Basic Principles of the Neurological Examination
Stance and Gait
Examination of the Head and Cranial Nerves
Examination of the Upper Limbs
Examination of the Trunk
Examination of the Lower Limbs
Examination of the Autonomic Nervous System
Neurologically Relevant Aspects of the General Physical Examination
Neuropsychological and Psychiatric Examination
Special Considerations in the Neurological Examination of Infants and Young Children
![]() Basic Principles of the Neurological Examination
Basic Principles of the Neurological Examination
Neurological diseases can often be diagnosed based on a carefully elicited history in combination with the physical examination. In order to ensure completeness, the examining physician should examine all patients according to the same general scheme, making individual variations where required. One may either test the individual components of the nervous system in a particular sequence (cranial nerves, reflexes, and motor, sensory, and autonomic function), or else orient the examination along topographic lines (head, upper limbs, trunk, lower limbs). The presentation in this chapter is topographically organized.
Neurology stands by itself as an independent medical specialty and field of research. Most neurological illnesses affect only the nervous system. Nonetheless, general medical illnesses often manifest themselves with neurological symptoms and signs (cf. p. 120ff.). The clinical neurological examination must therefore always include a general physical examination.
The practicing neurologist should indeed lay emphasis on the neurological aspects of the physical examination but cannot neglect its general aspects. Some of the basic principles of physical examination are listed below.
The examiner must talk to the patient, briefly explaining the purpose of individual steps in the examination where appropriate. This holds for patients of all ages, even more so for children.
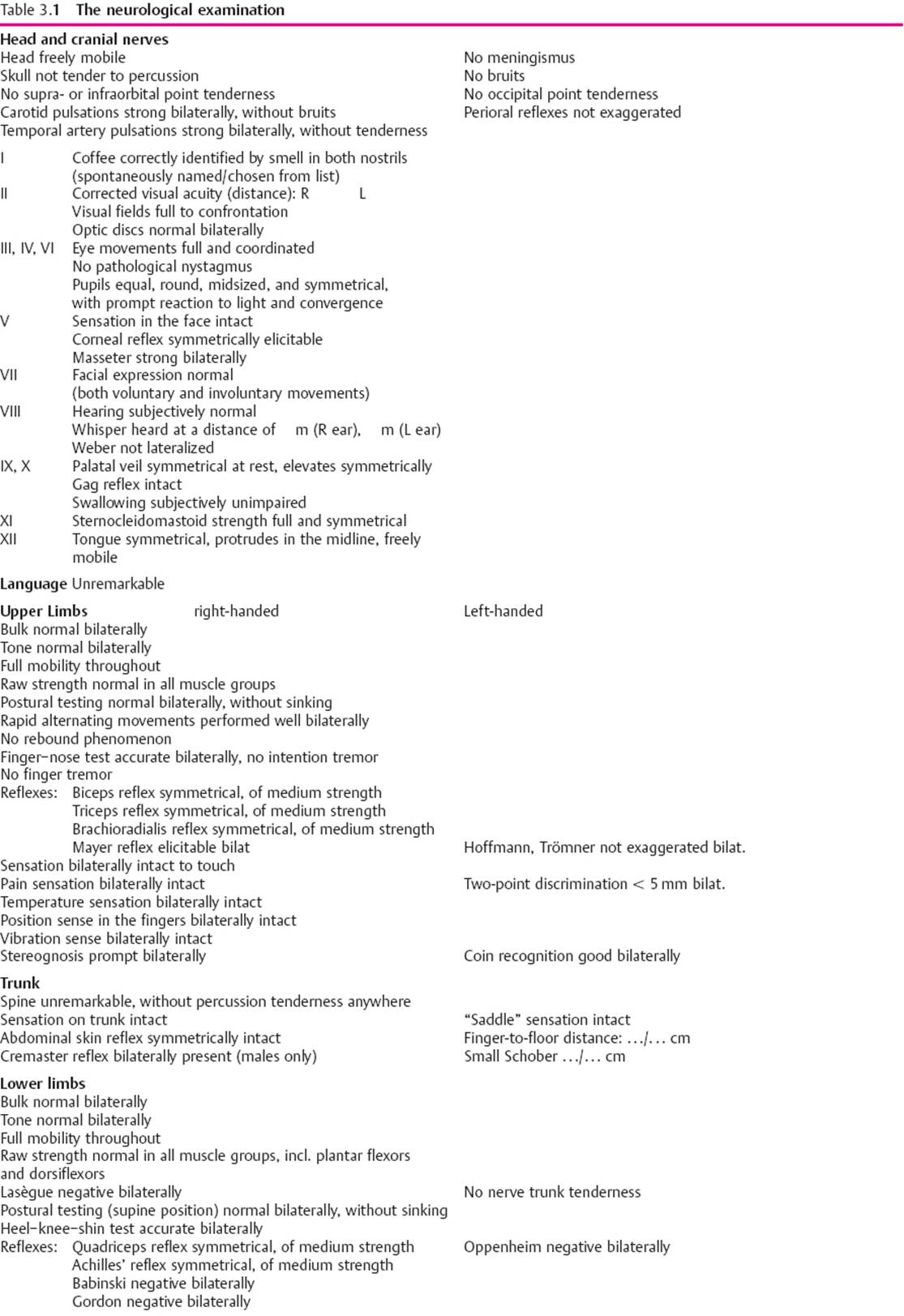
In principle, the neurological examination should always be complete and should always be performed in the same sequence, though the examiner is free to use whatever sequence he or she prefers. The individual components of the examination are listed in Table 3.1. In certain exceptional situations, a highly experienced clinician may choose to perform only a partial examination. This is generally to be avoided, however, as even the best neurologist can miss something important in this way. In addition, a thorough, methodical examination helps reassure the patient that the physician is competent and attentive.
Patients should be examined undressed, after being given clear instructions about which clothes to remove, usually everything but their underwear. The spine cannot be examined if the upper body remains clothed and, if the patient is wearing socks, sensation cannot be tested in the feet, and the Babinski reflex cannot be elicited.
As we have already stressed, the examination should always be systematic and complete; yet, the tentative diagnosis (or diagnoses) suggested by the history will direct the clinician to lay particular attention on certain aspects of the examination. There is no sense in the mechanical, unthinking performance of a rigidly identical examination on every patient.
As soon as possible after the examination is completed, the examiner should document the findings in writing. Global statements such as “Neuro unremarkable” are worthless. The findings can be summarized in an outline such as the one provided in Table 3.1. The main purpose of precise documentation is to enable the clinician to follow the development of a disease process from one examination to the next. It is also obviously indispensable for medicolegal reasons.
Moreover, certain findings should be quantified or numerically graded, particularly muscle strength (see Table 3.4, p. 30). Sensory disturbances should be documented precisely in terms of their topography and extent.
![]() Stance and Gait
Stance and Gait
General remarks. Though stance and gait are listed at the bottom of Table 3.1, we in fact recommend testing these functions as the first step in the examination of the undressed patient. Mere observation of the patient in a standing position can reveal evidence of a disease process, e.g., muscle atrophy, spinal deformities, and winging of the scapula. The patient's posture at rest may be abnormal, e.g., the exaggerated lumbar lordosis of muscular dystrophy (cf. Fig. 14.3, p. 266) or the stooped, rigid posture of the patient with Parkinson disease (cf. Fig. 6.33, p. 128). Stance and gait are best examined with the patient barefoot; meaningful findings can be obtained only if the patient has enough room to walk in. The testing of stance and gait often provides important clues to the type of disease process that is present. The sequence of tests is shown in Fig. 3.1a–g. The most important features of gait are whether the patient can walk at normal speed and without limping. If the patient limps, then the pathological side is the side that bears weight for the shorter time. The examiner should note the length of the patient's steps, the manner in which the feet are planted on and rolled off the ground, and the accompanying swinging of the arms. Some characteristic disturbances of gait are described in Table 3.2.
Walking on tiptoe and walking on the heels (Figs. 3.1b, c) let the clinician judge the strength of the calf muscles and the foot and toe extensors. If the plantar flexors are only mildly weak, the patient will still be able to walk on tiptoe, but will not be able to raise himself or herself on tiptoe while standing on one leg, or hop repeatedly on one foot (10 times in succession).
The “tightrope walk” (heel-to-toe walk) (Fig. 3.1d) is a very sensitive test of equilibrium and gait stability. The patient is instructed to place one foot firmly and directly in front of the other, at first while looking at the floor, then while looking straight ahead, and finally while looking at the ceiling. Heel-to-toe walking should be possible under all of these conditions. Heel-to-toe walking with the eyes closed is a more difficult task that many normal persons cannot perform.
The Romberg test (Fig. 3.1e) is a further test of equilibrium. The patient is asked to stand with the feet together and parallel and with eyes closed, for at least 20 seconds. This should be accomplished calmly and easily, without any appreciable swaying. The test can be made more difficult by having the patient turn or incline the head to one side. It can also be performed in combination with positional testing of the arms (see below).
The functions of the vestibular system (p. 201) and cerebellum (p. 80) can be tested in a number of ways, including with the Unterberger step test (Fig. 3.1f). The patient walks in place, with the eyes closed, raising the knee to the horizontal or above with each step. After 50 steps, the patient should have rotated no more than 45º from his or her original position. Larger rotations suggest disfunction of the vestibular apparatus on the side to which the patient has turned, or of the cerebellar hemisphere on that side. In the “star gait” test of Babinski and Weil, the patient keeps the eyes closed and walks two steps forward and two steps back, repeatedly. Disfunction of the vestibular system manifests itself as involuntary turning to the side of the lesion. In blind walking, the patient first looks at the examiner, who is standing some distance away, then closes the eyes, and walks toward him or her. Vestibular lesions cause a deviation to the side of the lesion.
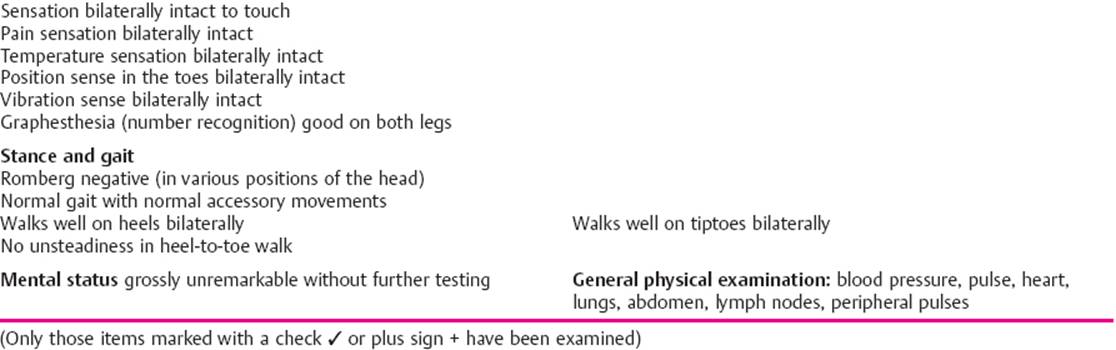
A number of common gait abnormalities are illustrated in Fig 3.2.

Fig. 3.1 Tests of stance and gait. a Normal gait. Note normal step length and arm swing. b Walking on tiptoes. c Walking on heels. d Heel-to-toe walking. One foot is placed precisely in front of the other. e Romberg test with eyes closed, combined with postural test of the upper limbs. f Unterberger step test: walking in place with eyes closed. See text for interpretation of results. g Babinski–Weil test with “star gait” (marche en étoile): the patient is asked to take two steps forward and two steps back, repeatedly, with eyes closed. For interpretation, see text.
Table 3.2 Characteristic disturbances of gait
|
Designation |
Abnormalities of gait |
Causes, Remarks |
|
Spastic gait (Fig. 3.2) |
slow, stiff, with audible dragging of the soles of the feet across the ground |
bilateral pyramidal tract lesion |
|
Ataxic gait (Fig. 3.2) |
uncoordinated, stamping, unsteady, deviating irregularly from a straight line; heel-to-toe walking tion, peripheral neuropathy impossible |
cerebellar dysfunction, posterior column dysfunction peripheral neuropathy |
|
Spastic–ataxic gait (Fig. 3.2) |
combination of the two above disorders; jerky, stiff, inharmonious gait |
most commonly seen in multiple sclerosis |
|
Dystonic gait |
uncontrollable additional movements interfering with the normal course of gait or dystonia |
basal ganglionic disease causing choreoathetosis or dystonia |
|
Hypokinetic gait (Figs. 3.2 and 6.33) |
slow gait, stiff, bent posture, small steps, lack of accessory arm movements; turning requires multiple small steps |
most commonly seen in Parkinson disease; similar picture in the lacunar state (cerebral microangiopathy, cf. p. 102) |
|
Small-stepped gait(“marche à petits pas”) |
small steps, unsteady, resembles hypokinetic gait but with more normal accessory movements |
“old person's gait” most commonly seen in the lacunar state, i.e., multiple small infarcts in the basal ganglia and along the corticospinal tracts, generally caused by atherosclerosis; distinguishable from parkinsonian gait mainly by the different accompanying signs |
|
Circumduction (Fig. 3.2) |
increased tone in the extensors of the paretic leg, which comes forward in a gentle outward arc, with a strongly plantar-flexed foot; hardly any accompanying movement of the flexed and adducted ipsilateral arm |
central (spastic) hemiparesis |
|
Steppage gait |
the advancing leg is raised high and then placed on the ground toe first, often with an audible slap |
unilateral: foot drop, e.g., in peroneal nerve palsy; bilateral: e.g., polyneuropathy or Steinert myotonic dystrophy |
|
Hyperextended knee(Fig. 3.2) |
with each step, the knee of the stationary leg is hyperextended |
prevents buckling of the knee when the knee extensors are weak—unilaterally, e. g., in quadriceps weakness due to a lesion of the femoral n.; bilaterally, e.g., in muscular dystrophy |
|
Hyperlordotic gait (Fig. 14.3) |
exaggerated lumbar lordosis |
e.g., in muscular dystrophy affecting the pelvic girdle, in boys with Duchenne muscular dystrophy |
|
Trendelenburg gait(Fig. 3.2) |
with each step, the pelvis tilts downward on the side of the swinging leg |
severe hip abductor weakness—unilaterally, e.g., in lesions of the superior gluteal n.; bilaterally, e.g., in muscular dystrophy affecting the pelvic girdle and in bilateral hip dislocation |
|
Duchenne gait (Figs. 3.2and 14.3b) |
with each step, the upper body tilts to the side of the stationary leg |
mild or moderate weakness of the hip abductors (as in Trendelenburg gait, but less severe), or as a pain-reducing maneuver in disorders of the hip joint |
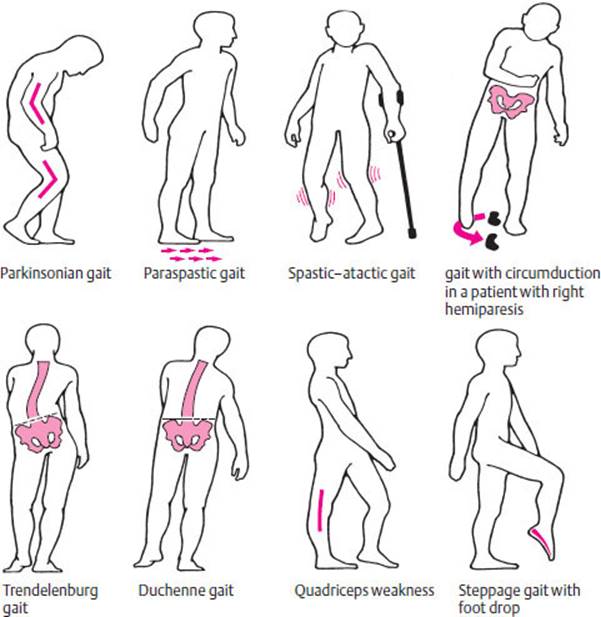
Fig. 3.2 Common gait disturbances
![]() Examination of the Head and Cranial Nerves
Examination of the Head and Cranial Nerves
Head and Cervical Spine
The examiner should first note the general appearance of the head and cervical spine (e.g., sunken temples in Steinert myotonic dystrophy) and the patient's facial expressions (e.g., paucity of facial expression in Parkinson disease). Young, healthy persons should be able to turn the neck and head almost 90° in either direction, so that the eye that is farther from the examiner disappears behind the root of the patient's nose. Further, the patient should be able to incline the head laterally 45° in either direction and to rotate it 60° to the right or left when the neck is maximally flexed (this rotation occurs only at the atlantoaxial and atlanto-occipital joints). Testing for meningismus is performed with the patient lying supine. This finding, if present, usually indicates meningeal irritation due to meningitis or subarachnoid hemorrhage, but is sometimes a reflexive response to space-occupying lesions of the posterior fossa. Meningismus consists of an isolated inhibition of neck flexion while the head can still be rotated. To test for meningismus, the examiner flexes the neck of the supine patient by bending the head forward. In genuine meningismus, the Lasegue sign (p. 211) is usually positive as well. If attempted passive flexion of the neck also induces flexion of the lower limbs at the knee or hip joint, this is called a positive cervical Brudzinski sign. This sign is often accompanied by a positive Kernig sign: when the patient is in the sitting position, the knee cannot be passively extended and, when the patient is supine, passive straight leg raising induces reflex knee flexion.
Auscultation of the skull may reveal a pulse-synchronous bruit over an arteriovenous fistula or an arteriovenous malformation. A carotid bruit may be due to stenosis.
The intrinsic reflexes of the facial musculature should always be examined. Tapping a finger placed over the lateral canthus of the patient's eye normally induces contraction of the ipsilateral orbicularis oculi m. This reflex normally weakens (habituates) on repeated tapping; if not, a bilateral lesion of the corticobulbar pathways is probably present. Excessively intense, bilateral contraction of the orbicularis oculi when the examiner taps on the patient's glabella (the glabellar or nasopalpebral reflex) also implies a bilateral corticobulbar lesion. Tapping on a tongue depressor placed on the patient's lips may induce lip protrusion (positive snout reflex). The masseter reflex (jaw jerk reflex) is elicited by gently tapping the patient's jaw from above when the patient's mouth is half open. Another way to elicit this reflex is to tap on a tongue depressor laid on the patient's mandibular teeth. The corneomandibular reflex (“winking jaw phenomenon”) consists of deviation of the slightly opened jaw when the cornea is touched. Its presence on only one side, or any marked asymmetry, implies an interruption of the ascending and descending brainstem pathways terminating in the pontomesencephalic reticular formation.
Cranial Nerves
Next, the cranial nerves are examined individually. Figure 3.3 and Table 3.3 provide an overview of the anatomy and function of the 12 cranial nerves. The clinical syndromes associated with lesions of individual cranial nerves are presented in Chapter 11 (pp. 180ff.). In this chapter, we will describe the main examining techniques and a selection of the important abnormal findings that can be elicited with each.
The first two cranial nerves (the olfactory and optic nn.) are, in reality, portions of the brain that have been displaced into the periphery. The remaining 10 cranial nerves structurally and functionally resemble the other peripheral nerves of the body. They have motor, somatosensory, special sensory, and autonomic functions.
CN I: Olfactory N.
Testing the sense of smell. Smell is tested individually in each nostril. The patient is asked to close his or her eyes and then to identify (or at least perceive) aromatic substances such as coffee, cinnamon, or vanilla that are held under the open nostril. Three-quarters of normal individuals can correctly identify coffee grounds. If there is doubt about the patient's ability to smell, asafetida (onion extract), a substance with an unpleasant stink, is used. Only a complete loss of the sense of smell (anosmia), not a mere diminution of it, is neurologically relevant. Anosmia most commonly follows severe traumatic brain injury (p. 180) but may also be due to frontal tumors, particularly olfactory groove meningioma, or postinfectious abnormalities of the nasal mucosa, e.g., after an upper respiratory “cold,” or in ozena.
If it is unclear whether anosmia is of neurological origin, the patient is given a dilute ammonia solution to smell. The unpleasant irritation that this produces is mediated, not by the olfactory n., but by the trigeminal n. If the patient fails to react, then he or she is probably suffering either from an acute process affecting the nasal mucosa (e. g., acute rhinitis) or from a psychogenic disturbance. The anosmia is not neurogenic in either case.
Fig. 3.3 Overview of the topographical relations of the cranial nerves and their sites of exit from the skull. ACP = anterior clinoid process, OA = ophthalmic a., PCommA = posterior communicating a., pit. = pituitary gland. III = oculomotor n., IV = trochlear n., V = trigeminal n., VI = abducens n., VII= facial n., VIII = vestibulocochlear n., IX = glossopharyngeal n., X = vagus n., XI = accessory n., XII = hypoglossal n. (Based on Mumenthaler, M.: Erkrankungen der Hirnnerven. In: Hornbostel H., Kaufmann W., Siegenthaler W.: Innere Medizin in Praxis und Klinik. Vol. II, 4th edn, Thieme, Stuttgart 1992)
Table 3.3 The 12 cranial nerves, their nuclei, and their functions
|
Cranial nerve |
Anatomical substrates (peripheral and central); innervated structures |
Function |
|
I Olfactory n. |
sensory neurons of the nasal mucosa (olfactory zone); olfactory fila, bulb, and tract; olfactory striae, amygdala |
perception of odors (only substances dissolved in the fluid of the nasal mucosa can be perceived) |
|
II Optic n. |
retina; optic nerve, chiasm, and tract; lateral geniculate body, optic radiation, primary visual cortex on the banks of the calcarine fissure |
visual perception |
|
III Oculomotor n. |
nucleus of the oculomotor n. and Edinger-Westphal nucleus (both are in the midbrain), nerve. Innervates the levator palpebrae m.; superior, inferior, and medial rectus mm.; and inferior oblique mm., as well as the constrictor pupillae m. |
raising the upper lid; most of the movements of the globe (eyeball); constriction of the pupil |
|
IV Trochlear n. |
nucleus of the trochlear n. (midbrain at its junction with the pons), nerve. Innervates the superior oblique m. |
depression of the adducted globe, internal rotation of the abducted globe |
|
V Trigeminal n. |
pontine and spinal nuclei of the trigeminal n. (sensory root), motor nucleus of the trigeminal n. (motor root), Gasserian ganglion, three peripheral nerve branches (the ophthalmic, maxillary, and mandibular nn.). Innervates the skin and mucosa of the head and face, and the muscles of mastication (temporalis, masseter, and medial and lateral pterygoid mm) |
sensation on the face, external ear, and mucosal surfaces of the head; innervation of the muscles of mastication |
|
VI Abducens n. |
nucleus of the abducens n. (pons), nerve. Innervates the lateral rectus m. |
abduction of the globe |
|
VII Facial n. |
nucleus of the facial n. (pons, motor fibers for the muscles of facial expression), superior salivatory nucleus (secretory fibers for the lacrimal, nasal, and palatal glands), nucleus of the tractus solitarius (gustatory fibers), nerve |
innervation of the muscles of facial expression and the stapedius m.; lacrimation and salivation; taste on the anterior two-thirds of the tongue |
|
VIII Vestibulocochlear n. (statoacoustic n., auditory n.) |
sensory neurons in the cochlea (cochlear root) and in the semicircular canals, utricle, and saccule (vestibular root), peripheral afferent nerve trunk, brainstem nuclei, and projecting fibers to higher regions of the CNS |
perception of sound and of bodily position, movement, and acceleration; regulation of balance |
|
IX Glossopharyngeal n. |
nucleus ambiguus (medulla, motor fibers for the muscles of the soft palate and pharynx), nucleus of the tractus solitarius (gustatory fibers from the posterior third of the tongue, somatosensory fibers from the palatal and pharyngeal mucosa); inferior salivatory nucleus, otic ganglion (secretory fibers for the parotid gland); nerve |
motor innervation of the palatal and pharyngeal muscles; somatosensory innervation of the palatal and pharyngeal mucosa; taste on the posterior third of the tongue; control of swallowing |
|
X Vagus n. |
nucleus ambiguus (medulla, motor fibers for the muscles of the soft palate and pharynx), dorsal nucleus of the vagus n., nucleus of the tractus solitarius (visceromotor and viscerosensory fibers for the thoracic and abdominal viscera), spinal nucleus of the trigeminal n. (sensory fibers from the pharynx, larynx, and external auditory canal); nerve trunk |
innervation of the laryngeal musculature, speech, sensation in the external ear canal and the posterior cranial fossa, autonomic fibers to the thoracic and abdominal viscera |
|
XI Accessory n. |
nucleus ambiguus (medulla, cranial root) and spinal nucleus of the accessory n. (C1–C5, spinal root), nerve trunk, sternocleidomastoid m. and upper portion of the trapezius m. |
turning the head to the opposite side, shrugging the shoulders |
|
XII Hypoglossal n. |
nucleus of the hypoglossal n. (medulla), nerve trunk, muscles of the tongue |
movement of the tongue |
CN II: Optic N.
Ophthalmoscopy. Inspection of the optic nerve papillae (optic discs) with the ophthalmoscope is an important technique for assessment of the optic n. Abnormal pallor indicates an optic nerve lesion (Fig. 3.4). In addition, inspection of the eye grounds can provide evidence of elevated intracranial pressure: in papilledema, the papillae are raised and hyperemic, and their margins are blurred. Enlarged retinal veins indicate impaired venous drainage due to intracranial hypertension (cf. Fig. 11.2, p. 183). A raised papilla with blurred margins can also be a sign of an inflammatory process affecting the optic n. (p. 182).
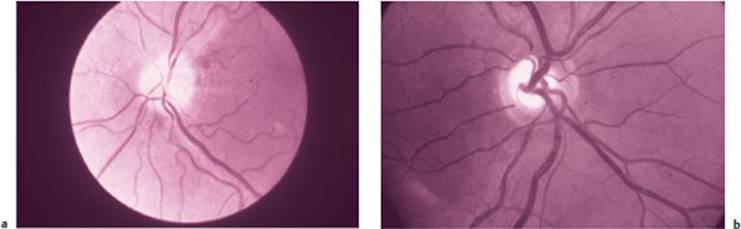
Fig. 3.4 Optic disc (papilla) of the right eye. a Pale, atrophic disc, b Normal disc (images kindly provided by the Department of Ophthalmology, University of Berne.) (For the color version of this figure, cf. Plate 1)
Testing of visual acuity for neurological purposes is usually performed with a wall chart seen from a distance. Refractive errors are corrected with eyeglasses if necessary.
Perimetry. Visual field testing is of particular importance in neurology. The visual fields can be roughly assessed in the neurologist's office or at the bedside with so-called finger perimetry (or digital confrontation, Fig. 3.5). The examiner sits directly in front of the patient and the patient fixes one eye on the examiner's nose. The examiner then moves a finger in each of the four quadrants of the visual field, testing each eye separately. The patient is asked whether he or she can see the finger. This method can reveal a major visual field defect, e. g., bitemporal hemianopsia or quadrantanopsia (p. 181). Various kinds of visual field defects, and the sites of the lesions that cause them, are depicted in Fig 3.6.
If visual neglect is suspected, the examiner should next perform double simultaneous stimulation of the visual field by moving the two index fingers at the same time in corresponding quadrants in the two halves of the field (left and right hemifields). The patient should report seeing both fingers. If both fingers are perceived on individual testing, but only one is seen on double simultaneous stimulation, this may be due to visual neglect. Monocular visual field defects are revealed by separate testing of the four quadrants of the visual field in each eye with a finger starting in the periphery and moving gradually toward the center.
Smaller (monocular or binocular) visual field defects can sometimes be detected by confrontational perimetry with a red object, but are usually revealed only by formal testing with equipment such as the Goldmann perimeter or octopus (p. 65).

Fig. 3.5 Testing the visual fields by digital confrontation. Above: double simultaneous testing for the detection of visual hemineglect. Below: individual testing of all four quadrants of the visual field of each eye.

Fig. 3.6 Visual field defects and the sites of the lesions that cause them. 1 Blindness in the left eye due to a left optic nerve lesion. 2 Bitemporal hemianopsia due to a lesion of the optic chiasm. 3 Right homonymous hemianopsia due to a lesion of the left optic tract. 4–6 Lesions at various sites in the left optic radiation: 4 Right upper quadrantanopsia due to a left temporal lobe lesion. 5 Right lower quadrantanopsia due to a left parietal lobe lesion. 6 Right homonymous hemianopsia, sparing macular vision, due to a left occipital lobe lesion.
CN III, IV, and VI: Oculomotor, Trochlear, and Abducens Nn.
Inspection. The examiner should first note the position of the eyes at rest, paying particular attention to the following: parallel position of the eyes, possible prominence of one eye, and symmetry of the palpebral fissures and of the pupils. The parallel position of the eyes is best assessed by observation of the small reflected images of light sources in the examining room in the patient's eyes, which should be at an analogous position on each cornea. A prominent globe (exophthalmos) can sometimes be appreciated by viewing the eyes tangentially from above (Fig. 3.7).
Testing of ocular motility. The anatomy of the six extraocular muscles and the three cranial nerves innervating them is shown in Fig. 3.8a, while the function of the extraocular muscles is described in Fig. 3.3and depicted in Fig. 3.8b. Eye movements are tested by having the patient keep the head stationary and follow the examiner's finger with his or her eyes. The motility of the globes is assessed along the vertical and horizontal axes. If abnormalities of eye movement can be seen directly by the examiner, or if the patient reports double vision (diplopia), then the manner in which eye movement is restricted (including any abnormality of the resting position of the eyes) and the type of double vision enable the examiner to determine which muscle (or muscles) is (are) paretic and, therefore, which cranial nerve is dysfunctional (paralytic strabismus). The eye muscles may, however, be weakened by intrinsic muscle lesions, rather than by cranial nerve palsies. A general principle for the interpretation of findings is that the positions of the eyes are farthest apart, and diplopia is therefore worst, when the patient looks in the direction of function of the paretic muscle (p. 189 ff.).

Fig. 3.7 A patient with a right carotid–cavernous fistula (i. e., a fistula between the right internal carotid a. and the cavernous sinus), a The tangential photograph reveals exophthalmos, b Conjunctival venous stasis is caused by elevated venous pressure.
A conjugate gaze palsy (p. 188) is the inability to perform a conjugate eye movement to direct the gaze in a particular direction, either horizontally or vertically. In such patients, the lesion is not in the peripheral portion of a cranial nerve; it is located centrally, within the brain (a supranuclear lesion, i. e., one that lies above the nuclei of the cranial nerves that innervate the extraocular muscles). In contrast to peripheral lesions, the eyes remain parallel and there is no double vision.
When testing eye movements, the examiner should also look for nystagmus (see below and p. 184). Deviations from the parallel axis are best detected by observing the reflected images on the patient's cornea.
A nonparallel (skewed) position of the two eyes without diplopia implies that the patient has concomitant strabismus, a result of longstanding impaired vision in one eye (usually from birth or early childhood). No cranial nerve palsy is present. Concomitant strabismus can be demonstrated with the aid of a cover test (Fig. 3.9). The patient keeps both eyes open while the examiner covers one eye and asks the patient to fix his or her gaze on a particular object in the room. The cover is then rapidly switched to the other eye, so that the previously covered eye must jump into position to keep the gaze fixated on the same object. The initially uncovered eye, now covered, deviates to one side, as can be shown by switching the cover back again (alternating concomitant strabismus; usually divergent, but sometimes convergent).
Assessment of the pupils. The examiner should note the shape (round or oblong) and size of the pupils. Normal pupils are generally of equal size and react equally to light. Inequality of the pupils is called anisocoria; a small degree of anisocoria is normal in some individuals. When the examiner illuminates the pupil of one eye, there should be reflex constriction of that pupil (the direct light response), accompanied by an equal reflex constriction of the other pupil (the consensual light response). To ensure that only one pupil is illuminated, the examiner shines a flashlight on one eye while blocking the light from the other eye with his or her own hand, held in the midline over the root of the patient's nose. Convergence is tested by having the patient fix his or her gaze on a distant point and then look at the examiner's finger, which is held close to the face. The normal reaction is adduction of both eyes (convergence) accompanied by simultaneous reflex constriction of the pupils (the near response). Pathological abnormalities of the pupillary reflexes and their significance with regard to localization are presented in Figure 11.12 on p. 194.
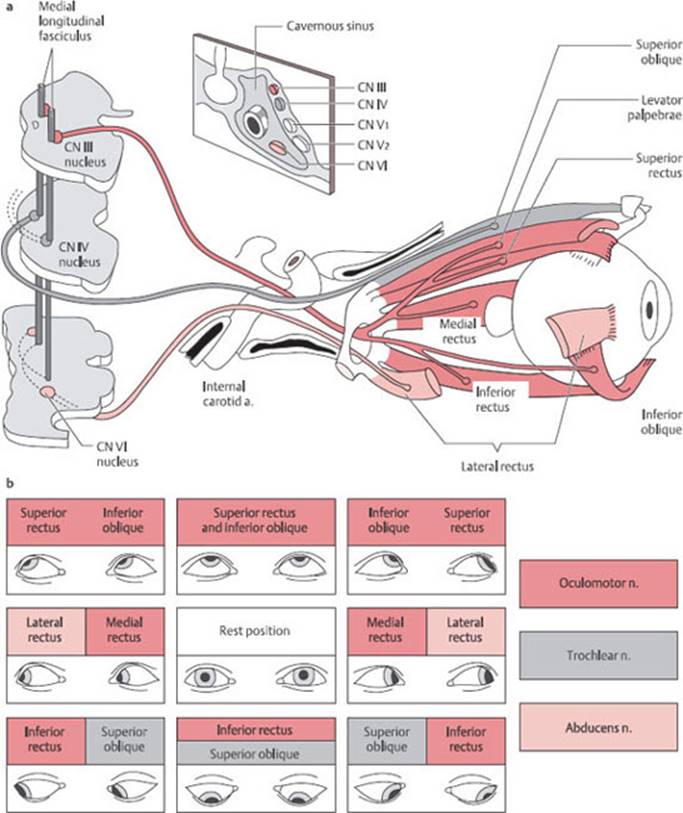
Fig. 3.8a The three nerves to the extraocular muscles and the muscles innervated by each, b Scheme according to Hering, indicating the direction of gaze in which the main function of each eye muscle is most strongly in evidence.
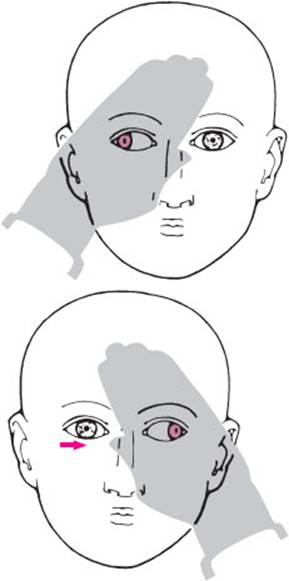
Fig. 3.9 Cover test. In concomitant, alternating, divergent strabismus, the covered eye (i. e., the one that is not fixating) deviates outward. When the cover is rapidly switched to the other eye, the newly uncovered eye moves to the fixating position, while the covered other eye now deviates outward with a positioning saccade (→).
CN V: Trigeminal N.
Testing sensation in the face. The somatosensory portion of this mixed cranial nerve originates in the ganglion cells of the Gasserian ganglion. The cutaneous and mucosal zones innervated by the trigeminal n. are shown in Fig 3.10. Sensation should be tested with a cotton swab or a piece of tissue paper. The latter can also be used to test the corneal reflex: the patient is asked to look upward and the tactile stimulus is delivered to the lower edge of the cornea to avoid engendering a visually induced fright reaction. The reflex response consists of immediate closure of the eyes.
Assessment of the muscles of mastication. The motor portion of the trigeminal n. runs in its third branch (the mandibular n.) to supply the muscles of mastication, i. e., the masseter and temporalis mm. and the medial and lateral pterygoid mm. The examiner tests the function of these muscles by placing his or her fingers in front of the angle of the jaw bilaterally and asking the patient to clamp the jaw tightly (press the teeth together). In unilateral (motor) trigeminal n. paresis, the contraction of the masseter m. on the affected side is palpably weaker and the masseter reflex may be weaker as well. When the patient opens the jaw, the mandible deviates to the side of the lesion because of the dominant effect of the pterygoid muscles on the healthy side.
CN VII: Facial N.
Assessment of the muscles of facial expression. The anatomy of the seventh cranial nerve is shown in Fig. 11.15 p. 196. In assessing its function, the examiner should note any asymmetry of the face, spontaneous facial expression(mimesis), and contractions of the facial muscles during movement: the patient should be systematically asked to furrow the brow, close the eyes tightly, show his or her teeth, and whistle. In lesions of the facial n., the corneal reflex is weak, because the efferent arm of the reflex arc is interrupted (rather than the afferent arm, as in trigeminal lesions). The clinical findings in facial nerve palsy, and the differentiation of peripheral and central facial weakness, are presented on p. 198 and in Figs. 11.16 and 11.18 on pp. 197 and 198.
Assessment of taste, lacrimation, and salivation. The facial n. also contains gustatory fibers supplying taste to the anterior two-thirds of the tongue. When a facial nerve lesion is suspected, taste in this region can be tested by the application of substances with the four basic modalities of taste—sweet, salty, sour, and bitter—to the corresponding half of the tongue. Appropriate solutions to use are, for example, 20% glucose, 10% sodium chloride, 5% citric acid, and 1% quinine. (Note: “bitter” is perceived in the mucosa of the posterior third of the tongue; this sensation is thus mediated by the glossopharyngeal n., not the facial n.). Peripheral lesions of the facial n. also cause diminished lacrimation and salivation, which are usually not noticed by the patient and require special tests to demonstrate. There may also be hypersensitivity to sound (hyperacusis).
CN VIII: Vestibulocochlear N.
Assessment of hearing. The anatomy of the vestibulocochlear nerve is depicted in Fig 3.11. The neurologist's assessment of the patient's hearing is generally limited to the determination whether (uni- or bilateral) hearing loss is present and, if so, whether it is due to impaired conduction of sound (middle ear process, obstruction of the external auditory canal) or to a sensorineural deficit (process affecting the inner ear or the cochlear portion of the eighth cranial nerve). The examiner tests hearing separately in each ear by speaking or whispering words from distances of 5 to 6 m. The patient must inactivate hearing in the ear not being tested by forcefully rubbing a finger back and forth in the external auditory canal. Total deafness, i.e., deafness even for very loud sounds, is never due to a middle ear process alone.
Differentiation of conductive and sensorineural hearing loss. These two types of hearing loss can be distinguished with the aid of the Rinne and Weber tests (Fig. 3.12).
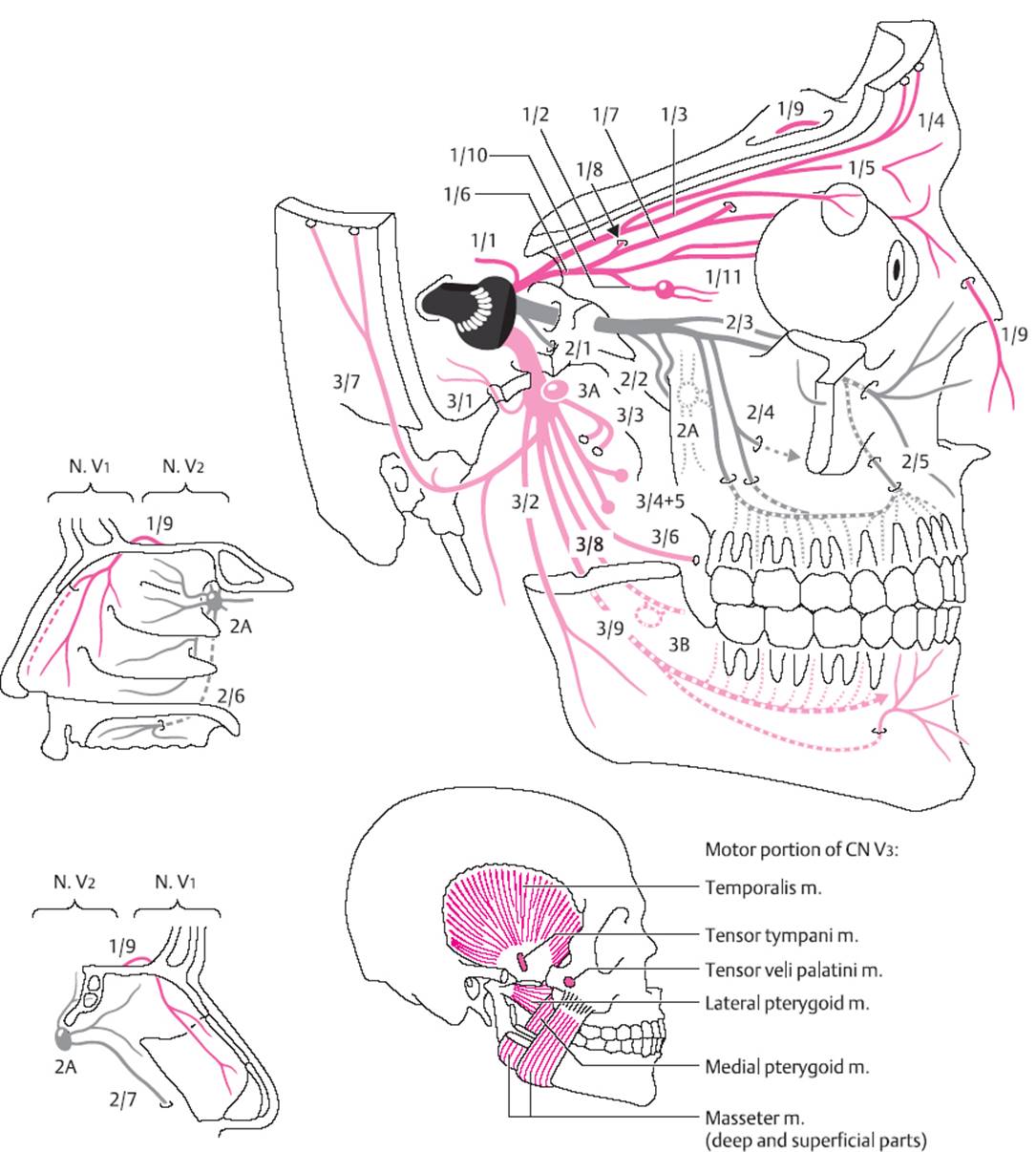
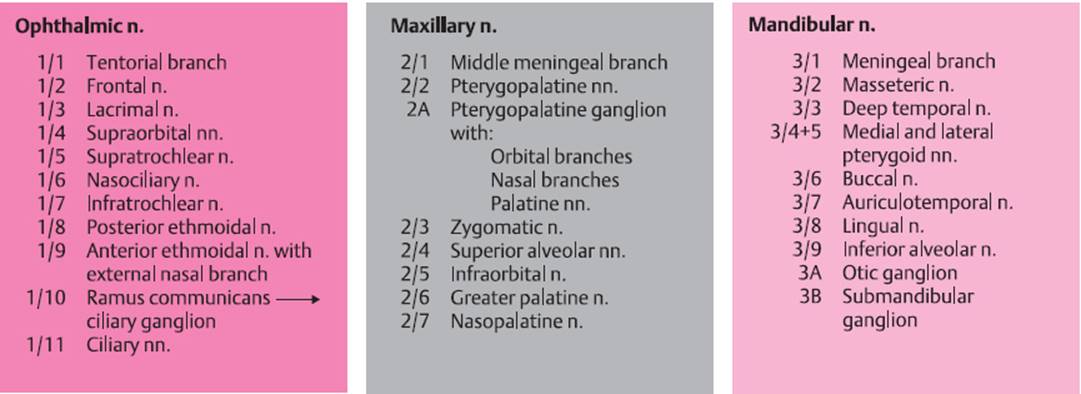
Fig. 3.10 Anatomy of the somatosensory and motor portions of the trigeminal n.

Fig. 3.11 Anatomy of the internal ear and vestibulocochlear n. (schematic drawing).
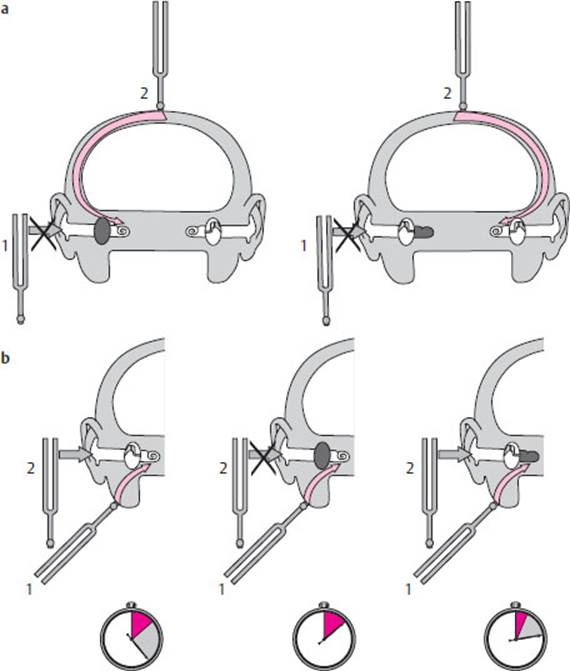
Fig. 3.12 Weber and Rinne hearing tests, a Weber test: in a patient with right-sided conductive hearing loss (picture at left), the tuning fork cannot be heard when held next to the ear (1). If the tuning fork is placed on the forehead (2), however, it is heard, and the tone is localized to the side of the hearing loss, i. e., to the right ear. In contrast, in a patient with right-sided sensorineural hearing loss (picture at right), the tone is localized to the normally hearing (left) ear. b Rinne test: the tuning fork is first placed on the mastoid process (1). As soon as the tone is no longer heard, the tuning fork is held next to the ear. If hearing is normal, the tone will now be heard again (2). In right-sided conductive hearing loss (middle picture), the tone will not be heard again when the tuning fork is held next to the ear (negative Rinne test). In rightsided sensorineural hearing loss, however, the tone will be heard, though for a shorter time than normal, both by bone conduction and with the tuning fork held next to the ear (positive, i. e., normal Rinne test).
Rinne test. Air conduction of sound is better than bone conduction in normal individuals, as can be demonstrated by the following procedure: first, a vibrating tuning fork is placed on the mastoid process. As soon as the subject can no longer hear the tone, the tuning fork is removed from the mastoid process and placed next to the ear. The tone should then be heard again, and should take approximately twice as long to disappear as it did on the mastoid process. This is called a “positive,” i. e., normal, Rinne test. If the time during which the tone is heard by air conduction is shorter than normal, or if the tone is not heard in this way at all, then the Rinne test is negative, indicating conductive hearing loss (that is, a middle ear process or obstruction of the external auditory canal). In patients with sensorineural hearing loss, the Rinne test is positive (normal).
Weber test. The vibrating tuning fork is placed on the middle of the forehead or on the vertex. Normally, the tone is heard equally loudly in both ears and is localized to the midline. The tone is lateralized to the worse ear in conductive hearing loss and to the better ear in sensorineural hearing loss (due to a process affecting the cochlea or the cochlear part of the eighth cranial nerve). When unilateral hearing loss has been present for many years, the Weber test no longer lateralizes.
Assessment of vestibular function. The most common symptom of a lesion affecting the labyrinth or the vestibular portion of the vestibulocochlear nerve is vertigo. Patients usually describe a directional or systematic type of vertigo, e. g., rotational vertigo (“like on a merry-go-round”), a feeling of turning to the side, or an “elevator” feeling. They can often state the direction of the vertigo. In contrast, dizziness of nonvestibular origin—for example, due to a brainstem lesion—is often not as well defined. Such patients may complain of giddiness, swaying, or seeing black before their eyes (see p. 201).
The objective sign of a lesion of the vestibular portion of the vestibulocochlear nerve is nystagmus. This is a rapid, rhythmic jerking movement of both eyes in the same direction (also called “jerk nystagmus”). A slow conjugate deviation in one direction is followed by a rapid conjugate movement that returns the eyes to the original position and then the cycle starts again. The slow deviation is the truly pathological component of nystagmus; the rapid component is a reflex correction to preserve fixation. By convention, the direction of nystagmus is given as the direction of the rapid phase. Nystagmus may be horizontal (toward the right or the left), vertical (upbeat or downbeat), or rotatory (clockwise or counterclockwise). Nystagmus of vestibular origin can sometimes be seen even when the patient looks straight ahead (nystagmus that beats spontaneously in this way is called spontaneous nystagmus); in other cases, it appears only when the examiner has the patient look to the side. In either case, nystagmus of vestibular origin always beats in the same direction (away from the side of the lesion), regardless of whether it appears when the patient looks straight ahead, to the right, and/or to the left.
Spontaneous nystagmus of vestibular origin must be distinguished from physiological end-gaze nystagmus and from gaze-evoked nystagmus. End-gaze nystagmus arises when the patient looks all the way to one side or the other (into the monocular visual field); its rapid phase beats in the direction of gaze, it is seen in both eyes to the same extent, and it disappears spontaneously after a number of beats. It is found symmetrically in normal individuals. If end-gaze nystagmus is seen on examination, the examiner should bring the test object about 10° back into the binocular visual field. The nystagmus is clinically significant only if it is still present after this maneuver (gaze-evoked nystagmus, p. 185). Some common pathological types of nystagmus are listed and described in Table 11.1, p. 185.
Instruments for assessing vestibular function. Frenzel goggles make nystagmus easier to observe. They contain strong magnifying lenses that render the patient unable to fixate, as well as a lamp to illuminate the globes. Nystagmus can often be suppressed by fixation and, if so, is only visible when the patient wears Frenzel goggles (head shaking is a further provocative maneuver). The magnification provided by the Frenzel lenses also makes it easier for the examiner to see fine movements.
Vestibular lesions can be assessed objectively by testing of the rotational and caloric excitability of the corresponding labyrinth. In the normal case, irrigation of the external auditory canal with warm water induces nystagmus with the rapid phase toward the irrigated ear (with cold-water irrigation, the rapid phase is toward the opposite ear). If a vestibular lesion is present, the induced nystagmus is diminished or absent.
Tests of balance and coordination. Certain abnormalities in the tests of stance and gait described above (Un-terberger step test, Babinski–Weil test, heel-to-toe walking, p. 13) indicate dysfunction of the vestibular apparatus. In a further test, the Bárány pointing test, the patient is asked to stretch out his or her arm forwards and then bring it down to a target provided by the examiner, e. g., the examiner's index finger. The patient is then asked to repeat the movement with eyes closed, still trying to hit the target as accurately as possible. In unilateral vestibular lesions, the arm deviates to the side of the lesion during its downward course. The same can also be observed, however, with lesions of the ipsilateral cerebellar hemisphere.
CN IX and X: Glossopharyngeal and Vagus Nn.
The efferent fibers from the nucleus ambiguus to the muscles of the palate, larynx, and pharynx reach these structures through the glossopharyngeal and vagus nn. The larynx is innervated by two vagal branches, the superior laryngeal n, and the recurrent laryngeal n. The glossopharyngeal n. carries somatosensory fibers from the soft palate, the posterior pharyngeal wall, the tonsillar fossa, and the middle ear, as well as gustatory fibers from the posterior third of the tongue. The vagus n. carries somatosensory fibers from the external auditory canal, part of the external ear, and the meninges of the posterior fossa. It also carries efferent parasympathetic fibers to the thoracic and abdominal viscera (cf. Table 3.3).
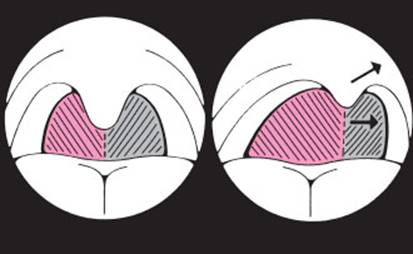
Fig. 3.13 Palatal deviation. In right glossopharyngeal nerve palsy, the palate and posterior pharyngeal wall deviate to the normal left side when the patient gags.
Examination of the pharynx and larynx. The motor function of the ninth and tenth cranial nerves is assessed by inspection of the palate and throat and, more importantly, by observation of the movements of these structures during phonation (“a–aa–ah ...”) and after induction of the gag reflex by touching the posterior pharyngeal wall with, e. g., a cotton swab. Unilateral weakness of the palatal veil and the pharyngeal muscles makes these structures deviate laterally away from the side of the lesion, as shown in Fig 3.13. Hoarseness due to a unilateral recurrent laryngeal nerve palsy can sometimes be heard only when the patient sings.
CN XI: Accessory N.
Examination of the sternocleidomastoid and trapezius mm. The external (final) branch of the purely motor accessory n. supplies the sternocleidomastoid m. and the upper portion of the trapezius m. To test the sternocleidomastoid m. on one side, the examiner asks the patient to turn the head to the opposite side against resistance, then observes and palpates the muscular contraction at the anterior edge of the lateral triangle of the neck (Fig. 3.14).
The upper portion of the trapezius m. is examined as follows: the examiner stands in front of the patient, puts both hands on the patient's shoulders, grasps the upper edge of the trapezius m. on either side between the thumb and index finger, and asks the patient to shrug the shoulders against resistance. In unilateral accessory nerve palsy, the shrug is less powerful on the affected side and the trapezius m. is palpably thinner and weaker (Fig. 3.15).

Fig. 3.14 Testing the sternocleidomastoid m. The patient attempts to turn the head to the left against the examiner's resistance. The right sternocleidomastoid m. contracts.
CN XII: Hypoglossal N.
The twelfth cranial nerve is a purely motor nerve to the muscles of the tongue. Lesions of this nerve produce atrophy and weakness of the tongue. A unilateral lesion usually produces a longitudinal furrow; when protruded, the tongue deviates to the weaker side because of the predominant force of the intact contralateral genioglossus m., which “pushes” the tongue across the midline (Fig. 3.16).
Phonation, Articulation, and Speech
Assessment of the patient's voice and speech is a compulsory part of the neurological examination. The examiner should pay attention to possible hoarseness, to the volume of speech (e. g., hypophonia in Parkinson disease, p. 128), and to possible disturbances of articulation (dysarthria), of the tempo of speech, and of its linguistic form and content (aphasia, p. 41).
![]() Examination of the Upper Limbs
Examination of the Upper Limbs
General aspects. The examiner should ask the patient which hand he or she mostly uses, right or left. Only persons who use a pair of scissors, a knife, or a sewing needle with their left hand, or write with the left hand, are true left handers. Any abnormalities of muscle bulk should be noted, in particular isolated atrophy of muscle groups. Fasciculations must be deliberately sought: in our experience, these involuntary contractions of groups of muscle fibers, which induce no movement, can be seen under the skin only by careful observation of the unclothed patient from an adequate distance and for a sufficient length of time. The trophic state of the skin, the papillary pattern of the fingertips, and the configuration of the nails should also be assessed. Important positive findings include anomalies of finger posture, tremor, or other involuntary movements. The mobility of the larger joints should be tested individually and the pulses in the limbs should be felt. Vascular bruits should be listened for in the supraclavicular fossa when indicated.
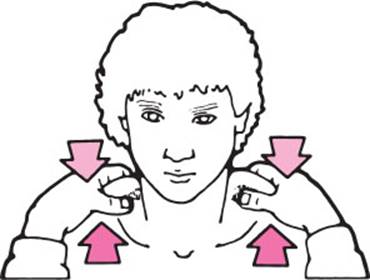
Fig. 3.15 Testing the upper portion of the trapezius m. The examiner places his or her hands on the patient's shoulders, grasping the upper edge of the trapezius m. on each side between his or her thumb and index finger. The patient is then asked to shrug the shoulders. Unilateral weakness, reduced contraction, or diminished volume of the trapezius m. can be palpated.

Fig. 3.16 Atrophy and weakness of the right half of the tongue in a lesion of the right hypoglossal n.
Motor Function and Coordination
A number of standard tests are used to assess motor function and coordination. Diadochokinesis is the ability to carry out rapid alternating movements, e. g., pronation and supination of the forearm (Fig. 3.17). Such movements will be abnormally slow (bradydiadochokinesia) or irregular (dysdiadochokinesia) on one side or both in the presence of paresis, extrapyramidal processes, and cerebellar diseases. In the postural test, the patient extends both arms horizontally in front, in supination, with eyes closed (Fig. 3.18). An involuntary sinking, or pronation of one arm (“pronator drift”), or involuntary flexion at the elbow or wrist, indicates motor hemiparesis of central origin; conjugate deviation of both arms to one side implies an ipsilateral lesion of the labyrinth or cerebellum. In the arm-rolling test, the patient rapidly rotates the forearms around each other in front of the trunk (Fig. 3.19). Mild hemiparesis is evident as markedly diminished movement of the affected limb. In the finger–nose test, the patient keeps his or her eyes closed and brings the index finger slowly to the tip of the nose, in a wide arc. This can normally be done smoothly and confidently (Fig. 3.20a). Fluctuating deviation of the finger from the ideal arc is a manifestation of ataxia, indicating either a proprioceptive disturbance or a lesion in the ipsilateral cerebellar hemisphere. On the other hand, if the deviation first appears when the finger is near its target and worsens as it approaches, this is called intention tremor (Fig. 3.20c) and is caused by lesions of the dentate nucleus of the cerebellum or of its efferent projections. A positive rebound phenomenon consists of inadequate braking of the normal, small rebound movement that occurs when the patient isometrically contracts a muscle against the examiner's resistance and the resistance is suddenly removed (Fig. 3.21). If the patient is sitting, the examiner can test for rebound of the biceps brachii m. (while taking care lest the patient hit himself or herself in the face). If the patient is lying on the examining table, the patient can be asked to stretch out one arm and raise it a short distance into the air, then press strongly downward against the examiner's resistance. If the examiner suddenly lets go, a healthy subject will brake the ensuing downward movement of the arm in time, but a patient with hemiparesis or cerebellar disfunction will hit the table with it.
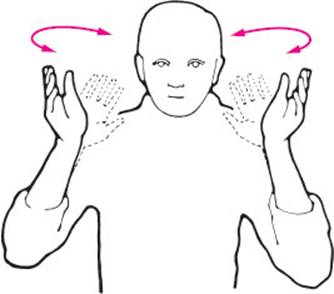
Fig. 3.17 Testing of diadochokinesis by rapid pronation and supination of the forearms.

Fig. 3.18 Positional testing of the upper limbs.

Fig. 3.19 Arm-rolling test. A normal subject rotates both arms to a roughly equal extent, while a patient with central hemiparesis (even if mild!) moves the nonparetic limb much more than the paretic one.

Fig. 3.20 Finger–nose test, a Normal, smooth, confident movement. b Ataxic movement c Intention tremor: the closer the finger comes to its target (nose), the more it deviates from the ideal line of approach.
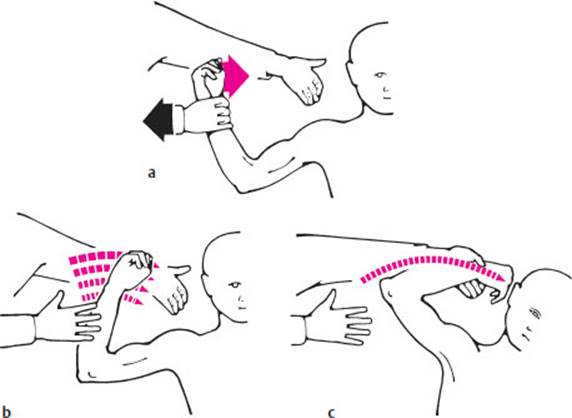
Fig. 3.21 Rebound phenomenon due to a cerebellar lesion, a Method of testing: the examiner's other hand protects the patient's face, b When the examiner suddenly releases the patient's actively flexed arm, the ensuing involuntary flexion should be promptly braked, c Braking is inadequate (the rebound phenomenon is positive) in the presence of an ipsilateral cerebellar lesion
Muscle Tone and Strength
Muscle tone in the upper limbs can be tested with wide-amplitude passive movement of the radiocarpal joint or of the elbow. The movement should be rapid, but not rhythmic (so that the patient cannot predict its course). Diminished muscle tone (hypotonia) is a characteristic sign of intrinsic muscle lesions, peripheral nerve lesions, ipsilateral cerebellar dysfunction, and hyperkinetic extrapyramidal diseases. Spasticity is a type of elevated muscle tone produced by lesions of the pyramidal pathway (Fig. 3.22a). The resistance of a spastic upper limb to passive movement is usually strong at first, but may then suddenly give way (“clasp-knife phenomenon”); alternatively, it may increase on continued passive movement. Rigidity is a viscous or waxy resistance to passive movement that can be felt to an equal extent throughout the entire movement; it is most commonly found in Parkinson disease (Fig. 3.22b). The accompanying parkinsonian cogwheel phenomenon is best appreciated at the radiocarpal joint. The examiner should fix the patient's forearm with one hand, grasp the patient's fingertips with the other, and alternately flex and extend the radiocarpal joint, slowly and with a wide excursion, but not in perfect rhythm (Fig. 3.23). The examiner will then feel multiple, brief impulses of resistance at irregular intervals, giving the overall impression of a saccadic movement (Fig. 3.22c). Elevated muscle tone may also result from active opposition to passive movement when the patient apparently cannot relax the muscular contraction. This phenomenon, known by the German term Gegenhalten (“opposition”), is seen in frontal lobe lesions.
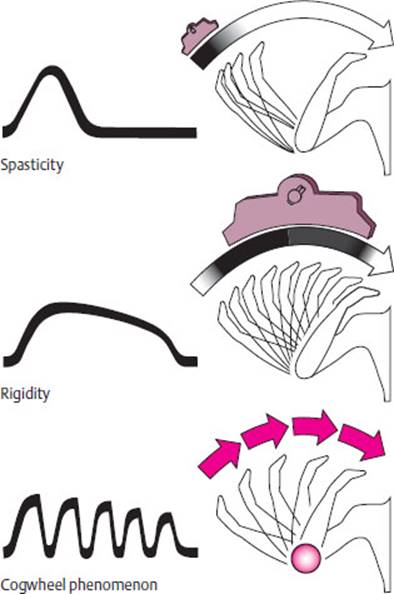
Fig. 3.22 Abnormalities of muscle tone and the cogwheel phenomenon.
Muscle strength is tested in groups of muscles that carry out a single movement, or, if necessary, in individual muscles. The patient is asked to contract the corresponding muscle(s) actively against the examiner's resistance.The examiner then judges the strength of contraction at the end-point of the related movement. Thus, the examiner tests biceps strength by trying to extend the patient's flexed elbow against resistance and triceps strength by trying to flex the extended elbow against resistance. The evaluation of potential lesions of individual nerve roots or peripheral nerves requires specific testing of the particular muscles or muscle groups innervated by these nerves (see p. 208). For the purpose of documentation, muscle strength can be graded semiquantitatively with the MRC scale shown in Table 3.4.Incomplete paralysis is called paresis and complete paralysis is called plegia. Further terms describe the distribution of weakness in the body: hemiparesis or hemiplegia affects one side of the body, paraparesis or paraplegia affects both lower limbs, and quadriparesis or quadriplegia affects all four limbs (less common synonyms for the last two are tetraparesis and tetraplegia). Paralysis of both arms, or brachial diplegia, is a rare occurrence.
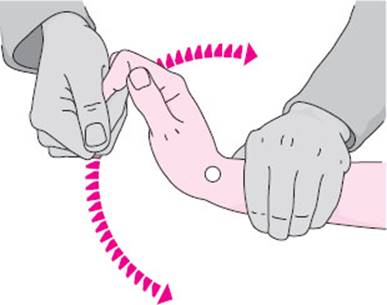
Fig. 3.23 Testing for the cogwheel phenomenon in the radiocarpal joint. The examiner fixes the patient's forearm with one hand, grasps the patient's fingers with the other, and moves them slowly (but not rhythmically) back and forth.
Table 3.4 Grading of muscle strength.
The 0–5 scale of the British Medical Research Council (MRC).
|
M0 |
= |
no muscle contraction |
|
M1 |
= |
visible contraction not resulting in movement |
|
M2 |
= |
movement of the body part only when the effect of gravity is eliminated |
|
M3 |
= |
movement against gravity |
|
M4 |
= |
movement against moderate resistance |
|
M5 |
= |
full strength |
(Grades M3 and M4 can be optionally subdivided by adding plus or minus signs)
Reflexes
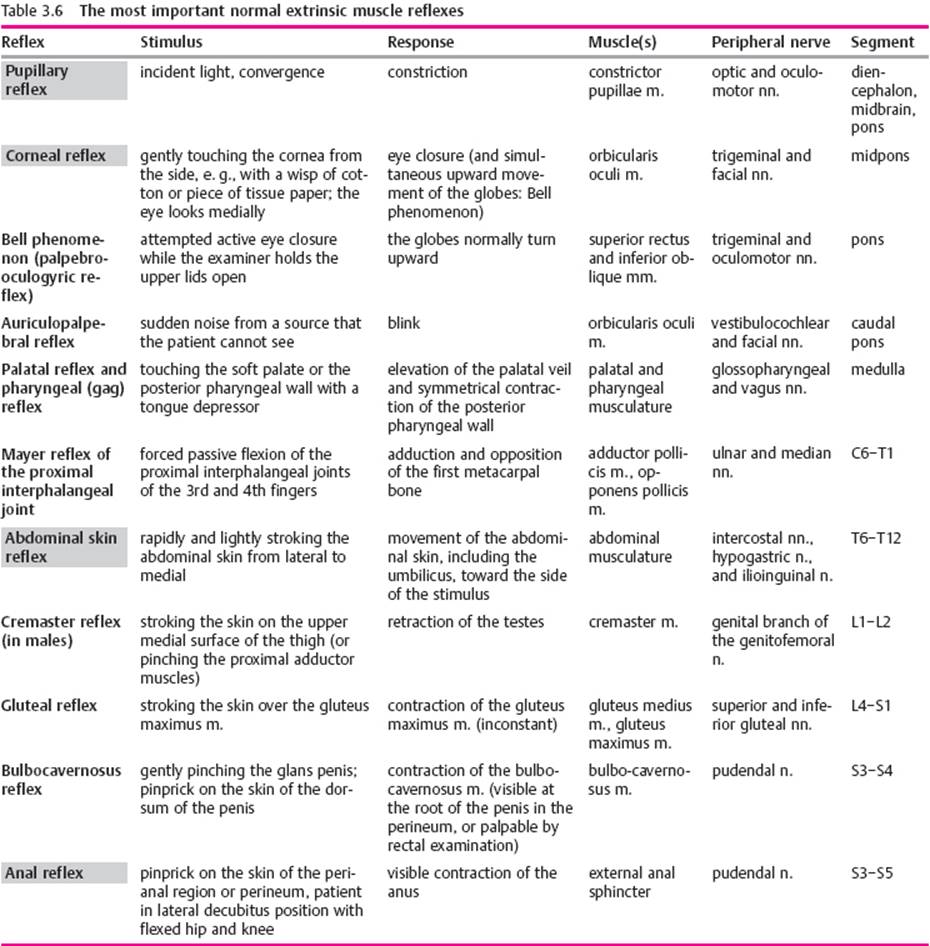
Types of reflexes. Reflexes are processes that are induced by a specific stimulus, always take the same course, and cannot be voluntarily influenced by either the patient or the examiner. For the intrinsicmuscle reflexes, alternatively called proprioceptive muscle reflexes, the site (muscle) of the eliciting stimulus is the same as that of the reflex contraction; for extrinsic (exteroceptive) reflexes, the stimulus and the response are at different sites and the afferent and efferent arms of the reflex loop, therefore, belong to different peripheral nerves or segmental nerve roots. Extrinsic reflexes become less intense (habituate) on repeated stimulation.
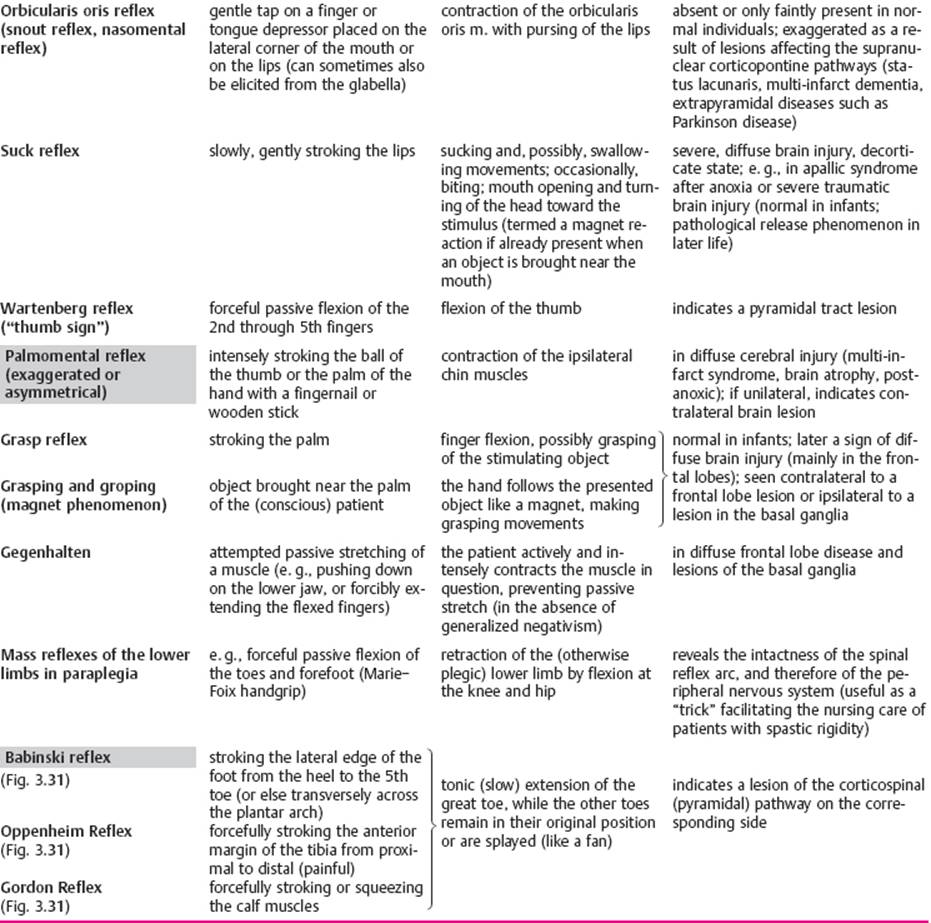
Pathological reflexes are usually not seen in normal individuals, or only up to a certain age; they are found in various disease processes affecting the CNS. Some pathological reflexes are of the extrinsic type. The more important reflexes, and the segmental nerve roots and peripheral nerves that mediate them, are listed in Tables 3.5–3.7.
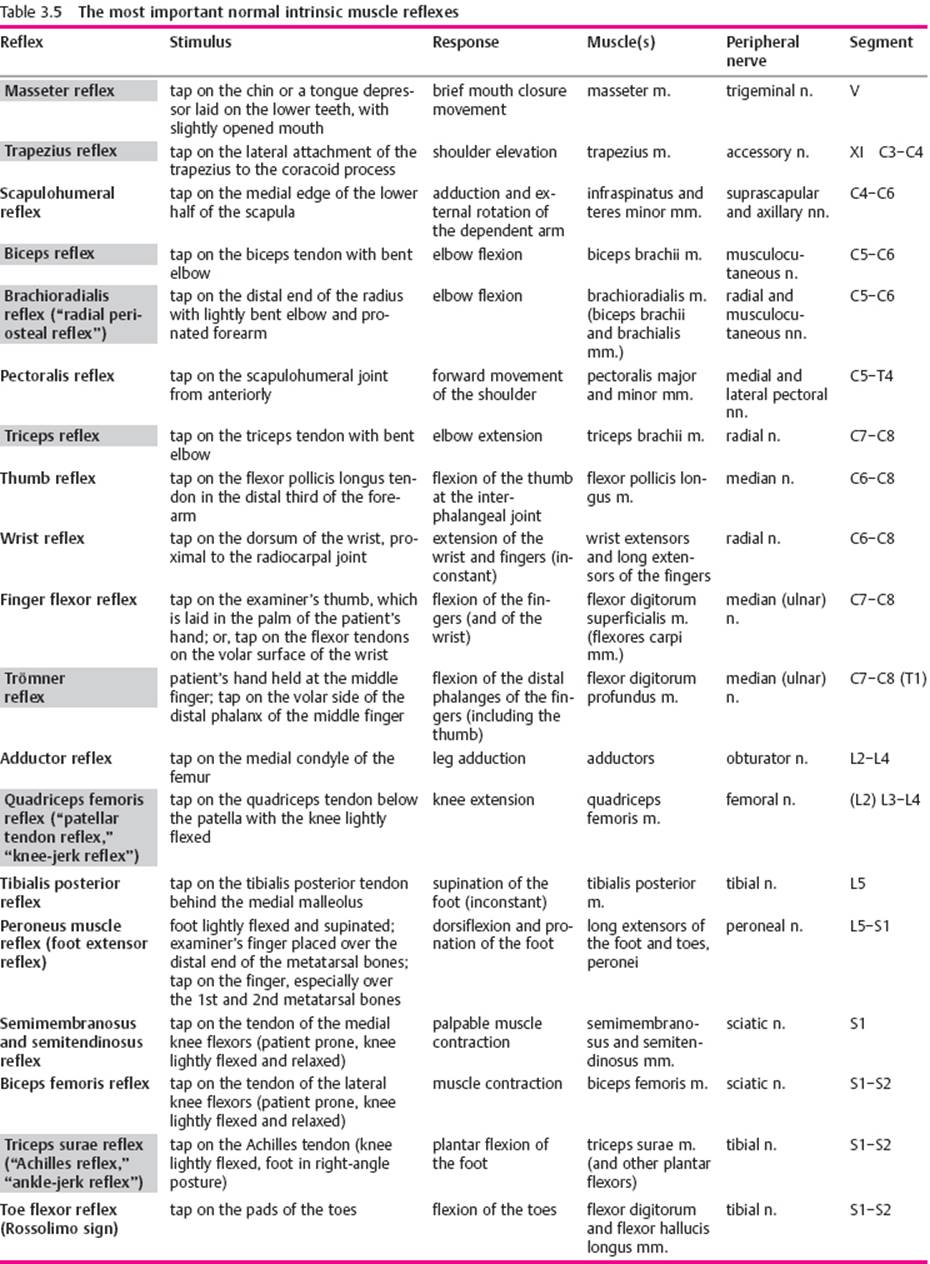

Intrinsic muscle reflexes of the upper limb. The intrinsic muscle reflexes are elicited by a rapid, and adequately forceful, blow on the tendon of a muscle or on the bone to which the tendon is attached. The resulting, transient stretching of the muscle excites receptors in the muscle spindles, in which afferent impulses are generated. These travel to the spinal cord and excite the α-motor neurons innervating the stimulated muscle (usually by way of interneurons at the same segmental level). The upper limb reflexes that are usually tested are the triceps, biceps, and radial periosteal reflexes (Table 3.5). The last-named reflex is elicited by a tap on the styloid process of the radius; this is followed by contraction, not only of the brachioradialis m., but also of the biceps and brachialis mm. The elicitation of these reflexes is illustrated in Fig 3.24.
The two important finger fIexor reflexes are essentially variations of the same reflex. The Trömner reflex is elicited by a rapid tap on the pads of the patient's lightly flexed fingers. The response consists of flexion of the distal interphalangeal joints of the fingers and thumb (only in the hand that was stimulated, not in the other hand). To elicit Hoffmann sign, the examiner gently grasps the distal phalanx of one of the patient's fingers (usually the middle finger) between his or her own thumb and index finger, then lets it snap back as the thumb slides off the patient's fingernail. The response is the same as in the Tromner reflex (Fig. 3.25).

Fig. 3.24 Elicitation of the intrinsic muscle reflexes of the upper limb.

Fig. 3.25 Elicitation of the Trömner reflex.
The more common abnormalities of the intrinsic muscle reflexes and their significance are presented in Table 3.8.
Facilitating maneuvers. Initially faint or not clearly elicitable intrinsic muscle reflexes can be enhanced with various maneuvers based on the principle that preloading of the intrafusal muscle spindle fibers makes them more sensitive to stretch. Forceful contraction of practically any muscle group in the body results in a generalized sensitization of all muscle spindle fibers. Thus, all of the intrinsic muscle reflexes can be made stronger by having the patient forcefully lift his or her head from the headrest (in the supine position), clench the teeth, make fists, strongly plantar-flex the feet, or interlock the hands and pull hard (this is called the Jendrassik handgrip). These maneuvers are illustrated in Fig 3.26.
Pyramidal tract signs in the upper limb. Lesions along the pyramidal pathway produce characteristic changes in the pattern of the reflexes that are normally present, as well as other, pathological reflexes that are normally absent. Evidence for a lesion of the pyramidal pathway is generally less obvious in the upper limb than in the lower limb, because there are no “classic pyramidal tract signs” for the upper limb, as there are for the lower (cf. p. 38). One important clue is exaggeration of the physiological intrinsic muscle reflexes, especially if asymmetric. Two others are spreading of the reflex zones and unusual briskness of certain intrinsic reflexes that, under normal circumstances, are only barely elicitable, or not at all, e.g., the trapezius and pectoralis reflexes (cf. Table 3.5). The Tromner reflex and Hoffmann sign can also be of pathological significance if abnormally brisk or unilaterally exaggerated. Absence of the Mayer reflex of the metacarpophalangeal joint is also considered a pyramidal tract sign: forceful passive flexion of the middle finger at the metacarpophalangeal joint is normally followed by reflex adduction of the metacarpal bone of the thumb (Fig. 3.27), but not if there is a lesion in the pyramidal pathway. Another pyramidal tract sign is flexion and opposition of the thumb when the examiner forcefully pulls on an actively flexed finger.
Table 3.8 Significance of the more common abnormalities of the intrinsic muscle reflexes
|
Abnormality |
Significance |
Remarks |
|
Apparent absence of all reflexes |
very weak reflexes, or inadequate examining technique |
facilitation maneuvers, e.g., Jendrassik handgrip |
|
True generalized areflexia |
polyneuropathy, polyradiculopathy anterior horn cell disease myopathy Adie syndrome congenital areflexia |
sensory deficit, perhaps paresis muscle atrophy without sensory deficit (same) inspect pupils often familial |
|
Absence of an individual reflex or reflexes |
nerve root lesion peripheral nerve lesion |
e. g., triceps reflex (C7), Achilles reflex (S1) |
|
Very weak reflexes |
usually without pathological significance |
often seen in older patients |
|
Very brisk reflexes |
if generalized, often without pathological significance |
particularly in younger patients |
|
Pathologically exaggerated reflexes |
“pyramidal tract signs,” spasticity |
compare sides (hemiparesis?) and compare upper with lower limbs (paraparesis?) |
|
Positive Hoffmann sign and Trömner reflex |
normal if symmetrical and without other, accompanying “pyramidal tract signs” |

Fig. 3.26 Facilitation maneuvers make the intrinsic muscle reflexes more intense and easier to elicit, a Jendrassik hand grip. b Same effect with active, strong raising of the head off the headrest. c Active plantar flexion of the foot.
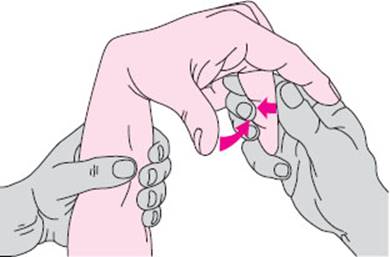
Fig. 3.27 The Mayer reflex of the metacarpophalangeal joint is elicited by forceful passive flexion of the middle finger. Involuntary adduction of the thumb normally follows; absence of the reflex suggests a lesion of the pyramidal pathway.
Sensation
Sensory testing takes time, patience, and good cooperation from the patient. Its general purpose is to identify any sensory deficit that may be present, delimit its site and extent precisely, and determine which sensory modalities are affected. The pattern of findings obtained in this way usually permits classification of the causative lesion as central, radicular, or peripheral. During the examination, the clinician must keep in mind what he or she is looking for with each examining technique in each part of the body where it is being applied.
The sense of touch (esthesia) is tested with the patient's eyes closed. The examiner lightly touches various sites on the patient's body with a finger, a feather, a piece of tissue paper, or the like. Precise quantitative testing can be performed with graded instruments, such as von Frey hairs or an adjustable Wartenberg pinwheel, but is not necessary in routine practice. (Sharp pinwheels can also transmit infectious diseases such as hepatitis and AIDS; sterilization before each use is mandatory!) It generally suffices to describe a deficit as either a deficient sense of touch (hypesthesia) or an absent sense of touch (anesthesia). Depending on the clinical situation, the examiner may want to measure sensation quantitatively in a particular dermatome or in the distribution of a particular peripheral nerve, or to compare sensation on mirror-image sites on the body.
Two-point discrimination, stereognosis. The epicritic component of the sense of touch (ultimately derived from Greek krites, “judge”) is tested on the pads of the fingers, e.g., by determining the patient's ability to discriminate two simultaneous stimuli located close together. This can be done with a pair of calipers or simply with the two points of an unfolded paper clip. The two pointed ends are placed on the skin simultaneously, initially very close together, and then at increasing distances until the patient reports feeling two separate stimuli. The threshold distance is usually larger when the stimuli are simultaneous than when they are successively applied; on the fingertips, it should be no more than 5 mm. Epicritic sensation can also be tested by having the patient identify a coin by touch, or “read” a number written on the patient's fingertip. Normal performance on these tests also requires intact stereognosis.
Vibration and position sense. Vibration sense (pallesthesia) is tested with a vibrating 64- or 124-Hz tuning fork solidly placed on various bony prominences of the body, i. e., sites where the bone is covered only by skin. The intensity of vibration can be graduated, if desired, with the aid of special adjustable tuning forks, such as the Rydel–Seiffer model, which allows grading in eighths. This is mostly unnecessary, as there is an easier method: as soon as the patient reports that the vibration is no longer felt, the examiner tests his or her own vibration sense with the same tuning fork at an analogous position. If the examiner still clearly feels the vibration, then the patient unquestionably has a deficit of vibration sense (the rarely used scholarly terms are pallhypesthesia for a partial deficit, pallanesthesia for a total deficit). Milder deficits can usually be detected only in the periphery (e.g., at the ankles), while more severe ones are evident further up the trunk. Vibration sense usually declines by one- or two-eighths over the course of normal aging.
The examiner tests position sense by passively moving some part of the patient's body (in the hands, usually the middle finger) and asking the patient in which direction it is being moved. The patient should not, of course, be able to observe the movement visually.
Temperature sense (thermesthesia) should be tested particularly when a central lesion is suspected, because the pain and temperature pathways run separately from those of the other sensory modalities in the spinal cord and brainstem, and do not join them until the level of the thalamus (p. 74).
A lesion that affects the spinothalamic tract in the spinal cord or brainstem, but spares the other sensory pathways, produces a dissociated sensory deficit: pain and temperature sensation are impaired in the corresponding part of the body, but the sense of touch is preserved. A partial deficit of temperature sense is called thermhypesthesia, a total one thermanesthesia.
To test the sense of temperature, the examiner fills two test tubes or special-purpose metal containers with cold and warm water and applies them to different parts of the patient's body. Thermal stimuli can be delivered in graded fashion, if desired, by varying their temperature, area, and duration.
The ability to feel pain (algesia) should be tested by pinching a fold of skin, never by pinprick. A partial deficit is called hypalgesia, a total one analgesia.
Allesthesia or allocheiria is the perception of a tactile stimulus somewhere other than the site at which it was delivered. This phenomenon can occur in normal individuals and is of uncertain significance. (Alloesthesia and allochiria are variant spellings.)
![]() Examination of the Trunk
Examination of the Trunk
The back and spine are examined with the patient standing. Inspection may reveal scoliosis or an alteration of the normal lordosis or kyphosis of particular segments of the vertebral column. Protruding ribs on one side (often visible only when the patient bends forward) are a sign of torsional scoliosis. As one looks at the patient from behind, there is a triangular gap to either side of the patient's waist, formed by the dependent arm, the rib cage, and the upper border of the pelvis; asymmetry of this gap is a further sign of scoliosis. A plumb line from the spinous process of C7 should overlie the natal cleft; deviations should be measured and documented (preferably in centimeters, rather than finger breadths). One should also look for stepping of the lumbosacral vertebrae (e.g., in spondylolisthesis, p. 260) or tenderness of the spinous processes to pressure or percussion. Techniques for testing the mobility of the cervical spine were described above in Examination of the Head and Cranial Nerves (p. 16). The mobility of the thoracolumbar spine is tested by having the patient bend the trunk forward, backward, and to either side, and then rotate it to either side. On forward bending with extended knees, young patients should be able to touch the ground (finger-to-ground distance 0 cm). Spinal mobility can be quantified with the two Schober tests: the small Schober index pertains to the lumbosacral spine, the large Schober index to the thoracic spine. To measure the small Schober index, place a mark on the patient's skin 10 cm above the spinous process of L5, have the patient bend forward as far as possible, and measure the distance again; it should now be at least 15 cm. The large Schober index is measured similarly, starting from a point 30 cm below the spinous process of C7, which on maximal forward bending should move to at least 32 cm below it. Any diminution of the normal cervical lordosis is best seen when the patient stands with shoulders and heels to the wall and bends the head as far back as possible. The back of the patient's head normally touches the wall; if not, the distance from the occipital protuberance to the wall should be measured in centimeters. An abnormality of this type is found, e.g., in ankylosing spondylitis.
Reflexes. The abdominal skin reflexes are extrinsic muscle reflexes. They are tested by rapid stroking of the abdominal skin (e. g., with a wooden stick) from lateral to medial, at three different segmental levels, on either side. They can be enhanced, if necessary, by having the patient lift his or her head off the headrest. Diminution of the abdominal skin reflexes indicates a lesion of the pyramidal pathway. A diminished or absent reflex at only one level on one side suggests a segmental peripheral lesion. Total bilateral absence is usually an artifact of deficient examining technique, but may also be caused by an obese or flaccid abdominal wall (e.g., after pregnancy). “True” bilateral absence of all abdominal skin reflexes is seen in bilateral lesions of the pyramidal pathway; an accompanying sign in such patients is unusual briskness of the intrinsic reflexes of the abdominal musculature. These are tested by tapping at the sites of muscle attachment, e.g., at the costal margin or the symphysis pubis. Alternatively, the examiner can place his or her own hand on the abdomen and tap on it. The cremaster reflex is tested (in males) by stroking the medial surface of the thigh or by forceful pressure with a finger near the origin of the adductor muscles. The anal reflex is tested by stimulating the perianal skin, e.g., with a pointed wooden stick. This induces reflex contraction of the anal sphincter. The anal reflex is sometimes easier to appreciate on rectal examination with a gloved finger (with which the examiner can also assess sphincter tone); it is abolished by lesions of the cauda equina and conus medullaris (p. 143 ff.).
Sensation. Sensation on the trunk is tested to localize a possible sensory level due to a spinal cord lesion. A sensory level is a segmentally delimited sensory deficit. If caused by a bilateral lesion of one or more spinal nerve roots, it is limited to one or a few dermatomes; if caused by spinal cord transection, it covers the entire body from the toes up to the rostral border of the injured spinal segment. The segmental height of a sensory level should be located as precisely as possible by testing both from above and from below.
![]() Examination of the Lower Limbs
Examination of the Lower Limbs
The procedure here is essentially the same as in the upper limbs (cf. Examination of the Upper Limbs,pp. 27 ff.). Particular attention should be paid to the examination of the peripheral pulses, because pathological processes frequently affect the circulation of the lower limbs. The pedal and popliteal pulses should be palpated; the pulses in the abdominal vessels should be examined by auscultation, as should those of the femoral a., both in the groin and in the proximal adductor canal. The Ratschow test is a provocative test of the blood supply to the leg: the examiner holds up both legs of the supine patient and the patient rotates the feet back and forth. A normal individual can do this for several minutes without difficulty, but, if arterial insufficiency is present, pain soon develops in the feet. In addition, when the legs are brought back to the horizontal position, the skin takes a longer time than normal to regain its usual pink color (in patients of light complexion) and venous refilling is likewise delayed.
Coordination and Strength
The following motor tests should be performed: in the heel–knee–shin (HKS) test, the patient closes the eyes, brings the heel of one leg through the air in a wide arc to place it on the opposite knee, then slides the heel down the shin to the front of the ankle, and finally back up to the knee (Fig. 3.28). Unsteadiness indicates ataxia. In the postural test, the patient lies supine, raises the lower limbs so that the hips and knees are at right angles, and holds them in this position (Fig. 3.29). The examiner looks for possible sinking of a leg, indicating (mild) paresis. Strength, too, should be tested in the supine patient. Additional special tests are used for individual muscle groups. For example, a patient with quadriceps weakness has trouble stepping up onto a stool or chair, or standing up from a sitting position (if the weakness is bilateral). The dorsiflexors of the feet and toes should always be tested, because these distal muscles are frequently weakened early in the course of many different neurological disorders. Great toe dorsiflexion, for example, is weak in L5 radiculopathy. In suspected polyneuropathy, it may be useful to palpate the contractions of the muscles of the dorsum of the foot and to compare the patient's ability to spread the toes on the two sides.
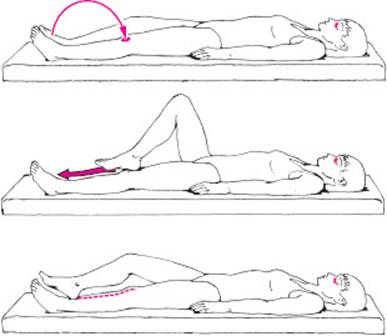
Fig. 3.28 The heel–knee–shin test. With eyes closed, the patient brings one heel to the opposite knee, then slides it down the shin.

Fig. 3.29 Postural test of the legs in the supine position.
Reflexes
Intrinsic muscle reflexes. The quadriceps reflex (patellar tendon reflex) and Achilles' reflex are the most important intrinsic muscle reflexes of the lower limb. They should be tested in every patient (Fig. 3.30). In some situations, it may also be advisable to test the adductor reflex or the knee flexor reflexes. The latter are elicited by tapping the biceps femoris tendon (lateral border of the popliteal fossa) and the semimembranosus and semitendinosus tendons (medial border of the popliteal fossa). The inconstantly present tibialis posterior reflex is elicited by a tap on the tendon of this muscle behind the medial malleolus, while the foot is held in mild pronation. The response consists of supination.
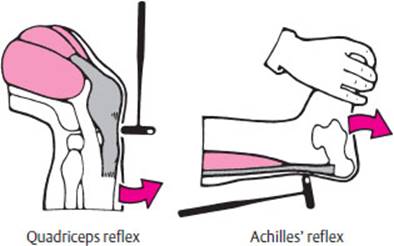
Fig. 3.30 Testing of the quadriceps and Achilles' reflexes.

Fig. 3.31 Pyramidal tract signs in the lower limbs. a Babinski sign. b Oppenheim reflex. c Gordon reflex.
Pathological reflexes. There are a number of important pathological reflexes in the lower limb whose presence implies a lesion of the pyramidal pathway. Chief among these is the Babinski reflex or “Babinski sign” (Fig. 3.31a). To elicit it, the examiner forcefully strokes the lateral plantar surface of the patient's foot, proceeding from the heel toward the toes. The pathological response is a slow, tonic dorsiflexion of the great toe, usually accompanied by fanning of the other toes. (Babinski himself called these phenomena “signe de l'orteil”— the great toe sign— and “signe de I'éventail” —the fan sign.) The same response can sometimes be elicited by stroking other parts of the foot, particularly the anterior ball of the foot from lateral to medial. The Oppenheim sign is the Babinski phenomenon evoked by a painfully intense stroke along the edge of the tibia, from the knee downward (Fig. 3.31b); the Gordon signis the same phenomenon evoked by pressing or forcefully squeezing the calf muscles (Fig. 3.31c). The Rossolimo sign (toe flexor reflex) consists of flexion of the second through fifth toes in response to a tap, from the plantar side, on their distal phalanges; it is a somewhat unreliable indicator of a pyramidal tract lesion. These additional pathological reflexes need not be sought if the “classic” Babinski reflex is present, but only when it is absent or equivocal despite other clinical evidence of a pyramidal tract lesion. “Mute soles,” i. e., the lack of any toe movement at all when the Babinski reflex is tested, is a preliminary stage of the Babinski reflex in some patients and clinically meaningless in others. Mute soles in deeply comatose patients are associated with a poorer prognosis.
All of the important reflexes of the lower limbs are summarized in Tables 3.5–3.7, including the normal intrinsic and extrinsic muscle reflexes and the pathological reflexes.
Sensation
The earliest and most sensitive evidence of a mainly distal sensory deficit in the lower limbs, e.g., in polyneuropathy, is an impairment of vibration sense. Normal persons can feel vibration in all joints down to the distal interphalangeal joints of the toes. They can also recognize numbers drawn on the skin of the lower leg and usually on the pad of the great toe as well (stereognosis). Position sense in the great toe is tested by holding it on both sides and alternately dorsiflexing and plantar-flexing it; the patient should be able to state in which direction the toe was moved. Position sense is impaired, for example, by posterior column lesions.
![]() Examination of the Autonomic Nervous System
Examination of the Autonomic Nervous System
Many clinical tests of the autonomic nervous system have been devised; not a few are rather cumbersome. We will merely mention some of them here: testing of pupillary reactivity after the local application of various substances, measurement of the rise in blood pressure after the administration of ephedrine, observation of changes in blood pressure with orthostasis or on a tilt table, observation and measurement of sweating after warming of the body or observation of local sweating with the aid of pilocarpine iontophoresis, measurement of the pulse on inspiration and expiration or after the administration of 1 mg of atropine, assessment of voiding and erectile function (in males), etc. Such tests are generally used only in selected patients to answer specific questions. All patients, however, should be asked about possible disturbances of autonomic function when the history is taken (urination, defecation, sexual function, sweating).
![]() Neurologically Relevant Aspects of the General Physical Examination
Neurologically Relevant Aspects of the General Physical Examination
Many internal illnesses have neurological symptoms, sometimes as the main or sole manifestation of disease. The clinician performing a neurological examination should pay special attention to any potential symptoms or signs of a general, not exclusively neurological condition.
The patient's general appearance may suggest a wasting illness, such as a malignant neoplasm, or an endocrinopathy. Abnormal pallor of the skin may be a sign of anemia and a straw-yellow coloration may indicate pernicious anemia due to vitamin B12 deficiency. The skin should also be carefully inspected for evidence of neurocutaneous diseases, vasculitic processes, or collagen vascular disease, which, taken together, are not at all uncommon. Findings to look for include the café-aulait spots of neurofibromatosis (von Recklinghausen disease), abnormal shape and quality of the nails, herpetic vesicles, etc. The cardiovascular examination is very important: the blood pressure must be measured, pulses felt in the upper and lower limbs, and vascular bruits listened for, particularly in the neck, the supraclavicular fossae, the abdomen, and the groin bilaterally. The patient should also be examined for possible organomegaly or lymphadenopathy.
![]() Neuropsychological and Psychiatric Examination
Neuropsychological and Psychiatric Examination
Psychopathological Findings
Many neurological illnesses are associated with psychiatric disturbances of greater or lesser severity. The organic neurological clinical picture is only complete once any psychopathological abnormalities that may be present have been thoroughly assessed and documented.
The examiner should first determine whether the patient is awake and alert. If not, he or she will be unable to receive and process incoming stimuli in the normal way. The patient may have a disturbance of consciousness of varying degrees of severity, ranging from drowsiness to coma, as described in Table 3.9.
In addition to the patient's level of consciousness and attention, the examiner should assess his or her orientation, concentration, memory, drive, affective state, and cognitive ability. The overall psychopathological picture is composed of these elements. If mental functioning is disturbed by an underlying neurological illness (so called psycho-organic syndrome or organic brain syndrome), the manifestations often progress in a characteristic sequence, regardless of the etiology. At first, short-term and long-term memory, concentration, and attention are impaired; the patient is easily fatigued and has difficulty processing new information or performing complex tasks. Later, the patient becomes progressively disoriented, first to time, then to place, and then to person. Reactive depression is common at this stage. Ultimately, all spontaneous activity ceases; the patient loses interest, lacks drive, and in the end becomes permanently confused. Disturbances of this type can often be discerned in the patient's behavior, growing increasingly evident to the examiner over the course of the clinical interview and physical examination. Further historical data from the patient's family are often helpful. The MiniMental Status Test(Table 3.10) is widely used to assess cognitive function. For congenital psycho-organic abnormalities (mental retardation) and acquired forms (dementia), see p. 137.
Table 3.9 Degrees of impairment of consciousness, and other abnormal states of consciousness
|
Designation |
Features |
|
Normal consciousness |
oriented to place, time, and person (self), answers questions promptly and appropriately, follows commands correctly |
|
Drowsiness |
mostly awake, responds to questions and commands slowly but usually correctly (after repetition if necessary), moves in response to a sufficiently intense stimulus, usually oriented and coherent |
|
Somnolence |
mostly asleep, arousable with a moderately intense stimulus, generally requires repetition of questions or commands but then responds correctly, reacts slowly and after a delay but usually correctly |
|
Stupor |
asleep unless awakened, can only be awakened with a strong (auditory) stimulus or perhaps only with a mechanical stimulus, cannot answer questions or follow commands or does so only after intense repetition, and then only incompletely |
|
Coma |
unconscious, cannot be awakened, does not respond to a verbal or auditory stimulus, may respond to painful stimuli of graded intensities with specific (localizing) self-defense, nonlocalizing withdrawal of a limb, or abnormal flexion or extension responses, depending on the grade of coma (see also Table 2.54) |
|
Confusion |
inappropriate spontaneous behavior and responses to questions and commands, deficient orientation to place, time, and/or person (self); the confused patient may be fully conscious, less than fully conscious, or agitated (see below) |
|
Agitation |
motor unrest, inappropriate spontaneous behavior, cannot be quieted by verbal persuasion, more or less disoriented, does not follow commands appropriately |


Neuropsychological Examination
The neuropsychological examination is designed to detect cognitive deficits (particularly in the areas of language, recognition, and the performance of motor tasks) and disorders of perceptual processingthat may be due to a focal cortical lesion.
The localizing significance of various neuropsychological deficits is illustrated in the diagram of Fig 3.32.
Aphasia. Language disorders due to cortical disfunction are called aphasia and are generally caused by left-sided lesions. A basic distinction is drawn between abnormalities of language production (motor aphasia or Broca aphasia) and of language comprehension (sensory aphasia or Wernicke aphasia). In Broca aphasia, there is a paucity of spontaneous speech, even though the “organic apparatus” for speech production (phonation, respiration, vocal muscles) remains intact. In Wernicke aphasia, speech comprehension is impaired despite intact hearing and processing of nonlinguistic auditory signals.

Fig. 3.32 Cognitive deficits that typically result from focal brain lesions (diagram adapted from A. Schnider).
The examiner begins to assess the patient's spontaneous speech while taking the history; if necessary, the patient can be given specific language tasks, e.g., “Describe this picture.” Various kinds of abnormality may be noted. The patient's utterances may be found to be unusually poor in meaning-bearing words and overloaded with connectives and “function words.” Sentences may be faultily constructed (paragrammatism). The flow of speech may be either considerably greater than normal or slow and hesitant (telegraphic speech). Individual words may be deformed in certain characteristic ways (e. g., sound substitutions or phonematic paraphasias, such as “cog” for “dog”), or words may be used in place of other words from the same semantic category (semantic paraphasias, e. g., “table” for “chair”). Some words may be replaced by invented pseudowords (neologisms). Impaired language comprehension may be manifested by the patient's inability to point out various objects in the room, including parts of his or her own body, when these are named by the examiner. Complex commands are an even more sensitive functional test. The patient can be asked, for example, to place a certain named object in between two other named objects, or to interpret a complicated sentence, such as the following: “Not in the closet, but on top of it, was where he had placed his hat. Where was the hat?” Aphasic patients often make errors in the repetition of spoken sentences and in the naming of objects or parts of the body that are shown to them. Reading and writing may also be impaired.
Disturbances of spatial processing are usually caused by right-hemispheric lesions. Evidence for such a disturbance is present if the patient has unusual difficulty in spontaneously drawing or copying three-dimensional figures (cube, house, etc.). Deficits of this kind are often accompanied by neglect of the left side of space and the left half of the patient's own body (hemispatial neglect).
Apraxia. Disturbances in the goal-directed execution of complex actions or sequences of actions are known as apraxia. If the individual components of a single action cannot be put together correctly, the patient is suffering from ideomotor apraxia. Different parts of the body can be affected individually. In facial apraxia, for example, the patient may be unable to follow a command to execute certain motor tasks with the face, e.g., drinking through a straw or clicking the tongue. A patient with ideomotor apraxia of the upper limbs may be unable to salute or to mime the action of slapping someone in the face; a patient with ideomotor apraxia of the lower limbs may be unable to kick an imaginary football. In ideational apraxia, individual actions can be performed, but cannot be combined into more complex sequences. A patient might thus be unable to ready a letter for mailing, as this requires several steps: folding the letter, putting it in the envelope, sealing the envelope, and putting a stamp on it. Cortical lesions causing apraxia are usually on the left side.
Agnosia is an inability to recognize and correctly interpret incoming stimuli in a particular sensory modality even though sensation as such is intact. A patient with visual agnosia, for example, has no visual impairment but cannot recognize objects on sight; the patient can name an object only after feeling or hearing it (e.g., the jangling of a bunch of keys).
Special types of agnosia include an inability to recognize colors (color agnosia) or faces (prosopagnosia). The responsible lesion is in the visual association cortex, i. e., in the occipital or occipitotemporal region, in one or both hemispheres. Stereognosis is tested by putting a familiar object (key, pair of scissors) in the patient's hand and asking him or her to palpate it and name it (with eyes closed). An inability to do this despite intact sensation is called tactile agnosia. Further special types of agnosia are finger agnosia and autotopagnosia (difficulty recognizing parts of one's own body). Anosognosia is the denial or trivialization of one's own neurological deficits, e.g., hemiplegia or even blindness.
Higher cognitive functions. More than just the basic neuropsychological functions described above must be intact so that the individual can thrive in his or her social environment and cope adequately with the demands of everyday life. A person's fund of knowledge, memory, intelligence (by which we mean a capacity for abstract thought and problem solving), personality, and social behavior are all of vital importance, as are his or her mood and motivation. The assessment of these higher cognitive functions requires a careful weighing of historical information (particularly from persons in the patient's social environment: family, friends, colleagues), in addition to certain standardized neuropsychological tests. There are specific tests for the patient's fund of knowledge, logical thinking, and cognitive skills such as the recognition of differences, the formation of categories, and the interpretation of symbolic information, e. g., proverbs. These so-called higher “integrative” functions depend not only on an intact cerebral cortex, but also on other, deeper regions of the brain.
![]() Special Considerations in the Neurological Examination of Infants and Younq Children
Special Considerations in the Neurological Examination of Infants and Younq Children
Most of the techniques presented above for the neurological examination of adults cannot be used in infants or small children. In this age group, the important clinical indicators of nervous system function are body posture, spontaneous motor behavior, and the reflex motor responses induced by certain specific stimuli.
In taking the clinical history, the examiner must inquire about any problems that may have occurred during the child's gestation and delivery. In the physical examination, attention should be paid to any constant, fixed postures of the limbs or asymmetry of the skull (plagiocephaly). The tension of the fontanelles should also be assessed by inspection and palpation.
Reflexes
General aspects. The primitive motor functioning of healthy infants and toddlers is mainly controlled by a number of reflex mechanisms. These reflexes can be affected by neurological disease so that they are absent, or exaggerated, or persist beyond the age at which they normally disappear.
Postural reflexes control the posture of the body and its relation to the ground. Positioning reflexes return the body to a “normal” position after a perturbation; the vestibular system plays an important role in these reflexes. Finally, statokinetic reactions and equilibrium reactions provide the body in motion with important protective movements and righting responses.
The manner of eliciting the reflexes described in this section is illustrated in Fig 3.33.
Reflexes reflecting the state of maturation of the infantile CNS. A wide variety of reflexes can be pathologically altered in developmental disorders of the CNS. We will only present the more important ones here.
The doll's-eyes phenomenon is induced by turning the head from side to side or up and down, in an awake, supine infant. The eyes make a compensatory movement in the opposite direction and thus stay in their original position with respect to outside space. This vestibular reflex is demonstrable at birth and persists for the first six weeks of life.
The foot placement reflex is elicited by holding the infant upright under the axillae (while supporting the head) and allowing the dorsum of a foot to touch the edge of the table. A normal newborn infant will flex the hip and knee and put the foot on the table. This reflex disappears in the first few weeks of life.
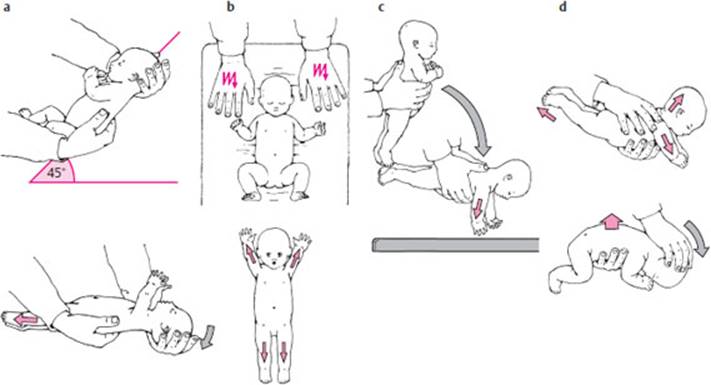
Fig. 3.33 Reflexes in the infant. a Moro reflex: the infant is held by the examiner in a diagonal, half-supine position, with one hand under the trunk and one hand supporting the head. When the examiner suddenly tips the infant toward the horizontal, momentarily reducing the supportive pressure on the occiput, the infant extends its upper and lower limbs. b The same response can be induced in a supine infant if the examiner suddenly strikes and depresses the mattress. c Parachute reflex: the examiner suddenly tips the infant forward, from a vertical position toward the horizontal. Normally, the arms are extended, as if to break the infant's fall. d Landau reflex: an infant held around the trunk in a prone position tends to keep the limbs extended and the head tilted upward. When the head is passively tilted downward, the normal response is flexion of the limbs (positive Landau reflex). (Modified from Lietz, R.: Klinische-neurologische Untersuchung im Kindesalter, 2nd edn, Deutscher Ärzteverlag, Cologne, 1993).
The stepping reflex is seen when the examiner holds the infant under the axillae so that the soles of the feet just touch the surface of the examining table and then slowly moves the infant forward. The infant will then make stepping movements with the feet. This reflex, too, is elicitable only in the first few weeks of life.
In the tonic hand-grasp reflex, the infant forcefully grasps the examiner's index finger when it is placed in the palm of the hand. The grasp is so tight that the infant can even be held up by the examiner's finger. In the analogous foot-grasp reflex, there is tonic flexion of the toes on stimulation of the sole of the foot. The tonic hand-grasp reflex is present in the first two months of life, then gradually diminishes till it totally disappears, usually in the third month of life, and no later than the fourth.
To elicit the Moro reflex, the examiner holds the infant in a diagonal, half-supine position, with one hand under the trunk and one hand supporting the head. The infant is then suddenly tipped toward the horizontal, while the support under the occiput is momentarily released. The body flexes as if in fright and the arms are first extended and then brought forward as if in a hug (Fig. 3.33a). A similar response can be elicited in a supine infant by suddenly striking and depressing the mattress (Fig. 3.33b). The Moro reflex is no longer seen after the third or fourth month of life. Its absence in the first few months of life is usually associated with severe brain damage.
Support reactions are tested by pressing on the infant's palms or soles. The infant extends the corresponding limb as if to support its weight with it. Support reactions are present at birth in the legs and develop in the arms over the first four or five months of life. Cerebral lesions make these reactions abnormally intense.
The positioning reflexes are evoked by a combination of afferent input from the vestibular system and from receptors in the skin, joints, and muscles. In the parachute reflex, the vestibular system plays the most important role: the examiner holds the infant around the trunk with both hands, lifts it off the examining table, holds it at about a 60° angle, and then suddenly tips the infant forward into a horizontal position, near the surface of the table (or crib). Infants aged about four months or older will extend their arms, downward and in mild abduction, and open their hands, as if to break the fall (Fig. 3.33c).
In the Landau reflex, the examiner first lifts the infant into the air in a prone position; the infant will respond by extending the limbs and head. The examiner then flexes the infant's head, and the infant flexes the limbs as well (Fig. 3.33d). This reflex should be demonstrable from the fourth to the 18th month. In infants with cerebral damage, the Landau reflex appears late or not at all, or else it persists longer than normal.
To elicit the asymmetric tonic neck reflex (nuchal reflex), the examiner slowly turns the supine infant's head to one side, while preventing any movement of the shoulders. The arm and leg are then extended on the side to which the head is turned and flexed on the other side (fencing posture). This reflex is present in newborns and disappears at the age of four months. Persistence after the sixth month is pathological.
The Babinski sign (p. 38) is normally present in infants and usually disappears when the child learns to walk. It is absent in all healthy children from the age of two years onward.
The diagram in Fig. 3.34 represents the stages of normal motor development in infancy and early childhood. Some abnormal findings that may suggest a cerebral motor disorder at different times in the first year of life are listed in Table 3.11.
Table 3.11 Findings suggesting a cerebral motor disorder in the first year of life
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

Fig. 3.34 Stages of normal motor development in infancy and early childhood.