Mark L. Willenbring, MD
CHAPTER OUTLINE
■ DEVELOPMENT OF MODERN APPROACHES TO TREATMENT
■ THE SPECTRUM OF HEAVY DRINKING AND ALCOHOL USE DISORDERS
■ TYPES OF TREATMENT AND TREATMENT EFFECTIVENESS
■ INTEGRATING THE EVIDENCE AND PERSONALIZING PRACTICE
■ SUMMARY AND CONCLUSIONS
Attempts to change the course and consequences of heavy drinking undoubtedly started soon after the discovery that fermenting grain or fruit yielded a drink that changed the way humans felt and behaved, since some of them behaved badly. Throughout most of history, personal, moral, social, and legal methods have comprised the tools available for this task. Other than purely custodial care, professional treatment for alcohol use disorder (AUD) is a relatively recent addition, beginning with the promulgation of professional treatment programs in the latter part of the 20th century. Research concerning the nature and course of AUD and the efficacy of various treatments has grown considerably since then, providing a growing evidence base for clinicians. Consequently, the evidence base upon which addiction medicine rests is considerable, as good as or better than that for many other common complex disorders. At the same time, recent research advances have led to a reconsideration of some basic assumptions upon which treatment and research have been based. New research inspired by this reconsideration will likely lead to development of new and innovative approaches for treating AUD. It is likely that the number and effectiveness of treatments available for treating AUD will increase significantly in the next decade.
This enthusiasm is tempered by limitations of the infrastructure for providing treatment and implementing new treatments when they become available. Treatments are only effective if they are accessible and acceptable to those with the disorder. Very few people, only about one in eight, who develop DSM-IV alcohol dependence ever sought or received treatment in an addiction treatment center* (1,2). In addition, most treatment offered lasts a few weeks for a disorder that often lasts years. This limits the population level impact of treatment and means that many people suffer needlessly. A related but independent challenge is lack of implementation of new research findings and treatments in clinical settings. The addiction treatment system is not configured to facilitate implementation of new treatments (3,4), and the quality of care for heavy drinking and AUD in general medical settings is among the worst in health care (5). Although not the focus of this chapter, these limitations are so important that any discussion about treatment must consider them and how to overcome them. Unless these barriers are addressed, treatment for AUD will have a small impact on the burden of heavy drinking and AUD in our society.
This chapter provides an overview of current research on treatment for heavy drinking and AUD. The various behavioral and pharmacologic treatments are addressed in detail in other chapters. Consequently, the goal of this overview is to provide a context to help guide interpretation of the research and guidelines provided in other chapters. There are four sections. First, I briefly review recent historical trends in research on change in drinking behavior, including a discussion of different ways to assess outcome. Second, I present a framework for conceptualizing heavy drinking and AUD severity along a spectrum, and I propose a continuum of care that corresponds to the spectrum of disorder. The changes in diagnosis from DSM-IVto DSM-5 will be addressed here as well. The question of how to define a goal of treatment for different stages of disorder is raised. Third, I briefly discuss overall treatment effectiveness and address the question of what causes change in drinking behavior. Finally, I examine the challenge of applying research findings to individual patients, that is, the art of evidence-based medicine.
DEVELOPMENT OF MODERN APPROACHES TO TREATMENT
Professional treatment for AUD that is supported by a base of basic and clinical research is a relatively new field compared to other areas of medicine. For most of history, custodial treatment was all that was available. Modern behavioral treatment approaches grew initially out of the success of Alcoholics Anonymous (AA) on the one hand and the growth of academic psychiatry and psychology after World War II on the other. AA was established in 1935, its Big Book was published in 1939, and it rapidly spread (6). The Minnesota Model of treatment was initially conceived by a psychologist and a physician working at Willmar State Hospital in Minnesota in the 1950s. They collaborated with two early recovery centers run by recovering AA members, Pioneer house and Hazelden, to create a treatment model that combined counseling and education and the 12 Steps of AA. Dan Anderson, a cocreator of the model, moved to the Hazelden Foundation in 1961, an organization that has been influential in its popularization (7). The Johnson Institute, another Minnesota organization, was established in 1966 to help spread the Minnesota Model; it also developed the procedure known as an intervention, where people close to an alcohol-dependent person come together to share their concern (and usually shuttle the soon-to-be patient off to treatment). Subsequently, the model has been adopted internationally, and it is the most prevalent form of treatment available in the United States (3,7).
Key features of the Minnesota Model are the use of both professional staff and trained recovering alcoholics, patient and family education, strong linkage to AA, a requirement of abstinence from all addictive substances other than tobacco and caffeine, and belief that alcoholism is a primary, progressive disease that cannot be cured, although it can be arrested through abstinence and AA. It was initially provided only in 28-day programs in hospitals or residential facilities but is now provided in outpatient settings as well. The primary modalities used in most programs are group counseling and education (8). Twelve-Step Facilitation is a manualized version of the Minnesota Model that has been adapted for an individual outpatient approach (9).
At about the same time in history, the fields of psychology and psychiatry were undergoing substantial development and expansion as well, primarily because the Veterans Administration rapidly expanded mental health services following World War II (10,11). Pavlov discovered classical conditioning in the 1920s (12), and B.F. Skinner first published on operant conditioning in 1935 (13). The concepts of group therapy and therapeutic community were first proposed in the mid-1940s, with subsequent development and spread in the 1950s and 1960s (14). Albert Ellis developed the first type of cognitive–behavior therapy, Rational-Emotive Therapy, in the mid-1950s (15), and Aaron Beck developed cognitive therapy for depression in the 1960s (16). Specific therapies for AUD based on these earlier psychological theories include therapeutic communities, aversion therapy, cognitive–behavior therapy, skills training, community reinforcement, and contingency management. More recently, William Miller and colleagues developed an approach based on stages of change and motivation (17,18).
Over the same period, pharmacotherapy for alcohol dependence was attempted with many new psychiatric medications as they were discovered or developed. Examples include lithium carbonate, anxiolytics, tricyclic antidepressants, antipsychotics, and phenytoin. Although initial reports regarding these medications reported efficacy in open-label studies, subsequent research for all except disulfiram failed to substantiate early claims. Disulfiram was approved for use as a deterrent or aversive agent in 1949. It took 46 years for the next medication, naltrexone, to be approved for treatment of alcohol dependence in 1995. More recently, acamprosate and topiramate have been shown to be effective (19–21). Multiple pharmacotherapy agents are now under investigation, and it is very likely that there will be additional medications available in the future.
Research on the nature, causes, consequences, course, and treatment of AUD developed in parallel during this time. Major advances have been made in identifying genetic, developmental, and environmental risk factors for AUD, describing its natural history and treatment response, as well as social and biomedical consequences of heavy drinking and AUD. Excellent animal models now exist for studying the neurobiology of the disorder as well as identifying potential treatment approaches. The methodology for clinical studies has advanced as well, resulting in refinement of methods and widespread agreement on use of various instruments for determining outcome. Manualization and sophisticated monitoring of the application of behavioral techniques have allowed true comparisons of efficacy with a high degree of confidence in the validity of the trials.
It is obvious that considerable progress toward enlightened, humane, and effective treatment has been made in a relatively short time. Nevertheless, the historical development of modern treatment has also created some unique obstacles that must be overcome in order for progress to continue. In the vast majority of community programs (not including the Veterans Administration medical system), psychoeducational group counseling and referral to AA provided by counselors with minimal education are the only modalities offered (3,4,22). In most cases, there is no physician involvement in treatment other than treating withdrawal. Furthermore, it is a time-limited treatment focused on inducing and maintaining remission and offers little except repetition for patients who not respond (4). Because of the lack of integration of addiction treatment programs with medical and psychiatric treatment, few programs are able to identify and treat coexisting mental and physical disorders in their patients, even though these are very common in a treatment-seeking population (22). The quality of counseling in community programs is poor, often consisting of casual talk unrelated to therapy (23), and supervision is minimal. Very few community treatment programs offer currently available pharmacotherapy or even educate their patients about it (3,4,24). In sum, although progress has been made, much more remains to be done.
How Should Treatment Outcome Be Determined?
An additional legacy of the unique history of treatment for AUD is controversy about what the goal of treatment should be, and how outcome should be measured. Until relatively recently, total, continuous, permanent abstinence was considered by most to be the only goal of treatment and the only measure of outcome. Reasons for this are complex but include the strongly held belief of AA members and Minnesota Model treatment providers that anything less than a commitment to total lifetime abstinence would result in failure. Additionally, abstinence was easier for researchers to measure and verify. Also, certain strains of American Protestantism have held the view that any consumption of alcohol is sinful and dangerous (25,26). Thus, for a habitual drunkard, becoming abstinent is equated with moral redemption. AA grew out of early members’ experience with the Oxford Group, which was grounded in Christian evangelism and incorporated sharing of one’s sins to others in a group that included others who had already experienced a spiritual transformation. In fact, Bill Wilson, one of the founders of AA, experienced a sudden transformative experience he called his “hot flash” (6). To this day, a spiritual awakening is considered to be at the heart of the path of AA (27).
On the other hand, some researchers believed that drinking (including heavy drinking) was a learned behavior and that it might therefore be possible for patients to learn new ways of (moderate) drinking. Treatment methods based on this idea were developed and eventually compared to abstinence-based approaches, which generated considerable controversy and outright animosity (28). Whether abstinence or reduced drinking should be the goal remains a matter of contention. Reduced drinking as a goal has been labeled as “harm reduction,” an unfortunate term that describes a pragmatic public drug policy most interested in results, as opposed to a more idealistic one focused more on intention. In the case of clinical care, the term is used to describe a pragmatic approach when continuous abstinence cannot be obtained, either because the individual is unwilling to endorse a goal of abstinence or because treatment is unable to help the patient achieve and maintain abstinence. In other words, “harm reduction” means staying engaged with a patient and continuing to provide treatment even when full remission (a “cure”) is not currently obtainable. Since treatment of chronic illness comprises the bulk of current health care, noncurative care for AUD is similar to that provided for any other, noncurative, chronic illness such as diabetes mellitus or arthritis. However, “harm reduction” is not used to describe treatment for these others diseases. Since this term can be interpreted by some as “giving up” on the patient, it not only is noninformative but distorts the meaning and intention of longitudinal care provision and should be abandoned when applied to clinical care.
A more recent twist on this debate is whether abstinence or nonabstinent remission is equivalent to “recovery.” One prominent 12-step–oriented treatment facility convened a consensus panel to define recovery (29). The panel concluded that recovery required sobriety (in this case, abstinence from alcohol and all other nonprescribed drugs), which was a necessary but not sufficient condition for recovery. In their view, in addition to sobriety, recovery required personal health (improved quality of life, physical, mental, and spiritual health) and citizenship (social health, contributing and interacting with the community at large). In a study of recovering volunteers from the community, Laudet (30) found that most considered total abstinence necessary for recovery. However, recovery entailed additional goals, such as well-being, a new life, or a second change, suggesting not only wellness as a goal but also regaining what was lost through addiction. Subjects also believed that recovery was an ongoing process or way of life rather than something that is achieved at a specific point in time. This emphasis on recovery coincides with a similar focus on recovery from mental illnesses (31), and an overall increase in attention to patient-rated outcomes in health care (32,33). More research on recovery processes and trajectories in AUD is needed.
The research community has developed increasingly sophisticated ways to measure outcome, although they are far from perfect. There are three broad categories of outcome: drinking behavior, symptoms or diagnostic criteria of dependence, and functioning in multiple life areas such as occupational achievement, social function, and psychological and physical health. Depending on the method used, these functional areas may or may not be explicitly linked to drinking behavior. That is, some instruments or studies attempt to quantify adverse life consequences of drinking, while others simply measure functioning without reference to drinking.
Drinking behavior is most often determined by taking the individual through a structured process of retrospective reconstruction (the most commonly used instrument for this is the Timeline Follow-Back) (34–36). Retrospective self-report is still the standard approach in most treatment trials, and most research supports its general validity and reliability (35). Recent research using interactive voice response and personal digital assistants offer one alternative that may eliminate memory errors (24,36–40), but daily monitoring of drinking may itself lead to drinking reductions, thus complicating interpretation (41,42). Eventual development of biosensors that can measure blood alcohol concentration continuously will likely supplant self-report measures, but they may also cause drinking reductions themselves.
Another way to measure outcome is whether or not the disorder, as determined by diagnostic criteria, is still present after treatment. Although different studies use slightly different approaches, a reasonable approach for clinicians mirrors that used for other disorders. For the outcome of treatment of AUD, using the Diagnostic and Statistical Manual of the American Psychiatry Association criteria (DSM-5) (43), recovery is defined as no longer meeting any of the 11 criteria of AUD (full remission), irrespective of drinking. Partial remission means meeting one AUD criterion but not enough to qualify for the AUD diagnosis, and nonremission is continuing to meet two or more criteria. Importantly, since drinking quantity and frequency are not included in the diagnosis, they are not considered in DSM-5. A recent epidemiologic study divided outcomes into these categories: abstinent recovery, nonabstinent recovery (meeting no diagnostic criteria for DSM-IV (44) abuse or dependence and not exceeding maximum drinking recommendations from the National Institute on Alcohol Abuse and Alcoholism), risk drinking (not meeting diagnostic criteria for AUD but exceeding maximum drinking recommendations), symptomatic but not dependent (meeting one or two dependence criteria or one or more abuse criteria), and dependent (meeting three or more criteria) (45). Note the addition of the category of nonabstinent remission, another violation of traditional dogma about recovery. Nonabstinent remission turns out to be the most common outcome 20 years after onset of DSM-IV alcohol dependence, followed by abstinence (45).
In the earliest studies of outcome, this type of categorical or dichotomous measures (abstinent or drinking, relapse or not) was used. Over time, use of simple categories was largely supplanted by variable-based approaches, where average values of a continuous drinking variable were compared among groups using increasingly sophisticated statistical techniques. Percent days abstinent and percent days heavy drinking are common examples. This variable-centered approach has advantages, such as using more data and allowing use of parametric statistics, thus increasing statistical power. This approach also allows for a wider range of outcomes rather than a few predetermined categories. However, variable-based approaches also hide complexity. For example, in medication trials especially, it seems likely that with any one medication, only a portion of the study population will demonstrate a response, while the majority may not respond at all. Consequently, a robust response in a minority of individuals may only move the mean a small distance, suggesting that the treatment is only minimally effective overall (which is true, for the entire study population). Variable-centered analysis may miss such an effect entirely. For example, in a reanalysis of two studies of naltrexone, both of which were negative with the a priori variable-based analysis, trajectory analysis found that naltrexone recipients were significantly more likely to be in an abstinent trajectory (46). Trajectory analysis also yields results that are more clinically intuitive. For example, one such analysis examined three different trajectories through the follow-up period: stable remission, stable nonremission, and unstable (47). A more recent study examined drinking trajectories prior to treatment entry and found that they predict outcome (48). Comparing the likelihood of being in various trajectories for different treatments is easier for most people to grasp, compared to a change in a continuous variable such as mean percent days abstinent. Consequently, trajectory analysis is likely to be used more often in the future. Rapid development in pharmacogenomics suggests the possibility of being able to identify likely responders to different medications before treatment starts. However, at this time, no genetic marker that reliably predicts response has been identified (49).
In some other medical disorders such as cardiovascular disease, outcomes are often measured in terms of reduction in disease-related adverse consequences. For example, the value of therapies for hypertension or hyperlipidemia is determined by how well they reduce the risk for adverse consequences such as stroke, myocardial infarction, and death. A recent study on the global burden of disease found that alcohol was the fifth leading cause of disability globally, a 32% increase since 1990 (50). In the United States, the disease burden from AUD, compared to all other health conditions, was ranked 22nd, up from 26th in 1990, a 26% increase. In 2010, alcohol use was the eighth leading cause of death, and the seventh leading cause of years of life lost in the United States (50). According to one estimate, 54% of premature deaths are due to acute conditions and 46% due to chronic conditions. Because acute deaths due primarily to trauma differentially affect young people, the years of life lost is higher for acute (65%) compared to chronic (35%) conditions. In middle age, chronic dependence is associated with a host of physical disorders such as liver fibrosis and cirrhosis, cancer and cardiovascular disease, social consequences such as unemployment and divorce, and mental illness such as depression and suicide. The relationship between these outcomes and alcohol consumption is complex, and however, is mediated by genetic vulnerability, other lifestyle factors such as smoking, social factors, and possibly choice of beverage.
Further complicating matters, alcohol consumption carries not only risks but potential benefits as well. Moderate alcohol consumption in middle-aged adults is associated with decreased incidence of cardiovascular disease and death, diabetes, Alzheimer disease, and stroke, although heavy drinking increases risk for these disorders in some studies (51–53). Thus, one must subtract potential beneficial effects of drinking from potential risk for adverse events when developing risk estimates. Most mortality data on people with AUDs have been obtained with samples of people seeking or receiving treatment for alcohol dependence. These studies have found that annual mortality is 1.4 to 4.7 times that of matched controls, depending on the sample studied (54–57). Since treatment seekers have more severe dependence, a higher prevalence of comorbid conditions, and less social capital than nontreatment seekers, information obtained by studying treatment populations applies only to the 20% or less of people with AUDs with the most severe and recurring form of dependence (58–60).
Social consequences are mediated by comorbid mental disorders, especially antisocial personality disorder, and are also highly context dependent. For example, whether one is arrested for driving while intoxicated depends on the laws of the particular jurisdiction in which driving occurs and how they are enforced, as well as whether an individual has a coexisting antisocial personality disorder. Societies vary markedly in their tolerance for various forms of social behavior associated with intoxication or dependence. At the same time, there remains a strong association between overall physical, mental, occupational, and social function and presence and degree of AUD. In a recent large community sample, as the number of diagnostic criteria met increased, function decreased, and functional impairment for severe dependence (6 to 7 criteria met) was similar to that for anxiety disorders and depression (1). Similarly, in a treatment sample, problems associated with drinking were strongly (but imperfectly) correlated with drinking outcomes (47). In a longitudinal study of help-seeking older adults with alcohol dependence, long-term abstinence was strongly associated with improved functional outcomes (54,61–63).
In sum, measures of drinking behavior are the easiest to measure reliably across studies and can be used as either categorical or continuous variables. Quantity and frequency alone are sufficient to determine whether a patient’s drinking constitutes a risk factor for future problems. However, drinking becomes an AUD when it causes clinically significant distress or impairment, and these variables are more difficult to measure. Similarly, the relationship between social and occupational function is complex and bidirectional. Since abstinence or low-risk drinking without symptoms of an AUD (remission) are most robustly predictive of continued recovery as well as function, yet are easier to measure, they may serve as the best single outcome measure. Categorical approaches, such as full remission, partial remission or risk drinking, and nonremission, offer an attractive and clinically intuitive way to measure outcome, and analysis of groups with different trajectories may prove to be more sensitive to detecting meaningful treatment effects in some studies.
THE SPECTRUM OF HEAVY DRINKING AND ALCOHOL USE DISORDERS
New research has provided a new and more complete view of the range of drinking, AUDs, and alcohol-related harms. However, some definitions are needed in order to describe drinking behavior and relate it to adverse events. In the United States, a “standard drink” is defined as the amount of ethanol in 1.5 oz (45 mL) of 80-proof spirits, 12 oz of beer, or 5 oz of table wine, each containing about 14 g of absolute ethanol (Table 23-1). Since actual alcohol levels in beer and wine vary, these amounts are meant to be approximate. The National Institute of Alcohol Abuse and Alcoholism of the National Institutes of Health recommends that men drink no more than 4 drinks per day and 14 drinks per week and that women drink no more than 3 drinks per day and 7 drinks per week (Table 23-2). Drinking within these limits is considered “low-risk” drinking. Lower limits or abstinence may be indicated in the presence of coexisting medical or psychiatric disorders, in older people, or when medication interactions are a concern. Women who are pregnant or at risk of becoming pregnant are advised to abstain. In this chapter, a day on which the limit is exceeded is considered a “heavy drinking day,” and “heavy drinking” is defined as drinking in excess of the maximum limits on a regular basis, such as exceeding the daily limits weekly or more often. “At-risk drinking” is heavy drinking in the absence of meeting any criteria for an AUD, while heavy drinking includes both at-risk drinking and symptomatic drinking (AUDs).
TABLE 23-1 TYPICAL BEVERAGES AND DRINK SIZES AND THE APPROXIMATE NUMBER OF US STANDARD DRINKS IN EACH
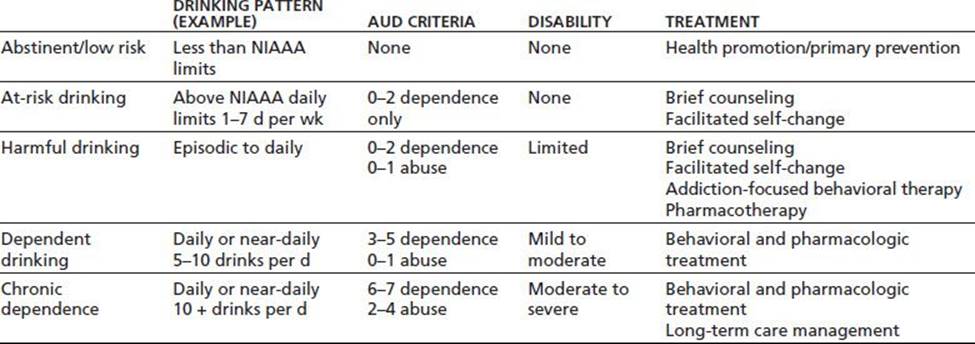
TABLE 23-2 CHARACTERISTICS OF INDIVIDUALS IN EACH CATEGORY OF DRINKING BEHAVIOR
NIAAA, National Institute on Alcohol Abuse and Alcoholism.
AUD criteria refer to all 11 DSM-IV criteria for abuse and dependence treated as a single-dimensional disorder. NIAAA maximum recommended drinking limits are as follows: women: 3 drinks per day and 7 per week; men: 4 drinks per day and 14 per week. Information in all cells is provided for illustrative purposes only and is not meant to imply formal definitions.
The continuum of drinking in the US adults is shown in Figure 23-1. About 70% of the US adult population report either being abstinent or engaging in low-risk drinking in any given year, about 21% are at-risk drinkers, and 9% have a DSM-IV AUD (5% abuse and 4% alcohol dependence) (1). (It is unclear how that will translate to DSM-5, but it is likely to be less than 9%, since DSM-5 AUD requires at least two positive criteria, while admitting to drinking, and driving is sufficient for a diagnosis of DSM-IV alcohol abuse.) At-risk drinking places an individual at higher risk for developing alcohol-related problems, such as an AUD, liver disease, or a mental disorder. As a health risk factor, at-risk drinking is analogous to high blood pressure or hyperlipidemia prior to end-organ damage. Also, alcohol addiction due to dys-regulation of the brain systems involved with motivation and reward can be thought of as end-organ damage to the brain caused by heavy drinking (64). Most heavy drinking occurs between the ages of 18 and 25, which is also when the prevalence of AUDs peaks (65). Not all heavy drinkers develop alcohol-related problems, and which type of problem a heavy drinker develops varies. Importantly, more than 40% of daily or near-daily heavy drinkers do not meet any criteria for AUD (66,67). Similarly, only 20% to 40% of people with alcoholic liver cirrhosis also have AUD (67,68). Finally, not all alcohol-related harms occur in people who have AUDs, in part because there are twice as many at-risk drinkers as there are people with AUDs. Trauma, in particular, may occur due to a single occasion of heavy drinking or in someone who only drinks to excess occasionally.
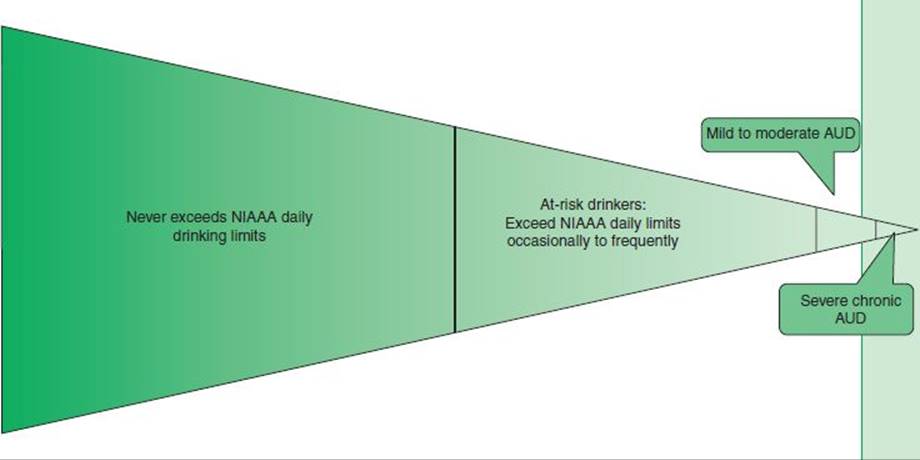
FIGURE 23-1 Spectrum of alcohol use and associated disorders in any given year. (Based on data from Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability, and comorbidity of DSM-IValcohol abuse and dependence in the United States: Results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry2007;64(7):830–842.)
The spectrum of severity for heavy drinking and AUD in the previous edition of this chapter used DSM-IV criteria but anticipated the joining of criteria for abuse and dependence into a single disorder in DSM-5. Thus, DSM-5 criteria will be used to inform the spectrum model presented below.
Diagnostic criteria for AUD can be grouped as such: (a) impaired control (going over limits, failed attempts to quit or cut down, continued drinking despite adverse psychological or physical effects), (b) increased salience (craving, spending much time anticipating, drinking and recovering, and reduced involvement in nondrinking activities), (c) physiologic adaptation (tolerance and withdrawal), and (d) complications of drinking (physically hazardous use, serious interpersonal problems, and role failure) (43). A threshold criterion is that drinking must also be causing clinically significant impairment or distress. Thus, heavy drinking itself is not considered an AUD, even if it results in physical harm. Drinking quantity and frequency patterns vary considerably among people who meet minimum criteria for AUD. Note, however, that most heavy drinkers do not meet criteria for AUD. People with AUD vary in many other ways as well, suggesting that the clinical diagnosis is actually composed of an unknown number of subgroups. This heterogeneity presents a serious problem for treatment research, since treatment of a depressed, anxious 38-year-old married woman drinking 6 drinks a day would presumably differ from that for a 22-year-old antisocial male with cannabis dependence who drinks a liter of vodka twice weekly. However, although there are exceptions, most studies of treatment have included all people meeting criteria for DSM-IV alcohol dependence. Similarly, most treatment programs essentially provide the same treatment to everyone entering the program.
There has been recent progress identifying different subgroups of people with AUD. Moss and colleagues (58) identified five subgroups of people meeting DSM-IV criteria for alcohol dependence, using data from the NESARC, a large epidemiologic study of a representative community sample in the United States, (69) and then examined their outcomes 3 years later (70). In that short time, more than 50% had remitted, yet seeking treatment was uncommon except in one small group. The middle-aged group with severe, chronic alcohol dependence, which comprised only 8% of the sample, had treatment-seeking rates of about 40% and was most likely to have persistent severe disorder. Among the large majority, treatment seeking was under 10%. Nevertheless, lifetime remission rates for AUD are over 90% (71). The difference between common depictions of AUD as chronic and progressive and requiring treatment, and the reality in the community is striking. It stems from studying the small group with severe and persistent AUD and then, mistakenly, generalizing to untreated individuals in the community.
Unfortunately, attempts to subtype AUD according to clinical and demographic characteristics among those seeking treatment have not been productive in terms of predicting differential response. Therefore, there is a pressing need to identify more robust subtypes of heavy drinkers, in particular subtypes that predict treatment response. Until that occurs, the individual physician must attempt to assimilate the latest information from randomized controlled trials and skillfully apply that information to an individual patient’s situation.
The Spectrum of Drinking, Disorders, and Treatment
The goal of treatment depends upon the nature, extent, and severity of the disorder. In place of the “one size fits all” approach initially developed for people with severe, relapsing AUD, an individualized approach that takes patient preferences into account is required. Coexisting conditions or circumstances are also important determinants of the therapeutic approach and methods used. The continuum of drinking presented in Figure 23-1 serves as a template upon which to project a continuum of care (Table 23-2).
Abstainers and low-risk drinkers require health promotion, such as education about the recommended maximum limits adjusted for that person’s individual situation. Health promotion is especially important for adolescents and women who are pregnant or at risk of becoming pregnant. High-risk groups, such as youth with a primary relative with AUD or who have conduct disorder, may require modification of advice and possibly more intensive interventions to prevent the development of heavy drinking and AUDs. The goal for at-risk drinkers is to reduce consumption, preferably below recommended maximum limits, in order to reduce risk of future harm. At-risk drinkers (and possibly those with mild AUD) respond well to facilitated self-change (72) and brief counseling by physicians in primary care, with about a 25% overall reduction in drinking 1 year later and a greater decrease in heavy drinking (73). Evidence is accumulating that college students respond to Internet-based individualized feedback as well as to brief counseling (74–76). Whether brief counseling is effective in emergency care settings is unclear, with some studies showing an effect and others not. For individuals with more than minimal levels of dependence, however, more intensive forms of treatment are needed. Brief counseling alone is not effective with more severely affected drinkers in general (73) or hospitalized heavy drinkers (because most have more severe AUD) (77,78).
Most studies of treatment of DSM-IV alcohol dependence have been done on middle-aged, treatment-seeking adults, especially white males and veterans. Since the average age of onset of alcohol dependence is 21 years (1) and the average age in most treatment studies is about 40, this means that most study subjects have chronic, relapsing, severe alcohol dependence and have been ill for a decade or more. This chronically ill group, which also has considerable comorbidity, represents a small minority of people who develop dependence at some point in their lives (58). The extensive study of this subgroup (and lack of study of others) has created a picture of alcohol dependence as an inevitably severe, chronic disorder resistant to treatment. In fact, new research has demonstrated that 72% of the US adults with a lifetime DSM-IV diagnosis of dependence have a single episode, lasting on average 3 to 4 years (1). Those with more than one episode, tend to average five episodes of decreasing length, suggesting that failure to achieve permanent remission after the first episode predicts a more chronic course (1).
At the same time, treatment study recruitment has shifted over time from patients in treatment programs to volunteers solicited through newspaper ads. Research volunteers recruited from community settings differ systematically from volunteers recruited from treatment programs; they are more functional, more likely to be employed, have less severe alcohol dependence, and are less likely to have coexisting other substance and mental or physical disorders (79). Furthermore, efficacy studies typically exclude people with significant comorbidities, homelessness, or lack of transportation. Consequently, generalizing from such studies to clinical populations where these co-occurring conditions are common is not straightforward. There is a gap in research knowledge on the effectiveness of treatments in more natural settings with a broader population, especially for studies of specific behavioral or pharmacotherapy treatments. The fact that overall outcomes from naturalistic treatment studies do not differ substantially from those in efficacy trials is reassuring (80,81), but more effectiveness research is needed, particularly in different settings such as primary care and general psychiatry.
Another pressing need is to develop and test treatment approaches for people with mild to moderate AUD and relatively few comorbidities. Such patients are unlikely to seek treatment in addiction treatment programs (70). In this type of patient, treatment with oral naltrexone plus brief behavioral support by health care clinicians is at least as effective as state-of-the-art outpatient addiction therapy (82,83). These findings suggest that pharmacotherapy with medical management may be an effective approach for patients with similar characteristics. If so, making such treatment available in primary care and general psychiatry would substantially increase access to effective care.
About two-thirds of individuals who develop dependence do so in adolescence or young adulthood. However, only about one-half of them go on to a chronic course (1). Those who do are more likely to have a family history of alcohol dependence and antisocial personality traits and to have started drinking in early adolescence (58). A pressing need is more research on early intervention in the course of illness for those at high risk for chronicity. Another third of dependent persons have mid-life onset of moderate severity dependence, and those who do are more likely to have coexisting psychopathology (58). This suggests that primary care and general psychiatry may be ideal settings in which to identify and treat this group.
For those who do not respond to self-change efforts and nonintensive or brief treatment, referral to specialty addiction treatment is needed. This type of stepped-care approach is implied in the Patient Placement Criteria—Second Edition by the American Society of Addiction Medicine (84). However, although the stepped-care approach makes sense intuitively, it has not be adequately examined for its effectiveness. Stepped-care or adaptive treatment designs are methodologically complex and require sophisticated design and analysis as well as large numbers of subjects. Adaptive study design is an emerging area of interest, however, and recent advances in statistical techniques make it more feasible. Such research can help answer questions about the best ways to structure the treatment system and to most effectively match patient needs and services offered. Attempts to improve outcomes by matching patient characteristics to treatment type have not yet yielded information of much use to clinicians, but such a body of knowledge is likely to develop over time.
At the most severe end of the spectrum are those unfortunate individuals with severe and persistent or recurrent alcohol dependence. In this group, coexisting substance, mental and physical disorders, and social disabilities are common, including antisocial personality, as is a family history of alcohol dependence and very early onset. Not surprisingly, they are the most likely to seek and receive treatment, often due to overt coercion (58). Even though most of this group has a chronic or recurrent course, addiction treatment programs typically offer treatment for only a few weeks or months. Furthermore, few programs are staffed to address the serious comorbidities present, so they are ignored or dealt with through referral (3). The effectiveness of treatment programs for this group is difficult to evaluate because there are many factors present that may be driving change. For example, serious physical illness, legal mandates, homelessness, unemployment and poverty, and family pressure frequently cause or contribute to a decision to seek treatment. Many of these factors are quite powerful and could account for much or all of whatever change occurs. More research is needed on the mechanisms of behavior change among heavy drinkers including those with severe disorders.
Research on long-term care management strategies similar to those used for other chronic disorders is promising, especially for people with alcohol dependence and serious mental or physical disorders. For example, studies of heavy drinkers with severe medical complications such as liver cirrhosis suggest that addressing drinking using a care management approach in the context of general medical care is effective at reducing drinking and inducing abstinence (85). In two studies of this approach, the 2-year mortality was about one-half of that in comparison groups receiving usual medical care (86,87). Integrating substance use interventions into community support programs for severely mentally ill people also has some support. These studies suggest that for harmful drinkers with serious medical or psychiatric illnesses, addressing drinking directly in the context of medical or psychiatric treatment is preferable to referral to a standard addiction treatment program that is not staffed so as to be able to address serious medical or psychiatric illnesses. At this time, there are no treatment approaches shown to be effective with severe and persistent alcohol dependence in the absence of comorbidities that cause serious dysfunction (88). Since this group members with severe AUD are frequently heavy consumers of health care, social, and criminal justice services, development of more effective treatments is a priority. It may be that external motivating factors, such as skillful application of legal coercion or contingency management may be effective with this group, especially when combined with “wraparound” services that integrate addiction, psychiatric, and medical care as well as social services and sober housing. What is clear is that treatment for these individuals needs to be structured with the goal of providing services intermittently or continuously for years to decades rather than weeks or months.
To summarize, recent research has shown that drinking and associated symptoms and problems occur along a continuum ranging from none to mild, moderate, and severe. A large majority of the US adults abstain or drink at low-risk levels. Most heavy drinkers are without current symptoms or problems but are at increased risk for physical, mental, and substance use disorders developing over time. In contrast to popular belief, most people who meet dependence criteria do not have a chronic course and most recover without professional treatment or even attendance at mutual help groups. It appears that most people, upon recognizing a problem attempt to change alone or with informal help, and the majority are eventually successful, albeit after several years of active AUD. Seeking help from mutual help groups or nonaddiction professionals (about 25%) and/or professional treatment programs (13%) occurs when informal attempts to change fail (or due to an external contingency such as a driving while intoxicated charge). A significant proportion of help seekers respond with improvement or remission, leaving a small but important group with severe and persistent dependence. This continuum of drinking and associated symptoms and problems suggests a corresponding continuum of care (Table 23-2).
Unfortunately, most of this continuum of care is not yet implemented or available. The quality of care for heavy drinking and AUDs in primary care is the lowest among 30 chronic conditions (5), and attempts to increase screening and brief intervention for at-risk drinking have met with little success in spite of a robust evidence base for their efficacy (73). Large numbers of Americans lack health insurance, and private insurance companies have disinvested in addiction treatment so that most treatment provided today is publicly funded (89). Treatment programs suffer from insufficient funds, resulting in poorly trained and underpaid staff and excessive turnover (3). The proportion of people with current dependence receiving treatment actually declined between 1991 to 1992 and 2001 to 2002 (1,90), and there is no evidence that the prevalence or public health burden of heavy drinking or alcohol dependence has decreased, with the important exception of a reduction in premature deaths among adolescents due to stricter drink-driving laws (90). Thus, much remains to be done and many challenges lie ahead. Nevertheless, this fuller understanding of the spectrum of drinking, disorders, and treatment approaches provides one possible conceptual framework for advancing investment and development of the continuum of care.
A major public health challenge is to provide earlier identification and appropriate treatment to a much broader spectrum of individuals who drink heavily or who have alcohol dependence than is currently the case. There is a pressing need to identify early intervention strategies for youth who begin drinking in early adolescence and who are at high risk for later development of severe chronic dependence. Early identification and treatment of heavy drinking and dependence in primary care and general mental health care would provide access for millions of people who otherwise will not receive treatment. Needed also is a better understanding of the factors driving change in heavy drinkers and how to facilitate that change both in addiction treatment and in other settings. Finally, effective and cost-effective care management strategies for managing chronic severe dependence need to be implemented. In order to provide this type of comprehensive care, the specialty addiction treatment sector will require substantial development so that addiction, psychiatric, medical, and social services can be provided in an integrated way and over longer periods of time.
TYPES OF TREATMENT AND TREATMENT EFFECTIVENESS
Multiple treatment modalities have been shown to be effective in the treatment of alcohol dependence. However, the best way to match the type and intensity of treatment to the individual needs of a patient with AUD remains unclear. For example, no systematic outcome advantage has been demonstrated for residential or intensive day program treatment compared to once or twice weekly outpatient treatment (91). Similarly, no behavioral treatment has been shown to be better than others that are conceptually distinct and use different behavioral techniques (92). Attempts to match specific behavioral therapies with clinical characteristics of patients have yielded little (92). Several medications are efficacious in reducing relapse or heavy drinking during early recovery, but none are clearly better than others, and there is not yet a way to predict how likely a patient is to respond to one rather than another. Finally, approximately 10% of people with AUD have a severe chronic form of the disorder, yet most treatment programs offer a few weeks or months of treatment, and information on management of AUD as a chronic illness is limited. In sum, current recommendations and practice regarding the selection and sequencing of treatments are based upon clinical experience and expert consensus and not randomized controlled trials. In practical terms, the addiction treatment offered or available likely depends on patient preference, availability, access, coercion, urgent needs such as imminent withdrawal or suicide risk, and clinician orientation rather than on scientific evidence. One of the key research challenges ahead is to develop methods to compare the effectiveness of different stepwise or adaptive strategies for deploying treatment modalities with demonstrated efficacy.
The outcome of treatment varies according to the diagnosis or stage of illness. At-risk drinkers who are identified and offered education and brief motivational counseling on average reduce drinking about 25% over the following year (73). Treatment outcome for AUD is remarkably similar across studies and treatment modalities, both behavioral and pharmacologic (80). In a typical treatment study, about one-third of subjects will be in full abstinent or nonabstinent remission for the following year, 30% to 40% will show substantial improvement but will have at least some episodes of heavy drinking, and 20% to 30% will not show an effect (47,80,91). However, over the course of the ensuing 5 to 10 years, most will suffer at least some relapse (93). Detailed information about each different behavioral and pharmacologic modality is provided in the appropriate chapters. However, no particular treatment or technique has proved to be overall more effective than others, thus raising the question of what the mechanisms of change really are. In fact, many people start reducing their drinking prior to treatment entry, and both study protocols and treatment programs require that someone be abstinent at treatment entry, whether or not they required medical support for withdrawal. For that matter, there are no clear criteria for distinguishing “still drinking” from “abstinent,” since treatment cannot take place if an individual is intoxicated. In other words, it is arbitrary how long abstinence is required in order to qualify as “abstinent.” In yet another randomized controlled trial of two behavioral treatments for alcohol dependence that showed no difference between brief motivational counseling versus a more extensive multimodal program of care, Orford and colleagues (94) qualitatively examined the process leading to help seeking in study subjects. They identified a “catalyst system” consisting of increasing problems and distress related to drinking, pressure from others, and a trigger event, which in turn led to the realization, “I can’t do this on my own.” Factors outside the treatment context continued to be important throughout the recovery process, especially after the discontinuation of treatment services. In another study of 15 community treatment programs, 5-year outcomes of patients who dropped out of treatment early did not differ from program completers (95). These findings suggest that the process of deciding to seek help is itself part of the change process and is arguably the most important, although it is not well understood. In the next section, we will examine the question of what causes change.
What Causes and Maintains Change in Drinking Behavior?
Help seeking is strongly associated with increased odds of achieving recovery, but help seekers differ systematically from non–help seekers. Help seekers on average are older, have more severe dependence and more coexisting mental and physical disorders, as well as less social support (45,96), and are more likely to have the relapsing form of the illness (1). For those who do seek help, both professional treatment and 12-step participation are associated with increased likelihood of recovery, especially abstinent recovery (45,62). For individuals older than 35 years, abstinence is much more stable an outcome than even light drinking without problems (95,97), while in younger persons, light drinking without problems (non-abstinent remission) is similar to abstinence in predicting continued remission 3 years later (97). In people who have been treated for AUD, recovery is in turn strongly associated with reduced mortality (54). Thus, full remission, whether abstinent or nonabstinent, should be the goal of treatment for AUD, tempered with the recognition that full recovery cannot always be achieved.
Unfortunately, such studies are not able to establish causality. Although help seeking and participation in treatment and 12-step groups are associated with improved outcomes and decreased mortality, it cannot be ruled out that people who have decided to change will seek treatment, while those who do not want to change do not, or that people who respond to treatment early develop more hope and motivation to continue. That is, treatment participation or continuation may be a result of change rather than the converse. There may be other unmeasured differences between the groups as well. At the same time, it is clear that people who achieve full remission of drinking have much better overall functional and medical outcomes than those with partial or no response. Furthermore, it appears that treatment followed by 12-step participation is a frequent and effective (but not the only) path to recovery for many people (45,62). Recently, Rudolf Moos has emphasized the importance of the interaction of personal and social resources instrumental in promoting remission (98). Specific theories and treatment components he identified include social control theory (support, goal direction, and structure), behavioral economics and behavioral choice theory (an emphasis on rewards that compete with substance use), social learning theory (focus on abstinence-oriented norms and models), and stress and coping theory (attempts to develop self-efficacy and coping skills). Conceptualizations such as these provide guidance for both research and clinical practice and are particularly helpful to approach the relationship of factors at different levels of analysis (neurobiologic, personal, and social). This type of integrative thinking and research will become increasingly important as the question of determinants of change is further explored. The National Institutes of Health, recognizing the importance of understanding the basic science of behavior change has initiated a major research effort called OppNet, which funds basic behavioral research across many NIH institutes and centers (99).
INTEGRATING THE EVIDENCE AND PERSONALIZING PRACTICE
Given the proliferation of new research, published in an ever-expanding number of professional journals, it is a challenge to understand and incorporate new findings into practice. Unfortunately, although studies of the efficacy of various treatments may help determine how one treatment compares to another treatment or to no treatment, there are few studies that address directly questions of central importance to clinicians. For example, should one recommend a few sessions of motivational enhancement therapy or an intensive day program for the treatment of dependence? If an at-risk drinker does not respond to brief motivational counseling, what is the appropriate next step? Is the stepped care strategy, where the least restrictive and expensive option for a particular patient’s situation is offered first, the best approach? How much evidence is required before recommending a new treatment? How much evidence is required before failure to offer or recommend a treatment based on personal taste or ideology is ethically indefensible?
Although it is not possible at this time to provide definitive or even approximate answers for many such questions, certain conclusions emerge from the current body of evidence. First, although differences among different behavioral techniques tend to be minor, the quality of behavioral treatment is important. Specifically, empathic and skillful therapy is more effective than confrontation and education. Furthermore, it is more important to engage someone with AUD in treatment than which particular treatment is used. Therefore, it makes sense to offer a variety of treatment options, since patients are likely to vary in their preferences. The same holds true for the setting of treatment. Unless someone is unable to abstain living in the community, there is no advantage of residential versus outpatient treatment. Second, currently available medications offer small but clinically important benefit in early recovery and therefore patients should routinely be made aware of them and offered the opportunity to use them. As with behavioral treatments, however, there is no consensus that any one medication is better than another or that there is a specific sequence in which they should be used. There is no evidence at this time that combining medications is more beneficial than mono-therapy. For appropriate patients (mild to moderate AUD, little or no coexisting psychopathology, socially stable, and motivated to change drinking), medication with medical care management and encouragement to abstain, adhere to treatment, and attend mutual help groups is as effective as specialized alcohol counseling. Third, a social network supportive of abstinence is at least as important as whatever treatment occurs in determining outcome (100). Except for referral to mutual help groups, this aspect of treatment tends to be neglected, to the detriment of our patients. Behavioral marital therapy, for example, has a strong evidence base (101). Finally, for any given diagnosis (e.g., at-risk drinking versus AUD), there is not yet a way to identify patient characteristics that reliably predict differential response to different treatments, although research in this area is promising.
SUMMARY AND CONCLUSIONS
From humble beginnings in recovery houses staffed by volunteer members of AA, the treatment for AUD has evolved in remarkable ways. Much has been learned about the genetics, neurobiology, psychology, social manifestations, epidemiology, and course of heavy drinking and alcohol dependence. Animal models available to study AUD are among the best available for any disease (102). With dedicated funding from the National Institutes of Health, a formidable research community has developed, providing a substantial body of sophisticated genetic and genomic, behavioral, neurobiologic, and pharmacotherapy research upon which to base treatment decisions and development of new treatments. The focus of current research has evolved from whether treatment works to questions of how it works, for whom, how to individualize treatment, and how to increase access to affordable and appealing treatment. Unfortunately, the clinical infrastructure has not developed in concert with growth in scientific understanding, thus making implementation of new findings difficult. Changing this situation will first require changing how drinking and its attendant risks and adverse effects are conceptualized. The public health model described in this chapter provides a framework for understanding drinking, risk, and disorder as existing along a continuum, which in turn suggests a corresponding comprehensive continuum of care. This model may be helpful in formulating new directions for research and policy. It also provides a framework for integrating information about different types of prevention and treatment activities for the purposes of treatment planning. It has important implications about what treatment is, where and to whom should be offered, and who should provide it.
More than conceptual change will be required, however. Fully implementing a continuum of care for heavy drinking and AUD requires the continued development of new treatments, especially medications, and new ways to provide behavioral support for change to large numbers of people. Physicians, in particular, must play a central role in providing care to people in existing primary care and psychiatric practices. Recent movement toward medical homes that integrated behavioral care offers an opportunity to expand access to treatment for people with less severe AUD (32). A reinvestment into the specialty treatment sector is also required, but with a new focus: providing true comprehensive specialty care over longer periods of time. A reinvigorated addiction medicine specialty approach must integrate treatment for addiction with treatment of physical and mental disorders as well as social services such as housing and vocational services. Changes in how services are funded, where they occur, and how they are staffed will be necessary, so the configuration of funding streams must change as well, because funding mechanisms tend to reflect and therefore support the current configuration of services.
At the same time, in the next decade, we are likely to witness major advances in the understanding of and treatments available for heavy drinking and related disorders. Development of more effective pharmaceuticals and identification of indicators predicting response in individual patients will be central features. Having more effective, cost-effective, and appealing treatments may then drive system changes to facilitate their implementation.
REFERENCES
1.Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry 2007;64(7):830–842.
2.Dawson DA, Grant BF, Stinson FS, et al. Estimating the effect of help-seeking on achieving recovery from alcohol dependence. Addiction 2006;101(6):824–834.
3.McLellan AT, Meyers K. Contemporary addiction treatment: a review of systems problems for adults and adolescents. Biol Psychiatry 2004;56(10):764.
4.Addiction medicine: closing the gap between science and practice. New York, NY: The National Center for Addiction and Substance Abuse at Columbia University, 2012; http://www.casacolumbia.org/addiction-research/reports/addiction-medicine
5.McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003;348(26):2635.
6.Pittman B. AA The way it began. Seattle, WA: Glen Abbey Books, 1988.
7.White WL. Slaying the dragon: the history of addiction treatment and recovery in America. Bloomington, IN: Chestnut Health Systems, 1998.
8.Anderson DJ, McGovern JP, DuPont RL. The origins of the Minnesota model of addictions treatment—a first person account. J Addict Dis 1999;18:107–114.
9.Nowinski J, Baker S, Carroll K. Twelve Step Facilitation Therapy Manual: A Clinical Research Guide for Therapists Treating Individuals with Alcohol Abuse and Dependence, vol 1. Project MATCH Monograph Series. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1992.
10.Compas B, Gotlib I. Introduction to clinical psychology. New York, NY: McGraw-Hill Higher Education, 2002.
11.Menninger R, Nemiah J. American psychiatry after World War II: 1944–1994. Washington, DC: American Psychiatric Press, 2000.
12.Pavlov IP. Conditioned reflexes; an investigation of the physiological activity of the cerebral cortex. London: Oxford University Press: Humphrey Milford, 1927.
13.Skinner BF. Two types of conditioned reflex and a pseudo type. J Gen Psychol 1935:66–77.
14.Pines M. Forgotten pioneers: The unwritten history of the therapeutic community movement. Ther Commun 1999;20:23–42.
15.Ellis A. Reason and emotion in psychotherapy. Secaucus, NJ: Citadel, 1962.
16.Beck AT. Cognitive therapy and the emotional disorders. New York, NY: International Universities Press, 1976.
17.Zweben A. Clinical and methodological utility of a composite outcome measure for alcohol treatment research. AlcoholClin Exp Res 2003;27(10):1680–1685.
18.Miller WR, Rollnick S. Motivational interviewing: preparing people to change addictive behavior. New York: The Guilford Press, 1991.
19.Johnson BA, Rosenthal N, Capece J, et al. Topiramate for the treatment of alcohol dependence: results from a multi-site trial. Alcohol Clin Exp Res 2007;31(s2):261A.
20.Carmen B, Angeles M, Ana M, et al. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: a systematic review. Addiction 2004;99(7):811.
21.Bouza C, Angeles M, Munoz A, et al. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: a systematic review. Addiction 2004;99(7):811–828.
22.Fletcher AM. Inside rehab. New York: Viking Penguin, 2013.
23.Carroll KM, Farentinos C, Ball SA, et al. MET meets the real world: design issues and clinical strategies in the Clinical Trials Network. J Subst Abuse Treat 2002;23(2):73–80.
24.Abraham AJ, Knudsen HK, Roman PM. A longitudinal examination of alcohol pharmacotherapy adoption in substance use disorder treatment programs: patterns of sustainability and discontinuation. J Stud Alcohol Drugs 2011;72:669–677.
25.The book of discipline of The United Methodist Church , 2004. Nashville, TN: The United Methodist Publishing House, 2004.
26.Land R, Duke B. On Alcohol Use. 2008; http://www.sbc.net/redirect.asp?url=http%3A%2F%2Ferlc%2Ecom%2Farticle%2Fon%2Dal cohol%2Duse&key=alcohol&title=On+Alcohol+Use&ndx=SBC%2C+IMB%2C+NAMB%2C+ANNUITY%2C+LIFEWAY%2C+W-MU%2C+ERLC%2C+SEMINARIES Accessed 2008/03/31/.
27.Alcoholics anonymous (The Big Book, 3rd ed.). New York, NY: Alcoholics Anonymous World Services, 1976.
28.Sobell MB, Sobell LC. The aftermath of heresy: a response to Pendery et al.’s (1982) critique of ‘individualized behavior therapy for alcoholics’. Behav Res Ther 1984;22(4):413–440.
29.Betty Ford Institute Consensus Panel. What is recovery? A working definition from the Betty Ford Institute. J Subst Abuse Treat 2007;33(3):221–228.
30.Laudet AB. What does recovery mean to you? Lessons from the recovery experience for research and practice. J Subst Abuse Treat 2007;33(3):243.
31.Interventions for alcohol use and alcohol use disorders in youth. Alcohol Res Health 2005;28:163–174.
32.Arend J, Tsang-Quinn J, Levine C, et al. The patient-centered medical home: history, components, and review of the evidence. Mt Sinai J Med 2012;79(4):433–450.
33.Leamy M, Bird V, Le Boutillier C, et al. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Br J Psychiatry 2011;199(6):445–452.
34.Sobell LC, Sobell MB. Timeline followback user’s guide: a calendar method for assessing alcohol and drug use. Toronto, Ontarior, Canada: The Addiction Research Foundation, 1996.
35.Del Boca FK, Darkes J. The validity of self-reports of alcohol consumption: state of the science and challenges for research. Addiction 2003;98(Suppl 2):1.
36.Toll BA, Cooney NL, McKee SA, et al. Correspondence between Interactive Voice Response (IVR) and Timeline Followback (TLFB) reports of drinking behavior. Addict Behav2006;31(4):726–731.
37.Searles JS, Helzer JE, Rose GL, et al. Concurrent and retrospective reports of alcohol consumption across 30, 90 and 366 days: interactive voice response compared with the timeline follow back. J Stud Alcohol 2002;63(3):352.
38.Serre F, Fatseas M, Debrabant R, et al. Ecological momentary assessment in alcohol, tobacco, cannabis and opiate dependence: a comparison of feasibility and validity. Drug Alcohol Depend 2012;126(1–2):118–123.
39.Voogt CV, Poelen EA, Kleinjan M, et al. Targeting young drinkers online: the effectiveness of a web-based brief alcohol intervention in reducing heavy drinking among college students: study protocol of a two-arm parallel group randomized controlled trial. BMC Public Health 2011;11:231.
40.Cohn AM, Hunter-Reel D, Hagman BT, et al. Promoting behavior change from alcohol use through mobile technology: the future of ecological momentary assessment. Alcohol Clin Exp Res2011;35(12):2209–2215.
41.Ball SA, Todd M, Tennen H, et al. Brief motivational enhancement and coping skills interventions for heavy drinking. Addict Behav 2007;32(6):1105.
42.Helzer JE, Badger GJ, Rose GL, et al. Decline in alcohol consumption during two years of daily reporting. J Stud Alcohol 2002;63(5):551.
43.American Psychiatric Association. Diagnostic and Statistical Manual, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Publishing, 2013.
44.American Psychiatric Association. Diagnostic and statistical manual of psychiatric disorders, 4th ed., Text Revision. Wahington, DC: American Psychiatric Publishing, 2000.
45.Dawson DA, Grant BF, Stinson FS, et al. Recovery from DSM-IV alcohol dependence: United States, 2001–2002. Addiction 2005;100(3):281–292.
46.Gueorguieva R, Wu R, Pittman B, et al. New insights into the efficacy of naltrexone based on trajectory-based reanalyses of two negative clinical trials. Biol Psychiatry 2007;61(11):1290–1295.
47.Cisler RA, Kowalchuk RK, Saunders SM, et al. Applying clinical significance methodology to alcoholism treatment trials: determining recovery outcome status with individual- and population-based measures. Alcohol Clin Exp Res 2005;29(11):1991–2000.
48.Gueorguieva R, Wu R, Donovan D, et al. Baseline trajectories of heavy drinking and their effects on postrandomization drinking in the COMBINE study: empirically derived predictors of drinking outcomes during treatment. Alcohol 2012;46(2):121–131.
49.Hutchison KE. Substance use disorders: realizing the promise of pharmacogenomics and personalized medicine. Annu Rev Clin Psychol 2010;6:577–589.
50.Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013;380(9859):2224–2260.
51.Ellison RC. Balancing the risks and benefits of moderate drinking. Ann N Y Acad Sci 2002;957:1.
52.Dawson DA. Alcohol consumption, alcohol dependence, and all-cause mortality. Alcohol Clin Exp Res 2000;24(1):72–81.
53.Rehm J, Baliunas D, Borges GL, et al. The relation between different dimensions of alcohol consumption and burden of disease: an overview. Addiction 2010;105(5):817–843.
54.Timko C, DeBenedetti A, Moos BS, et al. Predictors of 16-year mortality among individuals initiating help-seeking for an alcoholic use disorder. Alcohol Clin Exp Res 2006;30(10):1711.
55.Saitz R, Gaeta J, Cheng DM, et al. Risk of mortality during four years after substance detoxification in urban adults. J Urban Health 2007;84(2):272–282.
56.Costello RM. Long-term mortality from alcoholism: a descriptive analysis. J Stud Alcohol. 2006;67(5):694–699.
57.Johnson JE, Finney JW, Moos RH. Predictors of 5-year mortality following inpatient/residential group treatment for substance use disorders. Addict Behav 2005;30:1300.
58.Moss HB, Chen CM, Yi Hy. Subtypes of alcohol dependence in a nationally representative sample. Drug Alcohol Depend 2007;91:149.
59.Bischof G, Rumpf HJ, Hapke U, et al. Types of natural recovery from alcohol dependence: a cluster analytic approach. Addiction 2003;98(12):1737.
60.Fein G, Landman B. Treated and treatment-naive alcoholics come from different populations. Alcohol 2005;35(1):19–26.
61.Moos RH, Moos BS. Long-term influence of duration and frequency of participation in alcoholics anonymous on individuals with alcohol use disorders. J Consult Clin Psychol2004;72(1):81–90.
62.Ilgen MA, Wilbourne PL, Moos BS, et al. Problem-free drinking over 16 years among individuals with alcohol use disorders. Drug Alcohol Depend 2008;92(1–3):116.
63.Moos RH, Moos BS. Protective resources and long-term recovery from alcohol use disorders. Drug Alcohol Depend 2007;86(1):46.
64.Koob GF. The neurobiology of addiction: a neuroadaptational view relevant for diagnosis. Addiction 2006;101(s1):23.
65.Grant BF. Prevalence and correlates of alcohol use and DSM-IV alcohol dependence in the United States: results of the National Longitudinal Alcohol Epidemiologic Survey. J Stud Alcohol 1997;58(5):464.
66.Dawson DA, Grant BF, Li TK. Quantifying the risks associated with exceeding recommended drinking limits. Alcohol Clin Exp Res 2005;29(5):902–908.
67.Wodak AD, Saunders JB, Ewusi Mensah I. Severity of alcohol dependence in patients with alcoholic liver disease. Br Med J 1983;287(6403):1420.
68.Smith S, White J, Nelson C, et al. Severe alcohol-induced liver disease and the alcohol dependence syndrome. Alcohol Alcohol 2006;41(3):274.
69.Grant BF, Dawson DA, Stinson FS, et al. The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV): reliability of alcohol consumption, tobacco use, family history of depression and psychiatric diagnostic modules in a general population sample. Drug Alcohol Depend 2003;71(1):7–16.
70.Moss HB, Chen CM, Yi H-Y. Prospective follow-up of empirically derived Alcohol Dependence subtypes in wave 2 of the National Epidemiologic Survey on Alcohol And Related Conditions (NESARC): recovery status, alcohol use disorders and diagnostic criteria, alcohol consumption behavior, health status, and treatment seeking. Alcohol Clin Exp Res2010;34(6):1073–1083.
71.Lopez-Quintero C, Hasin DS, de Los Cobos JP, et al. Probability and predictors of remission from life-time nicotine, alcohol, cannabis or cocaine dependence: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Addiction 2011;106(3):657–669.
72.Sobell MB, Sobell LC. Guided self-change model of treatment for substance use disorders. J Cogn Psychother. 2005;19(3):199–210.
73.Whitlock EP, Polen MR, Green CA, et al. Behavioral Counseling Interventions in Primary Care to Reduce Risky/ Harmful Alcohol Use by Adults: A Summary of the Evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2004;140(7):557–568 + I564.
74.Zisserson RN, Palfai T, Saitz R. “No-contact” interventions for unhealthy college drinking: efficacy of alternatives to person-delivered intervention approaches. Subst Abuse2007;28(4):119.
75.Cowell AJ, Brown JM, Mills MJ, et al. Cost-effectiveness analysis of motivational interviewing with feedback to reduce drinking among a sample of college students. J Stud Alcohol Drugs.Mar 2012;73(2):226–237.
76.Carey KB, Scott-Sheldon LA, Elliott JC, et al. Face-to-face versus computer-delivered alcohol interventions for college drinkers: a meta-analytic review, 1998 to 2010. Clin Psychol Rev2012;32(8):690–703.
77.Field CA, Baird J, Saitz R, et al. The mixed evidence for brief intervention in emergency departments, trauma care centers, and inpatient hospital settings: what should we do? Alcohol Clin Exp Res2010;34(12):2004–2010.
78.Saitz R, Palfai TP, Cheng DM, et al. Brief intervention for medical inpatients with unhealthy alcohol use: a randomized, controlled trial. Ann Intern Med 2007;146(3):167–176.
79.Humphreys K, Weingardt KR, Horst D, et al. Prevalence and predictors of research participant eligibility criteria in alcohol treatment outcome studies, 1970–98. Addiction2005;100(9):1249–1257.
80.Miller WR, Walters ST, Bennett ME. How effective is alcoholism treatment in the United States? J Stud Alcohol 2001;62(2):211–220.
81.Moos RH, Finney JW, Ouimette PC, et al. A comparative evaluation of substance abuse treatment: I. Treatment orientation, amount of care, and 1-year outcomes. Alcohol Clin Exp Res1999;23(3):529–536.
82.Anton RF, O’Malley SS, Ciraulo DA, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA2006;295(17):2003.
83.O’Malley SS, Rounsaville BJ, Farren C, et al. Initial and maintenance naltrexone treatment for alcohol dependence using primary care vs specialty care: a nested sequence of 3 randomized trials. Arch Intern Med 2003;163(14):1695–1704.
84.American Society of Addiction M. ASAM patient placement criteria for the treatment of substance-related disorders, (2nd ed.—Revised). Annapolis Junction, MD: ASAM Publications Distribution, 2001.
85.Lieber CS, Weiss DG, Groszmann R, et al. I. Veterans Affairs Cooperative Study of polyenylphosphatidylcholine in alcoholic liver disease: effects on drinking behavior by nurse/physician teams. Alcohol Clin Exp Res 2003;27(11):1757.
86.Willenbring ML, Olson DH. A randomized trial of integrated outpatient treatment for medically ill alcoholic men. Arch Intern Med 1999;159(16):1946–1952.
87.Willenbring ML, Olson DH, Bielinski J. Integrated outpatients treatment for medically ill alcoholic men: results from a quasi-experimental study. J Stud Alcohol 1995;56(3):337.
88.Kim TW, Saitz R, Cheng DM, et al. Initiation and engagement in chronic disease management care for substance dependence. Drug Alcohol Depend 2011;115(1–2):80–86.
89.Mark TL, Levit KR, Buck JA, et al. Mental health treatment expenditure trends, 1986–2003. Psychiatr Serv 2007;58(8):1041.
90.Hingson R, McGovern T, Howland J, et al. Reducing alcohol-impaired driving in Massachusetts: The saving lives program. Am J Public Health 1996;86(6):791.
91.Finney JW, Hahn AC, Moos RH. The effectiveness of inpatient and outpatient treatment for alcohol abuse: the need to focus on mediators and moderators of setting effects. Addiction1996;91(12):1773–1796.
92.Matching Alcoholism Treatments to Client Heterogeneity: Project MATCH posttreatment drinking outcomes. J Stud Alcohol 1997;58(1):7.
93.Vaillant GE. A 60-year follow-up of alcoholic men. Addiction 2003;98(8):1043.
94.Orford J, Hodgson R, Copello A, et al. The clients’ perspective on change during treatment for an alcohol problem: qualitative analysis of follow-up interviews in the UK Alcohol Treatment Trial. Addiction2006;101(1):60.
95.McKellar JD, Harris AH, Moos RH. Predictors of outcome for patients with substance-use disorders five years after treatment dropout. J Stud Alcohol 2006;67(5):685–693.
96.Timko C, Billow R, DeBenedetti A. Determinants of 12-step group affiliation and moderators of the affiliation-abstinence relationship. Drug Alcohol Depend 2006;83(2):111–121.
97.Dawson DA, Goldstein RB, Grant BF. Rates and correlates of relapse among individuals in remission from DSM-IV alcohol dependence: a 3-year follow-up. Alcohol Clin Exp Res2007;31(12):2036.
98.Moos RH. Theory-based active ingredients of effective treatments for substance use disorders. Drug Alcohol Depend 2007;88(2–3):109–121.
99.OppNet: Basic Behavioral and Social Science Opportunity Netowrk. 2013; http://oppnet.nih.gov/index.asp. Accessed 04/28/2013, 2013.
100.Zywiak WH, Longabaugh R, Wirtz PW. Decomposing the relationships between pretreatment social network characteristics and alcohol treatment outcome. J Stud Alcohol2002;63(1):114.
101.Powers MB, Vedel E, Emmelkamp PMG. Behavioral couples therapy (BCT) for alcohol and drug use disorders: a meta-analysis. Clin Psychol Rev 2008;28(6):952.
102.Heilig M, Egli M. Pharmacological treatment of alcohol dependence: target symptoms and target mechanisms. Pharmacol Ther 2006;111(3):855–876.
*Throughout this chapter, I distinguish between treatment, which is delivered by trained professionals for a fee, and mutual support obtained through voluntary groups such as Alcoholics Anonymous