuppressed were particularly affected in the 2009 pandemic, comprising from 4% to 10% of hospitalizations and fatalities. Ninety percent of deaths occurred in those under 65 years of age.
KEY POINTS
About the Virology and Epidemiology of Influenza
1. Influenza is caused by an enveloped RNA virus that is classified by specific surface proteins:
a) Hemagglutinins (HAs)
b) Neuraminidases (NAs)
2. Influenza A and B both cause epidemics; influenza A also causes pandemics.
3. Epidemics occur every 1 to 3 years, mainly in the winter.
4. “Antigenic drift” refers to changes in HA and NA proteins resulting from genetic mutation.
5. “Antigenic shift” refers to reassortment (exchange of genomic segments with other virus strains).
a) Occurs in influenza A.
b) Produces pandemic-causing viral strains.
c) Reassortment may occur in pigs.
6. Virus is spread by aerosolized respiratory secretions.
7. In the United States, 15 million infections occur annually in young people and 4 million in older adults.
8. Avian influenza (“bird flu”) is a concern:
a) The 1918 pandemic strain may have evolved from an avian strain.
b) The H5N1 strain has recently caused human disease in Southeast Asia (direct spread from birds; human-to-human spread is minimal).
Pathophysiology and Clinical Manifestations
The onset of influenza is abrupt. The patient can often say exactly when they fell ill with fever, headache, shaking chills, and myalgias. The fever may be quite high. It remains elevated for at least 3 days and usually resolves within 1 week. Fever and systemic symptoms predominate in the clinical picture, but a dry cough is invariably present and usually persists after the fever is gone. Rhinorrhea, cervical adenopathy, and nonexudative pharyngitis are common. Recovery can be prolonged, taking up to 3 weeks or even longer; during this period, the patient experiences cough and persistent fatigue.
KEY POINTS
About the Pathogenesis and Clinical Manifestations of Influenza
1. Infects the respiratory epithelium, causing cell necrosis and acute inflammation.
2. Is characterized by abrupt onset of high fever, shaking chills, headache, myalgias, pharyngitis, and rhinorrhea.
3. Several complications are possible:
a) Viral pneumonia [can progress to fatal acute respiratory distress syndrome (ARDS) and pulmonary hemorrhage].
b) Superinfection with Staphylococcus aureus, Haemophilus influenzae, or Staphylococcus pneumoniae.
c) Reye syndrome (associated with use of aspirin).
4. Avian influenza attacks children.
a) Severe disease occurs in children more than 12 years of age.
b) Symptoms include diarrhea and severe cough, in addition to fever.
c) Lymphopenia occurs, with prominent infiltrates on chest X-ray.
d) Acute onset of ARDS that develops 6–29 days after onset of fever leads to 78% mortality.
e) Cases have been seen in Southeast Asia, the Middle East, Turkey, and Nigeria.
Once influenza virus infects the respiratory epithelium, it kills the host cell as it replicates. The virus multiplies rapidly, producing large numbers of infectious viruses in the respiratory secretions and causing diffuse inflammation and damage. In severe cases, extensive necrosis occurs. Pulmonary function is abnormal even in normal hosts and may remain abnormal for a period of weeks after recovery.
It has become recognized that influenza may also cause a milder febrile upper respiratory disease or even mild illness without fever. The extent to which influenza causes milder diseases is not well characterized, due to the likelihood that the majority of such cases are not reported.
Human cases of avian influenza differ from typical human influenza in several ways. Although experience with H5N1 avian influenza remains limited, the disease typically presents with fever, cough, and respiratory failure, often accompanied by diarrhea. Almost all cases report close contact with poultry, and the virus has predominantly infected children. Lymphopenia and abnormalities on chest X-ray are common. Mortality has been high among hospitalized cases, although the full clinical spectrum of infection is not well established. Unlike most previous influenza strains, H5N1 is particularly virulent in children over the age of 12 years with no underlying diseases (those that would be predicted to have a strong immune system). Within 6–29 days of the onset of fever, many of these patients develop a respiratory distress syndrome and die of respiratory failure. Of the 23 cases reported from Southeast Asia in 2004, 18 (78%) died. The initial cases were reported in China, Thailand, and Vietnam. Subsequently, cases were reported in Azerbaijan, Djibouti, Egypt, Indonesia, Iraq, Laos, Nigeria, and Turkey. The WHO is tracking new cases, and up-to-date information can be obtained by visiting http://www.who.int/csr/disease/avian_influenza/en/ (accessed January 15, 2013).
Clinical manifestations of the 2009 SOIV were generally similar to those of seasonal H1N1 influenza. Gastrointestinal symptoms may be more common than in typical seasonal influenza. The virus exhibits a greater propensity to replicate in lower respiratory epithelium, possibly explaining the high incidence of pneumonia that led to hospitalization during the initial pandemic.
Complications
The major complications of influenza are viral pneumonia and secondary bacterial pneumonia.
In influenza pneumonia, rapid progression to dyspnea and hypoxia occurs. The clinical and radiographic picture is that of acute respiratory distress syndrome (ARDS), and antibiotics are ineffective. Mortality in this situation is very high. The lungs are hemorrhagic, and there is diffuse involvement, but little inflammation. This complication was a major cause of death among young adults during the 1918 pandemic, but is rarely seen today. However, recent experience with avian influenza virus suggests that, if the H5N1 strain adapts to humans, the incidence of this complication could greatly increase.
In some cases of influenza pneumonia, patients initially appear to be recovering from the virus, but then suddenly relapse with fever and typical signs of bacterial pneumonia (see Chapter 4, case 4.1). As a consequence of damage to the tracheobronchial epithelial lining, secondary bacterial pneumonia develops, with Staphylococcus aureus, Haemophilus influenzae, and Streptococcus pneumoniae being the most common offenders (see Chapter 4).
As noted with varicella virus, use of aspirin during influenza has been associated with the development of Reye syndrome. Reye syndrome is characterized by fatty infiltration of the liver and changes in mental status, such as lethargy or even delirium and coma. No specific treatment of Reye syndrome is available other than correction of metabolic abnormalities and reduction in elevated intracranial pressure.
Diagnosis
The most useful characteristic distinguishing influenza from other respiratory illnesses is the predominance of the systemic symptoms. In addition, the epidemic nature of the disease in the community is helpful in making a diagnosis. When influenza is circulating in a community, an adult displaying the symptoms described earlier is highly likely to have influenza. Rapid influenza detection tests (RIDTs) are now available, and some can detect both the A and B types of influenza in throat and nasal swabs. However, the sensitivity of these tests is somewhat variable, depending on the source and quality of the specimen and on other factors, possibly being as low as 60%. Further, the likelihood of false positives is high when influenza incidence is low and, conversely, the likelihood of a false negative is high when influenza is circulating in the community. Therefore, treatment should not be withheld in cases consistent with influenza while awaiting the results of RIDT, nor solely on the basis of a negative RIDT. The CDC-recommended indications for further influenza testing by culture or RT-PCR are shown in Table 14.4.
Table 14.4. When to Consider Further Influenza Testing
Treatment
Amantadine and rimantadine inhibit influenza A virus infection by binding to a virus membrane protein. These drugs were long used for prevention and treatment of influenza A. However, influenza A is now widely resistant to both amantadine and rimantadine, and the U.S. Advisory Committee on Immunization Practices therefore recommends that amantadine and rimantadine not be used for the treatment or chemoprophylaxis of influenza A in the United States.
Two NA inhibitors, zanamivir and oseltamivir, are highly effective in inhibiting both type A and B influenza. Zanamivir has to be administered by inhalation; oseltamivir is given orally. Both agents can be used for prophylaxis and treatment, and they are most effective when administered soon after the onset of infection. Recently, rare but serious psychiatric and neurologic side effects have been associated with oseltamivir, particularly in pediatric patients. These side effects include panic attacks, delusions, delirium, convulsions, depression, loss of consciousness, and suicide.
Both oseltamivir and zanamivir are active against H5N1 avian influenza in animal and in vitro models. Resistance to oseltamivir has already been documented. Whether widespread resistance to oseltamivir will present a significant obstacle in the management of an avian influenza outbreak is unknown.
Resistance to oseltamivir mediated by a NA mutation has been documented in the 2009 H1N1 S-OIV, and has arisen during therapy in immunocompromised patients. Such strains have generally remained sensitive to zanamavir. Recently, however, multidrug resistant strains have been reported, complicating the choice of antiviral regimens. Infectious disease consultation is recommended for all severely ill influenza patients.
KEY POINTS
About the Diagnosis and Treatment of Influenza
1. Commercial immunodetection methods are available for early diagnosis; viral culture is confirmatory.
2. Treatment should not be withheld when clinically indicated based on the results of rapid diagnostic tests or while awaiting test results.
3. Amantadine and rimantadine should no longer be used because of widespread resistance.
4. Neuraminidase inhibitors zanamivir and oseltamivir are effective for types A and B influenza alike.
a) Give these agents early.
b) Resistance to oseltamivir has been reported for the H5N1 strain of avian influenza and the 2009 swine-origin pandemic strain.
c) Oseltamivir associated with neurologic and behavioral side effects, particularly in children.
Treatment should be started as rapidly as possible, although treatment is still beneficial when started more than 48 hours after onset of disease symptoms. Treatment is generally for 5 days, although it may be extended in cases of severe disease or in immunocompromised patients. Shedding may be prolonged in such patients although the significance of such shedding after clinical improvement is unknown. Doubling of the dose may be considered in severe cases of pneumonia and is generally well tolerated.
ECMO has been shown to improve survival in severely ill patients with H1N1 influenza during the 2009 outbreak.
Prevention
Influenza vaccine is a trivalent inactivated vaccine directed against types A and B influenza. The strains selected for each year’s vaccine are based on the strain that was circulating worldwide the previous year. The effectiveness of the vaccine depends to some degree on the success of the match between the vaccine and the circulating strains. Vaccination decreases both disease severity and the infection rate.
The groups that should be targeted for influenza vaccination include:
• All persons aged 6 months and older should be vaccinated annually.
• Protection of persons at higher risk of influenza-related complications should continue to be a focus of vaccination efforts as providers and programs transition to routine vaccination of all persons aged 6 months and older.
• When vaccine supply is limited, vaccination efforts should focus on delivering vaccination to persons who:
• are aged 6 months through 4 years (59 months);
• are aged 50 years and older;
• have chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, neurologic, hematologic, or metabolic disorders (including diabetes mellitus);
• are immunosuppressed (including immunosuppression caused by medications or by human immunodeficiency virus);
• are or will be pregnant during the influenza season;
• are aged 6 months through 18 years and receiving long-term aspirin therapy and who therefore might be at risk of experiencing Reye syndrome after influenza virus infection;
• are residents of nursing homes and other chronic-care facilities;
• are American Indians/Alaska Natives;
• are morbidly obese (body-mass index is 40 or greater);
• are health care personnel;
• are household contacts and caregivers of children aged younger than 5 years and adults aged 50 years and older, with particular emphasis on vaccinating contacts of children aged younger than 6 months.
A live attenuated influenza vaccine (LAIV) that is administered as a nasal spray is also available. This vaccine is approved for use in patients 2–49 years of age. The LAIV is considered equally efficacious as inactivated vaccine. Side effects are generally minor and consist mainly of cough and rhinorrhea, which may be more common in adults than children. An increased risk of respiratory side effects has been noted in younger children. Because of the potential risks of a live vaccine, LAIV should not be administered to immunocompromised patients. Because of the potential risk of shedding and transmission of LAIV, health care workers should avoid contact with severely immunocompromised patients for 7 days after vaccination. The “Populations That Should Not Be Vaccinated with Live Attenuated Influenza Vaccine” below shows a complete list of patients in whom LAIV is contraindicated.
Populations That Should Not Be Vaccinated with Live Attenuated Influenza Vaccine
• Children under the age of 2 years or adults over the age of 49 years.
• People with asthma, reactive airway disease, or other chronic disorders of the pulmonary or cardiovascular systems; people with other underlying medical conditions, including metabolic diseases such as diabetes, renal dysfunction, and hemoglobinopathies.
• People with known or suspected immunodeficiency diseases or who are receiving immunosuppressive therapies.
• People with a history of Guillain–Barré syndrome. Pregnant women.
• People with a history of hypersensitivity, including anaphylaxis, to any of the components of LAIV or to eggs.
• Children or adolescents receiving acetylsalicylic acid or other salicylates (because of the association of Reye syndrome with wild-type influenza virus infection).
• Persons who care for severely immunosuppressed persons because of the theoretical risk of transmission of live attenuated virus.
Because of the potential for a pandemic originating from avian influenza, extensive efforts to produce effective vaccines against currently circulating strains are underway. Unfortunately, the vaccines that have been produced to date have been poorly immunogenic, and may require multiple immunizations to achieve adequate protection. Research on various strategies to improve and expand on current methods is continuing. Possible strategies include alternative routes of administration, adjuvants, recombinant DNA vaccines, and passive immunization.
HERPES SIMPLEX VIRUS
Epidemiology
Herpes simplex virus (HSV) is a ubiquitous human pathogen with two distinct types: HSV-1 and HSV-2. The HSV-1 type causes primarily orolabial lesions; HSV-2 causes genital lesions. More than 90% of adults worldwide exhibit serologic evidence of infection with HSV-1. The prevalence of HSV-2 infection is considerably lower, but ranges from at least 10% to as high as 80% depending on the population studied. As sexual activity (number of sexual partners and other STDs) increases, the likelihood of HSV-2 infection also increases. Transmission of HSV usually occurs person to person, by direct contact with infected secretions or mucosal surfaces.
Pathophysiology and Clinical Manifestations
Once HSV enters a mucosal or skin surface, it replicates in the epithelium and infects a nerve ending. It is then transported to the nerve ganglion where it establishes a latent infection that persists for the lifetime of the host. The trigeminal and sacral ganglia are the most common sites of HSV-1 and HSV-2 latency. Viral replication occurs in the ganglion during the initial infection.
Initial infection with HSV-1 is often subclinical and many people never experience clinical reactivation, although they are clearly seropositive. Others experience gingivostomatitis (especially small children). The lesions are usually ulcerative and exudative, and may involve extensive areas of the lips, oral cavity, pharynx, and perioral skin. Healing occurs over a period of several days to 2 weeks, usually without scarring. Secondary episodes result in fever blisters—the typical vesicular and ulcerative lesions. These occur most commonly at the vermilion border of the lips, but may also occur at other sites on the face or in the mouth. Many environmental factors may trigger a recurrence, such as sunlight exposure, stress, and viral infections. Secondary episodes are usually much less severe.
KEY POINTS
About the Epidemiology, Pathogenesis, and Clinical Manifestations of Herpes
Simplex Virus
1. Type 1 (herpes simplex virus, HSV-1) causes herpes labialis; more than 90% of people worldwide have been infected.
2. Type 2 (HSV-2) causes genital herpes; incidence varies from 10% to 80%, depending on sexual history.
3. Transmitted from person to person by contact with infected surfaces or mucosa.
4. Viral replication occurs in nerve ganglia; virus periodically reactivates causing recurrent infection.
a) HSV-1 resides in the trigeminal ganglion.
b) HSV-2 resides in the sacral ganglion.
5. Lesions are vesiculopustular and moderately painful.
6. Less common forms of skin infection also occur:
a) Herpetic whitlow is usually found in health care workers; can be mistaken for a bacterial infection.
b) Herpes gladiatorum develops in wrestlers at sites of skin abrasion.
7. Complications can be serious:
a) Herpes encephalitis (HSV-1) can manifest with personality changes, obtundation, and seizures. Mortality is 15%.
b) Herpes keratitis is a leading cause of blindness.
c) Cutaneous dissemination can occur in eczema patients, and bronchopneumonia is a possibility in debilitated patients.
In both women and men, HSV-2 causes genital herpes. Lesions may be vesicular, pustular, or ulcerative, involving the penis in men and vagina and cervix in women. Typical symptoms are pain, itching, dysuria, and vaginal or urethral discharge. The symptoms of primary infection tend to be more severe in women. Primary infection can be associated with aseptic meningitis and mild systemic symptoms such as fever. Occasionally, inflammation is severe enough to lead to temporary bladder or bowel dysfunction.
Both HSV-1 and HSV-2 can also affect many other sites in the body where they have been inoculated. “Whitlow” is an HSV infection of the fingers, resulting from the inoculation of virus into abraded skin. This condition may be seen in health care workers and others who have been exposed to the virus either from autoinoculation or person-to-person transmission. The lesions are vesicular and pustular, with local erythema, pain, and drainage. They are often mistaken for bacterial infections, resulting in unnecessary drainage and antibiotics. “Herpes gladiatorum” is the name given to HSV infection acquired by wrestlers, in whom the virus is inoculated into breaks in the skin during wrestling competition.
Complications
A potentially dangerous consequence of HSV infection of the cornea is HSV keratitis. This infection may be caused by either HSV-1 or HSV-2, but more commonly by HSV-1. Once HSV keratitis has occurred, the patient remains at risk of recurrences. This infection is one of the most common causes of blindness in the United States. Symptoms consist of tearing, pain, erythema, and conjunctival swelling. Dendritic corneal lesions are easily visualized by fluorescein staining (see Chapter 5, Figure 5.1). Involvement of deeper structures or corneal scarring can lead to blindness.
Annually, HSV encephalitis occurs in approximately 1 in 250,000 to 500,000 of the population. A preponderance of these cases is attributable to HSV-1; concurrent skin lesions are usually not present. Although HSV encephalitis may be the result of primary infection, most patients can be shown to have been previously infected. The disease is characterized by fever, altered mentation, and focal neurologic signs. Personality changes and bizarre behavior are common, and many patients experience seizures. The disease process typically affects the temporal lobe and is usually unilateral. It may progress in a fulminant manner with frank hemorrhagic necrosis of the affected areas of the brain. With antiviral treatment, mortality has been reduced, but remains above 15%, and most survivors exhibit long-term cognitive impairment.
Widespread cutaneous dissemination (eczema herpeticum) can be seen in people with eczema. Visceral dissemination of HSV is rare in the normal host, but herpetic tracheobronchitis is often seen in debilitated, intubated hospitalized patients, in whom it may occasionally progress to pneumonitis.
Diagnosis
The clinical diagnosis of labial or genital herpes is usually not difficult; however, the typical vesicle on an erythematous base, the “dewdrop on a rose petal,” is not always present. Culture of vesicle fluid is highly sensitive and specific. Direct staining for HSV antigens can also be used to diagnose infection.
Staining of lesion scrapings and examination for giant cells (the Tzanck test) is quick, but nonspecific and insensitive. The diagnosis of HSV encephalitis can be difficult, especially early in the course of the illness. A mild lymphocytic CSF pleocytosis is common, as are red blood cells and an elevated protein level. However, none of these findings are diagnostic. A PCR test of the CSF for HSV is highly sensitive and specific—the optimal laboratory test to confirm the diagnosis. Magnetic resonance imaging of the brain and electroencephalography often show abnormalities localizing to the temporal areas even early in the disease.
Treatment
First episodes of all types of HSV infection benefit from treatment. For both orolabial and genital herpes, oral acyclovir, famciclovir, and valacyclovir are all effective. Treatment of recurrent episodes of HSV-1 or HSV-2 is somewhat unsatisfactory. Although treatment may somewhat reduce duration of symptoms, especially in HSV-2, the results are not dramatic. Some patients find that early institution of therapy (as soon as prodromal symptoms such as tingling or itching appear) can be helpful. For patients with frequent and severe recurrent genital herpes, suppressive therapy can be helpful. Any of the three antivirals mentioned earlier can be used. For HSV encephalitis, treat every 8 hours with intravenous acyclovir 10 mg/kg, for a minimum of 14 days. Disseminated HSV infection, particularly in the immunosuppressed host, usually requires high-dose intravenous acyclovir therapy.
KEY POINTS
About the Diagnosis and Treatment of Herpes Simplex Virus
1. The diagnosis is made clinically, or with immunofluorescence and viral culture. For encephalitis, a polymerase chain reaction test of the cerebrospinal fluid is useful.
2. Primary skin infections can be treated with acyclovir, famciclovir, or valacyclovir.
3. Treatment of recurrent episodes is more controversial. Treat during the prodrome; suppressive therapy can be used for recurrent genital herpes.
4. Use high-dose, intravenous acyclovir for encephalitis or disseminated disease.
CYTOMEGALOVIRUS
Epidemiology
Human cytomegalovirus (CMV) is a common infection worldwide. Prevalence of the infection varies greatly based on socioeconomic factors, but no clear link to hygienic practices exists. In the United States, about 40–80% children are infected by puberty. Young children may be a major source of infection for adults; caretakers of young children may have a risk of infection that is 20 times normal. Person-to-person spread can occur by contact with almost any human body fluid or substance: blood, urine, saliva, cervical secretions, feces, breast milk, and semen. The virus is therefore also spread by sexual contact and by blood transfusion and organ donation.
Pathophysiology and Clinical Manifestations
Most human CMV infections are thought to be subclinical, but primary infection in the normal host occasionally results in a mononucleosis syndrome. Approximately 10–20% of mononucleosis cases are caused by CMV, which is the major cause of heterophil (Monospot)-negative mononucleosis. Mononucleosis caused by CMV is more common in slightly older adults, but it can be difficult to distinguish clinically from EBV-associated mononucleosis. Pharyngitis and cervical adenopathy have been suggested to be less common, but both may be observed with CMV mononucleosis. Fever in CMV mononucleosis lasts on average for more than 3 weeks. Mild liver enzyme abnormalitites are common, although severe hepatitis and jaundice are rare. Rash is present in about 30% of patients, and ampicillin provocation of rash has been noted. Other complications of CMV infection in the normal host include hepatitis, pneumo-nitis, and Guillain–Barré syndrome. Many of the laboratory findings of EBV mononucleosis are also seen in CMV infection. Symptoms may persist for as long as 32 weeks in some patients with a remitting and relapsing course. CMV infection acquired by blood transfusion may result in a systemic syndrome characterized by persistent fever and malaise.
CMV infection of the immunocompromised host produces most of the morbidity and mortality associated with the virus. Infection may produce severe disease in any of multiple organs, causing retinitis, hepatitis, pneumonitis, gastrointestinal disease (gastric and esophageal ulcers and colitis), meningoencephalitis, or polyradiculopathy. Further details of preventive strategies in these patients are discussed in Chapter 15. However, these manifestations may be present during primary infection of normal hosts as well. CMV infection may result in Guillain–Barré syndrome. In one prospective study of Guillain–Barré syndrome, 12% of patients had symptoms following laboratory-confirmed CMV infection.
KEY POINTS
About Cytomegalovirus Infection
1. Infection with cytomegalovirus (CMV) is common worldwide. In the united States. 40–80% of children are positive.
2. Young children are the primary source of infection for adults.
3. The virus is transmitted by blood, urine, saliva, cervical secretions, semen, feces, and breast milk.
4. Many infections are subclinical, and CMV is a leading cause of heterophil-negative mononucleosis.
5. In the immunocompromised host, the virus causes retinitis, hepatitis, pneumonitis, gastrointestinal disease (gastric and esophageal ulcers and colitis), and polyradiculopathy.
6. The diagnosis can be made by noting a rise in immunoglobulin G titer (to four times normal levels), or quantitative PCR.
7. The disease is self-limiting in the normal host. The immunocompromised patient should be treated with ganciclovir or foscarnet.
Intrauterine CMV infection of the fetus is a major cause of congenital malformations and adverse sequelae. Primary infection of the seronegative mother is most commonly associated with congenital disease and symptoms. Approximately half of such infections are estimated to lead to intrauterine fetal infection and the risk is highest earlier in pregnancy. Severe CMV disease in the neonate is associated with jaundice, petechiae, and visceral involvement. CNS findings are often prominent and include microcephaly, chorioretinitis, and cerebral calcifications. A syndrome of lethargy and seizures may occur at birth. Immediate perinatal death may occur, and survivors have significant incidence of neurologic sequelae, microcephaly, and mental retardation. Although infection after birth is not associated with such severe manifestations, subtle defects in cognitive development and deafness have been associated with perinatal CMV infection.
CMV infection has been epidemiologically linked to a higher incidence of cardiovascular disease and pathology. CMV may infect endothelial cells and incite an inflammatory response. Whether CMV plays a causative role in cardiovascular disease remains a matter of controversy and ongoing research.
Diagnosis
Viral culture is not useful for diagnosing CMV infection in the normal host. Virus may be shed for long periods in the urine and intermittently by persons infected in the past. The most reliable test is a rise in CMV IgG titer to four times baseline value. Detection of IgM antibody to CMV is also strong evidence for acute infection, although IgM can occasionally be seen in normal hosts during virus reactivation. Quantitative PCR of viral DNA is also widely available. Diagnosis of the various manifestations of CMV disease in the immunocompromised host is discussed in Chapter 15.
Prevention and Treatment
Antiviral treatment of CMV infection is almost never required in the normal host. Spontaneous resolution, even after a lengthy illness, is almost invariable. However, corticosteroids may be used for the same autoimmune or hematologic complications as are seen in EBV infection. Treatment with ganciclovir or foscarnet may be considered in those rare cases in which CMV appears to be causing specific organ-system disease (such as esophagitis) in the normal host. Valganciclovir is orally bioavailable form of ganciclovir. These agents are primarily used in the immunocompromised patient (see Chapter 15). A liposomal form of cidofovir has shown promise of strong antiviral activity and minimal renal toxicity in research trials.
The rise of resistance to ganciclovir and foscarnet is a serious problem in transplant patients and others who may require prolonged or repeated therapy. Ganciclovir resistance arises mainly from mutations in the viral kinase encoded by UL97. Resistance may also be due to mutations in the CMV DNA polymerase. Foscarnet resistance may also arise from mutations in the polymerase gene, although these are generally sensitive to ganciclovir.
Although a vaccine is not currently licensed for use, recent trials with a viral glycoprotein in seronegative pregnant women demonstrated 50% efficacy in preventing CMV infection.
FURTHER READING
Varicella Virus
Heininger U, Seward JF. Varicella. Lancet. 2006;368:1365-1376.
Jumaan AO, Yu O, Jackson LA, Bohlke K, Galil K, Seward JF. Incidence of herpes zoster, before and after varicella-vaccination-associated decreases in the incidence of varicella, 1992-2002. J Infect Dis. 2005;191:2002–2007.
Marin, M., J. X. Zhang, J. F. Seward. Near elimination of varicella deaths in the US after implementation of the vaccination program. Pediatrics. 2011;128:214-220.
Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352:2271-2284.
Shafran SD, Tyring SK, Ashton R, et al. Once, twice, or three times daily famciclovir compared with aciclovir for the oral treatment of herpes zoster in immunocompetent adults: a randomized, multicenter, double-blind clinical trial. J Clin Virol. 2004;29:248-253.
Smallpox
Casey CG, Iskander JK, Roper MH, et al. Adverse events associated with smallpox vaccination in the United States, January–October 2003.JAMA. 2005;294:2734-2743.
Hammarlund E, Lewis MW, Hansen SG, et al. Duration of antiviral immunity after smallpox vaccination. Nat Med. 2003;9:1131-1137.
Hammarlund E, Lewis MW, Hanifin JM, Mori M, Koudelka CW Slifka MK. Antiviral immunity following smallpox virus infection: a case-control study. J Virol. 2010;84:12754-12760.
Moore ZS, Seward JF, Lane JM. Smallpox. Lancet. 2006;367:425-435.
Reeves PM, Bommarius B, Lebeis S, et al. Disabling poxvirus pathogenesis by inhibition of Abl-family tyrosine kinases. Nat Med. 2005;11:731-739.
Smee DF, Bailey KW, Wong MH, Wandersee MK, Sidwell RW. Topical cidofovir is more effective than is parenteral therapy for treatment of progressive vaccinia in immunocompromised mice. J Infect Dis. 2004;190:1132-1139.
Talbot TR, Stapleton JT, Brady RC, et al. Vaccination success rate and reaction profile with diluted and undiluted smallpox vaccine: a randomized controlled trial. JAMA. 2004;292:1205-1212.
Yang H, Kim SK, Kim M, et al. Antiviral chemotherapy facilitates control of poxvirus infections through inhibition of cellular signal transduction. J Clin Invest. 2005;115:379-387.
Epstein–Barr Virus
Candy B, Hotopf M. Steroids for symptom control in infectious mononucleosis. Cochrane Database Syst Rev. 2006;3:CD004402.
Cohen JI, Jaffe ES, Dale JK, et al. Characterization and treatment of chronic active Epstein–Barr virus disease: a 28-year experience in the United States. Blood. 2011;117(22):5835-5849.
Crawford DH, Macsween KF, Higgins CD, et al. A cohort study among university students: identification of risk factors for Epstein–Barr virus seroconversion and infectious mononucleosis.Clin Infect Dis. 2006;43:276-282.
Fafi-Kremer S, Morand P, Brion JP, et al. Long-term shedding of infectious Epstein–Barr virus after infectious mononucleosis. J Infect Dis. 2005;191:985-989.
Odumade, O. A., K. A. Hogquist, et al. Progress and problems in understanding and managing primary Epstein–Barr virus infections. Clin Microbiol Rev. 2011;24(1):193-209.
Petersen I, Thomas JM, Hamilton WT, White PD. Risk and predictors of fatigue after infectious mononucleosis in a large primary-care cohort. QJM. 2006;99:49-55.
Swaminathan S, Wang F. Antimicrobial therapy of Epstein–Barr virus infections. In: Yu V, Merigan TC, Barriere S, et al., eds. Antimicrobial Therapy and Vaccines. Baltimore, MD: Williams & Wilkins; 2002. [For current update, visit http://www.antimicrobe.org/v02rev.asp]
Waninger KN, Harcke HT. Determination of safe return to play for athletes recovering from infectious mononucleosis: a review of the literature. Clin J Sport Med. 2005;15:410-416.
Hanta Virus
Duchin JS, Koster FT, Peters CJ, et al. Hantavirus pulmonary syndrome: a clinical description of 17 patients with a newly recognized disease. N Engl J Med. 1994;330:949-955.
Jenison S, Hjelle B, Simpson S, Hallin G, Feddersen R, Koster F. Hantavirus pulmonary syndrome: clinical, diagnostic, and virologic aspects. Semin Respir Infect. 1995;10:259-269.
Nichol ST, Spiropoulou CF, Morzunov S, et al. Genetic identification of a hantavirus associated with an outbreak of acute respiratory illness. Science. 1993;262:914-917.
Severe Acute Respiratory Syndrome
Donnelly CA, Fisher MC, Fraser C, et al. Epidemiological and genetic analysis of severe acute respiratory syndrome. Lancet Infect Dis. 2004;4:672-683.
Huang J, Ma R, Wu CY. Immunization with SARS-CoV S DNA vaccine generates memory CD4+ and CD8+ T cell immune responses. Vaccine. 2006;24:4905-4913.
Lau SK, Woo PC, Li KS, et al. Severe acute respiratory syndrome coronavirus-like virus in Chinese horseshoe bats. Proc Natl Acad Sci U S A. 2005;102:14040-14045.
Peiris JS, Guan Y, Yuen KY. Severe acute respiratory syndrome. Nat Med. 2004;10:S88-S97.
Influenza
Kandun IN, Wibisono H, Sedyaningsih ER, et al. Three Indonesian clusters of H5N1 virus infection in 2005. N Engl J Med. 2006;355:2186-2194.
Monto AS. The threat of an avian influenza pandemic. N Engl J Med. 2005;352:323-325.
Shinya K, Ebina M, Yamada S, Ono M, Kasai N, Kawaoka Y. Avian flu: influenza virus receptors in the human airway. Nature. 2006;440:435-436.
Taubenberger JK, Reid AH, Lourens RM, Wang R, Jin G, Fanning TG. Characterization of the 1918 influenza virus polymerase genes. Nature. 2005;437:889-893.
Tumpey TM, Basler CF, Aguilar PV, et al. Characterization of the reconstructed 1918 Spanish influenza pandemic virus. Science. 2005;310:77-80.
Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic (H1N1) 2009 Influenza. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Eng J Med. 2010;362(18):1708-1719.
Zimmer SM, Burke DS. Historical perspective, emergence of influenza A (H1N1) viruses. New Engl J Med. 2009;361(3):279-285.
Cytomegalovirus
Gandhi MK, Khanna R. Human cytomegalovirus: clinical aspects, immune regulation, and emerging treatments. Lancet Infect Dis. 2004;4:725-738.
Pass RF, Zhang C, Evans A, et al. Vaccine prevention of maternal cytomegalovirus infection. N Engl J Med. 2009;360(12):1191-1199.
Razonable RR, Brown RA, Wilson J, et al. The clinical use of various blood compartments for cytomegalovirus (CMV) DNA quantitation in transplant recipients with CMV disease. Transplantation. 2002;73:968-973.
Smieja M, Gnarpe J, Lonn E, et al. Multiple infections and subsequent cardiovascular events in the Heart Outcomes Prevention Evaluation (HOPE) Study. Circulation. 2003;18(107):251-257. Staras SA, Dollard SC, Radford KW, Flanders WD, Pass RF, Cannon MJ. Seroprevalence of cytomegalovirus infection in the United
States, 1988-1994. Clin Infect Dis. 2006;43:1143-1151.
Wreghitt TG, Teare EL, Sule O, Devi R, Rice P, et al. Cytomegalovirus infection in immunocompetent patients. Clin Infect Dis. 2003;37(12):1603-1606.