DEFINITION
Chronic and progressive inflammatory disease of the axial skeleton with sacroiliitis (usually bilateral) as its hallmark. Peripheral joints and extraarticular structures may also be affected. Most frequently presents in young men in second or third decade; strong association with histocompatibility antigen HLA-B27.
CLINICAL MANIFESTATIONS
• Back pain and stiffness—not relieved by lying down, often present at night forcing pt to leave bed, worse in the morning, improves with activity, insidious onset, duration >3 months (often called symptoms of “inflammatory” back pain).
• Extraaxial arthritis—hip and shoulders 25–35%, other peripheral joint involvement up to 30%, usually asymmetric.
• Chest pain—from involvement of thoracic skeleton and muscular insertions.
• Extra/juxtaarticular pain—due to “enthesitis”: inflammation at insertion of tendons and ligaments into bone; frequently affects greater trochanter, iliac crests, ischial tuberosities, tibial tubercles, heels.
• Extraarticular findings—include acute anterior uveitis in about 20% of pts, aortitis, aortic insufficiency, GI inflammation, cardiac conduction defects, amyloidosis, bilateral upper lobe pulmonary fibrosis.
• Constitutional symptoms—fever, fatigue, weight loss may occur.
• Neurologic complications—related to spinal fracture/dislocation (can occur with even minor trauma), atlantoaxial subluxation (can lead to spinal cord compression), cauda equina syndrome.
PHYSICAL EXAMINATION
• Tenderness over involved joints
• Diminished chest expansion
• Diminished anterior flexion of lumbar spine (Schober test)
EVALUATION
• Erythrocyte sedimentation rate (ESR) and C-reactive protein elevated in majority.
• Mild anemia.
• Rheumatoid factor and ANA negative.
• HLA-B27 may be helpful in pts with inflammatory back Sx but negative x-rays.
• Radiographs: early may be normal. Sacroiliac joints: usually symmetric; bony erosions with “pseudowidening” followed by fibrosis and ankylosis. Spine: squaring of vertebrae; syndesmophytes; ossification of annulus fibrosis and anterior longitudinal ligament causing “bamboo spine.” Sites of enthesitis may ossify and be visible on x-ray. MRI is procedure of choice when plain radiographs do not reveal sacroiliac abnormalities and can show early intraarticular inflammation, cartilage changes, and bone marrow edema.
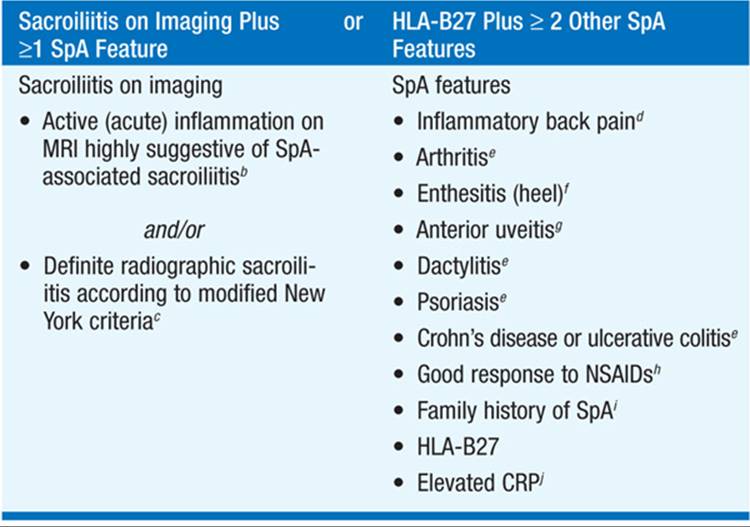
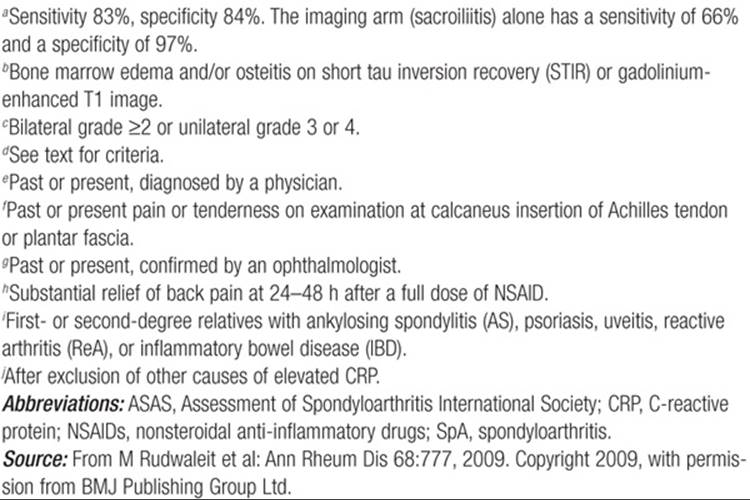
DIAGNOSIS (TABLE 171-1)
TABLE 171-1 ASAS CRITERIA FOR CLASSIFICATION OF AXIAL SPONDYLOARTHRITIS (TO BE APPLIED FOR PATIENTS WITH BACK PAIN ≥3 MONTHS AND AGE OF ONSET <45 YEARS)a
Differential Diagnosis
Spondyloarthropathy associated with reactive arthritis, psoriatic arthritis, enteropathic arthritis (Table 171-2). Diffuse idiopathic skeletal hyperostosis.
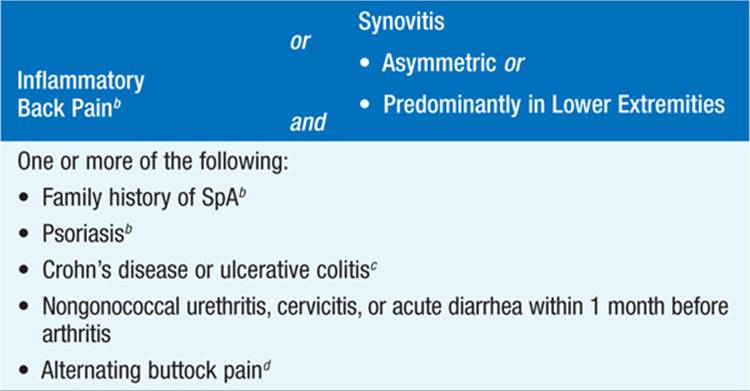
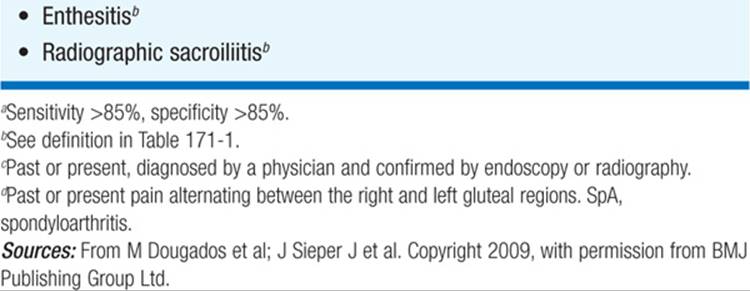
TABLE 171-2 EUROPEAN SPONDYLOARTHROPATHY STUDY GROUP (ESSG) CRITERIA FOR SPONDYLOARTHRITISa
TREATMENT Ankylosing Spondylitis
• Exercise program to maintain posture and mobility is important.
• TNF modulatory agents (etanercept, infliximab, adalimumab, golimumab) have been found to suppress disease activity and improve function.
• NSAIDs (e.g., indomethacin 75 mg slow-release daily or bid) useful in most pts.
• Sulfasalazine 2–3 g/d is of modest benefit, primarily for peripheral arthritis.
• Methotrexate, widely used but has not been of proven benefit.
• No documented therapeutic role for systemic glucocorticoids.
• Intraarticular glucocorticoids for persistent enthesitis or peripheral synovitis; ocular glucocorticoids for uveitis with systemic immuno-suppression required in some cases; surgery for severely affected or deformed joints.

For a more detailed discussion, see Taurog JD: The Spondyloarthritides, Chap. 325, p. 2774, in HPIM-18.