Katie Sprinkel and Stephen Colucciello
There is substantial regional variation in the etiology of facial trauma, and in the developed world interpersonal violence has surpassed motor vehicle collisions (MVCs) as the most common cause of facial fractures (1). The use of seat belts as restraint devices in vehicles has been repeatedly shown to result in a decreased incidence of facial lacerations and fractures, whereas the protective effect of airbags is less clearly established in facial trauma (2). Other causes include falls, sports injuries, and gunshot wounds, with gunshot wounds and MVCs resulting in the highest injury severity (1). The most frequently fractured facial bones in descending order are the nasal bones, orbital floor, zygomaticomaxillary complex, maxillary sinuses, and mandibular ramus (1).
CLINICAL PRESENTATION
The presentation of maxillofacial trauma depends largely on the mechanism of injury; understanding the mechanism of injury can aid in predicting the severity and risk for associated injuries. Patients who sustain significant blunt trauma (e.g., MVC) often suffer multiple injuries, and their initial evaluation and stabilization should follow a standard trauma protocol. Neglecting potentially serious chest, abdominal, or pelvic injuries in the multiple-trauma patient with distracting facial deformity is a dangerous error. Facial injuries in women in particular are a marker for intimate partner violence, which is underreported and should be investigated when taking the patient’s history. Studies estimate between 1/3 and 2/3 of women who present with facial trauma are victims of intimate partner violence (IPV), and the most common injuries are to the midface (3). Overall, assaults most frequently involve young males as the perpetrators with alcohol being the main contributing factor. Mandibular, orbital floor, nasal, and zygomaticomaxillary complex fractures most commonly result from assault, whereas MVCs tend to cause more complex midface injury patterns (1).
Victims of penetrating maxillofacial trauma are less likely to have serious injuries to distant organ systems but may experience injury to the globe, brain, or neck. High-velocity injuries have a high rate of airway compromise, with nearly a third requiring urgent airway control, either intubation or a definitive surgical airway (4). The emergency physician must be particularly attuned to both central nervous system (CNS) and vascular injury in penetrating trauma as well.
Airway compromise and management of hemorrhage are the most urgent concerns in maxillofacial injury. Airway problems can result from a posteriorly displaced tongue, dislodged teeth, oral hemorrhage and vomitus, or injury to the soft tissues surrounding the airway. A decision for definitive airway control is based on the patient’s level of consciousness, severity of injury, risk for aspiration or airway obstruction by delayed edema, and hematoma formation (5). Clinicians who elect to perform blind nasotracheal intubation should be aware of the rare risk of intracranial placement of the endotracheal tube (6). The risk of delayed airway compromise has prompted some authors to recommend intubating patients who present with significant intraoral blood or moderate-sized hematomas in the neck or face, although definitive support in the literature is lacking (7). For patients who require transfer for definitive care, the emergency physician should consider the risk of developing airway compromise en route to the trauma center and complications may increase with the length of transport. When in doubt, it is best to obtain a definitive airway prior to transport. Given the significant vascularity of facial structures, maxillofacial trauma may infrequently result in enough blood loss to cause hypotension and, rarely, exsanguination. The incidence of severe hemorrhage ranges from 1% to 11%, with the highest incidences occurring in patients with midfacial fracture (8,9). The tamponade effect of the facial musculature combined with the relative accessibility for direct pressure makes life- threatening hemorrhage in adults relatively uncommon.
DIFFERENTIAL DIAGNOSIS
The sometimes dramatic appearance of facial trauma may distract the examining physician from more serious injuries. Once the airway is ensured and brisk facial bleeding controlled, other life threats must be quickly and systematically excluded. Then, the emergency physician should attempt to specifically address bony and soft tissue facial injuries.
Brain injury is the most common associated injury, occurring in up to 79% of patients with single facial fracture, and 88% of patients with two or more facial fractures (10). Previously, some suggested that facial fractures may decrease the risk for intracranial injury. Recent evidence supports the contrary, noting that patients with facial fractures, especially involving the midface, actually have an increased risk of traumatic brain injury (10). This link suggests that the clinician should have a low threshold for performing head computed tomography (CT) in patients with any facial fracture, especially those who have altered mental status, neurologic deficit, or perhaps a worrisome mechanism of injury. The converse is also true. In one study, 10% of comatose blunt trauma victims had significant unsuspected facial bone fractures that were diagnosed by routine facial CT (11).
The incidence of concomitant cervical spine fracture in the setting of facial fracture is not insignificant, reports range from 1% to 8% with that number increasing with number of facial fractures (10,11). The use of the Nexus or Canadian Cervical Spine Rules provides evidence-based guidelines for cervical radiography and the presence or absence of a facial fracture alone should not determine the need for cervical spine imaging unless it is considered a “distracting injury.” See Chapter 28, “Cervical Spine Fractures” (12). There is some data to suggest that facial fracture is a risk factor for injury to the carotid or vertebral vessels, which is more frequent in blunt trauma than previously recognized. Recent guidelines recommend imaging (CT angiography) to screen for cerebrovascular injury if the patient has displaced midface or complex mandibular fractures (13).
Loss of vision is another significant concern, occurring in as high as 6% of maxillofacial trauma. Visual testing and red color perception are the most useful tests but not always possible in the unconscious patient. Pupillary size and shape, reactivity to light, lid lacerations and globe tension to palpation may also reveal important clues to ocular or periorbital injury (14,15).
ED EVALUATION
Aside from airway concerns, maxillofacial injuries are seldom life threatening. However, other organ system injuries carry significant morbidity and potential mortality. After resuscitation and addressing significant injuries to other organ systems, the emergency physician should perform a thorough and directed examination of the face. Anatomic complexity, swelling, lacerations, pain, and altered level of consciousness pose challenges to an optimal physical examination. A systematic approach can help surmount these challenges.
A complete history, including specifics about the mechanism of injury, should be obtained, ensuring that certain injuries are not overlooked. High-yield general questions include the presence of loss of consciousness, facial numbness, weakness, and visual disturbances. Specifically, for periorbital injuries, the emergency physician should ask about blurred vision, pain on extraocular motion, and diplopia. Monocular diplopia indicates a problem with the lens or retina in a single eye; binocular diplopia that involves eye movement suggests nerve palsy, muscle injury, or entrapment. For midface and jaw injuries, ask about dental malocclusion and trismus.
The emergency physician should begin with inspection and evaluate the patient from multiple perspectives. This should include both the “bird’s eye view” as well as the “worm’s eye view,” which involves inspection from above and below to reveal subtle facial asymmetries. Loss of contours, edema, ecchymosis, and hemorrhage are clues to soft tissue and underlying bony injuries (eFig. 23.1). Facial elongation in the frontal plane can occur with high-grade Le Fort fractures (“donkey” facies) (16). Ecchymoses around the eyes (raccoon eyes) and over the mastoid areas (Battle’s sign) are associated with basilar skull fractures. Raccoon eyes, which usually take several hours to develop, are nonspecific and may be associated with nasoorbitoethmoid (NOE) injuries, Le Fort, orbital, and frontal bone fractures. Facial function is tested by examining the muscles of facial expression. Patients should be asked to close their eyes tightly, raise their eyebrows, purse their lips, smile, and frown. Fractures of the temporal bone may be associated with a posttraumatic Bell palsy with weakness of the facial muscles on the affected side (16). Difficulty with opening and closing the mouth may be secondary to jaw muscle spasm, or it is less commonly associated with fractures of the mandible, zygoma, or maxilla. Evaluating extraocular motions is just as important as testing facial function. Inability to gaze upward or downward, exophthalmos, or enophthalmos can be associated with periorbital fractures. Pain with extraocular movements suggests an occult periorbital fracture. The eye examination should encompass visual acuity, examination of the anterior chamber and pupil, extraocular motions, ptosis, periorbital sensation, and the swinging flashlight test to assess for a Marcus Gunn pupil (see Chapter 25). The ear canal is inspected for any lacerations or clear fluid leak that may represent cerebrospinal fluid (CSF). Using an otoscope, the tympanic membrane is examined for evidence of rupture or hemotympanum, seen as a purplish bulge of the membrane. This finding is associated with basilar skull fracture and fractures of the mandibular condyles. The external ear is examined for otohematomas, which can result in chronic deformity called “cauliflower ear.” In the nose, the most important findings include septal hematoma and CSF rhinorrhea. A septal hematoma is a bluish colored, bulging septal mass that is tender and boggy to palpation.

FIGURE 23.1 Nasoethmoidal fractures.

eFIGURE 23.1 Superficial facial injuries provide important visual clues to underlying soft tissue and bony injuries.
The emergency physician should consider testing bloody nasal discharge for CSF. A drop of the bloody fluid containing CSF will demonstrate a target or “halo sign” when placed on a paper towel or bed sheet, because the CSF migrates farther and faster than blood. This test can produce false-negative results with non-CSF fluids mixed with blood, whereas glucose and β-2 transferrin testing are more specific for CSF (10).
Palpation is another important part of the physical examination. The entire face should be palpated for tenderness, step-offs, bony crepitus, and subcutaneous air (often present with fractures involving the sinus). Facial stability is tested by placing a gloved hand in the patient’s mouth, grasping the hard palate, and rocking back and forth while the other hand simultaneously palpates the central face. The physician should be careful to not rock the teeth themselves if dental trauma exists, as dental avulsion may occur.
The final part of the examination of the face is a test for sensation. The branches of the trigeminal nerve are commonly disrupted or contused during facial injury and can cause sensory deficits to the face. The V1 branch of the trigeminal nerve is particularly susceptible to injury in the supraorbital notch. Damage to this nerve can result in anesthesia of the upper nose, eyebrow, and forehead. The infraorbital nerve can be disrupted as it courses through the floor of the orbit and is frequently damaged with orbital or zygomatic fractures. This results in ipsilateral numbness of the lower eyelid, side of the nose, upper lip, gums, and hard palate. Finally, the mental nerve can be injured when there is a mandibular injury resulting in ipsilateral anesthesia to the chin. The presence of facial anesthesia does not necessarily confirm a facial fracture; contusion to the nerve alone can produce similar numbness.
While plain radiographs (e.g., a Waters view, or occipitomental view, for midface fracture) may be effective as a screening tool for some facial fractures, there has been a gradual shift away from this modality (17). Ultrasound has been shown to have diagnostic value, recognizing its limitations with nondisplaced and complex fractures, especially in posterior orbital floor and mandibular condyle where sensitivity is especially low. Data is most impressive for nasal bone fractures, with a sensitivity of 90% to 100% and specificity of 98% to 100% with ultrasound (18). CT, however, is the gold standard for imaging in cases where there is concern for facial fracture with superior sensitivity, speed, cost, and utility in surgical planning (17). Interestingly, several studies have shown that the noncontrasted head CT ordered primarily for ruling out intracranial trauma, has the added advantage of evaluating for orbital, maxillary, and zygomatic fractures, citing sensitivities of 90% to 100% (19,20). The decision to add facial CT to a patient already undergoing head CT can be augmented by specific physical examination findings. Aid in the decision to add a facial CT to a patient’s planned head CT may come from the knowledge that 12% of trauma patients who require a head CT will have facial fractures as well as the fact that complicated orbital fractures may not be fully delineated on isolated head CT (21).
KEY TESTING
• Airway assessment and attention to hemorrhage take precedent, vision-threatening injury should also be evaluated with an ocular examination.
• If suspicion for facial fracture exists based on physical examination, facial CT is the gold standard imaging modality (17).
• Ultrasound shows promise in the diagnosis of facial fracture, in particular there is data showing nasal bone fractures, orbital fractures, anterior maxillary wall, and zygomatic arch fractures can be readily detected (18).
• Head CT should be strongly considered in any patient with facial fracture given the high incidence of concomitant intracranial injury.
• Facial fracture is also a marker of increased risk for cervical spine fracture in trauma, adherence to clinical decision rules is appropriate to determine need for cervical spine imaging.
• CT angiography (16-slice scanner) is recommended to screen for cervical vessel injury with displaced midface and complex mandible fractures (13).
ED MANAGEMENT
Fractures, bleeding, edema, and foreign bodies (such as loose teeth) may occlude the airway and distort anatomy minutes to hours after injury. Thus, it may be prudent to prophylactically secure the airway in patients with evidence of progressive swelling using rapid-sequence orotracheal intubation or an awake intubation. In patients with significant facial trauma, equipment for “backup” cricothyrotomy should be readily available as several factors may qualify them as “difficult airways.” These factors should be assessed prior to any intubation attempt, including the potential for poor mask seal precluding effective bag-valve-mask ventilation, cervical spine immobilization, and loss of normal landmarks with bony, soft tissue, and vascular injury.
The patient’s position on the stretcher dramatically affects the airway. Sitting up and leaning forward is the “position of life” as it clears the airway of blood and displaces any fractured bones or loose tissue forward. The patient can even self-suction blood with one or two Yankauer suction catheters. However, this position is not an option if there is significant concern for cervical spine injury.
Maxillofacial trauma can compromise the airway at the nasal, oropharyngeal, or laryngeal level. If collapse of the nasal airway results from posteroinferior displacement of maxillary fractures, definitive control may be achieved by pulling the face forward using anterior traction on the maxilla (38). The maxillary arch should be grasped above the front teeth to avoid pulling them out of their loosened sockets. If a prolapsed tongue is occluding the oropharyngeal airway (often seen in central mandibular fractures), the tongue can be pulled forward with a traction suture or towel clip. Maxillofacial trauma may also occur in conjunction with direct trauma to the neck, causing airway collapse at the level of the larynx. Cricothyrotomy is possible if the level of injury is above the larynx. In patients with injuries at or inferior to the larynx, endotracheal intubation under direct laryngoscopy may be attempted, but emergency tracheostomy may be necessary. If tracheal injury is inferior to a level at which tracheostomy will provide an adequate airway, emergent consultation with an ENT or thoracic surgeon is warranted (22).
Once the airway is secure and breathing is stabilized, the “C” of the trauma ABCs must be addressed. Although some patients with maxillofacial trauma may be hypotensive, isolated facial injuries rarely cause shock (8). Hemodynamic compromise should be ascribed to other injuries until proven otherwise. The blood supply to the face involves both branches of the external and internal carotid arteries with several anastomoses between each. Generally, if there is ongoing hemorrhage, direct pressure should be applied both internally to the anterior nares and externally where indicated. Immediate manual reduction of fracture fragments or dislocations may also slow the bleeding. If there is continued blood loss despite these maneuvers, particularly if there is massive nasopharyngeal bleeding, hemorrhage control may be achieved by using posterior nasal packing with either gauze, Foley catheter, or a commercially available nasal balloon (8). Care should be taken with posterior nasal packing to avoid the risk of intracranial placement. The McKesson prop, which is a rubber stopper placed in between the upper and lower teeth to push the midface upward, has also been proposed as a temporizing measure to tamponade bleeding from severe midface fractures (17). Seldom, with maxillary fractures, the posterior pharynx may need to be packed after endotracheal intubation. If hemorrhage continues, arterial ligation or embolization should be pursued (8).
Frontal Bone Fractures
The frontal bone is the strongest bone in the face, consisting of a thick anterior wall that can tolerate as much as 2200 lb of force, and a relatively thin posterior wall. Two-thirds of frontal bone fractures involve both anterior and posterior tables, and given the tremendous amount of force required to break these bones, the incidence of concomitant intracranial and other facial injury is high. These fractures also carry significant potential for infection (23). Therefore, patients with known or strongly suspected frontal bone fractures should undergo head CT scanning and meticulous evaluation for associated injuries, including orbital, nasal, and ethmoid fractures (24).
Frontal sinus injuries are often not obvious; suspicion is based on mechanism of injury (person’s head hits the dash of a car or assault with a heavy blunt object such as a brick). On inspection, the emergency physician should look for any depression of the forehead. Glabellar depression indicates fracture of the anterior wall of the frontal sinus. The presence of subcutaneous air indicates sinus disruption, and the supraorbital rims should be palpated for step-off or deformity. Palpation with a sterile gloved finger can help detect fractures that underlie open wounds. Though rare, posterior wall fractures may result without an anterior wall fracture (24). When testing sensation, it is important to realize that numbness in the distribution of the supraorbital nerve (forehead) may herald an occult fracture. CSF rhinorrhea, if present, indicates involvement of both the posterior wall and meninges (24). Some patients may present with postnasal drip as CSF may preferentially enter the oropharynx. Finally, all patients with frontal bone fractures deserve a thorough ophthalmologic examination due to high rate of concomitant injury.
Although plain films such as Waters and Caldwell views of the face can screen for fracture, if there is significant concern for fracture, axial and coronal CT is indicated to delineate the status of the posterior table and the nasal frontal outflow tract (14). Pneumocephalus is another significant finding which indicates dural violation (25).
Repair of the anterior wall of the frontal sinus can often be delayed; however, fracture of the posterior table requires urgent neurosurgical consultation. When the frontal sinus is fractured, prophylactic antibiotics are generally given. Commonly prescribed antibiotics include first-generation cephalosporins, erythromycin, trimethoprim–sulfamethoxazole, and amoxicillin-clavulanate. However, choice of antibiotics and when to start them is often left to the consultant. In addition, the presence of CSF rhinorrhea associated with frontal bone fractures usually prompts antibiotic prophylaxis by the consultant, although there has been conflicting evidence to the utility of this practice.
Orbital Fractures
Trauma to the orbital regions may range from simple soft tissue swelling around the eye to blindness. Immediate blindness from trauma is rare and is generally permanent, but delayed loss of vision is possible (15). A majority of blindness results from globe rupture; however, damage to the optic nerve (directly or indirectly) and retinal detachment can also lead to a loss of visual acuity. In addition, direct ocular trauma can produce a traumatic iritis. Injuries occurring as a result of trauma to the globe are discussed in detail in Chapter 25.
Fractures of the orbit are either “pure” or “impure.” Pure fractures affect only the internal orbit without orbital rim involvement, whereas impure fractures include the orbital rim. The blow-out fracture (eFig. 23.2) is a pure internal orbital fracture, usually involving the floor and medial portion of the orbit (24). These fractures occur with either direct force to the orbital rim or when a blunt force strikes the globe. Blow-in fractures consist of fractures and collapse of the orbital roof, which are strongly indicative of intracranial injury. If the fracture propagates to the orbital apex, it can place the optic nerve in jeopardy. This is called orbital apex syndrome and is an emergency if there are clinical or radiographic signs of optic nerve impingement (23).

FIGURE 23.2 Zygomaticomaxillary complex fractures.
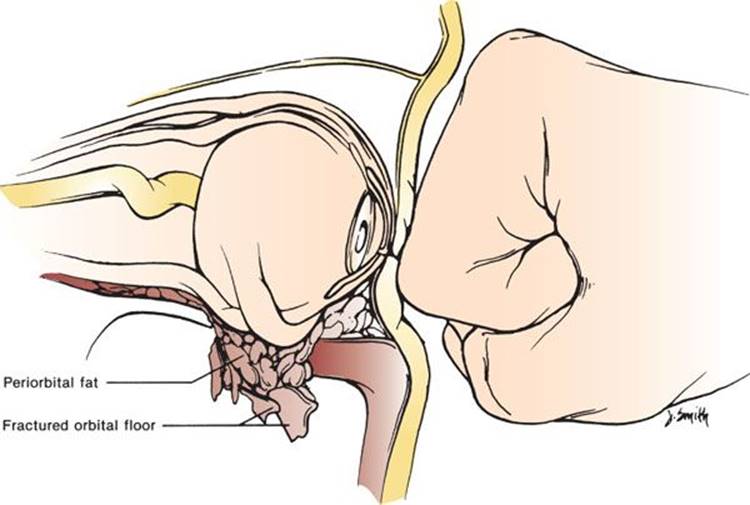
eFIGURE 23.2 Blow-out fracture.
The patient’s orbital region should be inspected for eyelid edema, lacerations, ecchymosis, enophthalmos (sunken globe), hypoglobus, proptosis, or obvious inability of the patient to deviate the involved eye. If the patient cannot look up or complains of diplopia on upward gaze, inferior rectus muscle entrapment associated with orbital blow-out fractures should be considered (26). However, most diplopia is a result of muscle hematoma or nerve injury and not a result of true muscle entrapment. The orbital rims should be palpated for bony step-offs or crepitus, which may indicate a fracture involving the sinuses. When palpating for irregularities, the unaffected side should be palpated for comparison, because the supraorbital and infraorbital nerve foramina can masquerade as fractures (24). Finally, the patient should be asked about numbness of the cheek, maxillary teeth, or upper lip. Paresthesias in these areas suggest a contusion or disruption of the infraorbital nerve (24). When there are findings consistent with fracture in the orbital region, the emergency physician’s first step is a meticulous evaluation of the globe. The ocular examination takes precedence because certain injuries (e.g., globe rupture) benefit from early diagnosis and management, and an adequate examination may be impossible as swelling progresses. In a patient with acute orbital trauma, the two most important ophthalmologic functions to evaluate are visual acuity and extraocular muscle mobility. If the eyelid is too swollen to allow for retraction and therefore an evaluation of visual acuity, light perception should be documented to ensure optic nerve integrity. When in doubt, involvement of ophthalmology is prudent. Retrobulbar hematoma, or more rarely, subcutaneous emphysema creating ocular compartment syndrome, must also be addressed emergently if a tense proptotic globe with decreasing visual acuity is identified. Lateral canthotomy should be performed in consultation with an ophthalmologist to prevent optic nerve ischemia, and mannitol, acetazolamide, and steroids may further decrease the possibility of optic nerve ischemia in the presence of increased intraocular pressure (26). Once ocular injuries have been identified, attention shifts to imaging of the orbital region. Plain radiographs are no longer recommended as screening tools as CT is the preferred test (27). Classic radiologic signs include the “hanging teardrop,” which appears when orbital fat herniates into the maxillary sinus, and air/fluid levels in the maxillary sinus.
Management of orbital blow-out fractures remains controversial but phone consultation with plastic surgery on call provides crucial follow-up. In addition to consultation, the following guidelines provide a reasonable basis for decision making in the emergency department (ED). In cases associated with minimal displacement, no entrapment, and no diplopia, the patient may be treated as an outpatient with head elevation, ice, pain medication, and surgical follow-up within several days (28). Absolute indications for surgery include acute enophthalmos, hypophthalmos, or muscular entrapment with mechanical gaze restriction, even despite lack of extraocular muscle entrapment on CT (23). Contraindications for urgent surgery include hyphema, retinal tears, and globe perforation, as soft tissue injuries of the eye may be aggravated by surgery for blow-out fractures. Timing of surgery is also controversial especially in the multiply injured patient and is a decision to be made by the consultant(s). Patients should be refrained from nose blowing, which can increase the risk for rare, but significant, orbital subcutaneous emphysema (29). If there is significant subcutaneous emphysema or other evidence of fracture into the maxillary sinus, some physicians prescribe prophylactic antibiotics against sinus pathogens, although the utility of this practice has not been studied in a prospective manner (23). First-generation cephalosporins, trimethoprim–sulfamethoxazole, or amoxicillin–clavulanate are often employed.
Nasal Fractures
Nasal bone fractures are the most common facial fracture, and can result in chronic deformity and nasal obstruction (30). Isolated nasal bone fractures typically do not require emergent treatment unless there is significant epistaxis or septal hematoma. A more severe injury involves trauma to the bridge of the nose and includes fractures of the medial orbital wall. This is termed a NOE fracture and can involve disruption of the cribriform plate with associated CSF rhinorrhea or intracranial injury (22).
Evaluation begins with a detailed history. The patient should be asked about previous nasal fractures and whether the nose looks normal, as nasal deformity can be secondary to either old or new trauma. Another important question regards difficulty breathing through the nose.
The nose should be inspected for swelling, ecchymoses, and deformity and palpated for crepitus. The emergency physician should move the nasal pyramid to both sides to detect any mobility. Using a nasal speculum inside each naris, the physician should note the position of the nasal septum and examine for lacerations and septal hematoma, which will appear as a bulging blue mass that is boggy to palpation with a finger or cotton swab. Any fluid from the nose should be tested for CSF.
Nasal bone fractures are often diagnosed by history and physical examination alone. Nasal bone radiographs have no clinical utility as they do not affect management (31). If there is no misalignment of the nose, the only treatment includes ice packs and analgesia. If the patient presents immediately with deformity and significant swelling has not developed, closed reduction using local anesthesia and manual pressure with or without forceps can be attempted according to the comfort and experience of the emergency physician. More often, soft tissue edema precludes adequate examination and the patient should be referred to ENT or plastic surgery as an outpatient. Often, open or closed reduction will be performed within 5 to 7 days, after swelling has subsided. Indications for immediate treatment include CSF rhinorrhea, the presence of septal hematoma, and lacerations with exposure of the underlying bony or cartilaginous elements (30).
Septal hematomas, if not drained in the ED, can lead to abscess formation or necrosis of the nasal cartilage, with resultant saddle nose deformity especially if the hematoma is bilateral. To drain a septal hematoma, the nasal mucosa is anesthetized with a topical anesthetic, and a no. 11 blade is used to make a mucosal incision through the inferior portion of the hematoma, excise a small amount of mucosa. The clot should be suctioned and the area irrigated before the nostril is packed in similar fashion to that for anterior epistaxis. The patient should be put on broad spectrum antibiotics and packing can be removed when there is no hematoma for 24 hours (32).
Nasoorbitoethmoid Fractures
NOE fractures result from significant forces to the bridge of the nose or medial orbital wall and rarely occur as isolated events. These injuries involve the central portion of the midface (the nasal bones, frontal processes of the maxilla, and ethmoid bones) (Fig. 23.1) and may result in a fracture of the cribriform plate with subsequent CSF leakage (22). In addition, these fractures may be associated with dural tears or lacrimal disruption.
A thorough history of the mechanism of injury can be helpful in making the diagnosis typically this will be high-energy blunt trauma. On examination, asymmetry or widening of the nasal bridge between the eyes should be noted (telecanthus) as this is the most troublesome permanent defect resulting from these fractures. The distance between the medial canthi is normally about half the interpupillary distance (approximately 32 to 35 mm for Caucasians). An increase in this distance suggests an NOE fracture. Also characteristics of NOE fractures are a flattened nasal bridge, enophthalmos, and epiphora (tears pouring over the eyelid) (33). These findings are increasingly difficult to detect as swelling progresses. Palpation of the medial orbital rim especially at the medial canthus may reveal crepitus, tenderness, or movement of bony fragments.
Plain radiographs are not useful in the diagnosis of NOE fractures because of thin bones and complex anatomy. Radiographic assessment should be performed with a facial CT scan with fine-cut axial and coronal images.
The emergency physician’s role in management of the patient with an NOE fracture is to make the diagnosis and to rule out associated lacrimal system injury or dural tear. NOE fractures should be repaired no later than 10 to 14 days, but if an NOE injury is identified, the patient will generally be admitted by a facial surgeon.
Zygomatic Fractures
The zygoma is a prominent bone in the lateral portion of the facial skeleton that attaches to the maxillary, frontal, and temporal bones. Occasionally, the zygoma is fractured exclusively through its body. However, because of the thickness of this bone, fractures often extend through weaker areas of the orbit and maxilla. Fractures through the suture lines where the zygoma attaches to the three adjacent bones are termed tripartite, tripod, or zygomaticomaxillary fractures, whereas fracture through the arch of the zygoma are termed (not surprisingly) zygomatic arch fractures (Fig. 23.2).
History and physical examination reliably detect most zygomatic fractures. The mechanism of this injury is usually a direct blow to the cheek with a bat or fist. The patient may complain of pain with, or difficulty in, opening the mouth, which can be a result of impingement of the bone fragment on the temporal muscle or coronoid process The patient’s range of mouth opening should be >30 mm; if it is less than this or there is cheek pain with jaw movement, a zygoma fracture should be suspected (26). Inspection of patients with zygomatic injuries may reveal flattening of the cheek or a downward orbital tilt secondary to disruption of the lateral canthal ligament. Lateral subconjunctival hemorrhage may be an important clue to an associated zygoma injury. Further examination may reveal binocular diplopia secondary to damage of the extraocular muscles or entrapment. Up to 90% of patients with blunt zygoma trauma will have hypesthesia in the infraorbital nerve distribution (26,34). Palpation of the zygomatic arch is accomplished by the intraoral approach (the index finger is placed along the outside of the upper rear molars to palpate the arch intraorally). A crushed arch may not permit an examining finger to slip under the arch on the involved side as compared to the opposite side (26).
If an isolated arch fracture is suspected, a submentovertex view, or “jug-handle” radiograph, may aid in diagnosis. If a tripod fracture or other complex fracture is suspected, a facial CT with fine cuts through the maxilla and orbit is indicated. Surgical consultation for possible open reduction and internal fixation should be obtained for these fractures, but treatment is often delayed until swelling has subsided and a complete evaluation can be preformed. In patients with isolated fractures of the zygomatic arch, ED management is limited to analgesia and surgical follow-up within several days. All patients with suspected fractures of the zygoma should avoid nose blowing to decrease the incidence of subcutaneous emphysema (26).
Maxillary Fractures
Maxillary fracture is the most common finding in patients who sustain penetrating facial trauma. In blunt trauma, maxillary fractures are often associated with other significant traumatic injuries, as these bones require considerable force to break. The Le Fort classification system is used to describe maxillary fractures and by definition all involve the pterygoid plate. In actual practice, pure Le Fort fractures are much less common than unilateral or bilateral mixed maxillary fractures (e.g., left Le Fort I with right Le Fort II).
• Le Fort I
• Transverse line separates the hard palate from the surrounding bone (Fig. 23.3).

FIGURE 23.3 Lines of fracture in Le Fort I, Le Fort II, and Le Fort III fractures are shown from different views.
• “Floating palate,” may involve dental mobility but nose does not move.
• Le Fort II
• Pyramidal fracture line extends into the orbital floor and inferior orbital rim, separates central maxilla and palate from the rest of the face
• Mobility of maxilla and hard palate is appreciable.
• Le Fort III (Craniofacial dysjunction)
• NOE, zygomas, and maxilla are separated from calvarium.
• Maxillary excursion reveals facial mobility, globes are kept in place by the optic nerve.
• Le Fort IV
• Le Fort III with associated frontal bone fracture.
Fractures of the maxilla are often associated with significant facial edema and bleeding, which may make diagnosis by inspection difficult. The emergency physician should note any asymmetry or loss of contour; an elongated oval or donkey face may be seen with high-grade maxillary fractures. Orbital ecchymosis, lengthening, and edema of the middle third of the face, and malocclusion are also present with Le Fort type II and III fractures. Facial nerve injury may also accompany maxillary fractures, with resultant facial muscle paralysis, and sensory deficits in the infraorbital distribution should be noted. When there is trauma to the lateral midface, the physician should carefully examine cheek wounds for clear or pink fluid leakage (saliva), representing possible parotid duct damage. Alternatively, blood may be expressed from the parotid duct located adjacent to the maxillary molars when the parotid gland is massaged. Providers should also be vigilant for CSF leaks presenting with rhinorrhea with Le Fort type II and III fractures.
Palpation of the maxillary structures follows inspection with special attention given to bony crepitus and abnormal mobility of the face upon stress maneuvers. To stress the face, the examiner firmly grasps the upper palate and rocks back and forth, checking for abnormal midface mobility with the other hand (eFig. 23.3). In patients with facial mobility, the fracture is further characterized by delineating the mobile portions of the face.
eFIGURE 23.3 Checking for abnormal midface mobility.
Severe epistaxis is commonly associated with maxillary fracture, with the internal maxillary artery being the most frequent culprit. Anterior and posterior nasal packing and fracture reduction can often decrease facial hemorrhage, although care should be taken with posterior nasal packing as intracranial placement of a Foley or commercial packing material could occur (2). If basic measures to tamponade have failed and life-threatening hemorrhage continues, arterial ligation or transcatheter arterial embolization are the next steps to address ongoing hemorrhage (8).
CT scan is required to delineate the extent of bony and soft tissue injury if there is suspicion for midface fracture, plain films are not sufficient. Penetrating trauma to the midface can involve injury to the brain and major vascular structures in the head and usually requires CT of the brain and occasionally diagnostic angiography. Multislice CT angiography have been recommended in cases of displaced midface fracture to screen for cerebrovascular injury (13). Surgical specialists should be consulted early when significant maxillary fractures are identified, early versus late repair will be determined by coexistent injuries.
Mandible Fractures
After nasal bone fractures, the mandible is the most commonly fractured facial bone. Because of its ring shape, the mandible is frequently broken in more than one place; one series found that more than half of mandibular fractures occur in at least two locations (35). Areas of the mandible that are most commonly fractured are the mandibular condyle, body, and the angle (Fig. 23.4).

FIGURE 23.4 Mandible fractures: sites and incidence.
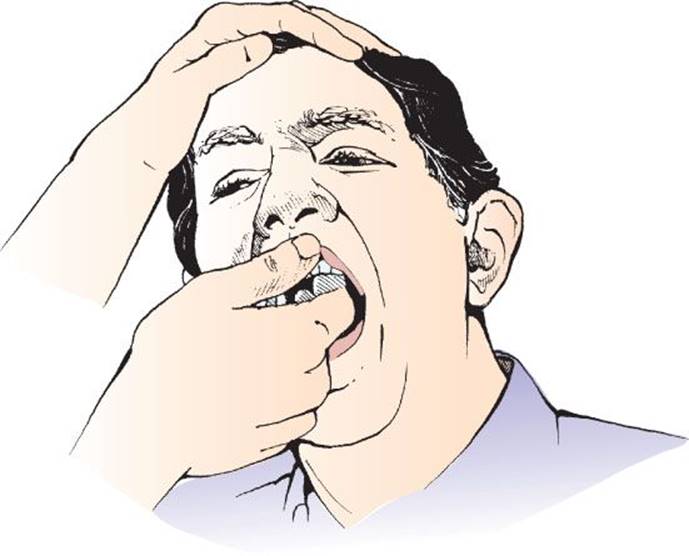
Patients should be asked whether their teeth fit together normally, as many fractures of the mandible or maxilla result in malocclusion. The proprioceptive receptors of the teeth allow for detection of as little as 1 to 2 mm of bite discrepancy (34). Then, the patient should be asked whether there is jaw pain with opening or closing of the mouth, and sensation should be assessed in the mental nerve distribution of the lower lip and chin. During the physical examination, the patient’s jaw is inspected for asymmetry. When a fracture is present, the chin is often deviated toward the injured side; with a unilateral dislocation, the jaw is deviated away from the injured side. Traumatic dislocation from acute blunt trauma is rare; fractures are far more common. Edema, bleeding, and hematomas can also provide evidence of fracture. Particularly, preauricular swelling or bleeding from the external auditory canal may indicate a condylar fracture, which can be notoriously difficult to identify on plain radiographs. A careful intraoral examination is of paramount importance to evaluate for open fracture, including any tenderness or irregularities in the contour of the mandible or altered dentition. A sublingual hematoma, although not common, is strongly suggestive of mandibular fracture. Normal condylar excursion should be assessed by placing the examiner’s fingers into the external ear canals and instructing the patient to open and close the mouth. In the patient with pain but without obvious fracture, the tongue depressor test has been shown to be a useful clinical tool to rule out mandible fracture with a sensitivity of 95% (36). A positive test, suggestive of possible fracture, is elicited when the patient reflexively opens his mouth when a tongue depressor clenched between the teeth on the side of the fracture is twisted by the examiner. Normally, a patient should be able to break the tongue blade when it is twisted between the teeth (eFig. 23.4).

eFIGURE 23.4 Tongue blade test.
CT scan has surpassed plain radiographs as the gold standard for diagnosis of mandibular fractures and have been shown to have greater sensitivity and utility in operative planning (14,37). The panoramic radiograph (Panorex) still holds some utility in defining dentition even after CT. Although evidence for prophylactic antibiotics in mandibular fractures is poor, standard practice is to give intravenous antibiotics for open mandibular fractures to cover oral pathogens (38). Penicillin G (2 to 4 million units IV) is the drug of choice, with clindamycin (600 to 900 mg IV) and first-generation cephalosporins serving as alternatives. Open fractures require admission for operative treatment, whereas most closed mandibular fractures can be treated on an outpatient basis with open reduction and internal fixation 3 to 5 days after injury to allow for swelling to decrease if patient comfort allows. A Barton bandage (Ace bandage wrapped around the head and jaw) and soft or liquid diets are helpful in cases of delayed repair.
Mandibular Dislocations
The temporomandibular joint is also subject to dislocation; this may occur during yawning, singing, or other movements that involve opening the mouth very widely. Dislocation can also occur during seizures, dystonic drug reactions, dental procedures, or more rarely after blunt trauma. Dislocation is often recurrent.
With mandibular dislocation, the history is often difficult to obtain because the patient has difficulty speaking. During inspection, asymmetry of the jaw is a clue to the diagnosis. A unilateral dislocation will often cause deviation of the mandible away from the affected side. A bilateral dislocation of both condyles will give the patient an underbite appearance (bottom teeth more anterior than upper teeth). The teeth will not occlude normally, and speech is often affected. Often there is significant masseter muscle spasm that can make reduction difficult.
Mandibular dislocations can be reduced by the emergency physician, sometimes requiring benzodiazepines or local anesthetic to relax the masseter or pterygoid muscles. Occasionally, conscious sedation may be required. There are two simple reduction techniques that are most often employed. In the first technique, the clinician faces the patient with thumbs wrapped in gauze to avoid being bitten. The physician’s thumbs are then placed under the posterior molars or on the mandibular ridge and the inferior surface of the mandible is grasped placing downward pressure on the molars. This will free the condyles and allow them to be pushed forward into place (28). In the second technique, the clinician stands behind the patient with gauze-wrapped thumbs on the posterior molars and fingers grasping the mandible anteriorly. Pressure is exerted downward and forward until the joint snaps into place (eFig. 23.5). An alternating rocking motion between right and left sides may help in reduction.

FIGURE 23.5 Important soft tissue structures of the face.

eFIGURE 23.5 Method for reduction of a mandible dislocation from behind.
Rarely, neither of the foregoing techniques will work, and reduction under general anesthesia may be required. Once reduction is accomplished, the patient’s jaw should be wrapped in a Barton bandage, and the patient should be instructed to avoid opening the mouth widely to prevent repeat dislocation. Though some physicians obtain x-rays to confirm the relocation of the condyles and to exclude any fractures that occurred during reduction, others do not find this necessary (16,22).
Soft Tissue Injuries
Many patients with facial fractures have associated cutaneous injuries. These do not routinely need to be closed in the patient who will undergo surgical evaluation in the ED, as the opening may be used for examination or repair. Rapid suture (“whip stitching”) is appropriate to achieve hemostasis in some cases, as the sutures can be easily removed by the consultant. Wound repair is important as cosmesis is of paramount importance to the patient. Laceration repair is discussed in Chapter 21. In addition to lacerations, oral, ocular, salivary, lacrimal, otologic, or neurologic injuries may be associated with maxillofacial trauma (Fig. 23.5).
Any dental appliances present should be removed to prevent their aspiration from compromising the airway. These appliances should be saved, as they are expensive and may provide important guides to pretraumatic oral alignment.
The significant incidence of ocular injuries associated with various facial fractures necessitates meticulous ophthalmologic evaluation in all patients sustaining maxillofacial trauma. Injuries to the lacrimal system, with associated findings such as epiphora, may be present in patients with midface fractures. Lacrimal disruption is rare in blunt trauma, even in patients with significant craniofacial injury. These injuries are discussed in Chapter 25.
Clear or pink fluid leakage from the cheek suggests parotid gland laceration or Stensen duct damage. Lacerations that cross an imaginary line drawn from the tragus of the ear to the corner of the lip may traverse the parotid duct or facial nerve. Parotid lacerations do not require repair, as commonly occurring salivary fistulas resolve spontaneously in less than a month. Stensen duct may be repaired by suturing the ends together over a stent; this is most appropriately performed by a surgical consultant.
Tympanic membrane rupture can occur when there is significant force applied to the condyles that fractures the temporal bone. They generally heal spontaneously, but referral may be necessary in those with large disruptions.
CRITICAL INTERVENTIONS
• Secure the airway in patients with evidence of progressive swelling or airway obstruction using rapid sequence orotracheal intubation. Consider “awake” intubation for those patients who are likely to be difficult to intubate but who are currently maintaining their airway.
• Have equipment for “backup” cricothyrotomy readily available when managing the airway of a patient with significant maxillofacial trauma.
• Include evaluation for vision-threatening injury with the initial assessment of facial trauma, including pupillary size and shape, reactivity to light, lid lacerations, globe tension, and visual acuity.
• Perform facial CT as the initial radiologic study if mechanism or physical examination findings are concerning for facial fracture.
• Perform cranial CT scanning in patients with significant facial fractures to rule out intracranial injury, especially with loss of consciousness or neurologic abnormalities. Cervical spine CT and CT angiography for cervical vessel injury should also be considered.
• Obtain urgent neurosurgical consultation for patients with posterior table fractures of the frontal sinus.
• Obtain urgent surgical or ophthalmologic consultation for patients with orbital fractures who have paralysis of extraocular motions, ptosis, and periorbital anesthesia (superior orbital fissure syndrome) or visual loss.
• In mandibular fractures, perform a thorough examination to evaluate for open fracture.
• Administer intravenous antibiotics (penicillin or clindamycin) to patients with open facial fractures.
DISPOSITION
In the vast majority of patients with maxillofacial trauma, the emergency physician can perform the initial resuscitation and stabilization without the need for consultation with maxillofacial specialists. The role of emergent surgical consultation in patients with airway compromise or refractory facial hemorrhage has been discussed.
Involvement of the appropriate surgical specialist is now recommended at a time earlier than had been standard in the past for patients with severe facial fractures. Delays in treatment have been shown to result in suboptimal outcome in some facial injuries (13).
Patients with CSF leak must be evaluated by a neurosurgeon in addition to a facial specialist. Although prophylactic antibiotics may be ordered by some consultants, in general they are not recommended as their use is not supported by the literature (39).
The surgical therapy for maxillofacial trauma is a rapidly evolving field. Patients with significant injuries should be transferred to referral centers if local consultants lack expertise in treating the injury in question. Before transfer, the patient who requires definitive care of maxillofacial injuries must be evaluated for other life- or limb-threatening injuries. Even in the setting of isolated maxillofacial trauma, the potential for airway deterioration may be present, and pretransfer stabilization in these instances may include intubation. The potential for airway compromise, as well as the high frequency of significant associated injuries, dictates a high level of training for personnel involved in the prehospital or interhospital transport of patients with significant maxillofacial trauma.
Common Pitfalls
• Failure to manage the airway aggressively with intubation or cricothyrotomy when indicated. Waiting too long in the presence of progressive swelling or hemorrhage may convert an urgent procedure into an emergent one.
• Failure to consider the presence of subtle or physically remote injuries. Particular attention should be paid to the neurologic and ophthalmologic examinations.
• Failure to realize that frontal bone injuries are associated with intracranial injury as well as infection.
• Failure to screen for and recognize intimate partner violence in patient presenting with facial trauma.
REFERENCES
1. Erdmann D, Follmar KE, Debruijn M, et al. A Retrospective analysis of facial fracture etiologies. Ann Plast Surg. 2008;60:398–403.
2. Stacey DH, Doyle JF, Gutowski KA. Safety device use affects the incidence patterns of facial trauma in motor vehicle collisions: An analysis of the national trauma database from 2000 to 2004. Plast Reconstr Surg.2008;121(6):2057–2064.
3. Halpern L. Orofacial injuries as markers for intimate partner violence. Oral Maxillofac Surg Clin North Am. 2010;22:239–246.
4. Kummoona R, Muna AM. Evaluation of immediate phase of management of missile injuries affecting maxillofacial region in Iraq. J Craniofac Surg. 2006; 17:217–223.
5. Lynham AJ, Hirst JP, Cosson JA, et al. ED Management of maxillofacial trauma. Emerg Med Australas. 2004;16:7–12.
6. Rosen CL, Wolfe RE, Chew SE, et al. Blind nasotracheal intubation in the presence of facial trauma. J Emerg Med. 1997;15:141–145.
7. Dolin J, Scalea T, Mannor L, et al. The management of gunshot wounds to the face. J Trauma. 1992;33:508–514.
8. Khanna S, Dagum A. A critical review of the literature and an evidence-based approach for life-threatening hemorrhage in maxillofacial surgery. Ann Plast Surg. 2012;69(4):474–478.
9. Shimoyama T. Kaneko T, Horie N. Initial management of massive oral bleeding after midfacial fracture. J Trauma. 2003;54:332–336.
10. Mulligan R, Mahabir R. The prevalance of cervical spine injury, head injury, or both with isolated and multiple craniomaxillofacial fractures. Plast Reconstr Surg. 2010;126(5):1647–1651.
11. Rehm CG, Ross SE. Diagnosis of unsuspected facial fractures on routine head computerized tomographic scans in unconscious multiply injured patient. J Oral Maxillofac Surg. 1995;53:522–524.
12. Bandiera G, Stiell IG, Wells GA, et al. Canadian S-Spine and CT Head Study Group. The Canadian C-spine rule performs better than unstructured physician judgment. Ann Emerg Med. 2003;42:395–402.
13. Bromberg WJ, Collier BC, Diebel LN, et al. Blunt cerebrovascular injury practice management guidelines: The Eastern Association for the surgery of trauma. J Trauma. 2010;68(2):471–477.
14. Sharabi SE, Koshy JC, Thornton JF, et al. Facial fractures. Plast Reconstr Surg. 2011;127:25e–34e.
15. Dancey A, Perry M, Silva DC. Blindness after blunt facial trauma: Are there any clinical clues to early recognition? J Trauma. 2005;58:328–335.
16. Hasan N, Colucciello S. Maxillofacial trauma. In: Tintinalli JE et al. eds. Emergency Medicine: A Comprehensive Study Guide. New York, NY: McGraw-Hill; 2000.
17. Turner BG, Rhea JT, Thrall JH, et al. Trends in the use of CT and radiography in the evaluation of facial trauma, 1992–2002: Implications for current costs. AJF Am J Roentgenol. 2004:183(3):751–754.
18. Adeyemo WL, Akadiri OA. A systematic review of the diagnostic role of ultrasonography in maxillofacial fractures. Int J Oral Maxillofac Surg. 2011;40:655–661.
19. Lewandowski RJ, Rhodes CA, McCarroll K, et al. Role of routine nonenhanced head computed tomography scan in excluding orbital, maxillary, or zygomatic fractures secondary to blunt head trauma. Emerg Radiol. 2004;10:173–175.
20. Marinaro J, Crandall CS, Doezema D. Computed tomography of the head as a screening examination for facial fractures. Am J Emerg Med. 2007;25:616–619.
21. Holmgren EP, Dierks EJ, Homer LD, et al. Facial computed tomography use in trauma patients who require a head computed tomogram. J Oral Maxillofac Trauma. 2004;62:913–918.
22. Parsa T, Adamo AK, Calderon Y. Initial management and evaluation of maxillofacial injuries. Available from: www.emedicine.com, 2007.
23. Mehta N, Butala P, Bernstein M. The imaging of maxillofacial trauma and its pertinence to surgical intervention. Radiol Clin N Am. 2012;50:43–57.
24. Ellis E, Scott K. Assessment of patients with facial fractures. Emer Med Clin North Am. 2000;18:411–448.
25. Martin B, Ghosh A. Antibiotics in orbital floor fractures. Best evidence topic reports. Emerg Med J. 2003;20:61–67.
26. Ceallaigh PO, Ekanaykaee K, Beirne CJ, et al. Diagnosis and management of common maxillofacial injuries in the emergency department. Part 3: Orbitozygomatic complex and zygomatic arch fractures. Emerg Med J.2007;24:120–122.
27. Brady SM, McMann MA, Mazzoli RA, et al. The Diagnosis and management of orbital blowout fractures: Update 2001. Am J Emerg Med. 2001;19(2):147–154.
28. Rupp TJ, Bednar M, Karageanes S. Facial fractures. Available from: www.emedicine.com, 2002.
29. Mohan B, Singh KP. Bilateral subcutaneous emphysema of the orbits following noseblowing. J Laryngol Otol. 2001;115:319–320.
30. Mondin V, Rinaldo A, Ferlito A. Management of nasal bone fractures. Am J Otolaryngol. 2005;26:181–185.
31. Oluwasanmi AF, Pinto AL. Management of nasal trauma–widespread misuse of radiographs. Clin Perform Qual Health Care. 2000;8:83–85.
32. Roberts JR, Hedges JR, Custalow C. Clinical Procedures in Emergency Medicine. 5th ed. Philadelphia, PA: Saunders; 2009.
33. Papadopoulos H, Salib N. Management of naso-orbital-ethmoidal fractures. Oral Maxillofac Surg Clin N Am. 2009;21:221–225.
34. Shepherd SM, Lippe MS. Maxillofacial trauma. Emer Med Clin North Am. 1987; 5:371–392.
35. Sun JK, LeMay DR. Imaging of facial trauma. Neuroimag Clin North Am. 2003; 12:295–309.
36. Caputo ND, Raja A, Shields C, et al. Re-evaluating the diagnostic accuracy of the tongue blade test: Still useful as a screening tool for mandibular fractures? J Emerg Med. 2012;45(1):8–12.
37. Wilson IF, Lokeh A, Benjamin CI, et al. Prospective comparison of panoramic tomography (Zonography) and helical commuted tomography in the diagnosis and operative management of mandibular fractures. Plast Reconstr Surg.2001;107(6):1369–1375.
38. Kyzas PA. Use of antibiotics in the treatment of mandible fractures: A systematic review. J Oral Maxillofac Surg. 2011;69:1129–1145.
39. Bell R, Dierks E, Homer L, et al. Management of cerebrospinal fluid leak associated with craniomaxillofacial trauma. J Oral Maxillofac Surg. 2004;62(6):676–684.