David N. Zull
Anaphylaxis is an acute, life-threatening condition; immediate recognition and treatment are critical. Manifestations may range from minor symptoms such as rash or lip swelling to sudden death from upper airway obstruction or shock. Even the patient who presents with urticaria alone can subsequently develop hypotension, bronchospasm, or laryngeal edema and should thus be treated with the same urgency as the patient with the full-blown anaphylactic syndrome.
The constellation of anaphylactic symptoms results from massive release of chemical mediators from mast cells and basophils throughout the body. For anaphylaxis to occur there must have been previous sensitization to a foreign substance, against which immunoglobulin E (IgE) was made by antibody-producing B lymphocytes. IgE binds to mast cells and basophils. On re-exposure to the foreign substance, antigen binds to the IgE on mast cells, which triggers massive release of chemical mediators from these cells. Anaphylaxis may also occur by mechanisms independent of IgE (formerly referred to as anaphylactoid reactions), including direct stimulation of mast cells and basophils or via activation of the complement cascade or the coagulation system (1–3).
Mediators released from activated mast cells include histamine, leukotrienes, prostaglandins, platelet-activating factor, tryptase, and cytokines. These mediators lead to an abrupt increase in vascular permeability and vasodilation, thereby resulting in hypotension, urticaria, and angioedema of the skin, upper airway, and gastrointestinal tract. Leukotrienes are potent bronchoconstrictors as well. In life-threatening anaphylaxis, concomitant activation of complement, coagulation pathways, and the kallikrein–kinin system may contribute as well (2,3).
It is estimated that 1% to 3% of the population are at risk for anaphylaxis during their lifetime and that 1% of these episodes will be fatal, resulting in 1,000 to 1,500 anaphylactic deaths per year in the United States (4). Penicillin is the most feared cause of anaphylaxis, accounting for up to 75% of fatal drug reactions. More than 5% of the population report sensitivity to penicillin, yet more than 90% of these patients are skin-test negative and will not react. Penicillin allergy is generally manifested by urticaria alone or a delayed maculopapular drug eruption, but an estimated 25 of 100,000 patients treated with penicillin experience an anaphylactic reaction, and one will die. There is cross-reactivity among all penicillin derivatives including amoxicillin, dicloxacillin, piperacillin, and ampicillin. First- and second-generation cephalosporins demonstrate cross-reactivity in 2% to 3% of penicillin-allergic patients (documented by a positive penicillin skin test). Patients with reported penicillin allergy who are skin-test negative have less than a 1% cross-reaction rate.
Reactions to third- and fourth-generation cephalosporins appear negligible but these agents should still be used with caution if there is a history of life-threatening anaphylaxis. The cephalosporin-allergic patient will react to other cephalosporins and the penicillins, ampicillin and amoxicillin. Penicillin- and cephalosporin-allergic patients do not react to the monobactam, aztreonam, except for those allergic to ceftazidine. The safety of imipenem in the penicillin-allergic patient parallels the penicillin–cephalosporin risk profile, while the risk with meropenem and ertapenem is negligible (5,6).
Systemic allergic reactions to Hymenoptera stings are estimated to occur in about 1% of children and 3% of adults, and they account for approximately 40 to 100 anaphylactic deaths per year in the United States (7,8). Although 90% of stings are in children, 90% of fatalities to hymenoptera stings occur in adults, as children often manifest urticaria alone, adults present with hypotension or syncope. In emergency department (ED) series of anaphylaxis, hymenoptera stings comprise 18% to 29% of cases (1,9–11). Yellow jackets, and to a lesser extent hornets, account for the majority of stings in the United States, especially in the late summer during dry spells. Honeybees are also a common culprit, with the Africanized form in the southern United States noteworthy for its aggressive pursuit and swarming behavior. Wasps, fire ants, harvester ants, and bumblebees are other stinging hymenoptera. Depending upon the severity of a systemic reaction, patients have a 15% to 75% risk of future reactions. In contrast, patients with large local reactions (>10 cm) are very low risk for systemic reactions on re-exposure. Secondary infection of hymenoptera stings is unusual, except when fire ant pseudopustules are unroofed. Kissing bugs in the Southwest are the most common nonhymenoptera insect whose bite can cause anaphylaxis. Bites and stings of other insects have been reported rarely to cause anaphylaxis; they include the horsefly, deerfly, blackfly, mosquito, caterpillar, centipede, and bedbug (7,8).
The administration of iodinated contrast media results in minor reactions like a transient rash in up to 2% of patients, but may exceed 4% in atopic or asthmatic patients and 7% in those with a history of prior contrast reactions. Anaphylaxis occurs in about 0.5% of IV iodinated contrast administrations, with 0.01% to 0.04% being life threatening. Contrast media reactions result from non-IgE mechanisms like direct mast cell degranulation or complement activation; thereby prior exposure is not required. Contrary to popular belief, there is no cross-reactivity in patients allergic to fish, shellfish, or topical iodine. There is no cross-reactivity of iodinated contrast with gadolinium, which has a reaction rate of less than 0.1% (12).
Foods are an increasingly recognized cause of fatal or near-fatal anaphylaxis and are the most common cause of anaphylaxis in outpatients, accounting for one-third of cases overall and for more than one-half of episodes in children. Peanuts, tree nuts, shellfish, milk, eggs, and wheat are most commonly implicated, but the latter three are limited to infants and toddlers. Shellfish predominates in adults, whereas nuts are the most common cause in older children. Peanuts and tree nuts account for more than 90% of fatalities (about 150 deaths per year in the United States), with highly allergic individuals reacting to the mere touch or smell of the food. Food-induced anaphylaxis manifests primarily with airway obstruction and rarely with hypotension. Gastrointestinal involvement is much more common in food reactions (40%) compared to other causes of anaphylaxis (4%) (13,14). Noteworthy is the presentation of anaphylaxis and abdominal pain subsequent to the ingestion of sushi, attributed to allergy to the Anisakis worm that may parasitize raw fish. Exercise and medications (NSAIDs) appear to have a facilitating effect in some food reactions (15). Oral allergy syndrome occurs in patients with a history of tree and weed pollen allergy in which there is sudden burning in the mouth and throat after ingestion of fresh fruit, nuts, or vegetables, followed by mild angioedema and sometimes modest systemic allergic symptoms.
NSAIDs are the most common medications causing anaphylaxis in the outpatient setting, often unrecognized due to their frequent use and over-the-counter availability (16). NSAIDs may also precipitate asthma exacerbations in over 5% of asthmatics and in the majority of patients with asthma and nasal polyps. NSAIDs also cause flares in patients with chronic urticaria and may facilitate anaphylaxis to other allergens.. Aspirin and all NSAIDs should be assumed to cross-react unless the patient has a clear history of tolerance to other NSAIDs; more than half of reactions are to a single NSAID. If an NSAID is required, COX-2 inhibitors (celecoxib, meloxicam) and nonacetylated salicylates (salsalate, diflunisal) can be used safely. For analgesia, acetaminophen in doses no more than 650 mg is the safest option (17).
Various parenteral therapeutic agents have been associated with anaphylaxis. After repeated administration, monoclonal antibodies like infliximab, or chemotherapeutic agents like platinum compounds, taxanes, and L-aspariginase, can result in acute allergic reactions (18). About 5% of patients administered alteplase (tPA) for ischemic stroke develop orolingual angioedema without other manifestations of anaphylaxis (19).
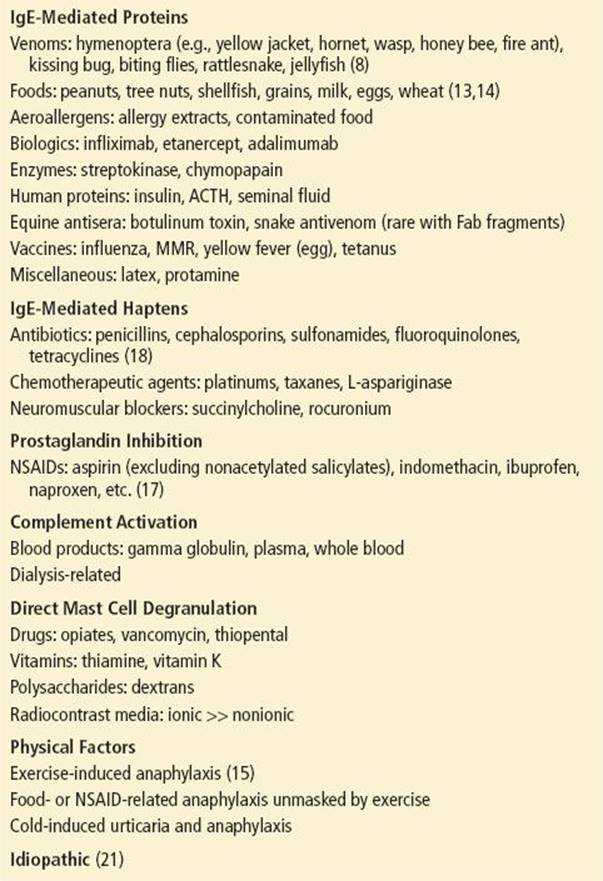
Exercise-induced anaphylaxis is usually associated with prior food or drug (NSAID) ingestion, but it can occur independently as well. Episodes are more common and severe during weather temperature extremes, after alcohol, and during prolonged exertion, yet many patients find that there is no reproducible pattern and most patients have exercised for years before experiencing their first episode. Wheat is the most commonly implicated food, followed by shellfish, fruits, and vegetables (15). Cold exposure itself can precipitate urticaria and sometimes anaphylaxis in patients who have cold urticaria, an inherited disorder. Perioperative anaphylaxis is usually related to paralytic agents or latex and is manifested by circulatory collapse with a paucity of skin findings. Exposure to human proteins such as blood products, insulin, or seminal fluid may rarely result in anaphylaxis. Many agents have a histamine-releasing effect, resulting in diffuse flushing but rarely anaphylaxis; these include opiates, thiamine, vitamin K, and vancomycin (20). Idiopathic anaphylaxis accounts for up to one-third of cases in various series and is notable for rapid-onset and recurrent, unpredictable episodes, often requiring chronic antihistamines and steroids to achieve remission Table 175.1 (21) summarizes etiologic factors in anaphylaxis.
TABLE 175.1
Etiologic Agents in Anaphylaxis
Repeated intermittent exposure to a substance or drug increases the risk of sensitization; the more direct the route to the systemic circulation, the greater the likelihood and severity of a reaction. The possible routes of exposure in descending order of severity are intravenous, intramuscular, subcutaneous, intradermal, inhalational, oral, other mucous membranes, and topical.
Symptoms of anaphylaxis usually begin <30 minutes after exposure and are often immediate. Antigens given orally may have a 2-hour delay before symptoms occur. In general, the more immediate the reaction, the more life-threatening it is. Symptoms may last only a few minutes, even without therapy but, on average, persist for 2 to 4 hours, with the exception of angioedema, which often persists beyond 24 hours. About 5% of patients with anaphylaxis experience a biphasic course, with recurrent anaphylaxis within 8 hours, despite earlier resolution. Delays in or inadequate use of epinephrine and steroids are often implicated in the recrudescence of symptoms (22).
CLINICAL PRESENTATION
Anaphylaxis is often heralded by premonitory symptoms (Table 175.2). Pruritus of the palms and soles, tingling about the mouth and tongue, generalized warmth, tightness in the chest, and a lump in the throat are commonly described. Dizziness or syncope secondary to hypotension may be presenting manifestations of anaphylaxis in the absence of any other signs or symptoms of allergic reaction.
TABLE 175.2
Symptoms and Signs of Anaphylaxis

More than 90% of patients have urticaria or angioedema. Urticaria (edema of the upper dermis) appears as raised erythematous wheals in evanescent pruritic patches. Angioedema represents edema of the deep dermis and appears as puffy, nonpitting areas of skin or mucous membrane. Angioedema is generally painless and nonpruritic; patients note only tingling and swelling in the affected areas. It tends to be most prominent about the face and lips and less so on the hands and arms.
Laryngeal edema resulting in acute upper airway obstruction is the principal cause of death from anaphylaxis. The onset can be dramatic and may be mistaken for a sudden cardiac death or acute upper airway obstruction from a foreign body. Angioedema of the lips, uvula, tongue, and oropharynx is less likely to obstruct the airway but must be treated aggressively because of the likelihood of concomitant edema of the larynx. Uvular edema, in particular, is a helpful marker for potential laryngeal involvement. Frequently, however, the patient complains of hoarseness and a lump in the throat, and the examination of the oropharynx is completely normal. Indirect laryngoscopy may reveal supraglottic or laryngeal edema, but this examination should not delay the prompt administration of epinephrine in a patient with these complaints.
Bronchospasm is common in the anaphylactic syndrome, but it tends to be mild unless the patient has a pre-existing history of asthma. Pulmonary edema, although reported in anaphylaxis, is generally considered a rare terminal event and not part of the syndrome.
Refractory hypotension is second only to laryngeal edema as a cause of death from anaphylaxis. A drop in blood pressure of 20 to 30 mm Hg is typical, but there is great variability. When sudden in onset, syncope or sudden death may occur.
Although it is usually overshadowed by other symptoms, abdominal cramping can occur in anaphylaxis, most notably in food-related episodes. Angioedema of the gut lining causes this colic as well as vomiting, diarrhea and, rarely, hematochezia. Rhinitis, nasal obstruction, chemosis, and conjunctivitis are other common manifestations of mucous membrane involvement, but they are not life threatening Acute coronary syndrome, takotsubo cardiomyopathy, and ventricular tachycardia have been reported, and nonspecific ST-T wave changes are commonly seen on the electrocardiogram in patients suffering from anaphylaxis. These cardiac manifestations are generally attributed to hypotension, hypoxia, and overzealous epinephrine therapy, although histamine and cytokines may induce coronary vasospasm and cardiac dysrhythmias (20).
Unique manifestations of anaphylaxis may be seen in specific patient subgroups. In pregnancy, vulvar and vaginal itching, low back pain, uterine cramping and preterm labor are described (23). In infants, neurologic presentations may predominate, with irritability, persistent crying, and somnolence (1,24,25).
DIFFERENTIAL DIAGNOSIS
The diagnosis of anaphylaxis is often obvious when antigen exposure is rapidly followed by urticaria, angioedema, bronchospasm, upper airway edema, and hypotension. Confusion in the diagnosis may occur when a delay in the development of symptoms obscures a cause-and-effect relation or when the syndrome is only partially expressed. Differentiating acute, severe urticaria, for example, from anaphylaxis is a moot point. The greatest confusion may arise when anaphylaxis presents as isolated hypotension; it should, therefore, be considered in the differential diagnosis of syncope and vascular collapse.
The acute development of isolated angioedema of the skin and upper airway is a common presentation of anaphylaxis, but it may also be due to hereditary angioedema (HA). This rare, autosomal dominant disease is characterized by the absence of a functional C1 inhibitor, allowing free activation of the complement cascade. HA is characterized by repeated episodes of angioedema of the skin (hands, feet, genitalia), upper airway, and gut. Episodes generally date from adolescence, clustering in the 11- to 45-year age range (26,27).
Attacks of HA may be precipitated by minor trauma, stress, and medications (estrogens, angiotensin-converting enzyme inhibitors [ACEIs]), but most occur without an external trigger. Vomiting and severe colicky abdominal pain is common and can mimic an acute abdomen or progress to small bowel obstruction from mucosal edema. Both urticaria and hypotension are absent in HA. Laryngeal edema can cause acute airway obstruction and death, but usually the progression is gradual, peaking in 8 hours. Typically, the edema will plateau for 24 hours, followed by gradual resolution over the next 2 days A reduction in the C4 level during an attack is diagnostic. Although it is routine to administer epinephrine, antihistamines, and steroids to patients with anaphylactic angioedema, these are generally ineffective in the hereditary disorder. C1 inhibitor concentrate is the most effective treatment in HA patients with airway compromise, providing relief of symptoms within 30 to 60 minutes. Fresh frozen plasma is an effective substitute, and it does not appear to exacerbate symptoms as was once suspected. Icatibant, a bradykinin receptor antagonist, or ecallantide, a kallikrein inhibitor, administered subcutaneously has shown efficacy as well (26,27).
Rapid development of edema of the upper airway may also result from viral or bacterial infection. However, pain, fever, and findings of erythema and exudate are not present in anaphylaxis. Airway compromise may occur in Stevens–Johnson syndrome and toxic epidermal necrolysis, but mucosal sloughing and bleeding distinguish them from anaphylaxis.
ACEIs produce cough in 10% to 20% of patients and life-threatening tongue and palatal angioedema in 0.1% to 0.7%. African Americans account for 70% to 90% of cases, with smoking, increasing age, and female gender further increasing the risk. Although the appearance is indistinguishable from anaphylactic swelling, the development is more gradual, and other features of anaphylaxis are absent. Patients may have been taking ACEIs for up to 10 years before an initial episode; the mean is 2 years, and about one-fourth of episodes occur within the first month of treatment. Angiotensin receptor blockers may be substituted for ACEIs, but similar angioedema has been described. ACEI-associated angioedema may be resistant to standard therapy but responds to fresh frozen plasma and bradykinin–kallikrein antagonists similar to HA (28,29).
Rarely, patients may experience stridor and obstructive airway symptoms secondary to vocal cord dysfunction or as a manifestation of hysteria; indirect laryngoscopy is the only means to verify these suspicions.
Scombroid fish poisoning may mimic anaphylaxis, presenting with acute urticaria, flushing, peppery taste in the mouth, vomiting, diarrhea, abdominal cramps, headache, and dysphagia. This syndrome occurs shortly after eating fish with a high histidine content (such as tuna or mahi-mahi) for which there has been a breach in the refrigeration process sometime between the catch and consumption, leading to bacterial breakdown of histidine to histamine. A clustering of cases of apparent anaphylaxis is often the clue to this entity (30).
Transient flushing seen in monosodium glutamate reactions may be confused with anaphylaxis, but the prominence of headache and numbness or tingling distinguishes it from an allergic reaction.
Systemic mastocytosis and the carcinoid syndrome may present with intense flushing and hypotension, mimicking anaphylaxis; prominent gastrointestinal symptoms, hepatomegaly, and provocation by alcohol help distinguish these entities. There has been increased recognition of mastocytosis in patients with idiopathic anaphylaxis. An elevated tryptase level between attacks is suggestive (21).
The systemic capillary leak syndrome is a rare disorder characterized by life-threatening episodes of hypovolemic shock, often accompanied by truncal and extremity swelling. Transient polycythemia and hypoalbuminemia during attacks are pathognomonic; the presence of a monoclonal gammopathy may provide a clue to the diagnosis between attacks.
Laboratory confirmation of anaphylaxis is problematic and rarely required. Plasma histamine rises transiently but normalizes within 60 minutes from onset. Serum tryptase peaks at 60 to 90 minutes from onset and may remain elevated for up to 5 hours, but it is less sensitive.
ED EVALUATION AND MANAGEMENT
Evaluation of the upper airway and careful blood pressure monitoring are the immediate priorities in the care of the patient with possible anaphylaxis. Angioedema of the lips, tongue, uvula, and soft palate, as well as symptoms of hoarseness, stridor, dysphagia, or lump in the throat should alert the physician to progressive airway compromise. Such patients are treated immediately with epinephrine 0.3 to 0.5 mL (1:1,000 dilution) IM (0.01 mL/kg in children to a maximum of 0.3 mL). For both children and adults, the IM route is preferred, as it has been demonstrated to have a faster onset and significantly higher blood levels than the subcutaneous route. The lateral thigh is the preferred injection site, demonstrating superior bioavailability compared to the deltoid region. The dose can be repeated at 5- to 15-minute intervals, to a maximum of 1 mg of epinephrine. β-adrenergic stimulation promotes the synthesis of cyclic AMP in mast cells, which blocks further release of chemical mediators. Epinephrine also exerts a therapeutic benefit by its α-adrenergic effect, causing vasoconstriction, which results in an improvement in blood pressure and a decrease in swelling of edematous tissues (2,3).
The patient is placed on a cardiac monitor and given oxygen by cannula, and an intravenous line of normal saline is established. If hypotension is present, saline should be infused wide open until the blood pressure responds (typically 1 to 2 L in an adult or 1 or 2 20-mL/kg boluses in a child). If hypotension persists or is profound from the outset, or if airway obstruction appears imminent, intravenous epinephrine may be administered. The most common error made in this situation is to give too much epinephrine too fast, precipitating cardiac dysrhythmias or chest pain. An aggressive approach would include the administration of 1 mL of 1:10,000 epinephrine diluted in 10 mL of normal saline and given as a slow IV push over 3 to 5 minutes (20 to 33 μg/min to 100 μg total). If life-threatening symptoms persist, this bolus can be repeated (31). A more conservative consensus approach recommends the preparation of a drip consisting of 1 mL (1 mg) of a 1:1,000 dilution of epinephrine in 250 mL of D5W infused at 1 to 10 μg/min (0.014 to 0.14 μg/kg/min) If cardiac arrest occurs in anaphylaxis, the epinephrine protocols above are not adequate treatment, and the dose should be escalated to 1 to 3 mg over 3 minutes (2,3).
Massive angioedema may preclude orotracheal intubation, such that cricothyroidotomy may have to be performed. Aerosolized epinephrine (racemic 2.25% solution, 0.5 mL in 3.5 mL saline; or levo-epinephrine 1:1,000, 5 mL) may decrease supraglottic and laryngeal edema, buying time while preparations are made to establish an airway and parenteral epinephrine can be administered. In addition, heliox decreases airflow resistance and improves ventilation in upper airway obstruction, providing a very valuable temporizing measure. If IV access is unavailable, sublingual or intraosseous injection or endotracheal administration of epinephrine is considered. If improvement in blood pressure and airway obstruction are incomplete, epinephrine can be continued 0.3 mL IM at 20-minute intervals or by an epinephrine drip (1 to 10 μg/min).
Hypotension generally responds to one or two IM doses of epinephrine and rapid saline infusion. It is important that the hypotensive patient be kept supine or in Trendelenburg position if the airway is not compromised, as they are exquisitely sensitive to preload, and assumption of an upright posture can lead to a precipitous drop in cardiac output and subsequent arrest, referred to as the empty heart syndrome. If hypotension persists, virtually all patients will respond to IV epinephrine. Patients who are refractory to IV epinephrine may respond to methylene blue, an inhibitor of nitric oxide production, given as an IV bolus of 1.5 to 2 mg/kg (32). Most patients with anaphylaxis do not require such intensive therapy, however. In general, one or two doses of epinephrine subcutaneously at 15- to 20-minute intervals and 1 L of saline IV are adequate. Patients with acute, severe urticaria alone may benefit from a single dose of epinephrine, yet it is usually not necessary because there is no life threat. Bronchospasm in anaphylaxis is responsive to epinephrine alone, but in patients with pre-existing asthma, repeated albuterol nebulizations may be necessary (2,3).
Corticosteroids are recommended in all patients with anaphylaxis. Although there is no immediate benefit to their administration, steroids speed the resolution of angioedema and urticaria and are thought to prevent a biphasic course in anaphylaxis (22). Dosage recommendations are similar to those for status asthmaticus: methylprednisolone (Solu-Medrol), 125-mg intravenous push, followed by 60 mg every 4 to 6 hours in patients whose symptoms persist despite standard therapy. Milder episodes are often treated with oral prednisone 40 to 60 mg initially.
Steroids have an important role in prophylaxis of anaphylaxis in patients allergic to iodinated radiocontrast material requiring IV contrast. The most common regimen is prednisone 40 mg orally at 13, 6, and 1 hour prior to administration of contrast (2,3). Although strong clinical evidence is lacking, consensus opinion suggests that all patients with anaphylaxis should receive an antihistamine such as diphenhydramine (Benadryl), 25 to 50 mg, to a maximum of 100 mg if needed. The route of administration depends on the severity of the reaction. Although less effective for pruritus, H2 blockers (famotidine 20 mg or ranitidine 50 mg IV push) appear equivalent to H1 blockers in urticaria and anaphylaxis, and they may offer an advantage if sedation and anticholinergic side-effects are undesirable. The combination of H1- and H2 blockers are superior to either agent alone, especially in severe anaphylaxis (33). The addition of fexofenadine (Allegra) or cetirizine (Zyrtec) orally allows more complete histamine blockade without associated sedation or anticholinergic effects and is safe when added to traditional antihistamines. Antihistamines should not be relied upon as the sole treatment in anaphylaxis, except perhaps in the most mild, self-limited of cases.
Preventing further exposure to the antigen is critical; for instance, a tourniquet can be placed above an injection site, the stinger of a honey bee can be removed, offending chemicals can be washed off, and even charcoal can be considered.
Throughout therapy, the vital signs are reassessed frequently, and the airway is checked for edema of the uvula or oropharynx. The patient is asked about symptoms of laryngeal edema or bronchospasm and examined for signs of stridor, retractions, or wheezing. These assessments are made at 1- or 2-minute intervals at first, with the intervals lengthened as the patient stabilizes.
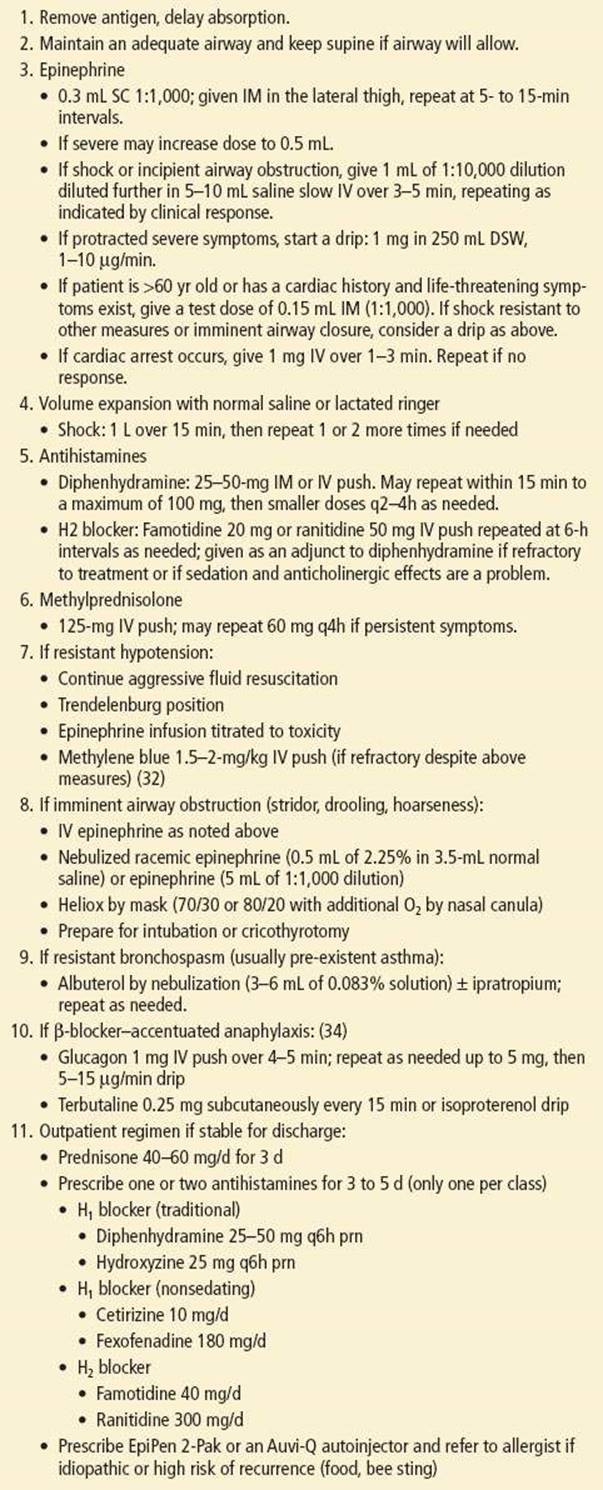
For patients older than age 60 or those with a cardiac history, saline is given cautiously for hypotension while monitoring closely for volume overload. Epinephrine should not be withheld in patients with potential upper airway obstruction or in those with hypotension unresponsive to volume loading. A test dose of epinephrine, 0.15 mL (1:1,000) IM can generally be given safely. If no chest pain or cardiac dysrhythmias develop, another test dose or a full dose is then given. IV epinephrine should be avoided in these patients unless death appears imminent without its use, but limiting the infusion to 1 to 4 μg/min. Pre-existing medications which the patient is taking may aggravate an episode of anaphylaxis or make the patient unresponsive to therapy. Most noteworthy is the patient on a β-adrenergic blocker, which may exacerbate bronchospasm as well as limit the efficacy of epinephrine, leading to a net α-adrenergic effect. In this situation, glucagon, 1 to 2 mg given IV over 5 minutes may be of great benefit, repeating the dose up to 5 mg total if needed, followed by an infusion of 5 to 15 μg/min titrated to response (18). Terbutaline, 0.25 mg subcutaneously, may also be considered. ACEIs have also been reported to aggravate hypotension and angioedema in anaphylaxis, necessitating more aggressive management Table 175.3 (2,34) summarizes treatment guidelines for anaphylaxis.
TABLE 175.3
Treatment of Anaphylaxis
Fatalities in anaphylaxis may occur in up to 2% of cases. Foods are generally responsible in children to young adults, while medications and venoms are the etiology in older adults. Risk factors for fatality in anaphylaxis include asthma, delay in administration of epinephrine, cardiopulmonary disease, upright posture maintained during the attack, systemic mastocytosis, and other atopic diseases (4,11).
CRITICAL INTERVENTIONS
• Administer epinephrine intramuscularly immediately for patients presenting with hypotension or acute angioedema of the lips, tongue, uvula, and soft palate.
• Administer epinephrine slow IV push or via infusion pump if there is imminent airway compromise, profound hypotension, or progression of symptoms despite IM epinephrine.
• In addition to IV epinephrine, treat supraglottic and laryngeal edema with aerosolized epinephrine while preparing to establish an airway.
• Hypotension should be treated with aggressive fluid resuscitation as well as maintaining the patient supine or in Tredelenburg position to enhance preload.
• Administer corticosteroids and antihistamines (H1 and H2) to all patients with anaphylaxis.
DISPOSITION
If all symptoms of anaphylaxis resolve rapidly and completely with initial therapy, the patient can be observed in the ED without further treatment. If symptoms do not recur in the next 2 to 4 hours, the patient may safely be discharged and should continue on a 3-day course of prednisone (40 mg/d) or a single dose of dexamethasone (10 to 20 mg) and a long acting antihistamine, such as fexofenadine (180 mg/d), cetirizine (10 mg/d), or famotidine (40 mg/d), saving diphenhydramine 25 mg as rescue therapy for pruritis or rash. An epinephrine autoinjector, such as EpiPen or Auvi-Q) should be prescribed for patients with food-related, Hymenoptera, and idiopathic anaphylaxis. Both the EpiPen 2-Pak and the Auvi-Q contain two doses of epinephrine as well as a training device. Discharge instructions should caution the patient to avoid any suspected inciting cause such as medications, foods, chemicals, or even exercise. The patient should be instructed to return to the ED immediately if hoarseness, dysphagia, wheezing, dyspnea, dizziness, or worsening rash with swelling develops. Follow-up with an allergist should be recommended, particularly if no obvious etiology has been identified in the ED or if desensitization is indicated.
Patients who had a life-threatening manifestation on presentation (shock or upper airway obstruction), even if it resolved with acute therapy, should be admitted. Those who had a slow or incomplete response to therapy or any worsening of symptoms during ED evaluation and treatment also require admission, as do elderly or debilitated patients or those with serious underlying cardiac disease. If hypotension or significant airway compromise persists, admission to an ICU is mandatory. For most of the remaining patients, a 12- to 24-hour observation period is indicated (10).
Because anaphylaxis can progress in such a fulminant manner, transfer to another institution is not recommended unless prolonged observation in the ED has shown the patient to be stable.
Common Pitfalls
• Giving epinephrine undiluted and too rapidly when intravenous administration is required (31).
• Withholding epinephrine therapy in the elderly or cardiac patient with imminent airway obstruction or refractory shock.
• Not recognizing the possibility of recrudescence of symptoms 4 to 8 hours after an initial complete response to therapy (22).
• Not identifying common etiologies of anaphylaxis, including over-the-counter NSAIDs, foods (shellfish, nuts), antibiotics (despite the lack of previous reactions and regardless of duration of therapy), antihypertensive drugs (β-blockers, ACEIs), and exercise.
• Not treating upper airway symptoms such as hoarseness, foreign body sensation, and dysphagia, with prompt administration of IM epinephrine.
• Not recognizing uvular and pharyngeal angioedema as warning signs of laryngeal involvement.
• Relying solely on epinephrine, antihistamines, and steroids in patients suspected of having HA or ACEI angioedema, and not considering the use of fresh frozen plasma, icatibant, ecallantide, or C1 inhibitor concentrate.
• Failing to recognize that anaphylaxis can present with shock or acute airway obstruction alone, without any other manifestations of the classic anaphylactic syndrome.
• Failing to prescribe EpiPen or Auvi-Q and to provide allergy referral to patients with idiopathic anaphylaxis and those at high risk for recurrent episodes.
REFERENCES
1. Fuzak JK, Trainor J. Comparison of the incidence, etiology, and management of anaphylaxis over time. Pediatr Emer Care. 2013;28:131–135.
2. Rutkowski K, Dua S, Nasser S. Anaphylaxis: Current state of knowledge for the modern physician. Postgrad Med J. 2012;88:458–464.
3. Simons FE. Anaphylaxis. J Allergy Clin Immunol. 2010;125:S161–S181.
4. Nowak R, Farrar JR, Brenner BE, et al. Customizing anaphylaxis guidelines for emergency medicine. J Emerg Med. 2013;45:299–306.doi: 10.1016/j.jemermed.
2013.01.018.
5. Campagna JD, Bond MC, Schabelman E, et al. The use of cephalosporins in penicillin-allergic patients: A literature review. J Emerg Med. 2012;42(5):612–620.
6. Solensky R. Allergy to β-Lactam antibiotics. J Allergy Clin Immunol. 2012;130(6):1442–1442.e5.
7. Pesek RD, Lockey RF. Management of insect sting hypersensitivity: An update. Allergy Asthma Immunol Res. 2013;5(3):129–137.
8. Shaker MS, Hsu D, Gruenberg DA. An update on venom allergy. Curr Opin Pediatr. 2013;25:1–6.
9. Brown AF, McKinnon D, Chu K. Emergency department anaphylaxis: A review of 142 patients in a single year. J Allerg Clin Immunol. 2001;108:861–866.
10. Gaeta TJ, Clark S, Pelletier AJ, et al. National study of US emergency department visits for acute allergic reactions, 1993 to 2004. Ann Allerg Asthma Immunol. 2007;98:360–365.
11. Webb LM, Lieberman P. Anaphylaxis: A review of 601 cases. Ann Allerg Asthma Immunol. 2006;97:39–43.
12. Brockow K, Ring J. Anaphylaxis to radiographic contrast media. Curr Opin Allergy Clin Immunol. 2011;11:326–331.
13. Cianferoni A, Muraro A. Food-induced anaphylaxis. Immunol Allergy Clin North Am. 2012;32(1):165–195.
14. Perry TT, Pesek RD. Clinical manifestations of food allergy. Pediatr Ann. 2013;42(6):96–101.
15. Jaqua NT, Peterson MR, Davis KL. Exercise-induced anaphylaxis: A case report and review of the diagnosis and treatment of a rare but potentially life-threatening syndrome. Case Rep Med.2013;2013:610726.
16. Gelincik A, Demirturk M, Yilmaz E, et al. Anaphylaxis in a tertiary adult allergy clinic: A retrospective review of 516 patients. Ann Allergy Asthma Immunol. 2013;110:96–100.
17. Chaudhry T, Hissaria P, Wiese M, et al. Oral drug challenges in non-steroidal anti-inflammatory drug-induced urticarial, angioedema, and anaphylaxis. Intern Med J. 2011;42(6):665–671.
18. Joerger M. Prevention and handling of acute allergic and infusion reactions in oncology. Annals Oncology. 2012;23(suppl 10):313–319.
19. Gorski EM, Schmidt MJ. Orolingual angioedema with alteplase administration for treatment of acute ischemic stroke. J Emerg Med. 2013;45(1):25–26.
20. Khoueiry G, Abi Rafeh N, Azab B, et al. Reverse Takotsubo cardiomyopathy in the setting of anaphylaxis treated with high-dose intravenous epinephrine. J Emerg Med. 2013;44(1);96–99.
21. Blatman KH, Ditto AM. Idiopathic anaphylaxis. Allergy Asthma Proc. 2012;33(suppl 1):S84–S87.
22. Tole JW, Lieberman P. Biphasic anaphylaxis: Review of incidence, clinical predictors, and observation recommendations. Immunol Allergy Clin North Am. 2007;27:309–326.
23. Simons FE, Schatz M. Anaphylaxis during pregnancy. J Allergy Clin Immunol. 2012;130:597–606.
24. Chipps BE. Update in pediatric anaphylaxis: A systematic review. Clin Pediatr. 2013;52(5):451–461.
25. Vezir E, Erkocoglu M, Kaya A, et al. Characteristics of anaphylaxis in children referred to a tertiary care center. Allergy Asthma Proc. 2013;34(3):239–246.
26. Bork K. Current management options for hereditary angioedema. Curr Allergy Asthma Proc. 2012;12(4):273–280.
27. Georgy MS, Pongracic JA. Hereditary and acquired angioedema. Allergy Asthma Proc. 2012;33(Suppl 1):S73–S76.
28. Al-Khudari S, Loochtan MJ, Peterson E, et al. Management of angiotensin-converting enzyme inhibitor-induced angioedema. Laryngoscope. 2011;121(11);
2327–2334.
29. Campo P, Fernandez TD, Canto G, et al. Angioedema induced by angiotensin-converting enzyme inhibitors. Curr Opin Allergy Clin Immunol. 2013;13(4):337–344.
30. Hungerford JM. Scombroid poisoning: A review. Toxicon. 2010;56(2):231–243.
31. Kanwar M, Irvin CB, Frank JJ, et al. Confusion about epinephrine dosing leading to iatrogenic overdose: Life-threatening problem with a potential solution. Ann Emerg Med. 2010;55:341–344.
32. Bauer CS, Vadas P, Kelly KJ. Methylene blue for the treatment of refractory anaphylaxis without hypotension. Am J Emerg Med. 2013;31:264.e3–e5.
33. Lin RY, Curry A, Pesola GR, et al. Improved outcomes in patients with acute allergic syndromes who are treated with combined H1 and H2 antagonists. Ann Emerg Med. 2000;36:462–468.
34. Lee S, Hess EP, Nestler DM, et al. Antihypertensive medication use is associated with increased organ system involvement and hospitalization in emergency department patients with anaphylaxis. J Allergy Immunol. 2013;131:1103–1108.