DEFINITION AND EPIDEMIOLOGY
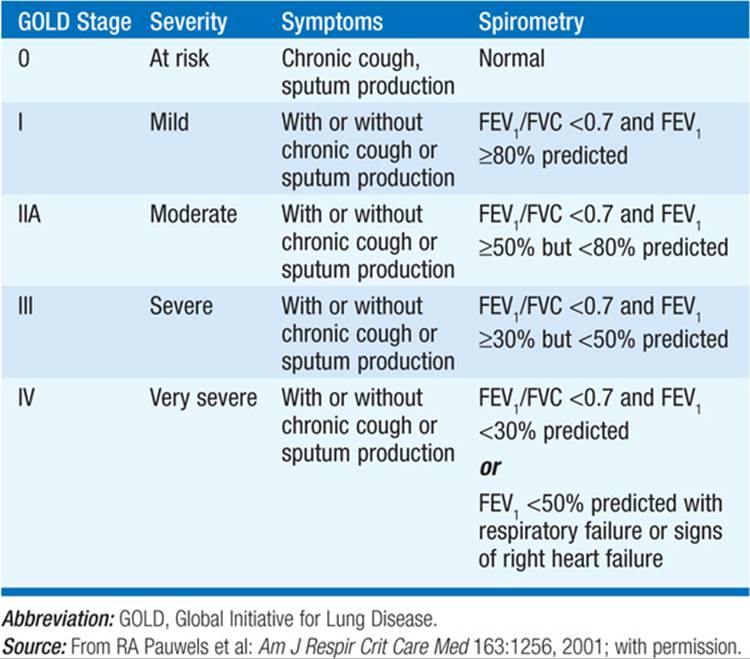
Chronic obstructive pulmonary disease (COPD) is a disease state characterized by chronic airflow obstruction; thus, pulmonary function testing is central to its diagnosis. The presence of airflow obstruction is determined by a reduced ratio of the forced expiratory volume in 1 s (FEV1) to the forced vital capacity (FVC). Among individuals with a reduced FEV1/FVC ratio, the severity of airflow obstruction is determined by the level of reduction in FEV1(Table 140-1): ≥80% is stage I, 50–80% is stage II, 30–50% is stage III, and <30% is stage IV. Cigarette smoking is the major environmental risk factor for COPD. The risk of COPD increases with cigarette smoking intensity, which is typically quantified as pack-years. (One pack of cigarettes smoked per day for 1 year equals 1 pack-year.) Individuals with airway hyperresponsiveness and certain occupational exposures (e.g., coal mining, gold mining, and cotton textiles) are likely also at increased risk for COPD. In countries in which biomass combustion with poor ventilation is used for cooking, an increased risk of COPD among women has been reported. COPD is a progressive disorder; however, the rate of loss of lung function often slows markedly if smoking cessation occurs. In normal individuals, FEV1 reaches a lifetime peak at around age 25 years, enters a plateau phase, and subsequently declines gradually and progressively. Subjects can develop COPD by having reduced maximally attained lung function, shortened plateau phase, or accelerated decline in lung function.
TABLE 140-1 GOLD CRITERIA FOR COPD SEVERITY
Symptoms often occur only when COPD is advanced; thus, early detection requires spirometric testing. The Pao2 typically remains near normal until the FEV1 falls to <50% of the predicted value. Hypercarbia and pulmonary hypertension are most common after FEV1 has fallen to <25% of predicted. COPD pts with similar FEV1 values can vary markedly in their respiratory symptoms and functional impairment. COPD often includes periods of increased respiratory symptoms, such as dyspnea, cough, and phlegm production, which are known as exacerbations. Exacerbations are often triggered by bacterial and/or viral respiratory infections. These exacerbations become more common as COPD severity increases, but some individuals are much more susceptible to developing exacerbations than others with similar degrees of airflow obstruction.
CLINICAL MANIFESTATIONS
History
Subjects with COPD usually have smoked ≥20 pack-years of cigarettes. Common symptoms include cough and phlegm production; individuals with chronic productive cough for 3 months per year for the preceding 2 years have chronic bronchitis. However, chronic bronchitis without airflow obstruction is not included within COPD. Exertional dyspnea is a common and potentially disabling symptom in COPD pts. Exercise involving upper-body activity is especially difficult for severe COPD pts. Weight loss and cachexia are common in advanced disease. Hypoxemia and hypercarbia may result in fluid retention, morning headaches, sleep disruption, erythrocytosis, and cyanosis.
Exacerbations are more frequent as disease progresses and are most often triggered by respiratory infections, often with a bacterial component. The history of prior exacerbations is a strong predictor of future exacerbations.
Physical Findings
The physical examination may be normal until COPD is fairly advanced. As disease progresses, signs of hyperinflation may become more prominent, including barrel chest and poor diaphragmatic excursion. Expiratory wheezing may be observed, but it does not predict the severity of obstruction or response to therapy. Persistently localized wheezing and digital clubbing raise the possibility of lung cancer.
During COPD exacerbations, signs of respiratory distress may be prominent, including tachycardia, tachypnea, use of accessory muscles of respiration, and cyanosis.
Radiographic Findings
Plain chest x-ray may show hyperinflation, emphysema, and pulmonary hypertension. It is typically performed to exclude other disease processes during routine evaluation and to exclude pneumonia during exacerbations. Chest CT scanning has much greater sensitivity for detecting emphysema but is typically reserved for the evaluation of advanced disease when surgical options such as lung volume reduction and lung transplantation are being considered.
Pulmonary Function Tests
Objective documentation of airflow obstruction is essential for diagnosing COPD. Standardized staging of COPD is based on postbronchodilator spirometry. In COPD, the FEV1/FVC ratio is reduced below 0.7. Despite prolonged expiratory efforts, subjects may not be able to achieve a plateau in their FVC. Increases in total lung capacity and residual volume, as well as reduced diffusing capacity for carbon monoxide, are typically seen in emphysema.
Laboratory Tests
α1 Antitrypsin (α1AT) testing, typically by measurement of the protein level in the bloodstream, is recommended to exclude severe α1AT deficiency. Augmentation therapy (a weekly IV infusion) is available for individuals with severe α1AT deficiency (e.g., PI Z). Pulse oximetry can determine the O2 saturation. However, arterial blood gases remain useful to assess the severity of CO2 retention as well as acid-base disorders. During acute exacerbations, arterial blood gases should be considered in pts with mental status changes, significant respiratory distress, very severe COPD, or a history of hypercarbia. Complete blood counts are useful in advanced disease to assess for erythrocytosis, which can occur secondary to hypoxemia, and anemia, which can worsen dyspnea.
TREATMENT COPD
OUTPATIENT MANAGEMENT
Smoking Cessation Elimination of tobacco smoking has been convincingly shown to reduce decline in pulmonary function and to prolong survival in pts with COPD. Although lung function does not typically improve substantially after smoking cessation, the rate of decline in FEV1 often reverts to that of nonsmokers. Pharmacologic treatment to assist with smoking cessation is often beneficial. Use of nicotine replacement therapy (available as a transdermal patch, gum, nasal spray, and oral inhaler) can increase rates of smoking cessation; oral bupropion (150 mg bid after starting at 150 mg qd for 3 days) also produces significant benefit and can be combined successfully with nicotine replacement. Varenicline, a partial agonist for nicotinic acetylcholine receptors, also can promote smoking cessation. All adult, nonpregnant smokers without specific contraindications should be offered pharmacologic treatment to assist with smoking cessation.
Nonpharmacologic Treatment Pulmonary rehabilitation improves dyspnea and functional status and reduces hospitalizations. Annual influenza vaccinations are strongly recommended; in addition, pneumococcal vaccination is recommended.
Bronchodilators Although inhaled bronchodilator medications have not been proven to increase longevity in COPD, they may significantly reduce respiratory symptoms. Short- and long-acting β-adrenergic agonists, short- and long-acting anticholinergics, and theophylline derivatives all may be used. Although oral medications are associated with greater rates of adherence, inhaled medications generally have fewer side effects.
Pts with mild disease can usually be managed with an inhaled short-acting anticholinergic such as ipratropium or a short-acting β agonist such as albuterol. Combination therapy and long-acting β agonists and/or long-acting anticholinergics should be added in pts with severe disease. The narrow toxic-therapeutic ratio of theophylline compounds limits their use, and either low doses or regular monitoring of serum levels are required.
Corticosteroids Chronic systemic corticosteroid treatment is not recommended in COPD pts due to the risk of multiple complications, including osteoporosis, weight gain, cataracts, and diabetes mellitus. Although inhaled steroids have not been proven to reduce the rate of decline of FEV1 in COPD, inhaled steroid medications reduce the frequency of exacerbations in individuals with severe COPD. Combinations of inhaled steroids and long-acting β agonists reduce COPD exacerbations and may reduce mortality—although that has not been conclusively shown.
Oxygen Long-term supplemental oxygen therapy has been shown to reduce symptoms and improve survival in COPD pts who are chronically hypoxemic. Documentation of the need for O2 requires a measurement of Pao2 or oxygen saturation (Sao2) after a period of stability. Pts with a Pao2 ≤55 mmHg or Sao2 ≤88% should receive O2 to raise the Sao2 to ≥90%. O2 is also indicated for pts with Pao2 of 56–59 mmHg or Sao2 ≤89% if associated with signs and symptoms of pulmonary hypertension or cor pulmonale. For individuals who meet these guidelines, continuous O2 therapy is recommended because the number of hours per day of oxygen use is directly related to the mortality benefit. Supplemental oxygen may also be prescribed for selected COPD pts who desaturate only with exercise or during sleep, although the evidence for benefit is less compelling.
Surgical Options for Severe COPD Two main types of surgical options are available for end-stage COPD. Lung volume reduction surgery can reduce mortality and improve lung function in selected pts with upper lobe–predominant emphysema and low exercise capacity (after pulmonary rehabilitation). Individuals who meet the criteria for the high-risk group (FEV1 <20% predicted and either a diffuse distribution of emphysema or lung carbon monoxide diffusing capacity <20% predicted) should not be considered for lung volume reduction surgery. Lung transplantation should be considered for COPD pts who have very severe chronic airflow obstruction and disability at a relatively young age despite maximal medical therapy.
MANAGEMENT OF COPD EXACERBATIONS COPD exacerbations are a major cause of morbidity and mortality. Critical decisions in management include whether hospitalization is required. Although there are no definitive guidelines to determine which COPD pts require hospitalization for an exacerbation, the development of respiratory acidosis, worsening hypoxemia, severe underlying COPD, pneumonia, or social situations without adequate home support for the treatment required should prompt consideration of hospitalization.
Key components of exacerbation treatment include bronchodilators, antibiotics, and short courses of systemic glucocorticoids.
Antibiotics Because bacterial infections often trigger COPD exacerbations, antibiotic therapy should be strongly considered, especially with increased sputum volume or change in sputum color. Common pathogens include Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Antibiotic choice should depend on the local antibiotic sensitivity patterns, previous sputum culture results for a particular pt, and the severity of disease. Trimethoprim-sulfamethoxazole, doxycycline, and amoxicillin are reasonable choices for subjects with mild to moderate COPD; broader-spectrum antibiotics should be considered for subjects with more severe underlying COPD and/or more severe exacerbations.
Bronchodilators Bronchodilator therapy is essential during COPD exacerbations. Short-acting β-adrenergic agonists by inhalation (e.g., albuterol q1–2h) are used; addition of anticholinergics is likely of benefit (e.g., ipratropium q4–6h). Administration of bronchodilators by nebulizer is often used initially because it is easier to administer to pts in respiratory distress. Conversion to metered-dose inhaler administration can be successfully achieved with appropriate training of the pt and staff.
Glucocorticoids Systemic steroids hasten resolution of symptoms and reduce relapses and subsequent exacerbations for up to 6 months. Dosing is not well worked out, but 30–40 mg of prednisone daily (or IV equivalent) is standard, with a total course of 10–14 days. Hyperglycemia is the most commonly reported complication and should be monitored.
Oxygen Hypoxemia often worsens during COPD exacerbations. Supplemental O2 should be administered to maintain Sao2 ≤90%. Very high O2 delivery can worsen hypercarbia, primarily due to increasing ventilation-perfusion mismatch. However, providing adequate O2 to obtain saturation of ~90% is the key goal. Therefore, supplemental O2 delivery should be focused on providing adequate oxygenation without providing unnecessarily high O2saturations. Pts may require use of supplemental O2 after hospital discharge until the exacerbation completely resolves.
Ventilatory Support Numerous studies suggest that noninvasive mask ventilation [noninvasive ventilation (NIV)] can improve outcomes in acute COPD exacerbations with respiratory failure (Paco2 >45 mmHg). Contraindications to NIV include cardiovascular instability, impaired mental status, inability to cooperate, copious secretions, craniofacial abnormalities or facial trauma, extreme obesity, or significant burns. Progressive hypercarbia, refractory hypoxemia, or alterations in mental status that compromise ability to comply with NIV therapy, hemodynamic instability, and respiratory arrest may necessitate endotracheal intubation for mechanical ventilation. Sufficient expiratory time is required to avoid the development of auto-PEEP.

For a more detailed discussion, see Reilly JJ Jr., Silverman EK, Shapiro SD: Chronic Obstructive Pulmonary Disease, Chap. 260, p. 2151, in HPIM-18.