DOORWAY INFORMATION
Opening Scenario
Eric Glenn, a 26-year-old male, comes to the office complaining of cough.
Vital Signs
BP: 120/80 mm Hg Temp: 99.9°F (37.7°C)
RR: 15/minute HR: 75/minute, regular
Examinee Tasks
1. Take a focused history.
2. Perform a focused physical exam (do not perform rectal, genitourinary, or female breast exam).
3. Explain your clinical impression and workup plan to the patient.
4. Write the patient note after leaving the room.
Checklist/SP Sheet
Patient Description
Patient is a 26 yo M.
Notes for the SP
■ Cough as the examinee enters the room.
■ Continue coughing every 3-4 minutes during the encounter.
■ Chest auscultation: When asked to take a breath, pretend to inhale while the examinee is listening to your right chest by moving your shoulders up, but do not actually breathe in.
■ Chest palpation: When the examinee palpates your right chest and asks you to say “99,” turn your face to the right side, and say it in a coarse, deep voice.
■ If asked about sputum, ask the examinee, “What does ‘sputum’ mean?”
■ During the encounter, pretend to have a severe attack of coughing. Note whether the examinee offers you a glass of water or a tissue.
Challenging Questions to Ask
“Do I need antibiotics to get better?”
Sample Examinee Response
“Possibly. Antibiotics don’t help with bronchitis because this condition is primarily caused by viruses that are not sensitive to antibiotics. However, if I find that you have bacterial pneumonia, antibiotics will be needed.”
Examinee Checklist
Building the Doctor-Patient Relationship
Entrance
□ Examinee knocked on the door before entering.
□ Examinee introduced self by name.
□ Examinee identified his/her role or position.
□ Examinee correctly used patient’s name.
□ Examinee made eye contact with the SP.
Reflective Listening
□ Examinee asked an open-ended question and actively listened to the response.
□ Examinee asked the SP to list his/her concerns and listened to the response without interrupting.
□ Examinee summarized the SP’s concerns, often using the SP’s own words.
Information Gathering
□ Examinee elicited data efficiently and accurately.
□ Examinee offered the SP a glass of water or a tissue during the severe bout of coughing.

Connecting with the Patient
□ Examinee recognized the SP’s emotions and responded with PEARLS.
Physical Examination
□ Examinee washed his/her hands.
□ Examinee asked permission to start the exam.
□ Examinee used respectful draping.
□ Examinee did not repeat painful maneuvers.

Closure
□ Examinee discussed initial diagnostic impressions.
□ Examinee discussed initial management plans:
□ Follow-up tests.
□ Safe sex practices.
□ HIV testing (and discussed consent).
□ Examinee asked if the SP had any other questions or concerns.
Sample Closure
Mr. Glenn, your cough is most likely due to an infection that can be either bacterial or viral. The chest pain you are experiencing is probably due to irritation of your lung membranes by an infection. Some of these infections can be more common with HIV, and given your sexual history, I recommend that we test for it. Another reason for your cough may be acid reflux, more commonly known as heartburn. We are going to test your blood and sputum and will obtain a chest x-ray to help us make a definitive diagnosis. We may also need to obtain a PPD to test for tuberculosis if your cough is persistent. In the meantime, I strongly recommend that you use condoms during intercourse to prevent STDs such as HIV as well as to prevent unwanted pregnancies. Do you have any questions for me?

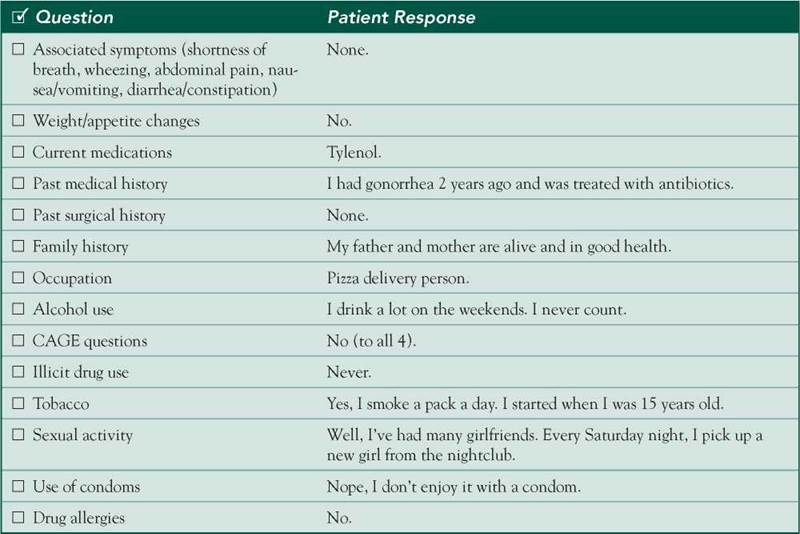
History
HPI: 26 yo M c/o cough x 1 week.
■ 2 weeks ago: fever, rhinorrhea, sore throat.
■ Persistent productive cough with small amount of white mucus but no hemoptysis.
■ Sharp, stabbing 8/10 pain in right chest, exacerbated by cough and deep inspiration.
■ Mild fever.
■ Denies chills, night sweats, SOB, or wheezing.
■ No recent travel.
■ No TB exposure.
■ No weight or appetite changes.
ROS: Negative except as above.
Allergies: NKDA.
Medications: Tylenol.
PMH: Gonorrhea 2 years ago, treated with antibiotics.
SH: 1 PPD since age 15; drinks heavily on weekends. CAGE 0/4. Unprotected sex with multiple female partners.
FH: Noncontributory.
Physical Examination
Patient is in no acute distress.
VS: WNL except for low-grade fever.
HEENT: Nose, mouth, and pharynx WNL.
Neck: No JVD, no lymphadenopathy.
Chest: Increase in tactile fremitus and decrease in breath sounds on the right side. No rhonchi, rales, or wheezing.
Heart: Apical impulse not displaced; RRR; normal S1/S2; no murmurs, rubs, or gallops.
Extremities: No cyanosis or edema.
Differential Diagnosis


CASE DISCUSSION
Patient Note Differential Diagnoses
This young man’s acute productive cough and pleuritic pain are likely caused by a viral respiratory infection or pneumonia. Rarely, severe coughing can lead to a rib fracture, which in turn can cause severe pleuritis.
■ Pneumonia: Pleuritic pain may signal lower respiratory tract infection. This diagnosis is often confirmed by characteristic chest exam findings, which may be difficult to elicit in an otherwise healthy patient. In this patient, increased tactile fremitus suggests airspace consolidation, but there are no bronchial breath sounds or rales to help suggest a focal pneumonia. The absence of dyspnea also argues against this diagnosis.
■ URI-associated cough: Acute cough frequently follows URI (“postinfectious”) and commonly persists for 1-2 weeks (or up to 6-8 weeks in patients with underlying asthma). Causes range from rhinosinusitis to acute bronchitis.
■ Acute bronchitis: Cough can also accompany acute URI. The acute onset of this patient’s symptoms points to an acute, not chronic, bronchitis.
Additional Differential Diagnoses
■ Pleurodynia: An uncommon acute illness usually caused by one of the coxsackieviruses. It occurs in summer and early fall and presents with acute, severe paroxysmal pain of the thorax or abdomen that worsens with cough or breathing. Most patients recover within three days to one week.
■ Other etiologies: Other causes of acute cough include aspiration (for which alcoholic, elderly, and neurologically impaired patients are at risk), pulmonary embolism (extremely rare in a young patient with no risk factors), and pulmonary edema (signs and symptoms of heart failure would be present). Given the patient’s history, he should be screened for HIV infection. Notably, there is no evidence of immunosuppression on exam (eg, no thrush), and in Pneumocystis jiroveci pneumonia, cough is usually nonproductive and accompanied by dyspnea.
Diagnostic Workup
■ CXR: To help diagnose pneumonia (ie, to see infiltrates and effusion), although a normal film does not necessarily rule it out.
■ CBC with differential: In acute infection, can reveal leukopenia or leukocytosis.
■ Sputum Gram stain and culture: Often low yield (due to contamination by oral flora and often discordant results between Gram stain and culture in pneumococcal pneumonia), but may help identify a microbiologic diagnosis in pneumonia.
■ Urine Legionella antigen, serum Mycoplasma PCR, cold agglutinin measurement: To help diagnose specific causes of atypical pneumonia. Seldom useful in the initial evaluation of patients with community- acquired pneumonia.
■ Bronchoscopy with bronchoalveolar lavage: An invasive test that is rarely necessary to diagnose community-acquired pneumonia, but a gold standard that is often used early when P jiroveci infection is suspected.
■ Pulse oximetry or ABG: May help determine the need for hospitalization.
■ HIV antibody: Although HIV is less likely in this scenario, an antibody test should be offered to all patients with risk factors for this infection.