Musculoskeletal complaints are extremely common in outpatient medical practice and are among the leading causes of disability and absenteeism from work. Pain in the joints must be evaluated in a uniform, thorough, and logical fashion to ensure the best chance of accurate diagnosis and to plan appropriate follow-up testing and therapy. Joint pain and swelling may be manifestations of disorders affecting primarily the musculoskeletal system or may reflect systemic disease.
INITIAL ASSESSMENT OF A MUSCULOSKELETAL COMPLAINT (SEE FIG. 53-1)
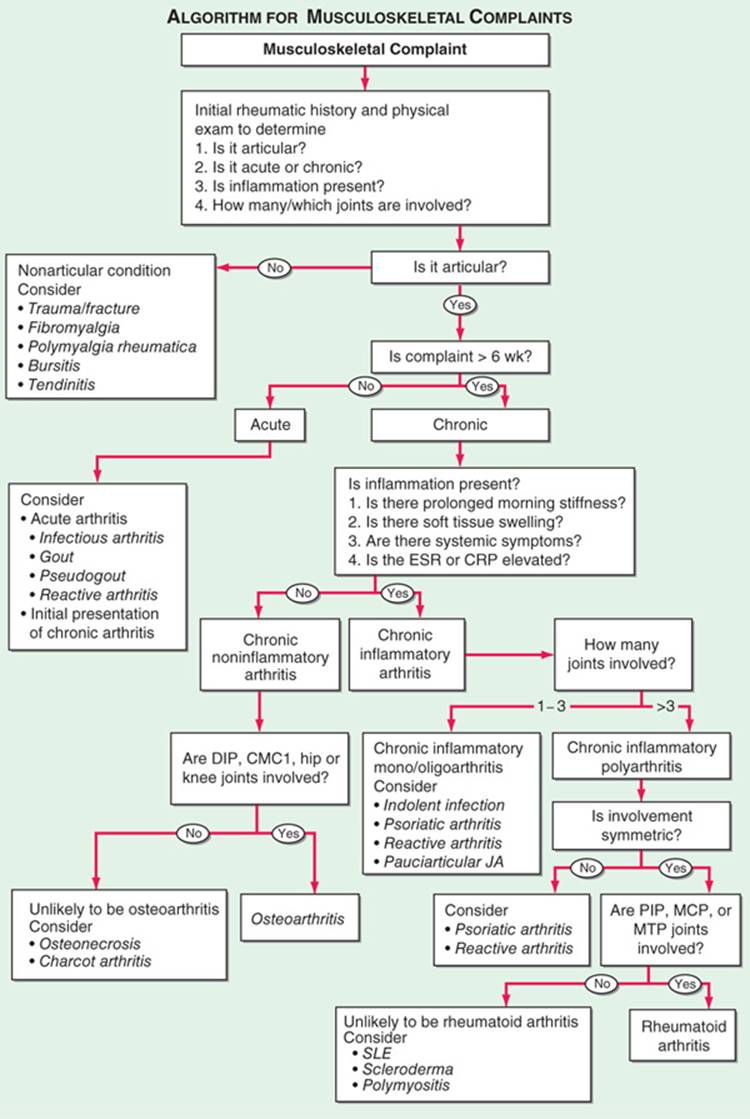
FIGURE 53-1 Algorithm for the diagnosis of musculoskeletal complaints. An approach to formulating a differential diagnosis (shown in italics). CMC, carpometacarpal; CRP, C-reactive protein; DIP, distal interphalangeal; ESR, erythrocyte sedimentation rate; JA, juvenile arthritis; MCP, metacarpophalangeal; MTP, meta-tarsophalangeal; PIP, proximal interphalangeal; SLE, systemic lupus erythematosus.
1. Articular versus nonarticular. Is the pain located in a joint or in a periarticular structure such as soft tissue or muscle?
2. Inflammatory versus noninflammatory. Inflammatory disease is suggested by local signs of inflammation (erythema, warmth, swelling); systemic features (morning stiffness, fatigue, fever, weight loss); or laboratory evidence of inflammation (thrombocytosis, elevated ESR or C-reactive protein).
3. Acute (≤6 weeks) versus chronic.
4. Localized versus systemic.
HISTORIC FEATURES
• Age, sex, race, and family history
• Symptom onset (abrupt or gradual), evolution (chronic constant, intermittent, migratory, additive), and duration (acute versus chronic)
• Number and distribution of involved structures: monarticular (one joint), oligoarticular (2–3 joints), polyarticular (>3 joints); symmetry
• Other articular features: morning stiffness, effect of movement, features that improve/worsen Sx
• Extraarticular Sx: e.g., fever, rash, weight loss, visual change, dyspnea, diarrhea, dysuria, numbness, weakness
• Recent events: e.g., trauma, drug administration, travel, other illnesses
PHYSICAL EXAMINATION
Complete examination is essential: particular attention to skin, mucous membranes, nails (may reveal characteristic pitting in psoriasis), eyes. Careful and thorough examination of involved and uninvolved joints and periarticular structures; this should proceed in an organized fashion from head to foot or from extremities inward toward axial skeleton; special attention should be paid to identifying the presence or absence of:
• Warmth and/or erythema
• Swelling
• Synovial thickening
• Subluxation, dislocation, joint deformity
• Joint instability
• Limitations to active and passive range of motion
• Crepitus
• Periarticular changes
• Muscular changes including weakness, atrophy
LABORATORY INVESTIGATIONS
Additional evaluation usually indicated for monarticular, traumatic, inflammatory, or chronic conditions or for conditions accompanied by neurologic changes or systemic manifestations.
• For all evaluations: include CBC, ESR, or C-reactive protein
• Where there are suggestive clinical features, include: rheumatoid factor, ANA, antineutrophilic cytoplasmic antibodies (ANCA), antistreptolysin O titer, Lyme antibodies
• Where systemic disease is present or suspected: renal/hepatic function tests, UA
• Uric acid: useful only when gout diagnosed and therapy contemplated
• CPK, aldolase: consider with muscle pain, weakness
• Synovial fluid aspiration and analysis: always indicated for acute mon-arthritis or when infectious or crystal-induced arthropathy is suspected. Should be examined for (1) appearance, viscosity; (2) cell count and differential (suspect septic joint if WBC count > 50,000/μL); (3) crystals using polarizing microscope; (4) Gram’s stain, cultures (Fig. 53-2).
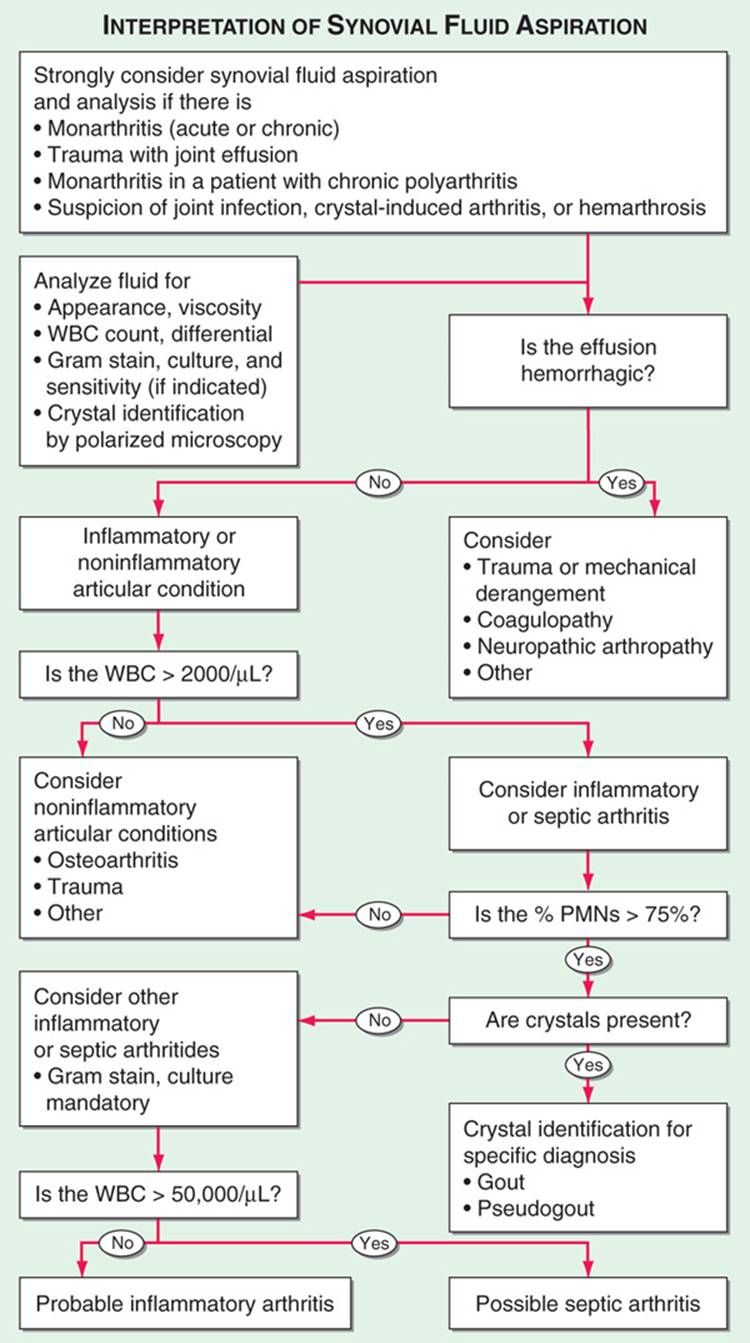
FIGURE 53-2 Algorithmic approach to the use and interpretation of synovial fluid aspiration and analysis. PMNs, polymorphonuclear leukocytes; WBC, white blood cell count.
DIAGNOSTIC IMAGING
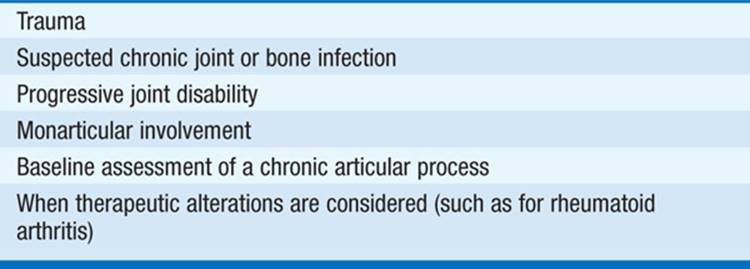
Conventional radiography using plain x-rays is a valuable tool in the diagnosis and staging of articular disorders (Table 53-1).
TABLE 53-1 APPLICATIONS FOR CONVENTIONAL RADIOGRAPHY IN ARTICULAR DISEASE
Additional imaging procedures, including ultrasound, radionuclide scintigraphy, CT, and MRI, may be helpful in selected clinical settings.
SPECIAL CONSIDERATIONS IN THE ELDERLY PATIENT
The evaluation of joint and musculoskeletal disorders in the elderly pt presents a special challenge given the frequently insidious onset and chronicity of disease in this age group, the confounding effect of other medical conditions, and the increased variability of many diagnostic tests in the geriatric population. Although virtually all musculoskeletal conditions may afflict the elderly, certain disorders are especially frequent. Special attention should be paid to identifying the potential rheumatic consequences of intercurrent medical conditions and therapies when evaluating the geriatric pt with musculoskeletal complaints.

For a more detailed discussion, see Cush JJ, Lipsky PE: Approach to Articular and Musculoskeletal Disorders, Chap. 331, p. 2818, in HPIM-18.