INFECTIOUS DISEASES
TUBERCULOSIS
Epidemiology
• U.S.: 10–15 million infected (10× ↑ risk if foreign-born or minority); worldwide: ~2 billion
• After resurgence in U.S. 1984–1992, rates declined, though slower than CDC goals
• Multidrug resistant (MDR) TB: resistant to isoniazid (INH) and rifampin (RIF). Can occur as new (not previously treated) infxn if exposed in former Soviet Republics, Russia, China
• Extensively drug resistant (XDR) TB resistant to INH, RIF, FQ and injectables
• Pts more likely to develop TB disease (NEJM 2011;364:1441)
High-prevalence populations (more likely to be exposed to & infected): immigrant from high-prevalence area, homeless, IDU or medically underserved, resident or worker in jail or long-term facility, HCW at facility w/ TB, close contact to Pt w/ active TB
High-risk populations (infected & likely to progress to active disease): HIV ![]() , immunosupp. incl. biologics, uncontrolled DM & smoking, close contact w/ active TB Pt, underweight, CKD, organ Tx, IVU, EtOH, malnourished, cancer, gastrectomy
, immunosupp. incl. biologics, uncontrolled DM & smoking, close contact w/ active TB Pt, underweight, CKD, organ Tx, IVU, EtOH, malnourished, cancer, gastrectomy
Microbiology & natural history
• Transmission of Mycobacterium tuberculosis via small-particle aerosols (droplet nuclei)
• 90% of infected normal hosts will never develop clinically evident disease
• Localized disease: healing & calcification or progressive 1° TB (at site of infection)
• Hematogenous spread: latent infection ± reactivation TB or progressive dissem. TB
Screening for prior infection
• Whom to screen: high-prevalence and high-risk populations (HIV ![]() Pts should have PPD testing as part of initial evaluation and annually thereafter)
Pts should have PPD testing as part of initial evaluation and annually thereafter)
• How to screen: Mantoux tuberculin test (ie, purified protein derivative or PPD) inject 5-TU (0.1 mL) intermed. strength PPD intradermally → wheal; examine 48–72 h
• How to interpret PPD: determine max. diameter of induration by palpation

• IFN-γ release assays (IGRA): (Ag-stimulated IFN-g release from Pt’s T-cells): can be used for screening where you would use PPD (MMWR 2010;59:1); ↑ Sp, esp. in BCG Rx’d Pts (Annals2008;149:177). Does not distinguish active vs. latent, or recent vs. remote infxn. Relies on host immune fxn; Se limited in immunosupp. Lack of gold standard for latent TB infxn compromises Se/Sp estimates (J Clin Epi 2010;63:257; CID 2011;52:1031).
Clinical manifestations
• Primary TB pneumonia: middle or lower lobe consolidation, ± effusion, ± cavitation
• TB pleurisy: can occur w/ primary or reactivation. Due to breakdown of granuloma w/ spilling of contents into pleural cavity and local inflammation. Pulmonary effusion ± pericardial and peritoneal effusions (tuberculous polyserositis).
• Reactivation TB pulmonary disease: apical infiltrate ± volume loss ± cavitation
• Miliary TB: acute or insidious; due to widespread hematogenous dissemination; usually in immunosupp, DM, EtOH, elderly or malnourished. Constitutional sx (fever, night sweats, weight loss) usually prominent. Pulm disease w/ small millet seed-like lesions (2– 4 mm) on CXR or chest CT (latter more Se) present in 60–80% of those w/ miliary TB.
• Extrapulmonary TB: lymphadenitis, pericarditis, peritonitis, meningitis, nephritis ± sterile pyuria, osteomyelitis (vertebral = Pott’s disease), hepatitis, splenitis, cutaneous, arthritis
• TB and HIV: HIV ![]() at ↑ risk infxn, progressive 1° infxn and reactivation. Risk of progression from infxn to disease >8–10%/y, higher risk with ↓ CD4. Reinfection (also w/ MDR) significant, esp. in hyperendemic areas.
at ↑ risk infxn, progressive 1° infxn and reactivation. Risk of progression from infxn to disease >8–10%/y, higher risk with ↓ CD4. Reinfection (also w/ MDR) significant, esp. in hyperendemic areas.
Diagnostic studies for active TB (high index of suspicion is key!)
• AFB smear (rapid dx) and culture (↑ Se & allows sensitivity testing) of sputum, BAL, pleura, etc.; avoid FQ if considering TB (can compromise dx yield)
• PCR: 94–97% Se c/w smear; 40–77% Se c/w culture (JAMA 2009;301:1014)
• CXR: classically fibrocavitary apical disease in reactivation vs. middle & lower lobe consolidation in 1° TB, but distinction imperfect. HIV ![]() assoc. w/ non-apical disease regardless of timing (JAMA2005;293:2740).
assoc. w/ non-apical disease regardless of timing (JAMA2005;293:2740).
• Adenosine deaminase testing: useful in extrapulmonary sites, best validated for ascites
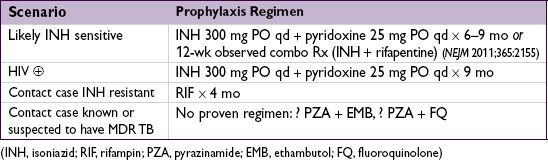
Preventive therapy (Annals 2009;150:ITC6-1; NEJM 2010;362:707)
• Prophylaxis reduces incidence of subsequent disease by 65–75%
• Treat Pts who are ![]() based on guidelines listed above or any exposed HIV
based on guidelines listed above or any exposed HIV ![]() or immunocompromised Pt
or immunocompromised Pt
• R/o active disease in any Pt w/ suggestive s/s before starting INH. If HIV ![]() , routinely ask if cough, fever or night sweats; if yes → ✓ sputum smear, CXR, CD4
, routinely ask if cough, fever or night sweats; if yes → ✓ sputum smear, CXR, CD4
• ✓ LFTs monthly (risk ↑ w/ age; Chest 2005;128:116): if 5× ULN or sx → stop TB meds & reeval
Treatment of active tuberculosis (Annals 2009;150:ITC6-1; NEJM 2013;368:745)
• Isolate Pt per infection control if hospitalized, modified isolation per Dept of Health if outPt
• Use multiple drugs (see below) to which organism susceptible; consult ID before empiric Rx if possible MDR-TB (suspect if prior TB Rx, from or travel to area w/ ↑ rates of MDR, exposure to person w/ likely MDR-TB, poor Rx adherence) or if INH resistance in community ≥4% (includes most of U.S.), extrapulm. TB or HIV ![]() (NEJM 2008;359:636)
(NEJM 2008;359:636)
• Screen for HIV in Pts starting TB Rx; if HIV ![]() , consult ID re: timing of concurrent HIV Rx
, consult ID re: timing of concurrent HIV Rx
• Promote adherence to Rx; directly observed Rx cost-effective if high risk for nonadherence
• Obtain monthly smears/cx on treatment until 2 consecutive are ![]() for TB
for TB
• Monthly clinical evaluation to monitor for Rx response and adverse drug rxns
• “Paradoxical worsening” of sx can occur after starting Rx. More common w/ extrapulm. TB (eg, tuberculoma, LAN) likely due to hypersensitivity response to killing of bacilli. More frequent/severe w/ concurrent immune reconstitution (eg, HIV ![]() Pts started on ARVs, Pts taken off immunosuppress, etc.). Must r/o tx failure (repeat Cx, imaging, etc.).
Pts started on ARVs, Pts taken off immunosuppress, etc.). Must r/o tx failure (repeat Cx, imaging, etc.).

