Douglas L. McGee
Disorders of the penis, including balanoposthitis, phimosis, paraphimosis, and priapism, require expeditious evaluation and treatment.
BALANITIS, PHIMOSIS, AND PARAPHIMOSIS
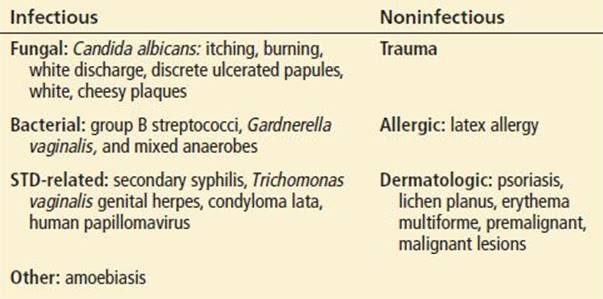
Balanitis (inflammation of the glans penis) and posthitis (inflammation of the prepuce of the penis) usually occur together, and are referred to as balanoposthitis when they do. Balanitis is more common in uncircumcised men who exercise poor hygiene, but also affects young boys. Patients with balanoposthitis have an edematous, erythematous, fissured, and painful prepuce and glans. A variety of skin changes are possible, depending on the etiology (Table 122.1).
TABLE 122.1
Causes of Balanoposthitis
When the foreskin is not retractable behind the glans penis, the condition is termed phimosis. Physiologic phimosis is present until normal adhesions between the foreskin and glans have separated. Although most young boys are able to retract the foreskin by puberty, retraction is usually possible at an earlier age (1). As normal secretions accumulate and epithelial sloughing occurs, smegma is normally formed and assists in the separation of the foreskin from the glans. Parents may confuse smegma with infectious discharge if expressed from the penis. Pathologic phimosis, or simply phimosis, occurs when retraction of the foreskin is not possible after puberty or when the foreskin was previously retractable. When balanoposthitis is severe, phimosis may occur and precipitate urinary retention.
Paraphimosis occurs when the retracted foreskin is not replaced, usually after cleansing or catheter insertion. After foreskin retraction, the constricting phimotic ring causes progressive edema and impairs venous return, threatening the viability of the glans. Although most patients complain of pain and usually provide a history of foreskin retraction, debilitated uncircumcised patients may not provide this history. History of circumcision may be available from medical records or from a caregiver. Do not confuse paraphimosis with balanitis in these patients.
ED EVALUATION
The emergency department (ED) evaluation for patients with balanoposthitis, phimosis, or paraphimosis is usually limited to the history and physical examination. Measure the patient’s blood glucose when there is infection with Candida albicans, and perform serologic testing if secondary syphilis is suspected. Acetic acid whitens the superficial epithelial skin layer when applied to lesions infected with human papillomavirus (HPV). Determine if the patient can urinate when severe phimosis or paraphimosis is diagnosed.
ED MANAGEMENT
The mainstay of ED management of balanoposthitis includes meticulous hygiene, including retraction of the foreskin and cleansing of the glans penis and prepuce, but the aggressive use of soap to clean under the prepuce is not advisable. Treatment of infectious balanoposthitis is directed against the offending organism. Fungal infections of the glans are treated with topical antifungal agents, and metronidazole is appropriate for Gardnerella sp, anaerobic infection, and Trichomonas sp. Secondary syphilis, if suspected, is treated according to established guidelines.
Asymptomatic phimosis does not require emergent treatment. Reassure concerned parents when physiologic phimosis is present, and discourage forceful retraction. Several studies demonstrate that medium- or high-potency topical steroids applied to the foreskin for 4 to 6 weeks are 85% to 90% effective when retraction is desired (2,3). However, several studies comparing steroid cream with placebo moisturizing showed resolution of phimosis in slightly more than half of the placebo group (4,5). When severe phimosis causes urinary retention or interferes with placement of a urinary catheter, a slit made in the dorsal aspect of the foreskin facilitates access to the urethral meatus (6). After providing local anesthesia of the penis with a dorsal nerve block or ring block placed at the base of the penis, gently separate adhesions between the foreskin and glans with a hemostat. Place one jaw of the hemostat inside the dorsal foreskin, taking care not to include the urethral meatus or glans. Close the hemostat to crush the foreskin for 3 to 5 minutes then incise the crushed area with straight scissors. The crushed edges rarely bleed but may require absorbable suture for hemostasis if they separate. Although some patients are satisfied with the cosmetic appearance of the foreskin after the dorsal-slit procedure, a urologist may perform an elective circumcision at a later date. Always return the foreskin to the reduced position after urinary-catheter placement.
Paraphimosis requires emergent treatment. After adequate sedation or penile anesthesia, attempt manual reduction. A simple initial approach to paraphimosis is to wrap the edematous prepuce with an elastic bandage to provide gentle, nontraumatic compression that slowly forces edematous fluid under the phimotic ring (7). Self-adhering bandages facilitate continuous compression. Wrap the phallus, starting at the glans with 3 to 4 wraps of compression bandage and leave in place for 20 minutes. Marked reduction in edema has resulted in autoreduction or may facilitate other methods of manual reduction if paraphimosis persists after compression. Place the fingers of both hands distal to the phimotic ring and foreskin and apply gentle, steady pressure on the glans with the thumbs (6). Gauze placed under the fingers may improve traction on the foreskin while bringing it over the glans, but lubricants are rarely helpful. Several other techniques are described to treat paraphimosis; application of these techniques are guided by the physician’s skill and training in the maneuvers. A 21-gauge needle may be used to puncture the edematous foreskin. Manual compression after puncture may allow the escape of enough edema fluid to facilitate reduction (7,8). Repeated punctures or blood aspirated from the engorged glans after a tourniquet is placed at the base of the penis may also allow reduction (9,10). Subdermal hyaluronidase (1 mL) injected into the edematous foreskin facilitates dispersion of edema fluid and may make reduction possible (11). Some recommend the application of granulated sugar to the edematous glans and foreskin to extract tissue water, reduce edema, and ease reduction (12). Gauze soaked in 20% mannitol wrapped around the edematous prepuce for 30 to 45 minutes may also facilitate reduction (13). When less aggressive methods fail, incise the phimotic ring to facilitate foreskin reduction (6).
CRITICAL INTERVENTIONS
• Return the foreskin after urinary catheter insertion in uncircumcised males.
• Paraphimosis is a urologic emergency that must be relieved in the ED.
DISPOSITION
Most patients with balanoposthitis may be treated as outpatients. Some diabetics may require inpatient treatment if the infection is severe and the diabetes is poorly controlled.
When phimosis is present and causes urinary retention, consider urologic consultation to relieve phimosis and allow free drainage of urine if a urinary catheter cannot be placed.
Emergent urology consultation is necessary if paraphimosis cannot be successfully relieved in the ED. Patients in whom paraphimosis has been successfully relieved require follow-up with their primary physician and may benefit from future circumcision.
Refer patients with skin lesions suspicious for precancerous changes or malignancy to a dermatologist for further evaluation.
Common Pitfalls
• Phimosis is normal in young boys and does not require treatment in asymptomatic adults.
• Paraphimosis, a urologic emergency, can be confused with balanitis unless it is recognized that the foreskin is retracted.
• Always return the foreskin its anatomic location after retraction.
PRIAPISM
Priapism is characterized by a prolonged, painful, unwanted penile erection, usually in the absence of sexual stimulation. The physiologic balance achieved between venous outflow and arterial dilatation of the corpora cavernosa controls erectile function. Priapism occurs when normal physiologic blood flow is altered disrupting this balance. Medications used to treat erectile dysfunction in men (sildenafil, papaverine, prostaglandin E1, etc.) are responsible for most cases of priapism (12). It is uncommon in boys, unless sickle cell disease is present, and it is rare in neonates (14). Henoch–Schönlein purpura is described as another cause of priapism (15). Patients with priapism complain of penile pain and persistent erection, even after ejaculation. The mean time to presentation in one series of 34 patients was 30 hours (16).
Priapism may be divided into “low-flow” and “high-flow” types (16). Low-flow priapism results from abnormal venous outflow, whereas high-flow priapism results from abnormally increased arterial inflow. Low-flow priapism is more common and is often caused by vasoactive drugs that cause engorgement of the corpora cavernosa. Impaired venous outflow causes sludging, thrombosis, acidosis, ischemia, and decreased oxygen tension within the corporal bodies. This pathophysiologic cascade causes the irreversible cellular damage and corporal fibrosis responsible for the long-term complications of low-flow priapism. Oral and intracavernosal agents used for erectile dysfunction, antihypertensive agents, psychotropic drugs, cocaine, and ethanol are among the drugs that have been implicated. Leukemia, sickle cell anemia, and a variety of neoplastic etiologies are also responsible for low-flow priapism (16). High-flow priapism is uncommon and usually results from trauma to the penis or perineum (17). Arterial fistula formation between the cavernosal artery and the corporal bodies increases arterial flow into the penis that exceeds venous outflow.
ED EVALUATION
The etiology of priapism can usually be ascertained with careful questioning. Determine the onset of erection and history of prior episodes of priapism. Pay careful attention to prescription or illicit drug use to help determine whether these agents are responsible. Sickle cell disease may be causative in patients at risk or known to have this disease. The penis is erect and painful to palpation. The corpora cavernosa is engorged and tender to palpation, but in contrast to normal erections, the corpus spongiosum (erectile tissue surrounds the urethra) and glans penis are usually flaccid.
Some authors recommend blood-gas analysis of blood aspirated from the corporal bodies to assist in differentiating between low- and high-flow states (16,17). Low pH, low oxygen tension, and high carbon dioxide levels suggest low-flow priapism, caused by venous obstruction. Blood-gas parameters similar to arterial blood suggest high-flow priapism, a condition usually seen after trauma. Because nearly all cases of priapism are low flow, and trauma is usually associated with high-flow priapism, differentiating between the two is not difficult in most cases, making blood gas analysis unnecessary. Doppler flow ultrasonography of the penis and perineum can be used to document arteriovenous fistulas when high-flow priapism is suspected (17). However, treatment of low-flow priapism should not be delayed pending ultrasonography.
ED MANAGEMENT
The ED management of priapism includes both pharmacologic and mechanical treatment options. Untreated ischemic priapism may result in permanent erectile dysfunction. Consider analgesia and sedation to facilitate detumescence. There is conflicting literature describing the efficacy of terbutaline in priapism. Some small clinical trials demonstrate that oral terbutaline is more effective than placebo in achieving detumescence (18), but others have found no benefit (19). Because of its relative safety in patients without hypertension or coronary artery disease, a trial of subcutaneous terbutaline (0.25 to 0.5 mL injected subcutaneously, repeated in 20 minutes if needed) or oral terbutaline (5 mg repeated in 15 minutes) may be attempted (17).
When sedation, analgesia, or terbutaline do not result in detumescence, corporal aspiration and irrigation is indicated (16,17). The penis is anesthetized, and 30 to 60 mL of blood is aspirated from a single corporal body at the 10 o’clock or 2 o’clock position after puncture with an 18- to 20-gauge needle; anastomoses between the corporal bodies obviate the need for bilateral aspiration. Do not puncture the glans. If the erection persists after aspiration, phenylephrine is carefully injected into the punctured corpus cavernosum. One milligram of phenylephrine is diluted in 9 mL of sterile saline to achieve a concentration of 100 μg/mL, and 100 to 200 μg aliquots of phenylephrine are injected up to three times to achieve detumescence. Monitor blood pressure and cardiac rhythm when repeated injections are required.
Sickle cell patients with priapism require analgesia, hydration, and supplemental oxygen but are also treated with the methods described above. Red blood cell exchange transfusion has been employed when traditional antisickling measures fail, but there is no evidence to support its efficacy (20,21). Emergent ED therapy is not required for high-flow priapism because it does not cause the ischemic injury seen in low-flow priapism.
CRITICAL INTERVENTIONS
• Treat patients with low-flow priapism with terbutaline, corporal aspiration, and/or phenylephrine injection.
• Priapism is a urologic emergency that requires ED treatment in coordination with the consulting urologist.
DISPOSITION
Patients with priapism may be discharged home to follow-up with an urologist after detumescence is accomplished in the ED. When ED treatment fails to relieve the erection or when high-flow priapism is suspected, urgent urologic evaluation is necessary.
Common Pitfalls
• Failure to obtain an adequate history to determine the etiology of priapism.
• Failure to achieve detumescence of priapism prior to discharge.
REFERENCES
1. Shahid SK. Phimosis in children. ISRN Urol. 2012;2012:707329.
2. Ghysel C, VanderEeckt K, Bogaert GA. Long-term efficacy of skin stretching and a topical corticoid cream application for unretractable foreskin and phimosis in prepubertal boys. Urol Int. 2009;82:81–88.
3. Zavras N, Christianakis E, Mpourikas D, et al. Conservative treatment of phimosis with fluticasone proprionate 0.05%: A clinical study in 1185 boys. J Pediatr Urol. 2009;5:181–185.
4. Pileggi FD, Vicente Y. Phimotic ring topical corticoid (0.1% mometasone furoate) treatment in children. J Pediatr Surg. 2007;42:1749–1752.
5. Zampieri N, Corroppolo M, Zuin V, et al. Phimosis and topical steroid: New clinical findings. Pediatr Surg Int. 2007;23:331–335.
6. Davis JE, Silverman MA. Urologic Procedures. In: Roberts JR, Custalow CB, Thomson TW, eds. Clinical Procedures in Emergency Medicine, 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:117–1129.
7. Pohlman GD, Phillips JM, Wilcox DT. Simple method of paraphimosis reduction revisited: Point of technique and review of the literature. J Pediatr Urol. 2013;9:104–107.
8. Barone JG, Fleisher MH. Treatment of paraphimosis using the “puncture” technique. Pediatr Emerg Care. 1993;9:298–299.
9. Kumar V, Javle P. Modified puncture technique for reduction of paraphimosis. Ann R Coll Surg Engl. 2001;83:126–127.
10. Raveenthiran V. Reduction of paraphimosis: A technique based on pathophysiology. Br J Surg. 1996;83:1247.
11. DeVries CR, Miller AK, Packer MG. Reduction of paraphimosis with hyaluronidase. Urology. 1996;48:464–465.
12. Kerwat AS, Shandall A, Stephenson B. Reduction of paraphimosis using granulated sugar. Br J Urol. 1998;82:755.
13. Anand A, Kapoor S. Mannitol for paraphimosis reduction. Urol Int. 2013;90:106–108.
14. Walker JR, Casale AJ. Prolonged penile erection in the newborn. Urology. 1997;50:796–799.
15. Lind J, Mackay A, Withers SJ. Henoch-Schönlein purpura and priapism. J Pediatr Child Health. 2002;38:526–527.
16. Harmon WJ, Nehra A. Priapism: Diagnosis and management. Mayo Clin Proc. 1997;72:350–355.
17. Tay YK, Spernat D, Rzetelski-West K, et al. Acute management of priapism in men. BJU Int. 1012;109(suppl. 3):15–21.
18. Low FC, Jarow JP. Placebo-controlled study of oral terbutaline and pseudoephedrine in management of prostaglandin E1-induced prolonged erections. Urology. 1993;42:51–53.
19. Govier FE, Jonsson E, Kramer-Levien D. Oral terbutaline for the treatment of priapism. J Urol. 1994;151:878–879.
20. Merritt AL, Haiman C, Henderson SO. Myth: Blood transfusion is effective for sickle cell anemia-associated priapism. CJEM. 2006;8:119–123.
21. Rogers ZR. Priapism in sickle cell disease. Hematol Oncol Cln North Am. 2005;19:917–928.