Stacie Zelman
EPIDEMIOLOGY
![]() Precipitous delivery in an emergency is a relatively uncommon occurrence. However, when a patient in active labor does present to the ED, careful preparation and education can help avoid serious complications of labor and delivery.
Precipitous delivery in an emergency is a relatively uncommon occurrence. However, when a patient in active labor does present to the ED, careful preparation and education can help avoid serious complications of labor and delivery.
CLINICAL FEATURES
![]() Any pregnant woman who is beyond 20 weeks’ gestation and appears to be in active labor should be evaluated expeditiously. Evaluation includes maternal vital signs, especially blood pressure, and fetal heart monitoring.
Any pregnant woman who is beyond 20 weeks’ gestation and appears to be in active labor should be evaluated expeditiously. Evaluation includes maternal vital signs, especially blood pressure, and fetal heart monitoring.
![]() A persistently slow fetal heart rate (<100 beats/min) is an indicator of fetal distress.
A persistently slow fetal heart rate (<100 beats/min) is an indicator of fetal distress.
![]() History should include time of onset of contractions, leakage of fluid, vaginal bleeding, and prenatal care.
History should include time of onset of contractions, leakage of fluid, vaginal bleeding, and prenatal care.
![]() A focused physical examination should include an abdominal examination evaluating fundal height, abdominal or uterine tenderness, and fetal position. A bimanual or sterile speculum examination should be performed if no contraindications exist.
A focused physical examination should include an abdominal examination evaluating fundal height, abdominal or uterine tenderness, and fetal position. A bimanual or sterile speculum examination should be performed if no contraindications exist.
![]() False labor is characterized by irregular, brief contractions usually confined to the lower abdomen. These contractions, commonly called Braxton Hicks contractions, are irregular in intensity and duration.
False labor is characterized by irregular, brief contractions usually confined to the lower abdomen. These contractions, commonly called Braxton Hicks contractions, are irregular in intensity and duration.
![]() True labor is characterized by painful, regular contractions of steadily increasing intensity and duration leading to progressive cervical dilatation. True labor typically begins in the fundal region and upper abdomen and radiates into the pelvis and lower back.
True labor is characterized by painful, regular contractions of steadily increasing intensity and duration leading to progressive cervical dilatation. True labor typically begins in the fundal region and upper abdomen and radiates into the pelvis and lower back.
DIAGNOSIS AND DIFFERENTIAL
![]() Patients without vaginal bleeding should be assessed with a sterile speculum examination and bimanual examination to assess the progression of labor, cervical dilation, and rupture of membranes.
Patients without vaginal bleeding should be assessed with a sterile speculum examination and bimanual examination to assess the progression of labor, cervical dilation, and rupture of membranes.
![]() Patients with active vaginal bleeding require initial evaluation with ultrasound to rule out placenta previa.
Patients with active vaginal bleeding require initial evaluation with ultrasound to rule out placenta previa.
![]() Abruptio placentae should be considered in patients with a tender, firm uterus and marked bleeding. However, bleeding does not have to be present.
Abruptio placentae should be considered in patients with a tender, firm uterus and marked bleeding. However, bleeding does not have to be present.
![]() Spontaneous rupture of membranes typically occurs with a gush of clear or blood-tinged fluid. If ruptured membranes are suspected, a sterile speculum examination should be performed and amniotic fluid obtained from the fornix or vaginal vault. Amniotic fluid is alkaline and will stain nitrazine paper dark blue and will “fern” if dried on a slide (Fig. 64-1). The presence of meconium in amniotic fluid should be noted.
Spontaneous rupture of membranes typically occurs with a gush of clear or blood-tinged fluid. If ruptured membranes are suspected, a sterile speculum examination should be performed and amniotic fluid obtained from the fornix or vaginal vault. Amniotic fluid is alkaline and will stain nitrazine paper dark blue and will “fern” if dried on a slide (Fig. 64-1). The presence of meconium in amniotic fluid should be noted.
![]() Avoid digital examinations in the preterm patient in whom prolongation of gestation is desired. Even one examination increases the chance of infection, especially if premature rupture of membranes is suspected.
Avoid digital examinations in the preterm patient in whom prolongation of gestation is desired. Even one examination increases the chance of infection, especially if premature rupture of membranes is suspected.
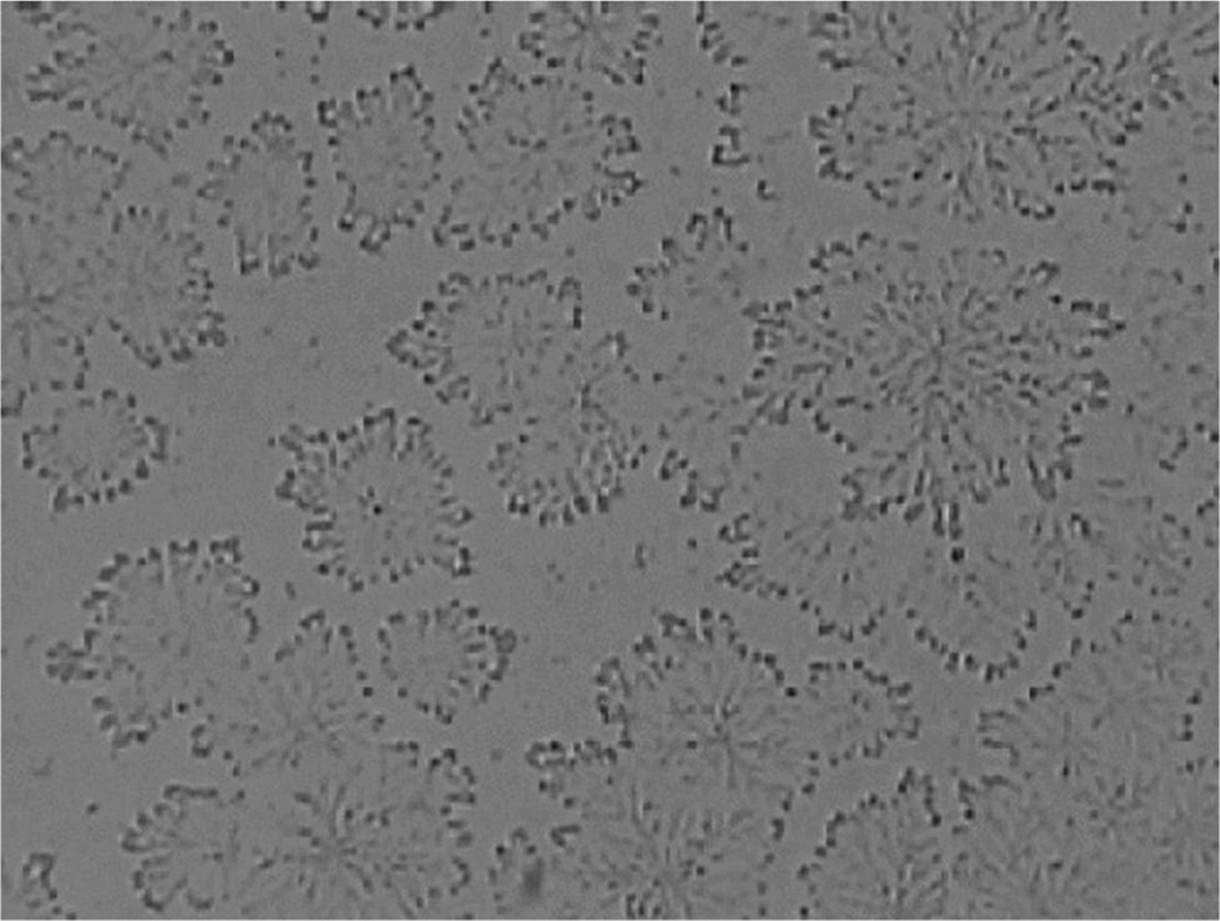
FIG. 64-1. Typical ferning of dried amniotic fluid
EMERGENCY DEPARTMENT CARE
![]() If the cervix is dilated in a woman experiencing active contractions, further transport, even short distances, may be hazardous. Preparations should be made for emergency delivery.
If the cervix is dilated in a woman experiencing active contractions, further transport, even short distances, may be hazardous. Preparations should be made for emergency delivery.
![]() Assess fetal position by physical examination, and confirm by ultrasound, if possible.
Assess fetal position by physical examination, and confirm by ultrasound, if possible.
![]() Place the patient in the dorsal lithotomy position.
Place the patient in the dorsal lithotomy position.
![]() Notify an obstetrician, if one is available.
Notify an obstetrician, if one is available.
EMERGENCY DELIVERY PROCEDURE (FIG. 64-2)
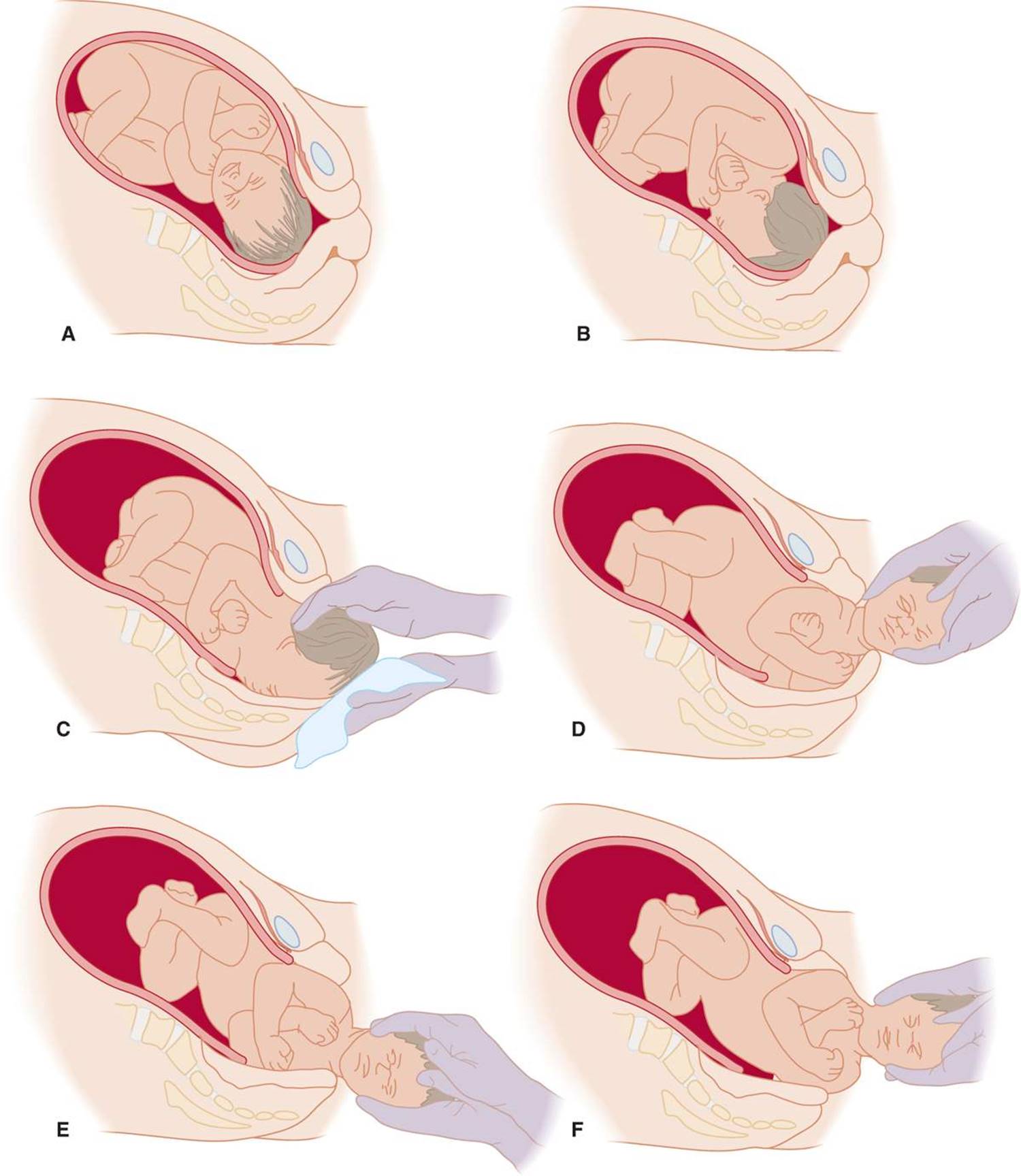
FIG. 64-2. Movements of normal delivery. Mechanism of labor and delivery for vertex presentations. A. Engagement, flexion, and descent. B. Internal rotation. C. Extension and delivery of the head. After delivery of the head, the neck is checked for encirclement by the umbilical cord. D. External rotation, bringing the thorax into the anteroposterior diameter of the pelvis. E. Delivery of the anterior shoulder. F. Delivery of the posterior shoulder. Note that after delivery, the head is supported and used to gently guide delivery of the shoulder. Traction should be minimized.
1. Control of the delivery of the neonate is the major challenge.
a. As the infant’s head emerges from the introitus, support the perineum with a sterile towel placed along the inferior portion of the perineum with one hand while supporting the fetal head with the other.
b. Exert mild counterpressure to prevent the rapid expulsion of the fetal head, which may lead to third- or fourth-degree perineal tears.
c. As the infant’s head presents, use the inferior hand to control the fetal chin while keeping the superior hand on the crown of the head, supporting the delivery.
d. This controlled extension of the fetal head will aid in the atraumatic delivery.
e. Ask the mother to breathe through contractions rather than bearing down and attempting to push the baby out rapidly.
2. After delivery of the head, palpate the neck for the presence of a nuchal cord.
a. A nuchal cord is present in up to 35% of all cephalad-presenting deliveries.
b. If the cord is loose, reduce it over the infant’s head; the delivery may then proceed as usual.
c. If the cord is tightly wound, clamp it in the most accessible area using two clamps in close proximity and cut to allow delivery of the infant.
3. After delivery of the head, the head will restitute or turn to one side or the other.
a. As the head rotates, place your hands on either side, providing gentle downward traction to deliver the anterior shoulder.
b. Then guide the fetus upward, delivering the posterior shoulder and allowing the remainder of the infant to be delivered.
4. Place your posterior (left) hand underneath the infant’s axilla before delivering the rest of the body. Use the anterior hand to grasp the infant’s ankles and ensure a firm grip.
5. Wrap the infant in a towel and stimulate it while drying.
6. Double clamp the umbilical cord and cut with sterile scissors.
7. Finish drying. Place the infant in a warm incubator, where postnatal care may be provided and Apgar scores calculated at 1 and 5 minutes after delivery. Scoring includes general color, tone, heart rate, respiratory effort, and reflexes.
8. Use of routine episiotomy for a normal spontaneous vaginal delivery is discouraged since it increases the incidence of third- and fourth-degree lacerations at the time of delivery.
9. If an episiotomy is necessary (eg, with a breech presentation), it may be performed as follows:
a. Inject a solution of 5 to 10 mL of 1% lidocaine with a small-gauge needle into the posterior fourchette and perineum.
b. While protecting the infant’s head, make a 2- to 3 -cm cut with scissors to extend the vaginal opening.
c. Support the incision with manual pressure from below, taking care not to allow the incision to extend into the rectum.
CORD PROLAPSE
If bimanual examination shows a palpable, pulsating cord:
a. Do not remove the examining hand; use the hand to elevate the presenting fetal part to reduce compression of the cord.
b. Immediate obstetric assistance is necessary, as a cesarean section is indicated.
c. Keep the examining hand in the vagina while the patient is transported and prepped for surgery to prevent further compression of the cord by the fetal head. Do not attempt to reduce the cord.
SHOULDER DYSTOCIA
![]() Shoulder dystocia first recognized after the delivery of the fetal head, when routine downward traction is insufficient to deliver the anterior shoulder. The anterior shoulder is trapped behind the pubic symphysis.
Shoulder dystocia first recognized after the delivery of the fetal head, when routine downward traction is insufficient to deliver the anterior shoulder. The anterior shoulder is trapped behind the pubic symphysis.
![]() After delivery of the infant’s head, the head retracts tightly against the perineum (“Turtle sign”).
After delivery of the infant’s head, the head retracts tightly against the perineum (“Turtle sign”).
![]() Upon recognizing shoulder dystocia, suction the infant’s nose and mouth and call for assistance to position the mother in the extreme lithotomy position, with legs sharply flexed up to the abdomen (McRoberts maneuver) and held by the mother or assistant.
Upon recognizing shoulder dystocia, suction the infant’s nose and mouth and call for assistance to position the mother in the extreme lithotomy position, with legs sharply flexed up to the abdomen (McRoberts maneuver) and held by the mother or assistant.
![]() Drain the bladder.
Drain the bladder.
![]() A generous episiotomy also may facilitate delivery.
A generous episiotomy also may facilitate delivery.
![]() Next, an assistant should apply suprapubic pressure to disimpact the anterior shoulder from the pubic symphysis.
Next, an assistant should apply suprapubic pressure to disimpact the anterior shoulder from the pubic symphysis.
![]() Do not apply fundal pressure because this will further force the shoulder against the pelvic rim.
Do not apply fundal pressure because this will further force the shoulder against the pelvic rim.
![]() A Woods corkscrew maneuver may be attempted—place a hand behind the posterior shoulder of the infant, and rotate the shoulder girdle 180 degrees.
A Woods corkscrew maneuver may be attempted—place a hand behind the posterior shoulder of the infant, and rotate the shoulder girdle 180 degrees.
BREECH PRESENTATION
![]() The primary concern with breech presentation is head entrapment.
The primary concern with breech presentation is head entrapment.
![]() Breech presentations may be classified as frank, complete, incomplete, or footling.
Breech presentations may be classified as frank, complete, incomplete, or footling.
![]() In any breech delivery, immediate obstetric consultation should be requested.
In any breech delivery, immediate obstetric consultation should be requested.
![]() Frank and complete breech presentations:
Frank and complete breech presentations:
a. Serve as a dilating wedge nearly as well as the fetal head, and delivery may proceed in an uncomplicated fashion.
b. Main point is to allow the delivery to progress spontaneously. This lets the presenting portion of the fetus to dilate the cervix maximally.
c. Consult obstetrical texts for a detailed description of maneuvers for breech delivery.
![]() Footling and incomplete breech positions are not considered safe for vaginal delivery because of the possibility of cord prolapse or incomplete dilatation of the cervix.
Footling and incomplete breech positions are not considered safe for vaginal delivery because of the possibility of cord prolapse or incomplete dilatation of the cervix.
POSTPARTUM CARE
![]() The placenta should be allowed to separate spontaneously and assisted with gentle traction.
The placenta should be allowed to separate spontaneously and assisted with gentle traction.
![]() Aggressive traction on the cord risks uterine inversion, tearing of the cord, or disruption of the placenta, which can result in severe vaginal bleeding.
Aggressive traction on the cord risks uterine inversion, tearing of the cord, or disruption of the placenta, which can result in severe vaginal bleeding.
![]() After removal of the placenta, gently massage the uterus to promote contraction.
After removal of the placenta, gently massage the uterus to promote contraction.
![]() Infuse oxytocin 10 to 40 U/1000 mL NS at a moderate rate to maintain uterine contraction. Oxytocin may also be given as 10 U IM.
Infuse oxytocin 10 to 40 U/1000 mL NS at a moderate rate to maintain uterine contraction. Oxytocin may also be given as 10 U IM.
![]() Episiotomy or laceration repair may be delayed until an experienced obstetrician is able to close the laceration and inspect the patient for fourth-degree (rectovaginal) tears.
Episiotomy or laceration repair may be delayed until an experienced obstetrician is able to close the laceration and inspect the patient for fourth-degree (rectovaginal) tears.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 105, “Emergency Delivery,” by Michael J. VanRooyen and Jennifer A. Scott.