Justin W. Sales
EPIDEMIOLOGY
![]() Pediatric urinary tract infections (UTIs) are now the most common serious bacterial infection in children following the introduction of successful immunizations.
Pediatric urinary tract infections (UTIs) are now the most common serious bacterial infection in children following the introduction of successful immunizations.
![]() Pediatric UTI occurs in up to 8% of febrile children presenting to the ED with no obvious source of infection.
Pediatric UTI occurs in up to 8% of febrile children presenting to the ED with no obvious source of infection.
![]() Two percent of boys and up to 8% of girls have a UTI during the first 8 years of life, with the highest incidence during the first year of life in both sexes.
Two percent of boys and up to 8% of girls have a UTI during the first 8 years of life, with the highest incidence during the first year of life in both sexes.
![]() Prevalence of UTI is three times higher in females; amongst males, uncircumcised infant boys have a 10 times higher risk than circumcised boys.
Prevalence of UTI is three times higher in females; amongst males, uncircumcised infant boys have a 10 times higher risk than circumcised boys.
PATHOPHYSIOLOGY
![]() UTIs typically occur from retrograde contamination of the lower urinary tract with organisms from the perineum and periurethral area. In neonates, however, UTIs typically develop after seeding of the renal parenchyma from hematogenous spread.
UTIs typically occur from retrograde contamination of the lower urinary tract with organisms from the perineum and periurethral area. In neonates, however, UTIs typically develop after seeding of the renal parenchyma from hematogenous spread.
![]() Escherichia coli is the most common cause of UTI in children. Additional pathogens include Klebsiella, Proteus, and Enterobacter species.
Escherichia coli is the most common cause of UTI in children. Additional pathogens include Klebsiella, Proteus, and Enterobacter species.
![]() Enterococcus species, Staphylococcus aureus, and group B streptococci are the most common gram-positive organisms and are more common in neonates. Chlamydia trachomatis may be present in adolescents with urinary tract symptoms and microhematuria. Adenovirus may cause culture-negative acute cystitis in young boys.
Enterococcus species, Staphylococcus aureus, and group B streptococci are the most common gram-positive organisms and are more common in neonates. Chlamydia trachomatis may be present in adolescents with urinary tract symptoms and microhematuria. Adenovirus may cause culture-negative acute cystitis in young boys.
![]() Factors influencing the development of UTI include virulence of the pathogen, congenital urinary tract abnormalities, vesicoureteral reflux, urolithiasis, poor hygiene, voluntary urinary retention, circumcision, and constipation.
Factors influencing the development of UTI include virulence of the pathogen, congenital urinary tract abnormalities, vesicoureteral reflux, urolithiasis, poor hygiene, voluntary urinary retention, circumcision, and constipation.
CLINICAL FEATURES
![]() Clinical features vary markedly by age as described below.
Clinical features vary markedly by age as described below.
![]() Neonatal UTI may present with a septic-like appearance. Features may include fever, jaundice, poor feeding, irritability, and lethargy.
Neonatal UTI may present with a septic-like appearance. Features may include fever, jaundice, poor feeding, irritability, and lethargy.
![]() Infants and young children typically present with gastrointestinal complaints, which may include fever, abdominal pain, vomiting, and change in appetite.
Infants and young children typically present with gastrointestinal complaints, which may include fever, abdominal pain, vomiting, and change in appetite.
![]() In school-aged children and adolescents, cystitis and urethritis (lower tract disease) typically present with urinary frequency, urgency, hesitancy, and dysuria. Pyelonephritis (upper tract disease) typically presents with fever, chills, back or flank pain, vomiting, and dehydration.
In school-aged children and adolescents, cystitis and urethritis (lower tract disease) typically present with urinary frequency, urgency, hesitancy, and dysuria. Pyelonephritis (upper tract disease) typically presents with fever, chills, back or flank pain, vomiting, and dehydration.
DIAGNOSIS AND DIFFERENTIAL
![]() The American Acadamy of Pediatrics clinical practice guideline from 2011 proposes criteria for UTI in infants and young children 2 to 24 months of age to include evidence of pyuria in addition to positive culture results.
The American Acadamy of Pediatrics clinical practice guideline from 2011 proposes criteria for UTI in infants and young children 2 to 24 months of age to include evidence of pyuria in addition to positive culture results.
![]() For infants less than 2 months of age, urine culture remains the gold standard for this age group.
For infants less than 2 months of age, urine culture remains the gold standard for this age group.
![]() A positive urine culture is defined as ≥5 × 104 colony-forming units (CFU)/mL of a single urinary pathogen. Growth of a urinary pathogen in any number from a suprapubic aspiration is considered a positive culture.
A positive urine culture is defined as ≥5 × 104 colony-forming units (CFU)/mL of a single urinary pathogen. Growth of a urinary pathogen in any number from a suprapubic aspiration is considered a positive culture.
![]() Urine culture results are not available to the emergency physician during the initial visit; therefore, urine chemical test strips that can detect leukocyte esterase and urinary nitrites in conjunction with microscopic urinalysis are employed to help predict the results of the urine culture and initiate treatment.
Urine culture results are not available to the emergency physician during the initial visit; therefore, urine chemical test strips that can detect leukocyte esterase and urinary nitrites in conjunction with microscopic urinalysis are employed to help predict the results of the urine culture and initiate treatment.
![]() In infants and children who are not able to void on command, bladder catheterization is the preferred method for urine collection. Suprapubic aspiration, although invasive, is also an acceptable means of obtaining a cultured specimen. High false-positive results and low specificity seriously limit the use of perineal bag specimens.
In infants and children who are not able to void on command, bladder catheterization is the preferred method for urine collection. Suprapubic aspiration, although invasive, is also an acceptable means of obtaining a cultured specimen. High false-positive results and low specificity seriously limit the use of perineal bag specimens.
![]() Urinary nitrites and leukocyte esterase alone are not sensitive markers for children who empty their bladders frequently. Urinary nitrites are highly specific and therefore helpful when positive.
Urinary nitrites and leukocyte esterase alone are not sensitive markers for children who empty their bladders frequently. Urinary nitrites are highly specific and therefore helpful when positive.
![]() Pyuria alone does not confirm a UTI. Causes of culture-negative pyuria include urethritis from kawa-saki disease, pelvic abscess or infections (appendicitis, pelvic inflammatory disease, colitis), or sexually transmitted diseases.
Pyuria alone does not confirm a UTI. Causes of culture-negative pyuria include urethritis from kawa-saki disease, pelvic abscess or infections (appendicitis, pelvic inflammatory disease, colitis), or sexually transmitted diseases.
![]() Causes of culture-negative dysuria include viral ure-thritis/cystitis, balanitis, and irritant urethritis from poor hygiene or clothing.
Causes of culture-negative dysuria include viral ure-thritis/cystitis, balanitis, and irritant urethritis from poor hygiene or clothing.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment and disposition depends on the age of the patient and severity of the illness.
Treatment and disposition depends on the age of the patient and severity of the illness.
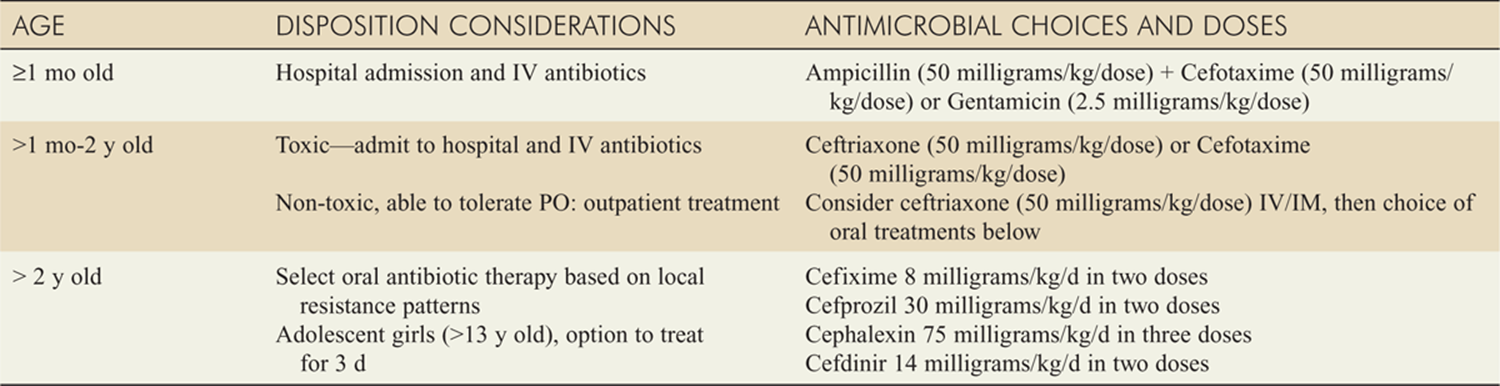
![]() Physicians should be familiar with the local susceptibilities of the common urinary pathogens in their geographic region. Medications listed in Table 77-1 are generally acceptable, but emerging resistance is a continuing problem.
Physicians should be familiar with the local susceptibilities of the common urinary pathogens in their geographic region. Medications listed in Table 77-1 are generally acceptable, but emerging resistance is a continuing problem.
![]() Neonates (under 1 month of age) with fever and UTI should be hospitalized and given intravenous antibiotics.
Neonates (under 1 month of age) with fever and UTI should be hospitalized and given intravenous antibiotics.
![]() Children over 1 month of age with fever and uncomplicated UTI may be appropriate for outpatient care with oral antibiotics if they appear well, can tolerate oral medication, are not dehydrated, and are not immunocompromised. They may receive a single dose of intramuscular or intravenous ceftriaxone (50 milligrams/kg) in the emergency department and start on outpatient oral antibiotics with close primary care follow-up.
Children over 1 month of age with fever and uncomplicated UTI may be appropriate for outpatient care with oral antibiotics if they appear well, can tolerate oral medication, are not dehydrated, and are not immunocompromised. They may receive a single dose of intramuscular or intravenous ceftriaxone (50 milligrams/kg) in the emergency department and start on outpatient oral antibiotics with close primary care follow-up.
![]() Older infants and children with fever and UTI complicated by vomiting, dehydration, any suspicion of sepsis, or inability to take oral antibiotics are hospitalized for intravenous antibiotics until they are afebrile and able to take oral medications.
Older infants and children with fever and UTI complicated by vomiting, dehydration, any suspicion of sepsis, or inability to take oral antibiotics are hospitalized for intravenous antibiotics until they are afebrile and able to take oral medications.
![]() Length of antimicrobial therapy should be 7 to 14 days.
Length of antimicrobial therapy should be 7 to 14 days.
![]() Adolescent girls (>13 years old) with UTI may be treated like adults with option for 3-day oral antibiotic regimen.
Adolescent girls (>13 years old) with UTI may be treated like adults with option for 3-day oral antibiotic regimen.
![]() Febrile infants with UTIs should undergo renal and bladder ultrasonography. The necessity of routine voiding cystourethrogram after the first febrile UTI has recently been challenged unless ultrasonography reveals high-grade or obstructive uropathy. This testing is arranged as an outpatient or performed during hospitalization and is not typically facilitated from the emergency department.
Febrile infants with UTIs should undergo renal and bladder ultrasonography. The necessity of routine voiding cystourethrogram after the first febrile UTI has recently been challenged unless ultrasonography reveals high-grade or obstructive uropathy. This testing is arranged as an outpatient or performed during hospitalization and is not typically facilitated from the emergency department.
TABLE 77-1 Treatment of UTI in Infants and Children
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 126, “Urinary Tract Infection in Infants and Children,” by Julie S. Byerley and Michael J. Steiner.