POISONOUS SNAKES
Two types of poisonous snakes are indigenous to the United States: pit vipers (rattlesnake, cottonmouth [water moccasin], copperhead) and coral snakes. Their distributions are as follows:
Northeast. Cottonmouth, copperhead, timber rattlesnake.
Southeast. Cottonmouth, copperhead, eastern diamondback rattlesnake, pygmy rattlesnake, eastern coral snake.
Central. Cottonmouth, copperhead, massasauga rattlesnake, timber rattlesnake, prairie rattlesnake.
Southwest. Cottonmouth, copperhead, pygmy rattlesnake, massasauga rattlesnake, northern black-tailed rattlesnake, prairie rattlesnake, sidewinder, Mojave rattlesnake, western diamondback rattlesnake, red diamondback rattlesnake, Texas coral snake, Sonoran coral snake.
Pacific Coast. Northern Pacific rattlesnake, southern Pacific rattlesnake, Great Basin rattlesnake, western diamondback rattlesnake, red diamondback rattlesnake, sidewinder, Mojave rattlesnake.
In the United States, 98% of venomous bites are from pit vipers. In addition, many “nonvenomous” species, such as colubrid (rear-fanged) snakes (including the red-neck keelback), are capable of producing venomous bites. There are no indigenous venomous snakes in Hawaii or Alaska.
Pit vipers are typified by rattlesnakes, which have a characteristic triangular head, vertical elliptical pupils (“cat’s eyes”), two elongated and hinged fangs in the front part of the jaw, heat-sensing (infrared-sensing) facial pits on the sides of the head midway between and below the level of the eyes and the nostrils, a single row of scales on the underbelly leading to the tail (not seen in nonpoisonous snakes), and rattles on the tail (Figure 179). The snake’s age is not determined by the number of rattles, since molting may occur up to four times a year. Because fangs are replaced every 6 to 10 weeks in the adult rattlesnake, bites may demonstrate from one to four large puncture marks. An adult pit viper can strike at a speed of 8 ft (2.4 m) per second. The rattlesnake may strike without a preliminary warning rattle.
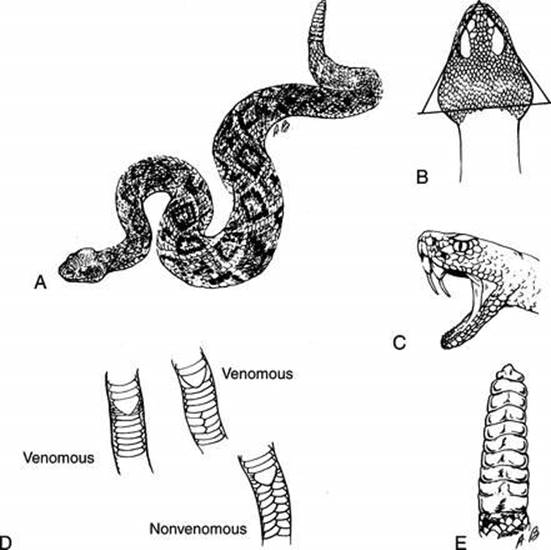
Figure 179 Rattlesnake. Typical rattlesnake appearance (A), with features of identification that include (B) triangular head, (C) hinged fangs, (D) single row of underbelly scales leading up to the anal plate, and (E) a rattle on the tail.
Coral snakes are characterized by their color pattern, with red, black, and yellow or white bands encircling the body (Figure 180). A general rule is “red on yellow—kill a fellow (venomous); red on black—venom lack (nonvenomous).” The fangs are very short and fixed; the snakes have round pupils, and they bite with a chewing, rather than striking, action.
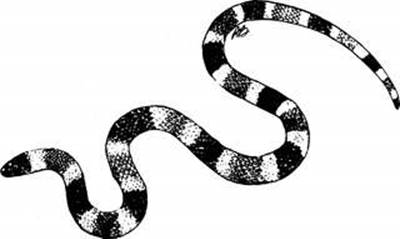
Figure 180 Coral snake.
Signs of Envenomation
Most snakebites do not result in envenomation, because the snake does not release venom, the skin is not penetrated, or the venom is not potent. Therefore, it is important to recognize the signs of envenomation, in order to avoid needless worry, evacuation, and improper therapy.
The most common signs of envenomation are as follows:
Pit Vipers
1. One or more fang marks. Most snakebites (venomous and nonvenomous) will demonstrate rows of markings from the teeth. In the case of venomous snakes, there will be one to four larger distinct markings from the elongated fangs that inoculate the victim with venom (Figure 181). Venomous snakebite wounds tend to bleed more freely than bites from animals and insects.
2. Burning pain at the site of the bite. This may not be present with the bite of the Mojave rattlesnake.
3. Swelling at the site of the bite. This usually begins within 5 to 10 minutes of envenomation and may become quite severe. This may not be present with the bite of the Mojave rattlesnake.
4. Numbness and tingling of the lips, face, fingers, toes, and scalp 30 to 60 minutes after the bite. This can also be present if the victim hyperventilates with fear and excitement (see page 300). If a victim of a snakebite has immediate symptoms, these are likely to be due to hyperventilation.
5. Twitching of the mouth, face, neck, eye, and bitten extremity muscles 30 to 90 minutes after the bite.
6. Rubbery or metallic taste in the mouth 30 to 90 minutes after the bite.
7. Sweating, weakness, nausea, vomiting, and fainting 1 to 2 hours after the bite. Additional symptoms include chest tightness, rapid breathing rate (20 to 25 breaths per minute), rapid heart rate (125 to 175 beats per minute), palpitations, headache, chills, and confusion.
8. Bruising at the site of the bite. This usually begins within 2 to 3 hours. Large blood blisters may develop within 6 to 10 hours.
9. Difficulty breathing, increased bleeding (bruising, bloody urine, bloody bowel movements, vomiting blood), and collapse 6 to 12 hours after the bite.
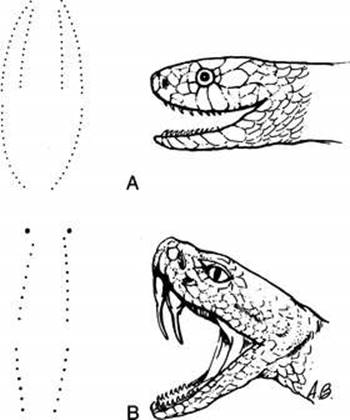
Figure 181 Snakebite patterns. A, Nonvenomous snake. B, Venomous snake.
Coral Snakes
1. Burning pain at the site of the bite may be present or absent. There is generally very little local swelling or bruising, and certainly much less than that seen with the bite of a pit viper.
2. Numbness and/or weakness of a bitten arm or leg within 90 minutes.
3. Twitching, nervousness, drowsiness, giddiness, increased salivation and drooling in 1 to 3 hours. Vomiting may occur.
4. Slurred speech, double vision, difficulty talking and swallowing, and impaired breathing within 5 to 10 hours.
5. Death from heart and lung failure.
Treatment of Snakebite
If a person is bitten by a snake that could be poisonous, act swiftly. The definitive treatment for serious snake venom poisoning is the administration of antivenom. The most important aspect of therapy is to get the victim to an appropriate medical facility as quickly as possible.
1. Don’t panic. Most bites, even by venomous snakes, do not result in medically significant envenomations. Reassure the victim and keep him from acting in an energy-consuming, purposeless fashion. If the victim has been envenomed, increased physical activity may increase his illness by hastening the spread of venom. If the victim is hyperventilating from fear, manage according to the instructions on page 300.
2. Retreat out of the striking range of the snake, which for safety’s sake should be considered to be the snake’s body length (for pit vipers, it is actually approximately half the body length). A rattlesnake can strike at a speed of 8 ft (2.4 m) per second.
3. Locate the snake. If possible, identify the species. If you cannot do this with confidence (which is really only important for the Mojave rattlesnake and coral snake), one can photograph the snake using a digital camera. Do not attempt to capture or kill the snake, for fear of wasting time and perhaps provoking another bite. Never delay transport of the victim to capture a snake. If the snake is dead, take care to handle it with a very long stick or shovel, and to carry the dead animal in a container that will not allow the head of the snake to bite another victim (the jaws can bite in a reflex action for up to 90 minutes after death). If you are not sure how to collect the snake, it is best just to get away from it.
4. Splint the bitten body part, to avoid unnecessary motion. Allow room for swelling within the splint. Maintain the bitten arm or leg in a position of comfort. Remove any jewelry that could become an inadvertent tourniquet.
5. Transport the victim to the nearest hospital.
6. Do not apply ice directly to the wound or immerse the part in ice water. An ice pack placed over the wound (as one would do for a sprain) is of no proven value to retard absorption of venom, but may be useful for pain control. Application of extreme cold can cause an injury similar to frostbite, and possibly lead to enough tissue loss to require amputation.
7. Application of the Extractor Pump (see Figure 204) is controversial. The manufacturer claims that if the device is applied according to the instructions provided, it can remove venom without the need for a skin incision. Animal research appears to refute this notion, and even to suggest that by using the device for a rattlesnake bite, it might cause concentration of tissue-toxic venom under the suction cup, leading to a more severe reaction. Until further notice, the Sawyer Extractor Pump is no longer recommended by snake bite experts.
8. If the victim is more than 2 hours from medical attention, and the bite is on an arm or leg, one may use the pressure immobilization technique (Figure 182): Place a 2 in × 2 in (5 cm × 5 cm) cloth pad (¼ in, or 0.6 cm, thick) over the bite and apply an elastic wrap firmly around the involved limb directly over the padded bite site with a margin of at least 4 to 6 in (10 to 15 cm) on either side of the wound, taking care to check for adequate circulation in the fingers and toes (normal pulses, feeling, and color). An alternative method is to simply wrap the entire limb at the described tightness with an elastic bandage. The wrap is meant to impede absorption of venom into the general circulation by containing it within the compressed tissue and microscopic blood and lymphatic vessels near the limb surface. You should then splint the limb to prevent motion. If the bite is on a hand or arm, also apply a sling. It should be noted that this recommendation is controversial, in that some experts believe that localizing venom in a single area might lead to an increased chance for tissue damage.
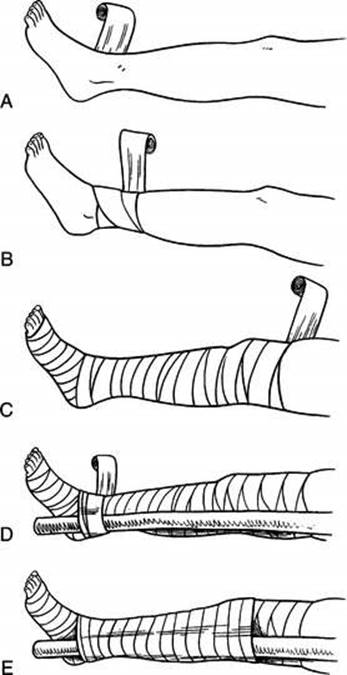
Figure 182 The pressure immobilization technique. A, Begin to wrap the limb directly over the bite site with an elastic bandage. B, Continue wrapping up the limb. C, Wrapped limb. D, Begin to apply a splint. E, Wrapped and splinted limb.
An alternative to the pressure immobilization technique is a constriction band (not a tourniquet) wrapped a few inches closer to the heart than the bite marks on the bitten limb. This should be applied tightly enough to only occlude the superficial veins and lymph passages. To gauge tightness, the rescuer should be able to slip one or two fingers under the band, and normal pulses should be present. The band may be advanced periodically to stay ahead of the swelling. It is of questionable usefulness if 30 minutes have intervened between the time of the bite and the application of the constriction band (or pressure immobilization technique). Again, this recommendation is controversial, for the reasons mentioned in the previous paragraph.
9. The impression of most snakebite experts is that incision and suction are of little value and probably should be abandoned. It appears that little venom can actually be removed from the bite site. Furthermore, the incision may set the stage for inoculation of bacteria, infection, and a poorly healing wound. Mouth contact with the incision may cause a nasty infection that leaves a noticeable scar; there is also the risk of transmission of blood-borne disease to the rescuer.
10. “Snakebite medicine” (whiskey) is of no value and may actually be harmful if it increases circulation to the skin.
11. There is no scientific evidence that electrical shocks applied to snakebites are of any value. On the contrary, there are experiments that refute this concept.
12. The bite wound should be washed vigorously with soap and water, and the victim treated with dicloxacillin, erythromycin, or cephalexin.
13. If the victim is many hours or days from a hospital, assist him to walk out or arrange for a litter rescue, allowing frequent rest periods and adequate oral hydration. Splinting and positioning (e.g., elevating or lowering) the bitten part are secondary to any effort to reach a facility where antivenom can be administered.
Watch for an allergic reaction (see page 66) caused by the snakebite. This might cause the victim to be short of breath with or without an airway obstruction from swelling of the mouth, tongue, and throat. Once the victim is in the hospital, the severity of envenomation will be ascertained, and the victim treated with antivenom if necessary. Such therapy must be carried out under the supervision of a physician, because serious allergic reactions to antivenoms are possible.
Avoidance of Poisonous Snakes
1. Know the behavior and habitats of snakes in your area. Avoid the known habitats of poisonous snakes, such as rocky ledges and woodpiles.
2. Do not reach into areas that you cannot visually examine first. Walk on clearly marked trails, and use a walking stick to move suspicious objects. Do not reach blindly behind rocks. In flooded areas, avoid touching tree limbs and brush.
3. Wear adequate protective clothing, particularly loose-fitting bloused trousers and boots to cover your feet and lower legs.
4. Never hike alone in snake territory. Carry an elastic wrap and a SAM Splint (see page 74).
5. Avoid hiking at night in snake territory. Carry a flashlight and walking stick.
6. Do not handle snakes unless you know what you are doing. Some authorities mention that a defensive bite by a snake may release more venom than an offensive (feeding) bite. You can be bitten and envenomed by seemingly dead or nonvenomous snakes. Stay at least one body length away from a snake.
NONPOISONOUS SNAKES
Many snakes (for example, the gopher snake and king snake) are nonvenomous and do not create serious medical problems with a bite. However, identifying a snake from the bite puncture wounds is often extremely difficult for the amateur. Unless the snake can be positively identified as a nonvenomous species, the victim should be considered to have been bitten by a poisonous snake and managed appropriately. The snake may be very carefully captured or photographed for identification (see page 350). If the snake is absolutely known to be nonvenomous, the wound should be washed vigorously with soap and water, and the victim treated with dicloxacillin, erythromycin, or cephalexin.
Gila Monster and Mexican Beaded Lizard
The Gila monster (Heloderma suspectum) (Figure 183) and Mexican beaded lizard (H. horridum), which can grow to 14 in (35 cm) long, are found in the Great Sonoran Desert area of southern Arizona and northwestern Mexico. They possess grooved teeth and venom glands. Most envenomations occur when an animal bites and holds on, or when a tooth is shed into the bite wound. If the Gila monster holds on, the grip may need to be loosened by mechanical means or incision of the jaw muscles.

Figure 183 Gila monster.
Symptoms of an envenomation include burning pain at the site of the bite, swelling of the bite wound, red or blue discoloration, nausea and vomiting, weakness, anxiety, rapid heart rate, and sweating. Low blood pressure is the most serious complication. Intense pain from the bite may last for 3 to 5 hours, and then subside after 8 hours.
The wound should be washed vigorously and all pieces of teeth removed. The victim should have his arm or leg splinted and should be transported to a hospital. Severe reactions are unusual; most victims recover uneventfully. Be prepared to treat the victim for shock (see page 60). Do not administer alcohol, stimulants, or narcotic pain medicines. Do not apply ice directly to the wound or immerse a bitten limb in ice water.
If it will be more than 24 hours before you can reach medical care, administer an antibiotic (cephalexin, erythromycin, or amoxicillin-clavulanate).