DOORWAY INFORMATION
Opening Scenario
Kelly Clark, a 35-year-old female, comes to the ED complaining of headache.
Vital Signs
BP: 135/80 mm Hg Temp: 98.6°F (37°C)
RR: 16/minute HR: 76/minute, regular
Examinee Tasks
1. Take a focused history.
2. Perform a focused physical exam (do not perform rectal, genitourinary, or female breast exam).
3. Explain your clinical impression and workup plan to the patient.
4. Write the patient note after leaving the room.
Checklist/SP Sheet
Patient Description
Patient is a 35 yo F, married with 3 children.
Notes for the SP
Hold the right side of your head during the encounter and look as if you are in severe pain.
Challenging Questions to Ask
“Do you have anything that will make me feel better? Please, doctor, I am in pain.”
Sample Examinee Response
“Yes, we have many options for medicines to relieve your pain, but first I need to learn as much as I can about your pain so that I can recommend the best medicine.”
Examinee Checklist
Building the Doctor-Patient Relationship Entrance
□ Examinee knocked on the door before entering.
□ Examinee introduced self by name.
□ Examinee identified his/her role or position.
□ Examinee correctly used patient’s name.
□ Examinee made eye contact with the SP.
Reflective Listening
□ Examinee asked an open-ended question and actively listened to the response.
□ Examinee asked the SP to list his/her concerns and listened to the response without interrupting.
□ Examinee summarized the SP’s concerns, often using the SP’s own words.
Information Gathering
□ Examinee elicited data efficiently and accurately.

Connecting with the Patient
□ Examinee recognized the SP’s emotions and responded with PEARLS.
Physical Examination
□ Examinee washed his/her hands.
□ Examinee asked permission to start the exam.
□ Examinee used respectful draping.
□ Examinee did not repeat painful maneuvers.
Closure
□ Examinee discussed initial diagnostic impressions.
□ Examinee discussed initial management plans:
□ Follow-up tests.
□ Examinee asked if the SP had any other questions or concerns.
Sample Closure
Mrs. Clark, it sounds as if your symptoms are due to a migraine headache, so the first thing I will do is prescribe some medications that will alleviate your pain. To ensure that there isn’t something else going on, however, I would like to get a CT scan of your head to rule out a mass or vascular problem as the cause of your headache. A blood test may also show if you have problems other than migraine. Do you have any questions for me?

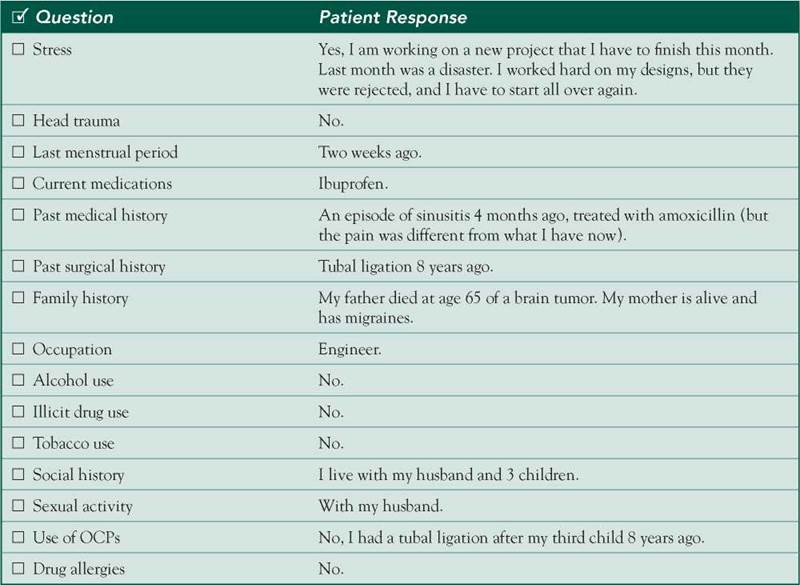
History
HPI: 35 yo F c/o daily headaches for 2 weeks. These headaches occur 2-3 times a day and last for 1-2 hours. The pain is sharp and pounding. The pain is located on the right hemisphere of the head, with no radiation or preceding aura. The pain reaches 9/10 in severity and prevents the patient from continuing her activities. Headaches are exacerbated by stress, light, and noise and are alleviated by resting in a dark room, sleeping, and taking aspirin. The pain is sometimes accompanied by nausea and vomiting. No changes in weight or appetite.
ROS: Occasional aches and pains.
Allergies: NKDA.
Medications: Ibuprofen, aspirin.
PMH: Headaches at age 20, accompanied by nausea. One episode of sinusitis 4 months ago, treated with amoxicillin.
PSH: Tubal ligation 8 years ago.
SH: No smoking, no EtOH, no illicit drugs. Patient is an engineer, lives with husband and 3 children, and is sexually active with husband only.
FH: Father died of a brain tumor at age 65. Mother has migraines.
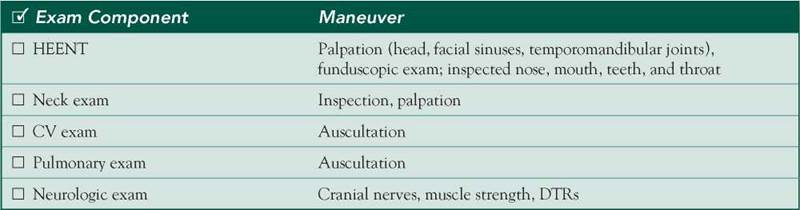
Physical Examination
Patient is in severe pain.
VS: WNL.
HEENT: NC/AT, nontender to palpation, PERRLA, EOMI, no papilledema, no nasal congestion, no pharyngeal erythema or exudates, dentition good.
Neck: Supple, no lymphadenopathy.
Chest: Clear breath sounds bilaterally.
Heart: RRR; normal S1/S2; no murmurs, rubs, or gallops.
Neuro: Mental status: Alert and oriented x 3, good concentration. Cranial nerves: 2-12 grossly intact. Motor: Strength 5/5 throughout. DTRs: 2+ intact, symmetric.
Differential Diagnosis


CASE DISCUSSION
Patient Note Differential Diagnoses
Headaches without neurologic findings on exam are common and have routine causes, but less common pathology should still be considered:
■ Migraine: Despite lacking an aura, the patient’s presentation is classic for this diagnosis. Migraines are more common in women and typically appear as a unilateral headache. They are often associated with aura, nausea, vomiting, and photophobia. A positive family history makes the diagnosis even more likely.
■ Tension headache: This is often associated with stress but is usually bilateral and squeezing. It lasts from hours to days and worsens as the day progresses. Tension headaches are often associated with stress and sleep deprivation.
■ Intracranial mass lesion: One-third of patients with brain tumors present with a primary complaint of headache. Headache is nonspecific and may mimic features of migraine. Certain brain tumors may have a familial basis. The patient’s lack of weight loss or neurologic findings on exam casts doubt on but does not rule out this diagnosis.
Additional Differential Diagnoses
■ Depression: Headaches may be worse on arising in the morning and are associated with other symptoms of depression. The patient also reports stress and rejection at work.
■ Pseudotumor cerebri: In pseudotumor cerebri, headaches may be focal but are usually accompanied by diplopia and other visual symptoms. The physical exam should reveal papilledema but may be normal during the first few days after the onset of illness.
■ Cluster headache: This involves unilateral periorbital pain, often accompanied by ipsilateral nasal congestion, rhinorrhea, lacrimation, redness of the eye, and/or Horner’s syndrome. Episodes of daily pain occur in clusters and often awaken patients at night. However, this rarely occurs in women (a similar entity seen in women is termed chronic paroxysmal hemicrania).
■ Sinusitis: This is a rare cause of headache. Although the patient had a sinus infection several months ago, there are no signs or symptoms of sinus or respiratory infection in this case.
Diagnostic Workup
■ CBC: To look for leukocytosis, a nonspecific sign of infection or inflammation. Mild normocytic anemia and thrombocytosis may also be seen in temporal arteritis.
■ CT—head or MRI—brain: Headache syndromes are largely clinical diagnoses. Neuroimaging is generally reserved for patients with acute severe headache, chronic unexplained headache, or abnormalities on neurologic exam. MRI provides greater anatomic detail, but CT is preferred to rule out acute bleeds.
■ LP: To look for elevated opening pressure in pseudotumor. CSF is otherwise normal. RBCs and xanthochromia can be seen in subarachnoid hemorrhage (perform if suspicion is high despite a negative CT scan).
■ CT—sinus: To look for sinusitis.