
Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State
Definition
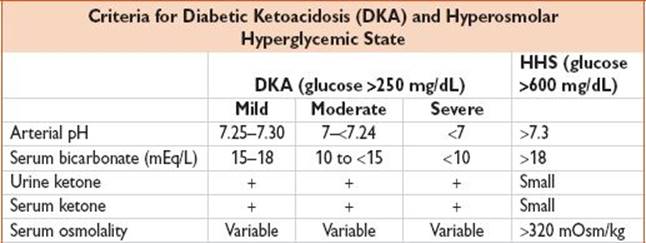
• See above for consensus diagnostic criteria. DKA characterized by uncontrolled hyperglycemia, metabolic acidosis, & increased ketone body concentration. HHS characterized by profound hyperglycemia & serum hyperosmolality, nl arterial pH & bicarbonate, & AMS.
• Marked by insulin deficiency & increased counterregulatory hormones
• HHS generally occurs in Type II diabetes; DKA generally occurs in Type I diabetes, but may occur in Type II diabetes w/ stressors:

History
• DKA often more acute in onset, c/w HHS which evolves over days to weeks
• Polyuria, polydipsia, N/V, dehydration, weight loss, abdominal pain, visual changes, AMS
• Take detailed med hx (see Differential table); consider new meds, med dose changes, incorrect use, intentional/accidental overdose, OTC/naturopathic meds, insulin pump use
• ROS of contrib causes: Fever, chills, cough, abdominal pain, diarrhea, urinary sx, depression
• RFs: Insulin pump users
Physical Exam
• Appears dry, Kussmaul respiration, lethargy, coma; abdominal tenderness (ileus)
Evaluation
• Labs: FSG, Chem 7 (elevated anion gap acidosis, pseudohyponatremia, total body Kμ+μ generally depleted despite lab value), Ca/Mg/Phosphorus, urine/serum ketones, β-hydroxybutyrate, nitroprusside test, UA, CBC, lactate, lipase, LFTs, serum osmolality, VBG, urine hCG; ABG if HD unstable or comatose; blood cultures, urines cultures if clinically indicated

• ECG: If older than 30 yr
• Imaging: CXR (r/o infection); may need abdominal CT or U/S if clinically indicated
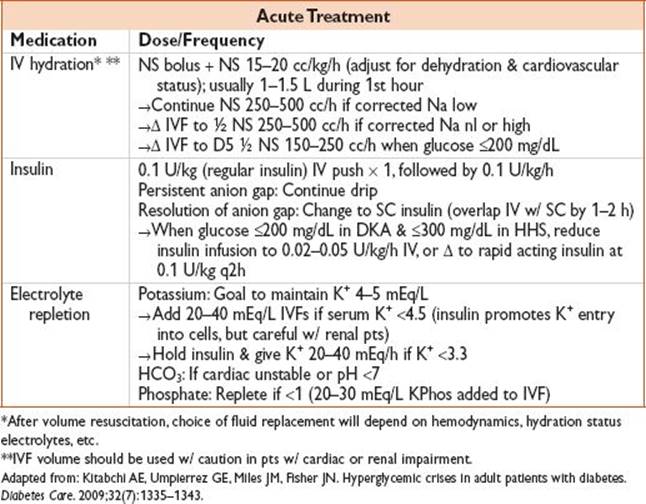
Treatment
• Supportive: Continuous cardiac monitoring, 2 large-bore IVs
• Electrolyte monitoring: Glucose fingerstick q1h; Chem 7, Ca/Mg/Phosphorus, VBG q2–4h
Disposition
• Home: None
• Admit: All pts will require admission, may need ICU monitoring
Pearls
• ∼10% of the DKA population may present w/ glucose ≤250 mg/dL
• An initial insulin bolus may not be necessary as some pts respond to fluid resuscitation
• Consider increasing continuous insulin dose if glucose does not decrease 50–75 mg/dL/h
• Tx w/ SC rapid-acting insulin q1–2h is an effective alternative to IV regular insulin
• Cx: Hypoglycemia, hypokalemia, fluid overload, cerebral edema