Khaled El-Ghariani1 & Zbigniew M. Szczepiorkowski2
1NHS Blood and Transplant and Sheffield Teaching Hospitals NHS Trust and University of Sheffield, Sheffield, UK
2Transfusion Medicine Service, Cellular Therapy Center, Dartmouth-Hitchcock Medical Centre and Geisel School of Medicine at Dartmouth, Hanover, New Hampshire, USA
The word apheresis is derived from the Greek meaning ‘a withdrawal’. Therapeutic apheresis is the process of using apheresis technology to manipulate patient's circulatory contents through removal or exchange, to achieve a therapeutic goal. The rationale for this is that it will remove or reduce a substance or substances implicated in the pathology of the disease being treated. Plasma exchange is the process of exchanging part of the patient's plasma with suitable replacement fluid. Different cellular components can be removed with high precision. Red cells can be exchanged, circulating stem cells and lymphocytes can be collected for transplantation and the excess white cells or platelets that are present in myeloproliferative disorders can be removed. Molecules such as low density lipoproteins and immunoglobulins can be specifically removed through the use of adsorption columns. A decision to offer these treatments to patients should be based on factors such as temporary benefits of apheresis, potential adverse effects and the availability and efficacy of other treatment modalities.
Cell separators
Efficient cell separators are currently available. These machines are equipped with sophisticated software and safety alarm systems to detect air and changes in access or inflow pressure. Apheresis technology is based on either filtration or centrifugal systems. Filtration systems use permeable membranes to separate blood into its cellular and noncellular components by subjecting it to sieving through a membrane with suitably sized pores. An example of a filtration system is the Infomed HF440 (Plate 39.1 in the plate section). Centrifugal systems use G forces to separate blood into different components. Centrifugation of blood within apheresis machines results in sedimentation of its components into distinct layers. Based on increasing density, these layers are plasma, platelets, monocytes, lymphocytes and haemopoietic progenitor cells (HPCs), granulocytes and red cells.
Apheresis machines use either continuous- or intermittent-flow technology. In the continuous-flow machines, blood is continuously pumped into a spinning disposable harness where separation takes place and components are either diverted to a collection bag or returned to the patient as required. These machines often require two points of access to the circulation, one for withdrawal and another for return blood to the subject. Examples of continuous-flow systems are Spectra Optia (TerumoBCT) (Plate 39.2 in the plate section), Amicus (Fenwal) and Com.Tec (Fresenius Kabi). Intermittent-flow machines collect blood into a bowl during the draw cycle and then centrifuge it down to separate plasma and cellular components. Different components are diverted to the collection bag or returned to the patient along with replacement fluid during the return cycle. This process requires a single point of access to the circulation. An example of a presently marketed intermittent-flow system is the UVAR XTS (Therakos). Apheresis systems are primed with normal saline to displace air from the harness and also to ensure isovolumia, an important prerequisite for patients with haemodynamic instability or sickle cell disease. In children and small adults, the extracorporeal volume may be relatively high and the system will need to be primed by a mixture of packed red blood cells and normal saline or albumin [1]. Cell separators must be qualified and maintained according to the manufacturer's recommendations and must be operated by trained personnel.
Patient assessment and treatment planning
A physician experienced in the use of cell separators should undertake clinical assessment, to weigh the patient's current health status and expected benefit against potential risks and inconveniences. Plasma exchange often provides relief of the patient's symptoms for variable lengths of time and it is usually only part of the patient's treatment plan. Informed consent must be obtained from all competent patients and from authorized family members when the patient is not able to be consented. Laboratory evaluations before the first procedure should be tailored to the patient's clinical status; these may include a full blood count, coagulation screen and biochemistry. These tests are repeated thereafter as required. Apheresis treatment plans will include the type of vascular access, volume to be exchanged, type of replacement fluid, frequency of procedures and monitoring of response to therapy. Adequate vascular access is crucial. Peripheral veins, usually located in the antecubital fossa, should be evaluated by apheresis staff early in planning and should be used wherever possible, especially for patients requiring a limited number of procedures. Central venous catheterization, though, is associated with an increased risk of complications related to apheresis procedures and is required for patients who have inadequate peripheral veins or who require frequent procedures. A rigid double-lumen catheter should be used. Trained staff must undertake central vein cannulation and postinsertion catheter care [2]. Maximum effort should be exerted to avoid failure of vascular access during the procedure; such failure is associated with disappointment to both patients and staff.
Haemopoietic progenitor cell (HPC) mobilization
Currently, haemopoietic cell transplantation in adults is more commonly undertaken using mobilized peripheral blood (PB) rather than bone marrow as a source of stem cells (see also Chapter 36). This is because HPC, Apheresis [HPC(A)] engrafts faster than marrow and can be harvested without the need for hospital admission or general anaesthesia [3]. In the steady state, HPCs circulate in the peripheral blood, albeit in very low numbers, of less than 0.1% of the total white blood cell count. To ensure adequate graft, mobilization of such cells from the marrow into the peripheral circulation is necessary. Granulocyte colony-stimulating factor (G-CSF) is used to mobilize healthy donors, whereas mobilization of autologous cells can be achieved by growth factors, mainly G-CSF and/or the administration of chemotherapy such as cyclophosphamide or disease-specific combination chemotherapy. Granulocyte-macrophage colony-stimulating factor (GM-CSF) is less effective and more toxic than G-CSF to be used routinely for most donors. The mechanism of HPC mobilization started to unravel revealing involvement of a number of different molecules. One of them is CXCR4 expressed by HPCs among other cells. The ligand of this receptor is stromal-derived factor 1 (SDF-1; CXCL12), which is produced by marrow stromal cells. The association of CXCR4 with its ligand mediates stem cell homing, trafficking and retention. Proteolytic enzymes, such as elastase, cathepsin G and matrix metalloproteinase-g, released from neutrophils following administration of chemotherapy and/or G-CSF, are thought to degrade molecules such as CXCR4 and SDF-1, which are important for anchoring stem cells to marrow stroma and induce mobilization. Also, G-CSF may have an inhibitory effect on expression of CXCR4 mRNA and the reduced expression of CXCR4 receptors enhance mobilization.
Most healthy donors are mobilized by G-CSF at a dose of 10 μg/kg/day. Progenitor cells usually peak after the fourth injection when harvesting starts and the procedure may be repeated until the target number of stem cells is achieved. Donor age, steady-state CD34 levels and the dose of G-CSF may impact on the CD34+ cell mobilization. G-CSF used in healthy donors has proven to be both effective and reasonably safe [4]. The most common symptoms are bone pain, headaches, fatigue and nausea. Reduction in arterial oxygenation has also been noted. Rare but serious effects of G-CSF have been reported. Splenic enlargement is very common and there are a few case reports of splenic rupture, either spontaneously or precipitated by minor trauma or viral infection. Donors are encouraged to report any pain or discomfort that they may experience over the splenic region. G-CSF has a procoagulant effect and may increase the risk of myocardial infarction or ischaemic strokes in susceptible individuals. The effects of G-CSF on genomic stability and possible long-term leukaemogenesis remain unclear; however, this concern justifies long-term follow-up of G-CSF-stimulated donors. Pegylation of G-CSF is a process in which a polyethylene glycol (PEG) moiety is conjugated to a G-CSF molecule. This increases its molecular mass, reduces its renal excretion and prolongs its half-life in excess of 30 hours. Data are accumulating to support the use of one or two injections of pegylated G-CSF to mobilize autologous stem cells [5]. Two branded forms of G-CSF (Granocyte and Neupogen) have been available since the early 1990s. Extensive data are available concerning their safety. Recently G-CSF biosimilar agents have become available. These are alternative biological versions of G-CSF with significantly lower cost. The long-term safety of biosimilars is not yet known and therefore their use in mobilizing allogeneic donors is not recommended [6].
The response of individuals to mobilization regimens is variable and some donors fail to mobilize enough HPCs into circulation, to allow collection of an adequate graft. Such poor mobilization is more common in autologous than allogeneic donors. Stem cell damage due to old age, previous exposure to chemotherapy and radiotherapy, or disease involvement of bone marrow is associated with poor mobilization in autologous donors. Stem cell toxic agents such as melphalan and carmustine and other commonly used chemotherapy agents such as fludarabine and lenalidomide are specifically known to impair mobilization. The percentage of donors who mobilize poorly varies widely between published studies. This is most likely due to inconsistency in the definition of poor mobilization and the differences in the donor groups studied. Patterns of donors' responses to mobilization treatment are likely to continue to change in the future, depending on changes in types of diseases treated, the patients' age profiles and comorbidities. Also, the effects of new cancer treatments need to be defined. A few reports suggested that therapies such as rituximab and bortezomib may not adversely affect mobilization. The mechanism of poor mobilization in healthy donors is unclear. However, experiments in mice have suggested a genetic control of the vigour and timing of mobilization. Individuals who prove to be hard to mobilize may respond favourably to mobilization at a later date or by using different mobilization treatment. If clinically indicated, it is worth undertaking further mobilization attempts in such individuals. Table 39.1 lists the options available to manage poor mobilization.
Table 39.1 Management options for poor mobilization.
|
1. Patients should be considered for stem cell mobilization and harvesting, if required, early in the course of their illness and before stem cell toxic agents are used in their treatment. 2. Leucocytapheresis is repeated daily for several days and a larger blood volume is processed to maximize yield. Leucocytapheresis may be started at a lower CD34+ cells count (e.g. 5–10 × 106/μL) in patients who are likely to be hard to mobilize. 3. Salvage plerixafor is introduced the day before the planned first day of apheresis if the CD34+ cell count and total leucocyte count predict mobilization failure. 4. Mobilization is repeated at a later date to allow marrow recovery using higher dose G-CSF ± chemotherapy ± plerixafor. Cells obtained from two mobilization attempts are likely to be adequate. 5. New agents such as stem cell factor (ancestim) could be used, ideally within the context of a clinical trial to evaluate this approach [21]. 6. Marginally low numbers of stem cells are accepted for transplantation. 7. Bone marrow is harvested instead. However, bone marrow from poor mobilizers may not be of good enough quality and delayed engraftment may follow. |
Plerixafor (Mozobil) is a CXCR4 antagonist that blocks this receptor reversibly and inhibits its interaction with SDF-1. This leads to HPC release into the circulation. Plerixafor synergizes with G-CSF and is usually administered the night before the planned first day of collection, at 240 μg/m2 subcutaneous injection. The introduction of plerixafor has provided clinical practice with a safe and effective new mobilizing agent [7,8]. Although current use of plerixafor is limited by increased drug cost, its judicious use in an appropriately selected patient population has been proven to be cost effective [9] and the drug has been approved by the US Food and Drug Administration (FDA) and the European Medicine Evaluation Agency (EMEA) for autologous HPC donations for patients with myeloma and non-Hodgkin's lymphoma. Because most patients are good mobilizers, the universal use of plerixafor is not justified. Plerixafor could be used in patients who have previously failed mobilization with a success rate of up to 70% [10]. However, use of plerixafor during the first mobilization of selected high risk patients could be more helpful by eliminating the need for a second mobilization, reducing the number of apheresis sessions required and avoiding delays in transplantation. This could be achieved by adopting a ‘just-in-time’ policy where patients' total leucocyte (white blood count) and blood CD34+ cell counts are monitored. Those with high leucocyte count (e.g. >10 × 109/L) and low CD34+ cell count (e.g. <15 × 106/μl) would be identified as potential mobilization failure and given plerixafor during their first mobilization attempt [11].
PB HPC collection (leucocytapheresis)
Leucocytapheresis, following chemotherapy and G-CSF mobilization, could commence when leucocyte counts are rising (≥1 × 109/L). However, currently, most centres use surface expression of CD34 on PB cells, measured by flow cytometry, to predict the optimal time to start HPC collection, to predict the success of collection and to enumerate HPC in the collected product [12]. CD34 is a heavily glycosylated phosphoglycoprotein expressed on progenitor cells of all lineages within the lymphohaemopoietic system, but not on mature cells. Endothelial progenitors, marrow stromal cells and osteoclasts also express CD34. Approximately, 1.5% of aspirated normal marrow mononuclear cells, less than 0.1% of nonmobilized PB and approximately 0.5% of cord blood cells are CD34+. The function of CD34 molecules remains elusive; however, analysis of its structure indicates that these molecules may have a role in cellular signal transduction and/or cell adhesion. CD34 is a surrogate marker for stem cells. Purified autologous CD34+ cells mediate haemopoietic engraftment whereas CD34– cells do not engraft. There is a clear correlation between the number of CD34+ cells infused and the rate of subsequent recovery of both neutrophils and platelets posttransplant [13]. Compared with marrow harvests, G-CSF mobilized grafts contain three- to fourfold higher CD34+ cells and about a 10- to 20-fold increase in CD3+ T cells. An optimal number of infused HPC(A) required for transplantation is not fully defined. However, to ensure timely engraftment and graft survival, there is a consensus to infuse at least 2.0 × 106/kg recipient body weight of CD34+ cells for autologous transplant and 4 × 106/kg of recipient body weight for allogeneic transplant [13]. A higher allogeneic cell number is required with increased HLA disparity between donor and recipient. In addition, a higher number of cells should be collected if tandem transplant or graft manipulation is contemplated. The maximum number of cells to be infused is not defined. However, in the autologous setting, the inconvenience and cost of harvesting of much higher cell numbers are not justified by improvement of clinical outcome. In some studies, infusion of very high numbers of allogeneic cells was found to be associated with a higher risk of extensive chronic graft-versus-host disease (GVHD) [13].
Administration of G-CSF just before leucocytapheresis should be avoided. G-CSF injections are usually followed by temporary reduction of circulating stem cells lasting for about 4 hours. The optimal harvesting time is between 4 and 12 hours after subcutaneous injection of G-CSF. Serial measurement of PB CD34+ cell count in autologous donors is usually obtained as soon as their total leucocyte approaches 1 × 109/L. Collection, started at a level of 20 CD34+ cells/μl, gives the best yield. However, collection may also start at 10/μL or even 5/μL in donors who may not mobilize so well. Healthy donors usually follow a more predicted course and their peak mobilization is usually reached at day 5, after four G-CSF injections. Some donors require further injections either because of delayed mobilization or because not enough cells were collected at the first collection.
Collection of HPC(A) is a technically challenging procedure and different machines collect cells with different efficiency and selectivity. Machine efficiency is measured by the percentage of CD34+ cells that can be collected at a specific peripheral CD34+ cell count. The collected yield can be enhanced by the machine's ability to process more volumes of donor blood within a reasonable period of time and without inconvenience to the donor. Selective machines manage to target HPC(A) with less contamination by other unwanted blood cells. This reduces platelets and red cell contamination of the harvest, which is important in two respects: first, such contamination affects stem cell cryopreservation and may increase infusion complications and, second, collection of other cells such as platelets may lead to thrombocytopenia in the donor.
Apheresis units should observe good manufacturing practice and qualify new machines against published data, as well as against existing equipment, to ensure that new technologies are safe and convenient to the donors, as well as able to meet required product specifications [14]. This is particularly important in cases where the unit deals with special donor groups such as children, or heavily pretreated autologous patients, who tend to mobilize poorly.
There are other important operational features of apheresis machines that should be taken into consideration. The volume of the end product should be optimized to minimize the amount of dimethylsulfoxide (DMSO) yet maximize viability of HPCs during transport and storage. Smaller volumes are easy to cryopreserve, require a smaller storage space and are associated with less DMSO infusion toxicity. However, it is equally important that the contamination of the final product with granulocytes is minimized, as they were shown to be the primary cause of infusion-related adverse reactions. Machines that have smaller extracorporeal volumes are less likely to cause transient anaemia and hypovolaemia in small subjects and children and so avert the need to prime with blood. Machines that are using a single point of access (i.e. single needle) to circulation are usually associated with an ability to process a smaller volume of blood and so give a lower yield of CD34+ cells.
Several machines, such as COBE Spectra, COBE Spectra Optia, Amicus (Fenwal) and Com.Tec (Fresenius Kabi), are able to collect stem cells with different efficiencies and selectivity. COBE Spectra is a commonly used apheresis machine. A new development of this technology, Spectra Optia is found to be at least equally efficient but also less sensitive to changes in blood flow due to less than optimal venous access. This machine, similarly to already marketed for this use Amicus and Com.Tec, is automated and has small end harvest and extracorporeal volumes [14].
A total of 2–3 patient blood volumes are usually processed by the apheresis machine at each leucocytapheresis procedure. Large-volume leucocytapheresis (processing of 3–6 blood volumes over a longer period of time or by increasing the blood flow into the apheresis machine) has been tried and shown to collect significantly higher CD34+ yields. This may reduce the number of leucocytapheresis procedures required and also limit exposure to G-CSF [15]. Although this practice is associated with donor inconvenience, citrate toxicity and platelet loss, it has been used successfully and extensively – particularly for allogeneic donors.
Plasma exchange
Plasma exchange is an effective treatment for many conditions, mainly immune in nature. Exchanging patient's plasma is associated with removal of a pathological substance or substances; an example is immunoglobulin in situations of hyperviscosity or autoimmune disorders such as myasthenia gravis. The removed plasma is most commonly replaced with human albumin solution (HAS) of 4.5%. (In the USA, it is called human serum albumin and is usually 5%). Up to one-third of the exchange volume can be replaced by normal saline if the patient's starting albumin level is normal; otherwise hypotension and/or peripheral oedema may follow. HAS is used because it provides the necessary oncotic pressure with fewer allergic reactions and an impressive safety record with regard to infection transmission. In other clinical scenarios, the exchange process is required not only to remove factors implicated in the disease pathogenesis but also to replace necessary plasma constituents. In thrombotic thrombocytopenic purpura (TTP), for example, plasma exchange removes autoantibodies to the von Willebrand factor-cleaving protease, an important enzyme otherwise known as ADAMTS13, and the associated ultralarge von Willebrand factor multimers. Plasma exchange is also required to replace the missing ADAMTS13; hence fresh frozen plasma (FFP) is used as a replacement fluid for TTP. Solvent detergent plasma is the recommended replacement fluid for TTP in the UK, while in the USA this product is not currently available. Clotting factors may also require replacement during the course of plasma exchange. A therapeutic dose of FFP (10–15 ml/kg) may be included as the last replacement fluid to be infused in cases where repeated exchange with albumin has depleted clotting factors in patients at a high risk of bleeding.
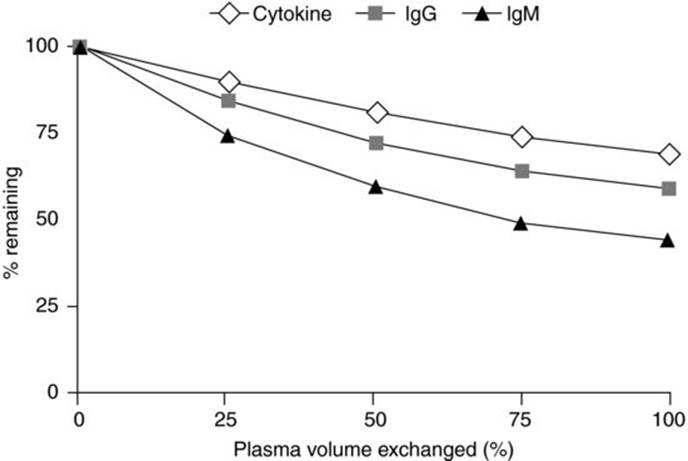
Plasma exchange treatment plans include determination of the amount of plasma to be exchanged in relation to the patient's estimated plasma volume and how to space the procedures to ensure efficiency. An exchange of 1.0–1.5 of the patient's plasma volume will exchange 63–78% of their plasma and is therapeutically effective in most situations. Larger volume exchange is associated with inconvenience, use of larger amounts of replacement fluid and brings little extra benefit (Figure 39.1) [16]. The frequency and total number of exchanges depend on the disease being treated and on the patient's response. Hyperviscosity, TTP and Goodpasture's syndrome require daily exchanges; others may respond to a course, e.g. five exchanges over 7–10 days.
Fig 39.1 Kinetics of plasma exchange. Reproduced with permission from El-Ghariani and Unsworth [16].
Response to treatment varies between patients. Criteria to monitor response to treatment should be agreed early in the treatment plan to avoid undertreatment, overtreatment or the continuation of ineffective treatment. TTP is monitored by measuring the platelet count and other parameters of haemolysis whilst Guillain–Barré syndrome and myasthenia gravis are assessed by clinical neurological improvement. Evidence is accumulating regarding the effectiveness, or otherwise, of different apheresis procedures to treat various disease processes (Table 39.2). The American Society for Apheresis (ASFA) publishes a guideline document every 3 years with assignment of ASFA Category (I to IV) and Recommendation Grade for different diseases [17].
Table 39.2 Disorders for which apheresis is accepted as first-line therapy, either as a stand-alone treatment or in conjunction with other modes of treatment (ASFA Category I indications®). Adapted from the American Society for Apheresis guidelines, 5th edition and Szczepiorkowski ZM et al. J Clin Apheresis2010, 25: 83–177 [17].
|
Plasma exchange |
|
Thrombotic thrombocytopenic purpura |
|
Hyperviscosity in monoclonal gammopathies |
|
Cryoglobulinemia |
|
Antiglomerular basement membrane disease (Goodpasture's syndrome) |
|
Myasthenia gravis |
|
Paraproteinemic polyneuropathies (IgG/IgA) |
|
Guillain–Barré syndrome |
|
Chronic inflammatory demyelinating polyradiculoneuropathy |
|
Red cell exchange |
|
Life- and organ-threatening sickle cell crisis |
|
Photopheresis |
|
Erythrodermic cutaneous T-cell lymphoma |
|
Heart transplant rejection prophylaxis |
|
Selective lipid removal (usually by adsorption column) for homozygote familial hypercholesterolemia |
|
Leucocytapheresis for hyperleucocytosis causing leucostasis |
Although large randomized trials support the use of plasma exchange in the treatment of Guillain–Barré syndrome, intravenous immunoglobulin (IVIG) is equally effective. Given the ease of administration, IVIG is usually a first-choice therapy. However, either of the two treatment modalities can be used if the other fails. Chronic inflammatory demyelinating polyneuropathy also responds to both plasma exchange and IVIG and the former can be used for maintenance treatment. In myasthenia gravis, plasma exchange has a clear therapeutic effect; however, the disease control is temporary and may be followed by a rebound. Plasma exchange is used to treat emergencies such as respiratory failure or swallowing difficulties and to prepare patients for thymectomy. Plasma exchange must be accompanied by an appropriate immunosuppressive regime if it is to be of long-term benefit in myasthenia gravis.
Paraproteinaemia causing clinically evident and progressive hyperviscosity syndrome is a medical emergency requiring urgent plasma exchange to lower the concentration of the responsible paraprotein. IgM, the largest immunoglobulin and mostly intravascular, is most likely to cause hyperviscosity. IgA and IgG3 tend to aggregate and, after IgM, are more likely than other isotypes or subclasses to be associated with hyperviscosity. One to three treatments will usually alleviate symptoms long enough for chemotherapy to take effect. These patients are often severely anaemic. They should not be transfused until the viscosity has been lowered as a rise in haematocrit can precipitate a serious worsening of their symptoms. Plasma exchange can also be life saving in cryoglobulinaemia associated with a fulminant clinical picture. Replacement fluids should always be warmed. At the same time, the cause of the cryoglobulinaemia must be determined and definitive chemotherapy instituted if appropriate. Plasma exchange plays a limited role in the treatment of autoimmune cytopenia; however, it is the treatment of choice for TTP and should be started as soon as the diagnosis is strongly suspected. Daily plasma exchange is needed for at least 2 days after the platelet count has returned to normal (i.e. over 150 × 109/L) and lactate dehydrogenase (LDH) is within the normal range. Plasma infusion can also be used to treat TTP if plasma exchange is not immediately available.
Plasma exchange is required as an adjuvant therapy in antiglomerular basement membrane disease (Goodpasture's syndrome). In the presence of pulmonary haemorrhage, it is important not to overload the patient with replacement fluids as this may provoke further bleeding. Plasma exchange may be used in certain cases of pauci-immune rapidly progressive glomerulonephritis and systemic vasculitis. Such cases need to be discussed with a specialist. Plasma exchange has no proven role in the management of systemic lupus erythematosus nephritis (SLE) or uncomplicated rheumatoid arthritis.
Red cell exchange
Red cell exchange involves the removal of a patient's red cells and concomitant infusion of allogeneic donor cells. This procedure, evolved as a manual procedure, can be performed by apheresis machines and is most commonly used to treat sickle cell disease and some parasitic infections such as malaria or babesiosis. A major advantage of this automated procedure is the isovolaemic nature of the exchange, which is important in preventing further complications occurring. A single red cell volume exchange removes approximately 60% of the red cells originally present in the patient's circulation. The patient's haematocrit, the fraction of the patient's red cells to be left in circulation after the exchange, the desirable final haematocrit and the haematocrit of the replacement fluid can be entered into the apheresis device's software, which then calculates the volume of red cells to be removed and estimates the volume of red cells to be used as replacement.
Exchange using normal red cells as a replacement fluid is beneficial in the treatment and prevention of certain sickle cell crises. Exchange should aim at raising the haemoglobin A to 70–80% to avoid further vasoclusive crises and treat the ongoing one. However, the final haematocrit following exchange should not exceed 30%. Hyperviscosity, associated with a higher haematocrit, is associated with a reduction in oxygen delivery. Neurological events after partial exchange, usually for priapism, have been observed and thought to be due to high end haemoglobin levels, a situation also known as ASPEN syndrome (an eponym for association of sickle cell disease, priapism, exchange transfusion and neurological events coined by Siegel et al. in 1993 [18]). Red cell exchange may not shorten an uncomplicated painful sickle cell crisis but may be considered in severe and frequent debilitating crises. A patient who survives an acute ischaemic stroke could be maintained on a regular exchange programme to prevent recurrence. For acute chest syndrome, life- or organ-threatening complications, red cell exchange can provide rapid reduction of sickle haemoglobin and is less likely to cause iron accumulation. Red cell exchange in sickle cell disease is associated with concerns such as increased requirement of allogeneic blood, which is associated with the risk of red cell alloimmunization.
Red cell exchange is an adjuvant therapy that should be considered for severely ill patients with malaria if parasitaemia is more than 10% or if the patient has severe malaria manifested by altered mental status, nonvolume overload pulmonary oedema or renal complications. Treatment is discontinued after achieving ≤5% residual parasitaemia. Absolute erythrocytosis causing hyperviscosity, thromboembolism or bleeding should be treated by tackling its primary cause and possibly by phlebotomy to maintain a normal haematocrit. However, erythrocytapheresis is also used to treat certain patients with polycythaemia, where removed red cells are replaced with albumin or saline to maintain isovolemia. This procedure is particularly useful in patients with polycythaemia vera, complicated by acute thromboembolism, severe microvascular complications or bleeding, especially if the patient is haemodynamically unstable.
Extracorporeal photochemotherapy (photopheresis)
Extracorporeal photochemotherapy (ECP) is a process in which the patient's mononuclear cells (MNC) are collected and exposed to ultraviolet A light (UVA) in the presence of photoactivating agents such as 8-methoxypsoralen (8-MOP). This process brings about immunomodulation, which can be therapeutically beneficial to patients with advanced cutaneous T-cell lymphoma (CTCL), GVHD and cardiac transplant rejection [19]. The mechanism of action of ECP is not fully understood; however, ECP induces lymphocyte apoptosis, which leads to changes in cytokine secretion patterns, more tolerant antigen presenting cells (APCs), induction of Treg cells and suppression of CD8+ effector cells. Interestingly, ECP does not lead to an increased incidence of opportunistic infection, a feature that is particularly useful in patients with extensive skin lesions. ECP can be best achieved by collecting MNC using a specialized cell separator such as the THERAKOSTM CELLEXTM system (most commonly used in the UK and USA). This machine delivers a calculated UVA radiation dose into the MNC suspension pretreated with 8-MOP, before returning the cells to the patient's circulation. Heparin and, less commonly, ACD-A are used as anticoagulants. Alternatively, ECP can be completed using a combination of a cell separator to collect leucocytes, 8-MOP is added to the apheresis product and the suspension is then exposed to UVA using an irradiation source (UV light box), such as the UV-matic irradiator and then re-infused. This practice is commonly used in Europe, but strict adherence to good manufacturing practice (GMP) regulations for re-infused products is required. ECP is contraindicated in the presence of psoralen hypersensitivity.
There is some evidence for the use of ECP in erythrodermic CTCL and steroid-refractory GVHD, but randomized controlled studies are needed. There is good evidence supporting the use of ECP in preventing cardiac rejection following transplantation. Randomized controlled trials have also shown a therapeutic benefit in type 1 diabetes mellitus, but the inconvenience associated with the procedure outweighs the clinical benefit. Patients with advanced CTCL (stage III/IV) typically receive ECP on two consecutive days once per month. For the management of chronic GVHD, an accelerated regime has been used to gain rapid control of the disease with two consecutive treatments administered initially every 2 weeks. In the USA often a higher frequency of two procedures per week for 12 weeks is used. ECP is a treatment option for patients with steroid refractory acute GVHD [20].
Complications of therapeutic apheresis
Complications occur in up to 10% of procedures; most are mild but, rarely, serious complications including deaths have been reported. Given the advances in technology, machine-related problems are unusual. Failure of the machine that will prevent red cell return can result in red cell loss of up to 200 ml of blood in newer instruments while up to 350 ml in older instruments. Central catheter-related complications, such as pneumothorax, internal bleeding, thrombosis and infections, are more common and can be serious. Allergic reactions to replacement fluids are uncommon but can be significant. These include anaphylactic reactions, hypotension and urticarial rashes. Reactions to HAS are now rare as the preparations contain lower amounts of significant contaminants than previously, especially of vasoactive kinins. HAS essentially carries no risk of infection and it does not increase the citrate return. Dilution of coagulation factors can occur following repeated plasma exchanges and may require the addition of FFP to the replacement fluid. FFP poses the risk of bloodborne infection (although virally inactivated products are now available), allergic reactions and also contributes to the citrate load as it contains approximately 14% citrate anticoagulant by volume. Side effects of the citrate anticoagulant, almost universally used, are particularly common. These result from hypocalcaemia and include paraesthesiae (digital and perioral), abdominal cramps and, rarely, cardiac dysrhythmias and seizures. Citrate toxicity usually responds to simple measures such as slowing the rate of return and providing extra calcium orally. Intravenous calcium may be required. Patients with renal failure who are receiving large amounts of citrate during plasma exchange may develop a profound metabolic alkalosis. Patients receiving repeated treatments over a long period of time can lose significant quantities of calcium. Complications during therapeutic apheresis may arise from underlying pathology or comorbidity. It is important that the clinical status is assessed prior to exchange. Where risks are increased, but benefit is likely, a suitable location for the procedure such as a high dependency unit may be required.
Key points
1. A physician experienced in the use of cell separators should assess the patient's need to have a therapeutic apheresis procedure taking into consideration potential risks and inconvenience.
2. Adequate vascular access is crucial. Central venous catheterization needs to be undertaken by trained staff to minimize risks to patients.
3. G-CSF with or without chemotherapy is currently the gold standard for HPC mobilization.
4. Donors who prove to be hard to mobilize may respond favourably to the addition of plerixafor to the G-CSF mobilization protocol.
5. Human albumin solution (4.5%) is the most commonly used replacement fluid for plasma exchange. Occasionally, plasma, possibly solvent detergent product, is needed.
6. Photopheresis induces immunomodulation without immunosuppression and is indicated for certain stages of cutaneous T-cell lymphoma, GVHD and solid organ transplant rejection.
References
1. Kim HC. Therapeutic apheresis in pediatric patients. In: BC Mcleod, ZM Szczepiorkowski, R Weinstein et al. (eds), Apheresis Priniciples and Practice, 3rd edn. Bethesda, MD: AABB Press; 2010.
2. Guidance on the use of ultrasound locating devices for placing central venous catheters, National Institute for Clinical Excellence, September 2002, ISBN: 1-84257-213-X. Available at: http://www.nice.org.uk.
3. To LB, Roberts MM, Haylock DN et al. Comparison of haematological recovery times and supportive care requirements of autologous recovery phase peripheral blood stem cell transplants, autologous bone marrow transplants and allogeneic bone marrow transplants. Bone Marrow Transplantation 1992; 9(4): 277–284.
4. Pulsipher MA, Chitphakdithai P, Miller JP et al. Adverse events among 2408 unrelated donors of peripheral blood stem cells: results of a prospective trial from the National Marrow Donor Program. Blood 2009; 113: 3604–3611.
5. Tricot G, Barlogie B & Zangari M. Mobilization of peripheral blood stem cells in myloma with either pegfilgrastim or filgrastim following chemotherapy. Haematologica 2008; 93: 1739–1742.
6. Shaw BE, Confer DL, Hwang WY et al. Concerns about the use of biosimilar granulocyte colony-stimulating factors for the mobilization of stem cells in normal donors: position of the World Marrow Donor Association. Haematologica 2011; 96(7): 942–947.
7. Di Persio JF, Micallef IN, Stiff PJ et al. Phase III prospective randomized double-blind placebo-controlled trial of plerixafor plus granulocyte colony-stimulating factor compared with placebo plus granulocyte colony-stimulating factor for autologous stem-cell mobilization and transplantation for patients with non-Hodgkin's lymphoma. J Clin Oncol 2009; 27(28): 4767–4773.
8. Di Persio JF, Stadtmauer EA, Nademanee A et al. Plerixafor and G-CSF versus placebo and G-CSF to mobilize hematopoietic stem cells for autologous stem cell transplantation in patients with multiple myeloma, Blood 2009; 113(23): 5720–5726.
9. Costa LJ, Alexander ET & Hogan KR. Development and validation of a decision-making algorithm to guide the use of plerixafor for autologous hematopoietic stem cell mobilization. Bone Marrow Transplantation 2010; 46: 64–69.
10. Durate RF, Shaw BE, Marin P et al. Plerixafor plus granulocyte CSF can mobilize hematopoietic stem cells from multiple myeloma and lymphoma patients failing previous mobilization attempts: EU compassionate use data. Bone Marrow Transplantation 2011; 46: 52–58.
11. Li J, Hamilton E, Vaughn L et al. Effective and cost analysis of ‘just-in-time’ salvage plerixafor administration in autologous transplant patients with poor stem cell mobilization kinetics. Transfusion 2011; 51: 2175–2182.
12. Gutensohn K, Magens MM, Kuehnl P et al. Increasing the economic efficacy of peripheral blood progenitor cell collections by monitoring peripheral blood CD34+ concentrations. Transfusion 2010; 50(3): 656–662.
13. Heimfeld S. HLA-identical stem cell transplantation: is there an optimal CD34 cell dose? Bone Marrow Transplantation 2003; 31: 839–845.
14. Reinhardt P, Brauninger S, Bialleck H et al. Automatic interface-control apheresis collection of stem/progenitor cells: results from an autologous donor validation trial of a novel stem cell apheresis device. Transfusion 2011, 51(6): 1321–1330.
15. Abrahamsen JF, Stamnesfet S & Liseth K. Large-volume leukopheresis yields more viable CD34+ cells and colony-forming units than normal-volume leukopheresis, especially in patients who mobilize low numbers of CD34+ cells. Transfusion 2005; 45: 248–253.
16. El-Ghariani K & Unsworth DJ. Therapeutic apheresis – plasmapheresis. Clin Med 2006; (4): 343–347.
17. Szczepiorkowski ZM, Winters JL, Bandarenko N et al. Guideline on the use of therapeutic apheresis in clinical practice – evidence-based approach from the Apheresis Applications Committee of the American Society for Apheresis. J Clin Apheresis 2010; 25: 83–177.
18. Siegel JF, Rich MA & Brock WA. Association of sickle cell disease, priapism, exchange transfusion and neurological events: ASPEN syndrome. J Urology 1993; 150(5 Pt 1): 1480–1482.
19. McKenna KE, Whittaker S, Rhodes LE et al. Evidence-based practice of photopheresis 1987–2001: a report of a workshop of the British Photodermatology Group and the UK Skin Lymphoma Group. Br J Dermatol 2006; 154: 7–20.
20. Perfetti P, Carlier P, Strada P et al. Extracorporal photopheresis for the treatment of steroid refractory acute GVHD. Bone Marrow Transplantation 2008, 42: 609–617.
21. Lapierre V, Rossi J-F, Azar N et al. Ancestim (r-metHu SCF) plus filgrastim and/or chemotherapy for mobilization of blood progenitors in 513 poorly mobilizing cancer patients: the French compassionate experience. Bone Marrow Transplantation 2011, 46: 936–942.
Further reading
Bensinger W, DiPersio JF & McCarty JM. Improving stem cell mobilization strategies: future directions. Bone Marrow Transplantation 2009, 43: 181–195.
Cashen AF, Lazarus HM & Devine SM. Mobilizing stem cells from normal donors: is it possible to improve upon G-CSF? Bone Marrow Transplant 2007; 39: 577–588.
George JN. How I treat patients with thrombotic thrombocytopenic purpura. Blood 2010, 116: 4060–4069.
Gertz MA. Current status of stem cell mobilization. Br J Haematol 2010; 150: 647–662.
Scarisbrick J. Extracorporeal photopheresis: what is it and when should it be used? Clin Expl Dermatol 2009; 34: 757–760.
Scarisbrick JJ, Taylor P, Holtick U et al. UK consensus statement on the use of extracorporeal photopheresis for treatment of cutaneous T-cell lymphoma and chronic graft-versus-host disease. Br J Dermatol 2008; 158(4): 659–678.
Siddiq S, Pamphilon D, Brunskill S et al. Bone marrow harvest versus peripheral stem cell collection for haemopoietic stem cell donation in healthy donors. Cochrane Database Syst Rev 2009, Issue 1: CD006406. DOI: 10.1002/14651858. CD006406.pub2.
To LB, Leversque J-P & Herbert KE. How I treat patients who mobilize hematopoietic stem cells poorly. Blood 2011; 118: 4530–4540.