Timur S. Durrani, MD, MPH, MBA
Neal L. Benowitz, MD
Heart disease and stroke cause the majority of deaths in the United States. The major risk factors for coronary heart disease—family history, hypertension, diabetes, lipid abnormalities, and cigarette smoking—explain only a minority of the cases. Other factors, such as stress and exposure to occupational or environmental toxic agents, are believed to contribute to the development of heart disease, although the magnitude of the risk is unknown.
CAUSATION IN TOXIC CARDIOVASCULAR DISEASE
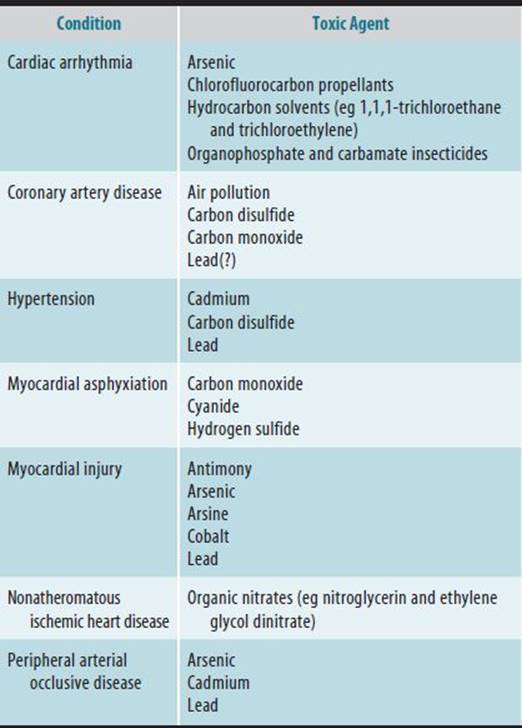
Table 24–1 lists the types and possible toxic causes of cardiovascular disease. Massive exposure may occur (eg, in acute carbon monoxide poisoning), but toxic cardiovascular disease usually is the result of chronic low-level exposures.
Table 24–1. Classification of cardiovascular diseases and possible toxic causes.
Problems in establishing the cause of cardiovascular disease include the following:
• Cardiovascular disease is common even in the absence of toxic exposures.
• There is usually nothing specific, either clinically or pathologically, to point to toxic cardiovascular disease.
• It is rarely possible to document high tissue levels of suspected toxic substances.
• It is difficult to establish occupational exposure levels over the 20 or more years it may take to develop cardiovascular disease.
• Cardiovascular toxic substances are likely to interact with other risk factors in causing or manifesting cardiovascular disease.
With these limitations in mind, this chapter discusses current information concerning toxic cardiovascular disease.
EVALUATION OF PATIENTS
Evaluation of patients with suspected toxic cardiovascular disease should include the following steps:
1. Take a detailed occupational history with attention to the temporal relationship between cardiovascular symptoms and exposure to toxic substances in the workplace.
2. Attempt to document exposure to suspected toxic substances by obtaining industrial hygiene data and, if possible, monitoring worker exposure directly.
3. Evaluate other cardiovascular risk factors.
4. Perform a complete physical examination.
5. Perform appropriate diagnostic studies such as exercise stress testing and coronary angiography to establish the presence and extent of coronary artery disease; echocardiography or radionuclide angiography to establish myocardial disease and the presence of cardiomyopathy; and ambulatory electrocardiographic recordings taken on workdays and at other times to document work-related arrhythmias, paying particular attention to variations in intervals such as PR, QT, and QRS.
CARDIOVASCULAR ABNORMALITIES CAUSED BY CARBON DISULFIDE
Chronic exposure to carbon disulfide appears to accelerate atherosclerosis and/or precipitate acute coronary ischemic events. Carbon disulfide is a widely used solvent, especially in the rubber and viscose rayon industries, in the manufacture of carbon tetrachloride and ammonium salts, and as a degreasing solvent. Early epidemiologic studies indicated that there is a 2.5- to 5-fold increase in the risk of death from coronary heart disease in workers exposed to carbon disulfide. However, more recent analyses of the results of multiple studies found association between carbon disulfide exposure and circulatory disease to be weaker and inconsistent.
![]() Pathogenesis
Pathogenesis
The mechanism of accelerated atherogenesis caused by carbon disulfide has not been proved. One theory is that carbon disulfide reacts with amino- and thiol-containing compounds in the body to produce thiocarbamates, which are capable of complexing trace metals and inhibiting many enzyme systems. This causes metabolic abnormalities such as disturbances of lipid metabolism and thyroid function and can lead to elevations of low-density lipoprotein/cholesterol concentrations and hypothyroidism, which are risk factors for atherosclerosis. Aldehyde dehydrogenase may be inhibited, resulting in a disulfiram-like reaction after alcohol ingestion. Other possible contributors to ischemic heart disease in workers exposed to carbon disulfide are increased vascular permeability, which may lead to greater lipid deposition; interference with normal inhibition of elastase activity, resulting in excess elastase activity with disruption of blood vessel walls and formation of aneurysms; depressed fibrinolytic activity, resulting in a greater tendency to thrombosis; and hypertension.
![]() Pathology
Pathology
The findings are those of accelerated atherosclerotic vascular disease involving the coronary, cerebral, and peripheral arteries. Renovascular hypertension also has been reported.
![]() Clinical Findings
Clinical Findings
A. Symptoms and Signs
Acute intoxication may produce symptoms and signs of encephalopathy or polyneuropathy, including fatigue, headaches, dizziness, disorientation, paresthesias, psychosis, and delirium. In cases of chronic exposure, patients may present with hypertension or manifestations of atherosclerotic vascular disease such as angina or myocardial infarction. An early sign of chronic carbon disulfide poisoning is abnormal ocular microcirculation, characterized by microaneurysms and hemorrhages resembling those of diabetic retinopathy. Disturbed color vision may be reported. Presenile dementia, stroke, and sudden death have been reported in patients with chronic poisoning.
B. Laboratory Findings
Findings may include a decrease in serum thyroxine levels and an increase in serum cholesterol levels, particularly those of the very-low-density lipoproteins. There are no practical methods for measuring carbon disulfide levels in biologic fluids.
C. Cardiovascular Studies
Delayed filling of the retinal arteries, as measured by fluorescein angiography, may be an early sign of vascular disease. The electrocardiogram sometimes shows evidence of ischemia or previous myocardial infarction. The presence of coronary artery disease may be confirmed by exercise stress testing and coronary angiography.
![]() Differential Diagnosis
Differential Diagnosis
The vascular findings in patients with chronic carbon disulfide poisoning are the same as those seen in any patient with atherosclerotic vascular disease. The most specific finding is abnormal ocular microcirculation in the absence of diabetes. The diagnosis is based on a clinical picture of premature vascular disease and a history of exposure to excessive levels of carbon disulfide for more than 5 or 10 years.
![]() Prevention
Prevention
Carbon disulfide exposure is primarily by inhalation. The Occupational Safety and Health Administration (OSHA) recommends that workplace exposure be limited to 20 ppm as an 8-hour time-weighted average (TWA) concentration, 30 ppm as an acceptable peak concentration for 30 minutes, and 100 ppm as a maximum peak. Periodic examination of the ocular fundi may help to detect early signs of vascular disease.
![]() Treatment
Treatment
Treatment consists of removing the worker from sources of carbon disulfide exposure and providing medical measures for atherosclerotic vascular disease.
![]() Course & Prognosis
Course & Prognosis
The course of the disease is similar to that of any atherosclerotic vascular disease. There is evidence of reversibility—at least of ocular changes—after exposure to carbon disulfide is discontinued.
CARDIOVASCULAR ABNORMALITIES CAUSED BY CARBON MONOXIDE
Excessive carbon monoxide exposure can reduce maximal exercise capacity in healthy workers; aggravate angina pectoris, intermittent claudication, and chronic obstructive lung disease; and aggravate or induce cardiac arrhythmias. Acute intoxications can cause myocardial infarction or sudden death. Chronic high-level carbon monoxide exposure may result in congestive cardiomyopathy.
Carbon monoxide is the most widely distributed of all industrial toxic agents and accounts for the greatest number of intoxications and deaths. It is formed wherever combustion engines or other types of combustion are present. Workers at high risk include forklift operators, foundry workers, miners, mechanics, garage attendants, and firefighters. Carbon monoxide poisoning also may occur with the use of faulty furnaces or heaters, particularly improperly vented kerosene or charcoal heaters. Cigarette smoking is an important source of carbon monoxide, and occupational sources may be additive to exposure from cigarettes. The solvent methylene chloride is metabolized within the body to carbon monoxide.
![]() Pathogenesis
Pathogenesis
The affinity of carbon monoxide for hemoglobin is more than 200 times that of oxygen. The binding of carbon monoxide and hemoglobin to form carboxyhemoglobin reduces the delivery of oxygen to body tissues because the oxygen-carrying capacity of hemoglobin is decreased and because less oxygen is released to tissues at any given oxygen tension (ie, there is a shift in the oxygen dissociation curve). Thus, a carboxyhemoglobin concentration of 20% represents a greater reduction in oxygen delivery than a 20% reduction in erythrocyte count. Other heme-containing proteins (eg, myoglobin, cytochrome oxidase, and cytochrome P450) bind 10–15% of the total-body carbon monoxide, but the medical significance of their binding at usual levels of exposure to carbon monoxide is unclear.
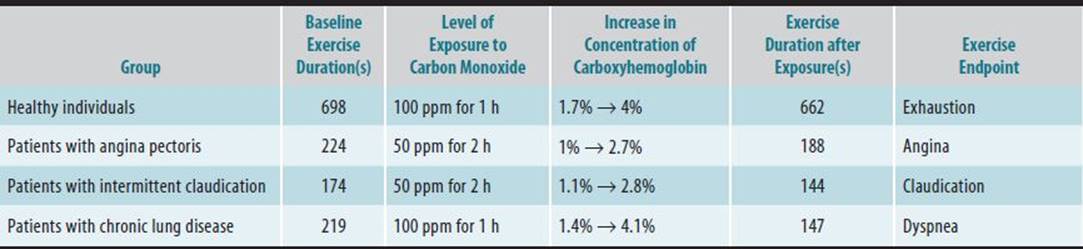
In healthy individuals exposed to carbon monoxide, the decrease in delivery of oxygen to tissues causes the cardiac output and coronary blood flow to increase to meet the metabolic demands of the heart. Although these compensatory responses enable healthy individuals to perform at normal work levels, their maximal exercise capacity is decreased. If, on the other hand, compensatory responses are limited, as in patients with coronary artery disease, carbon monoxide exposure may cause angina or myocardial infarction (Figure 24–1). Reduced exercise thresholds for the development of angina have been reported when carboxyhemoglobin concentrations are as low as 2.7% (Table 24–2). Carbon monoxide decreases the ventricular fibrillation threshold in experimental animals and may do the same in humans. This would explain why sudden death occurs in people who have coronary artery disease and are exposed to carbon monoxide, as has been reported to occur on smoggy days in large cities. Severe carbon monoxide poisoning (carboxyhemoglobin concentrations >50%) can cause severe hypoxic injury, including cardiovascular collapse.
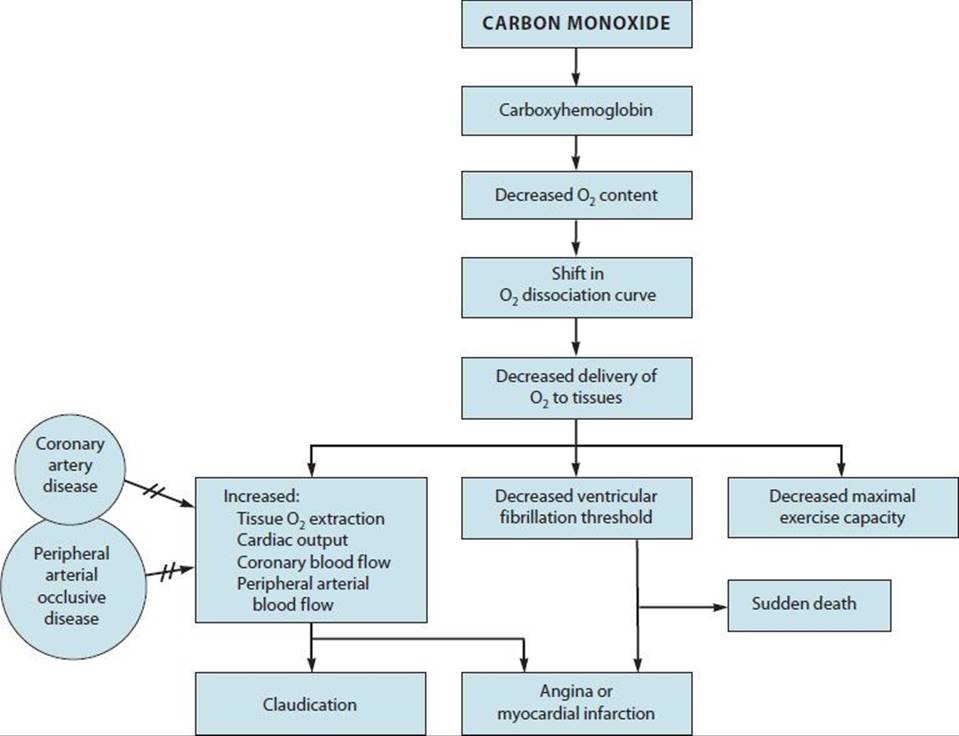
![]() Figure 24–1. Cardiovascular consequences of exposure to carbon monoxide. The presence of coronary artery disease or peripheral arterial occlusive disease prevents (//) the usual compensatory increase in coronary or peripheral arterial blood flow, which results in symptoms of arterial insufficiency.
Figure 24–1. Cardiovascular consequences of exposure to carbon monoxide. The presence of coronary artery disease or peripheral arterial occlusive disease prevents (//) the usual compensatory increase in coronary or peripheral arterial blood flow, which results in symptoms of arterial insufficiency.
Table 24–2. Effects of carbon monoxide on exercise capacity.
Chronic exposure to carbon monoxide is thought to accelerate atherogenesis. Cigarette smokers demonstrate advanced coronary and peripheral atherosclerosis, and carbon monoxide is believed to contribute. Several animal studies have tested the effects of chronic high-level carbon monoxide exposure combined with feeding of atherogenic diets; the results of some of these studies showed increased severity of atherosclerosis. Possible mechanisms include abnormal vascular permeability, increased vascular uptake of lipids, and increased platelet adhesiveness. Whether atherosclerosis is accelerated at levels of carbon monoxide commonly encountered in the workplace is unclear.
Chronic exposure to carbon monoxide results in increased red blood cell mass in response to chronic tissue hypoxia and in increased blood viscosity, which could contribute to acute cardiac events.
![]() Pathology
Pathology
Cardiac necrosis is observed often in cases of fatal carbon monoxide poisoning and presumably is due to severe hypoxia. Myocardial infarction may occur in workers who have coronary artery disease and are exposed to high levels of carbon monoxide, particularly while performing strenuous work or exercise. Cardiomyopathy with cardiac enlargement and congestive heart failure has been described in workers with chronic high-level exposure to carbon monoxide (carboxyhemoglobin concentrations >30%).
![]() Clinical Findings
Clinical Findings
A. Symptoms & Signs
Headache is typically the first symptom of carbon monoxide poisoning and may occur at carboxyhemoglobin concentrations as low as 10%. At higher concentrations, nausea, dizziness, fatigue, and dimmed vision are reported commonly.
In patients with angina pectoris or peripheral arterial occlusive disease, carbon monoxide exposure may reduce exercise capacity to the point of angina or claudication (see Table 24–2). All workers experience a reduction in maximal exercise capacity.
Although symptoms correlate poorly to carboxyhemoglobin levels, neuropsychiatric testing may reveal findings such as increased reaction time and decreased manual dexterity may be seen at carboxyhemoglobin concentrations between 5% and 10%. At concentrations of 25%, there may be decreased visual acuity and impaired cognitive function; at 35%, ataxia; at 50%, vomiting, tachypnea, tachycardia, and hypertension; and at higher levels, coma, convulsions, and cardiovascular and respiratory depression. Myocardial ischemia may be evident at any carboxyhemoglobin concentration in susceptible individuals.
B. Laboratory Findings
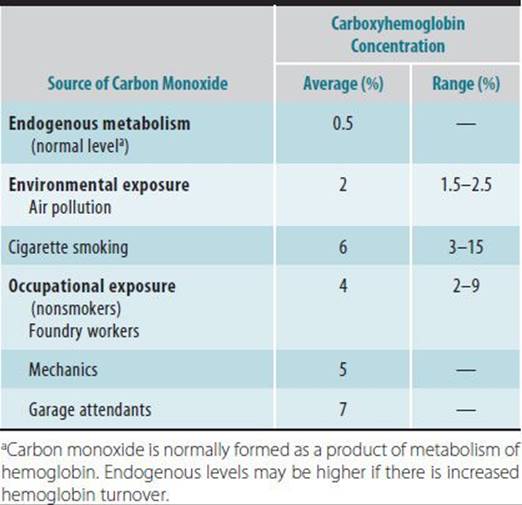
The only finding specific for carbon monoxide intoxication is elevation of the carboxyhemoglobin concentration. Table 24–3 lists normal carboxyhemoglobin concentrations and provides examples of concentrations resulting from exposure to carbon monoxide in the environment and the workplace.
Table 24–3. Normal carboxyhemoglobin concentrations and examples of concentrations resulting from exposure to carbon monoxide in the environment and the workplace.
Measurement of carboxyhemoglobin levels must be done using CO-oximetry with arterial or venous blood. The routine arterial blood gas instruments measures the partial pressure of oxygen dissolved in plasma (Po2), but oxygen saturation is calculated from the Po2 and is therefore unreliable in patients with CO poisoning. Conventional pulse oximetry gives falsely normal readings because it is unable to distinguish between oxyhemoglobin and carboxyhemoglobin. A newer pulse CO-oximeter can detect carboxyhemoglobin.
Although respiratory alkalosis caused by hyperventilation is observed commonly, there is respiratory failure in the most severe poisonings. When there is marked tissue hypoxia, lactic acidosis develops.
C. Cardiovascular Studies
The electrocardiograph (ECG) may show ischemic changes or myocardial infarction. Various types of arrhythmias, including atrial fibrillation and premature atrial and ventricular contractions, are observed. Abnormalities seen on the ECG usually are transient, although ST-T-wave abnormalities may persist for days or weeks.
![]() Differential Diagnosis
Differential Diagnosis
The most important clue to carbon monoxide poisoning is the occupational or environmental exposure history. A typical symptom, such as headache, confusion, or sudden collapse, with findings of myocardial ischemia or metabolic acidosis should suggest the diagnosis, and carboxyhemoglobin concentrations should be measured.
![]() Prevention
Prevention
Levels of carbon monoxide should be monitored if there are sources of combustion such as combustion engines or furnaces in the workplace. The current ACGIH 8-hour threshold limit value is 25 ppm, which at the end of an 8-hour workday results in a carboxyhemoglobin concentration of 2–3%. This concentration is tolerated well by healthy individuals but may impair function in people with cardiovascular or chronic lung disease. Workplace monitoring is done easily with a portable carbon monoxide meter. Biologic monitoring of workers involves measuring either the carboxyhemoglobin concentration in blood or the level of expired carbon monoxide, which is directly proportional to the carboxyhemoglobin concentration. Elevated carbon monoxide levels (as high as 7%) should be anticipated in cigarette smokers.
![]() Treatment
Treatment
Carbon monoxide is eliminated from the body by respiration, and the rate of elimination depends on ventilation, pulmonary blood flow, and inspired oxygen concentration. The half-life of carbon monoxide in a sedentary adult breathing air is 4–5 hours. The half-life can be reduced to 80 minutes by giving 100% oxygen by face mask or to 25 minutes by giving hyperbaric oxygen (3 atm) in a hyperbaric chamber.
![]() Course & Prognosis
Course & Prognosis
Recovery usually is complete after mild to moderate carbon monoxide intoxication in the absence of a cardiac complication such as myocardial infarction.
CARDIOVASCULAR ABNORMALITIES CAUSED BY ORGANIC NITRATES
In the 1950s, an epidemic of sudden death in young munitions workers who hand-packed cartridges of explosives was observed. It was discovered subsequently that abrupt withdrawal from excessive exposure to organic nitrates, particularly nitroglycerin and ethylene glycol dinitrate, may result in myocardial ischemia even in the absence of coronary artery disease. Occupations in which workers may be exposed to organic nitrates include explosives manufacturing, construction work involving blasting, weapons handling in the armed forces, and pharmaceutical manufacturing of nitrates.
![]() Pathogenesis
Pathogenesis
Nitrates directly dilate blood vessels, including those of the coronary circulation. With prolonged exposure (usually 1–4 years), compensatory vasoconstriction develops that is believed to be mediated by sympathetic neural responses, activation of the rennin-angiotensin system, or both. When exposure to nitrates is stopped, the compensatory vasoconstriction becomes unopposed (Figure 24–2). Coronary vasospasm with angina, myocardial infarction, or sudden death may result. Chest pain occurring during nitrate withdrawal has been termed Monday morning angina because it typically occurs 2–3 days after the last day of nitrate exposure. Case-control studies suggest a 2.5- to 4-fold increase in the risk of cardiovascular death in workers handling explosives.
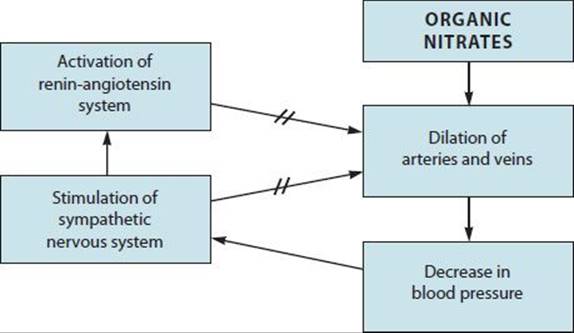
![]() Figure 24–2. Mechanism of vasospasm after withdrawal from chronic exposure to nitrates. Vasoconstrictor forces antagonize (//) nitrate-induced vasodilation. Withdrawal from exposure to nitrates results in unopposed vasoconstriction and in coronary vasospasm.
Figure 24–2. Mechanism of vasospasm after withdrawal from chronic exposure to nitrates. Vasoconstrictor forces antagonize (//) nitrate-induced vasodilation. Withdrawal from exposure to nitrates results in unopposed vasoconstriction and in coronary vasospasm.
![]() Pathology
Pathology
In patients who have died following withdrawal from nitrates, there is often no or minimal coronary atherosclerosis. In one patient, coronary vasospasm was observed during angiography, and the spasm was reversed promptly with sublingual nitroglycerin.
![]() Clinical Findings
Clinical Findings
A. Symptoms & Signs
Workers exposed to excessive levels of nitrates typically experience headaches and have hypotension, tachycardia, and warm, flushed skin. With continued exposure, the symptoms and signs become less prominent. After 1–2 days without exposure to nitrates—generally on weekends—there may be signs of acute coronary ischemia ranging from mild angina at rest to manifestations of myocardial infarction (eg, nausea, diaphoresis, pallor, and palpitations associated with severe chest pain), or sudden death may occur.
B. Laboratory Findings & Cardiovascular Studies
During episodes of pain, the ECG may show evidence of acute ischemia: ST-segment elevation or depression with or without T-wave abnormalities. At other times, in the absence of pain, the ECG may be perfectly normal. Typical findings of myocardial infarction include development of a pathologic Q wave on ECG and elevation of serum troponin and other cardiac enzymes. Results of exercise stress testing and coronary angiography may be normal.
![]() Differential Diagnosis
Differential Diagnosis
Workers chronically exposed to nitrates also may have organic coronary artery disease, which must be identified.
![]() Prevention
Prevention
Nitrates are extremely volatile and are absorbed readily through the lungs and skin. They can permeate the wrapping material of dynamite sticks, so workers who handle dynamite should be advised to wear cotton gloves. Natural rubber gloves should not be used because they tend to become permeated with nitrates and may enhance absorption.
With current automated processes in explosives manufacturing, direct handling of nitrates by employees is minimized. However, levels of nitrates in the workplace environment must be controlled by adequate ventilation and by air conditioning during periods of hot weather. The current OSHA permissible exposure limit (PEL) for nitroglycerin is 0.2 part per million (ppm) parts of air (2 mg/m[3]) as a ceiling limit. The OSHA PEL also bears a “Skin” notation, which indicates that the cutaneous route of exposure (including mucous membranes and eyes) contributes to overall exposure, but even at lower levels (0.02 ppm), personal protective gear is recommended to avoid headache. Although there are no readily available biochemical measures to detect excessive nitrate exposure, findings of progressively decreasing blood pressure and increasing heart rate during the workday are suggestive of excessive exposure. Monitoring for these signs in employees also may help to prevent adverse effects of exposure to nitrates.
![]() Treatment
Treatment
Treatment of myocardial ischemia caused by nitrate withdrawal includes cardiac nitrates (eg, nitroglycerin or isosorbide dinitrate) or calcium entry-blocking agents. Case reports indicate that ischemic symptoms may recur for weeks or months, indicating a persistent tendency to coronary spasm, so long-term cardiac nitrate or calcium blocker therapy may be needed. The worker should be removed from sources of organic nitrate exposure.
![]() Course & Prognosis
Course & Prognosis
In the absence of myocardial infarction or sudden death, anginal symptoms resolve fully after exposure to nitrate is stopped.
CARDIOVASCULAR ABNORMALITIES CAUSED BY HYDROCARBON SOLVENTS & CHLOROFLUOROCARBONS
Exposure to various solvents and propellants may result in cardiac arrhythmia, syncope with resulting accidents at work, or sudden death. Most serious cases of arrhythmia are associated with abuse of or industrial exposure to halogenated hydrocarbon solvents (eg, 1,1,1-trichloroethane and trichloroethylene) or exposure to chlorofluorocarbon (Freon) propellants. Nonhalogenated solvents and even ethanol present similar risks. Dilated cardiomyopathy, with or without histologic evidence of myocarditis, associated with severe cardiac failure has been reported in several people with occupational exposures to solvents, although causation is still unproven.
Exposure to solvents is widespread in industrial settings such as dry cleaning, degreasing, painting, and chemical manufacturing. Chlorofluorocarbons are used extensively as refrigerants and as propellants in a wide variety of products and processes. For example, a pathology resident developed various arrhythmias after exposure to chlorofluorocarbon aerosols used for freezing samples and cleaning slides in a surgical pathology laboratory.
![]() Pathogenesis
Pathogenesis
Figure 24–3 illustrates two ways in which halogenated hydrocarbons and other solvents are thought to induce cardiac arrhythmia or sudden death. First, at low levels of exposure, these solvents “sensitize” the heart to actions of catecholamines. For example, experimental studies show that the amount of epinephrine required to produce ventricular tachycardia or fibrillation is reduced after the solvents are inhaled. Catecholamine release is potentiated by euphoria and excitement as a consequence of inhalation of the solvent, as well as by exercise. This, in combination with asphyxia and hypoxia, causes arrhythmia, which can result in death. Second, at higher levels of exposure, solvents may depress sinus node activity, thereby causing sinus brady-cardia or arrest, or they may depress atrioventricular nodal conduction, thereby causing atrioventricular block. In some cases, they do both. Bradyarrhythmia then predisposes to escape ventricular arrhythmia or, in cases of more severe intoxication, to asystole. The arrhythmogenic action of solvents also may be enhanced by alcohol or caffeine.
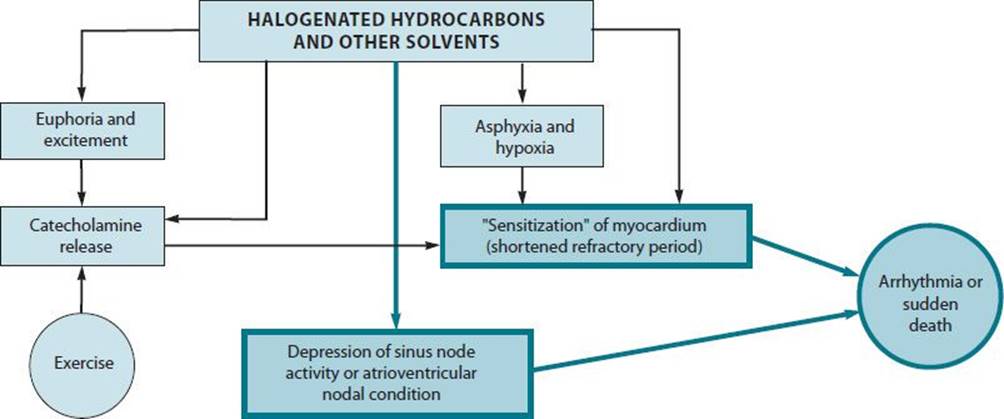
![]() Figure 24–3. Mechanisms of arrhythmia or sudden death following low-level exposure (light arrows) or high-level exposure (heavy arrows) to halogenated hydrocarbons and other solvents.
Figure 24–3. Mechanisms of arrhythmia or sudden death following low-level exposure (light arrows) or high-level exposure (heavy arrows) to halogenated hydrocarbons and other solvents.
![]() Pathology
Pathology
Most cardiovascular deaths following exposure to hydrocarbons are sudden deaths. Autopsies usually reveal no specific pathologic findings in sudden death cases but may reveal myocarditis in cases of dilated cardiomyopathy. The finding of a fatty liver suggests chronic exposure to high levels of halogenated solvents or to ethanol.
![]() Clinical Findings
Clinical Findings
A. Symptoms & Signs
Symptoms of intoxication with hydrocarbon solvents or chlorofluorocarbons include dizziness, light-headedness, headaches, nausea, drowsiness, lethargy, palpitations, and syncope. Physical examination may reveal ataxia, nystagmus, and slurred speech. The heart rate and blood pressure usually are normal, except at the time of arrhythmias, when a rapid or irregular heartbeat sometimes is accompanied by hypotension.
Convulsions, coma, or cardiac arrest may occur in severe cases of exposure to solvents. Workers who have heart disease or chronic lung disease with hypoxemia may be more susceptible to the arrhythmogenic actions of solvents.
B. Laboratory Findings
The concentrations of some hydrocarbons can be measured in expired air or in the blood.
C. Cardiovascular Studies
Arrhythmias induced by solvents or chlorofluorocarbons are expected to occur only at work, while the worker is exposed to these agents. The diagnosis is based on abnormalities observed during ambulatory electrocardiographic monitoring, which consist of one or more of the following: premature atrial or ventricular contractions, recurrent supraventricular tachycardia, and recurrent ventricular tachycardia. It is essential to monitor patients on both workdays and off days and to request a log of times of exposure to solvents or chlorofluorocarbons as well as a log of symptoms of palpitations or dizzy spells. A 12-lead ECG and an exercise stress test can help to determine the presence of coronary artery disease, which might increase sensitivity to hydrocarbon- or chlorofluorocarbon-induced arrhythmia.
![]() Differential Diagnosis
Differential Diagnosis
The diagnosis of solvent- or chlorofluorocarbon-induced arrhythmia is based on exclusion of other causes of arrhythmias at work (eg, the presence of a cardiac disease, metabolic disturbance, or drug abuse) and demonstration of a temporal relationship between episodes of arrhythmia and exposures to the toxic agent. The diagnosis is supported by industrial hygiene measurements documenting the level of exposure in the workplace and by objective and subjective evidence that the worker was intoxicated following exposure.
![]() Prevention
Prevention
Preventive measures include proper handling of solvents and propellants, adequate ventilation in the workplace, and in some cases, the use of protective respiratory equipment. Workers with heart disease—especially those with chronic arrhythmia—should be advised to avoid exposure to potentially arrhythmogenic chemicals.
![]() Treatment
Treatment
If a worker collapses and resuscitation is required, use of epinephrine and other sympathomimetic drugs should be avoided, if possible, because they may precipitate further arrhythmia. β-adrenergic blocking agents may be useful in managing solvent- or chlorofluorocarbon-induced arrhythmias. In cases of episodic arrhythmia, the worker should be removed from excessive exposure or advised to use protective respiratory equipment.
![]() Course & Prognosis
Course & Prognosis
Arrhythmias are expected to resolve fully after exposure to hydrocarbons is stopped.
CARDIOVASCULAR ABNORMALITIES CAUSED BY ORGANOPHOSPHATE & CARBAMATE INSECTICIDES
Early cardiovascular manifestations of intoxication with organophosphate and carbamate insecticides include tachycardia and hypertension. Later, there may be bradycardia and hypotension. Delayed repolarization with QT-interval prolongation and episodes of ventricular tachycardia may be seen for up to 5–7 days after acute intoxication. The ECG also commonly shows nonspecific ST- and T-wave changes. A number of arrhythmias, including premature ventricular contractions, ventricular tachycardia and fibrillation, and heart block and asystole, have been observed.
Intensive cardiac and respiratory monitoring of patients for several days after exposure is recommended, with particular attention to the possible late development of arrhythmia or respiratory failure. High-degree heart block and polymorphous ventricular tachycardia with a prolonged QT interval are treated optimally with cardiac pacing. The use of antiarrhythmic drugs that depress conduction (eg, quinidine, procainamide, and disopyramide) and calcium channel blockers should be avoided.
CARDIOVASCULAR ABNORMALITIES CAUSED BY HEAVY METALS
Several metals are associated with disturbances in cardiovascular function, but their causative role is not fully established.
![]() Antimony
Antimony
Therapeutic use of antimonial compounds for the treatment of parasitic infections produces electrocardiographic abnormalities—primarily T wave changes and QT-interval prolongation—and has caused sudden death in some patients. Electrocardiographic changes also have been observed in workers exposed to antimony. Although these changes usually resolve after removal from exposure, a few studies report increased cardiovascular mortality rates in exposed workers. Studies in animals confirm that chronic exposure to antimony can produce myocardial disease.
![]() Arsenic
Arsenic
Subacute arsenic poisoning caused by ingestion of arsenic-contaminated beer is associated with cardiomyopathy and cardiac failure. Chronic arsenic poisoning has been reported to produce “blackfoot disease,” which is characterized by claudication and gangrene, presumably secondary to spasms of the large blood vessels in the extremities. Arsenic exposure in drinking water is associated with an increased prevalence of hypertension. Acute arsenic poisoning can cause electrocardiographic abnormalities, and in one case it was reported to cause recurrent ventricular arrhythmia of the torsade de pointes type. A mortality study of copper smelters exposed to arsenic indicated that these workers have an increased risk of death as a result of ischemic heart disease.
![]() Arsine
Arsine
Arsine gas causes red blood cell hemolysis. Massive hemolysis produces hyperkalemia, which can result in cardiac arrest. Electrocardiographic manifestations progress from high, peaked T waves to conduction disturbances and various degrees of heart block and then to asystole. Arsine also may directly affect the myocardium, causing a greater magnitude of cardiac failure than would be expected from the degree of anemia.
![]() Cadmium
Cadmium
Some earlier epidemiologic and experimental animal studies linked high-level cadmium exposure with hypertension, but recent epidemiologic studies do not support the association. Environmental exposure to cadmium, as assessed by blood or urine levels, is associated with an increased risk of peripheral arterial disease.
![]() Cobalt
Cobalt
In Quebec City, Canada, in 1965 and 1966, an epidemic of cardiomyopathy occurred in heavy drinkers of beer to which cobalt sulfate had been added as a foam stabilizer. The mortality rate in affected patients was 22%, and a major pathologic finding in those who died was myocardial necrosis with thrombi in the heart and major blood vessels. Other clinical features in affected patients included polycythemia, pericardial effusion, and thyroid hyperplasia. Cobalt is known to depress oxygen uptake by the mitochondria of the heart and to interfere with energy metabolism in a manner biochemically similar to the effects of thiamine deficiency. Because individuals receiving higher doses of cobalt for therapeutic reasons have not developed cardiomyopathy, it is possible that cobalt, excessive alcohol consumption, and nutritional deprivation acted synergistically to produce cardiomyopathy in this epidemic. Occupational exposure to cobalt has been associated with diastolic dysfunction on echocardiography. Several cases of cardiomyopathy in workers exposed to cobalt have been reported.
![]() Lead
Lead
Exposure to excessive levels of lead causes chronic renal diseases, and epidemiologic studies suggest that it also contributes to hypertension in the absence of renal disease. Some of the workplace studies of exposure to lead report an increased incidence of ischemic electrocardiographic changes and an increased risk of hypertensive or coronary artery disease and cerebrovascular disease in exposed workers. Nonspecific electrocardiographic changes and fatal myocarditis in the absence of hypertension have been observed in children with lead poisoning. Cardiomyopathy in moonshine drinkers is also attributed to lead exposure. Studies in animals indicate that lead may have direct toxic effects on the myocardium.
CARDIOVASCULAR ABNORMALITIES CAUSED BY PARTICULATE MATTER
Epidemiologic studies, by using time-series analysis, have demonstrated an association between the level of exposure to air pollution and increased mortality, including increased mortality from cardiovascular disease and stroke. Higher levels of air pollution are associated with more hospital admissions for cardiovascular disease. Several case-control studies of welders have reported increased risk of myocardial infarction and cardiovascular mortality. Welders inhale fumes containing gases and respirable particles (as well as metals such as zinc).
Inhalation of particulates has been shown to alter heart rate variability, with an increase in average heart rate, and to increase plasma viscosity. Gaseous pollutants include oxidizing gases that generate free radicals, which may result in generalized inflammatory responses, endothelial dysfunction, and enhanced blood coagulation. Hemodynamic stress, inflammation, and hypercoagulability are the suspected mechanisms for the link between air pollution and acute cardiovascular events.
REFERENCES
Agarwal S: Heavy metals and cardiovascular disease. Angiology 2011;62:422 [PMID: 21421632].
Alissa EM: Heavy metal poisoning and cardiovascular disease. J Toxicol 2011;2011:870125 [PMID: 21912545].
Gelbke H: A review of health effects of carbon disulfide in viscose industry. Crit Rev Toxicol 2009;39:1 [PMID: 19852562].
Ghiasvand M: Ischemic heart disease risk factors in lead exposed workers. J Occup Med Toxicol 2013;8:11 [PMID: 23607481].
Gilboa SM: Association between maternal occupational exposure to organic solvents and congenital heart defects. Occup Environ Med 2012;69:628 [PMID: 22811060].
Moon K: Arsenic exposure and cardiovascular disease. Curr Atheroscler Rep 2012;14:542 [PMID: 22968315].
Poreba R: Environmental and occupational exposure to lead as a potential risk factor for cardiovascular disease. Environ Toxicol Pharmacol 2011;31:267 [PMID: 21787694]
Vijayakumar S: A prospective study on electrocardiographic findings of patients with organophosphorus poisoning. Cardiovasc Toxicol 2011;11:113 [PMID: 21336997].
![]() SELF-ASSESSMENT QUESTIONS
SELF-ASSESSMENT QUESTIONS
Select the one correct answer for each question.
Question 1: Chronic exposure to carbon disulfide
a. appears to accelerate atherosclerosis and/or precipitate acute coronary ischemic events
b. increases serum thyroxine levels
c. decreases serum cholesterol levels, particularly those of the very-low-density lipoproteins
d. is reliably monitored in biologic fluids
Question 2: Carbon monoxide exposure
a. enhances maximal exercise capacity in healthy workers
b. may aggravate angina pectoris but not intermittent claudication
c. has no effect on chronic obstructive lung disease
d. may aggravate or induce cardiac arrhythmias
Question 3: Nitrates
a. directly constrict blood vessels, including those of the coronary circulation
b. deactivate the rennin-angiotensin system
c. typically cause immediate chest pain
d. appear to cause a 2.5- to 4-fold increase in the risk of cardiovascular death in workers handling explosives
Question 4: Organophosphate and carbamate insecticides
a. can produce diverse cardiovascular disturbances, including tachycardia and hypertension, bradycardia and hypotension, heart block, and ventricular tachycardia
b. stimulate acetylcholinesterase, which causes accumulation of acetylcholine at cholinergic synapses and myoneural junctions
c. typically result in ataxia, nystagmus, and slurred speech
d. invariably result in arrhythmias with chronic exposure
Question 5: Arsine gas
a. causes red blood cell hemolysis
b. leads to hypokalemia resulting in cardiac arrest
c. electrocardiographic manifestations are diagnostic
d. only indirectly affects the myocardium