Rachel P.G. Rosovsky
INTRODUCTION
The association between cancer and thrombosis was first proposed by Armand Trousseau (Figure 19-1) when he recognized the condition of thrombophlebitis migrans, as a forewarning of occult malignancy (1). In 1865, he remarked, “Should you, when in doubt as to the nature of an affection of the stomach, should you when hesitating between chronic gastritis, simple ulcer, and cancer, observe a vein become infected in the arm or leg, you may dispel your doubt, and pronounce in a positive manner that there is a cancer …” (1). Although the association of hemostatic disorders and cancer has been studied extensively over the past 100 years, venous thromboembolism (VTE), defined herein as pulmonary embolus (PE) or deep vein thrombosis (DVT), remains a major cause of morbidity and mortality in cancer patients.
FIGURE 19-1 Armand Trousseau.
This chapter will explore the pathogenesis of thrombosis in cancer as well as the epidemiology and risk factors. The chapter will also focus on novel risk assessment models and the emergence of new biomarkers to classify patients at high risk of developing VTE. Current diagnostic and management strategies for VTE in cancer patients and the challenges of antithrombotic therapy in this population will be examined. This update will evaluate the results of several randomized controlled trials aimed at assessing the clinical benefit of antithrombotic prophylaxis in cancer outpatients. Finally, new therapeutic developments in this area will be addressed.
PATHOGENESIS
The pathophysiological mechanisms of thrombosis in cancer patients are complex and involve multiple clinical and biological factors including tumor cells, the hemostatic system, inherited and acquired thrombophilia, and exogenous contributors such as chemotherapy and radiotherapy (2). Tumors contribute to thrombosis through the expression of procoagulant factors including tissue factor, cancer procoagulant, and adhesion molecules. Recent experimental models of human cancers have shown that an integral feature of neoplastic transformation from cancer cells is through activation of clotting proteins (3–6). The role of tissue factor-bearing microparticles (MP) contributing to thrombin generation has also been explored in vitro and in vivo studies. Zwicker et al. found that VTE developed in 34.8% of cancer patients with elevated levels of MP compared to 0% in those without detectable levels (7). Tumor cells can also induce platelet activation and aggregation through secretion of proteases. Tumor-related release of various cytokines, growth factors, and proteases including tumor necrosis factor α (TNFα), interleukin 1β, and vascular endothelial growth factor (VEGF) contribute not only to angiogenesis and inflammation but also to the activation of the hemostatic system. Furthermore, tumor cells interact directly with the host blood vessels, endothelial cells, leukocytes, and monocytes leading to host cell inflammatory responses (2). These many and varied interactions lead to both a direct and an indirect activation of the clotting system, an increase in thrombin generation, and ultimately a hypercoagulable state.
EPIDEMIOLOGY
Venous thrombosis is a common complication in patients with cancer. Although the exact incidence of VTE in cancer patients is unknown, it occurs in approximately 15%, with reports ranging from 4% to 30% (8, 9). These numbers likely underestimate the problem as VTE often causes no symptoms. In a recent study, clinically unsuspected PE was present in up to 4.4% of oncology patients undergoing CT scans for other indications (10). If symptoms are present, they are often nonspecific or attributed to a patient’s underlying malignancy.
Certain malignancies exhibit high rates of VTE, such as hematological malignancies and neoplasms, especially if high grade, of the pancreas, gastrointestinal tract, ovary, brain, colon, kidney, lung, and prostate (11–15). However, it is unclear if the high rates are due to the underlying properties of particular cancers or merely reflect the high prevalence of certain cancers. Nevertheless, it is well documented that cancers diagnosed at the same time as an episode of VTE are more likely to have distant metastases and lower survival rates (16, 17). One study showed that cancer patients with VTE had a 1-year survival of 12% as compared to 36% in cancer patients without VTE (17). Similarly, patients who develop VTE within a year after a cancer diagnosis are more likely to have advanced stage and poorer prognosis when compared to analogous cancer patients without VTE (17). A study of over 235,000 cancer patients showed that after adjusting for age, race, and stage of disease, VTE at the time of or within 1 year of cancer diagnosis was a significant predictor of death within that year (16). VTE is the second leading cause of death in cancer patients, with cancer progression being number one (18). It also appears that cancer patients with VTE are two to three times more likely to have recurrent VTE and two to six times more likely to experience hemorrhagic complications from anticoagulant therapy than noncancer patients with VTE (19, 20). These findings clearly indicate that VTE may be more aggressive and difficult to treat in cancer patients than in noncancer patients.
The association between cancer and thrombosis is further supported by many studies, suggesting that an idiopathic VTE is often associated with occult cancer. Approximately 10% of patients who present with an idiopathic or unprovoked VTE are diagnosed with cancer within the next 1–2 years (21). These provocative findings raise the unanswered question as to whether all patients with idiopathic VTE should undergo extensive cancer screening. The SOMIT study attempted to address this matter (22). Patients with an idiopathic VTE were randomized to either extensive or nonextensive cancer screening and followed for 24 months. Subjects in the extensive screening arm seemed to have a shorter delay in the diagnosis of cancer, their cancers were detected at earlier stages, and they had a lower cancer-related mortality (22). Unfortunately, this trial was stopped prematurely due to recruitment issues leaving these conclusions unsubstantiated. In a more recent prospective cohort study of 630 patients with a first episode of idiopathic VTE, extensive screening, which included abdominal and chest CT and mammogram, detected six additional cancers (2.0%; 95% CI, 0.74–4.3), compared to limited screening (23). At the 2.5 years of follow-up, cancer was diagnosed in 3.7% in extensive screening group and 5.0% in limited and there was no significant difference in death rates. Thus, this study concluded that the low yield of extensive screening and lack of survival benefit did not support routine screening for cancer in patients with an idiopathic VTE.
A recent systematic review of this question found that an extensive screening strategy employing an abdominal and pelvic CT statistically significantly increased the number of undiagnosed cancer from 49.4% to 67% in patients with an unprovoked VTE (24). However, this review could not address the complication rates, cost-effectiveness, or morbidity and mortality difference associated with an extensive screening approach. The use of PET-CT was recently investigated to screen for occult malignancy in 40 patients who presented with an unprovoked VTE (25). Twenty-five patients (62.5%) had abnormal findings requiring additional evaluations and of these, only one occult malignancy was discovered. This malignancy, however, was detected in a patient with unexplained abdominal pain and unintentional weight loss of 40 pounds, which are symptoms concerning for a malignancy. Hence, larger studies are needed to evaluate the cost-effectiveness of PET-CT in this population.
Current recommendations are to provide age appropriate cancer screening for patients who present with idiopathic VTE, and any additional testing should be driven by what is discovered in a thorough history and physical examination. Given the SOMIT observations, albeit underpowered, future studies evaluating extensive cancer screening for patients with idiopathic VTE are warranted.
RISK FACTORS
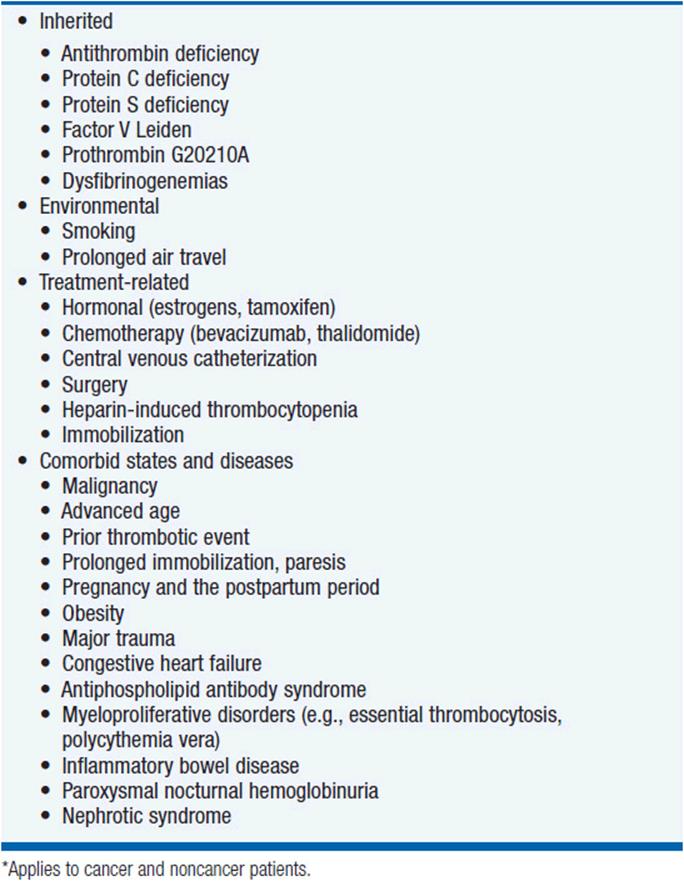
Many inherited and acquired risk factors are associated with the development of VTE and are listed in Table 19-1. Cancer patients may have additional risk factors related to their malignancy, including surgery, immobilization, chemotherapy, some forms of hormone therapy, and the presence of indwelling central venous catheters (CVCs). Without appropriate prophylaxis, cancer patients have twice the risk of developing postoperative DVT and three times the risk of developing a fatal PE than patients without cancer (26). Long-term immobilization, often due to lengthy hospital stays, also increases the risk of developing VTE. Furthermore, comorbid conditions, distant metastases, advanced age, obesity, prior history of VTE and elevated platelet count are associated with increased VTE risk (12, 13, 27, 28).
TABLE 19-1 RISK FACTORS FOR VENOUS THROMBOEMBOLISM (VTE)*
In addition to patient-related risks, there are treatment-related risks. Tamoxifen, estrogen, thalidomide, L-asparaginase, cisplatin, and VEGF inhibitors are a few of the cancer therapies associated with high rates of thromboembolic complications, especially when used in combination with other chemotherapeutic agents. In a trial involving over 2600 women with early stage breast cancer, the incidence of developing VTE was 0.2% with placebo and 0.9% with tamoxifen (29). Another trial involving women with advanced stage breast cancer showed that the incidence of VTE was 2.6% with tamoxifen alone versus 13.6% with tamoxifen plus chemotherapy (30). Similarly, in studies involving multiple myeloma, treatment with thalidomide alone had a risk of 2%. The risk increased to 33% with the addition of chemotherapy (31). Cancer patients who receive either cytotoxic or immunosuppressive therapy have a 6.5-fold increased risk of developing a VTE when compared to noncancer patients, and a twofold increased risk compared to cancer patients not receiving chemotherapy (32). In a recent systematic review of 8216 cancer patients, those receiving cisplatin-based chemotherapy had a significantly increased rate of VTE compared to patients who did not (RR, 1.67l 95% CI, 1.25 – 2.23; p = 0.01) (33). Furthermore, venous thrombosis, and in particular, cortical sinus thrombosis, is a frequent complication of L-asparaginase treatment, and it is related to inhibition of the synthesis of anticoagulant factors, protein C and protein S.
Erythropoiesis-stimulating agents (ESAs) are often given to patients with chemotherapy induced anemia. However, recent studies show that ESAs administered to patients with cancer increase not only risk of VTE but also risk of mortality (13, 34, 35). As such, the FDA label now limits the use of ESA to patients receiving chemotherapy for palliative intent. ESAs are no longer indicated for patients receiving chemotherapy for curative intent.
Many new antiangiogenic agents are under investigation and used in practice to treat a variety of cancers. In a systematic review of 15 RCT, patients receiving bevacizumab, the recombinant humanized monoclonal antibody to VEGF, had an increased risk of VTE compared to controls (RR 1.3; 95% CI, 1.13–1.56; p<0.001) (36). Similarly in a meta-analysis of anti-epidermal growth factor receptor (EGFR) agents, the associated RR of VTEs was 1.32 (95% CI 1.07–1.63; p = 0.01) in patients who received anti-EGFRs versus controls (37). The risk was highest with the use of cetuximab and panitumumab (13).
CVCs are another common risk factor for VTE. These devices are commonplace among cancer patients who require long-term chemotherapy. The reported incidence of catheter-related thrombosis ranges from 5% to 75%, and this wide range likely reflects the distinct types of malignancy, the kind of catheter used, and the duration of its implantation (38). In addition, the complications associated with CVC-related thrombosis can result in loss of catheter function, postphlebitic syndrome of the upper extremity, PE, and even mortality. There have been major efforts to identify disease management approaches to decrease the risk of VTE with CVC, and these mechanisms are discussed in the Prevention section of this chapter.
RISK PREDICTIVE MODELS
Trying to predict the risk of VTE in cancer patients is a major clinical challenge. Patients at high risk of developing VTE may benefit from prophylactic anticoagulation, whereas patients at low risk may have unnecessary and unfavorable consequences from this practice, such as bleeding. Therefore, the development of risk assessment tools and predictive biomarkers to identify high-risk patients is clinically relevant and important.
One novel and promising tool is the Khorana score, which uses baseline clinical and laboratory variables to predict the risk of chemotherapy-associated VTE (39). The score assigns points to cancer site (2 points for very high-risk sites such as pancreatic or gastric and 1 point for high-risk sites such as lung, ovarian, or bladder), platelet count ≥350 × 109/l (1 point), hemoglobin ≤ 10 g/dl or the use of erythropoietin-stimulating agents (1 point), leukocyte count ≥11 × 109/l (1 point), and body mass index ≥35 kg/m2 (1 point). A score of ≥3 is considered high risk and correlates with a rate of symptomatic VTE in 6.7% of patients undergoing chemotherapy. This model was recently modified in another study to include platinum or gemcitabine-based chemotherapies (40).
The Ottawa score is another clinical prediction rule aimed at identifying recurrent VTE risk in patients with cancer-associated VTE (41). The independent variables include sex, primary tumor site, tumor-node-metastasis (TNM) stage, and prior VTE. High-risk predictors include female, lung cancer, and history of VTE and are given 1 point each. Low-risk predictors include breast cancer and stage 1 cancer of any origins and are given –1 and –2 points, respectively. A score of ≤0 correlates with a low clinical probability of recurrent VTE (<4.5%), whereas a score of ≥1 correlates with a high clinical probability of recurrent VTE (≥19%). Future prospective trials are warranted to demonstrate the reproducibility, generalizability, and safety of the Khorana and Ottawa scores as well as to determine their effectiveness as a tool for treating cancer patients at risk of VTE.
BIOMARKERS
Identifying biomarkers to help predict the risk of VTE in cancer patients is one of the largest growing areas of research. Data from the prospective Vienna Cancer and Thrombosis Study (CATS) demonstrated that elevated levels of P-selectin were predictive of VTE in cancer patients (42). The probability of developing VTE at 6 months was 11.9% in patients with high levels of P-selectin compared to 3.7% in patients with low levels. This group also found that patients with elevated D-dimer and high prothrombin fragment 1+2 (F 1+2) compared to patients with nonelevated levels were associated with an increased risk of VTE (15.5% vs 5%) (43). Thrombin generation is another potential biomarker studied by the Vienna CATS group (44). Elevated peak thrombin levels conferred an 11% risk of developing VTE compared to 4% in patients with lower levels. An expansion of the original Khorana score to include D-dimer and P-selectin appears to improve the VTE risk prediction tool (45). There was a 26-fold higher probability of developing VTE in patients with a high score compared to patients with a low score. However, this expanded risk score requires further validation studies but may be limited by the lack of widely available P-selectin assays.
In the last few years, the role of tissue factor-bearing MP in connection with cancer progression and thrombosis has been investigated. In an immunohistochemical study, high levels versus low levels of MP in pancreatic cancer patients correlated with the development of VTE (26.3% vs 4.5%) (46). Similarly, Zwicker et al. found that VTE developed in 34.8% cancer patients with detectable levels of MP compared to 0% in patients with undetectable levels (7).
Biomarkers may improve the stratification of cancer patients with regard to their risk of VTE. The efficacy and safety of prophylactic anticoagulation in patients with these elevated biomarkers needs to be addressed in well-designed RCTs.
CLINICAL MANIFESTATIONS
Cancer patients can present with a wide range of thromboembolic events. The two most commonly recognized are DVT and pulmonary embolism (PE). However, symptoms and signs may result from migratory thrombophlebitis, nonbacterial thrombotic endocarditis, disseminated intravascular coagulopathy (DIC), thrombotic microangiography, and arterial thrombosis. Cancer patients may also present with multiple clinical sequelae as was originally reported in 1977 by Sack et al. in a review of 182 cases of neoplasia associated with alterations in blood coagulation (47). Figure 19-2 is an expansion of the original Venn diagram created by Sack et al. which represents the interrelations between the various clinical phenomena. Discussion of all these clinical presentations is beyond the scope of this chapter and, therefore, only DVT and PE will be presented in detail.
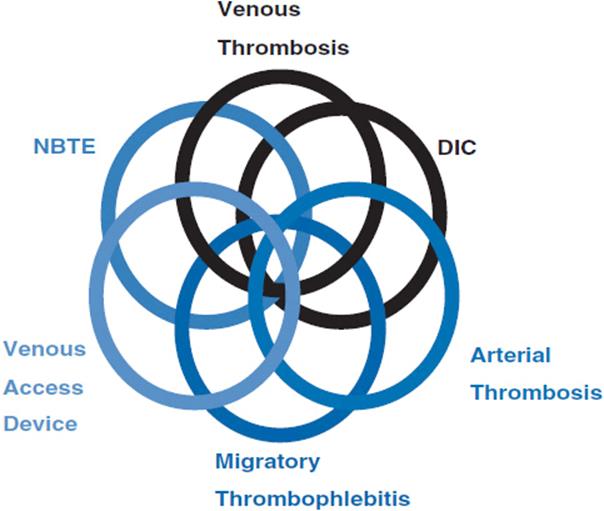
FIGURE 19-2 Venn diagram of relationships between clinical signs.
Patients with DVT may experience complaints of leg pain, swelling, tenderness, discoloration, venous distension, or a palpable cord. Nonspecific symptoms of PE include dyspnea, tachypnea, tachycardia, pleuritic chest pain, cough, and wheeze. Signs may include hemoptysis, hypotension, syncope, coma, pleural effusion, or pulmonary infiltrates. Each of these clinical features can be a manifestation of other cardiac or pulmonary processes, such as pneumonia or heart failure, making the diagnosis of PE difficult.
Data from the MASTER registry in Italy demonstrated that the clinical presentation of acute VTE in cancer patients is different and more extensive than in patients without cancer (48). The incidence of bilateral DVT and rates of iliocaval thrombosis were higher in the cancer patients. The management of VTE in the cancer patients was also more problematic with a higher incidence of hemorrhage and need for inferior vena cava (IVC) filters.
Other consequences of DVT and PE include acute morbidity or even death. Some of the short- and long-term complications due to thrombotic events consist of extension of the clot, embolization, postthrombotic syndrome, pulmonary hypertension, and recurrent VTE. Furthermore, there may be significant morbidity associated with long-term anticoagulation or with placement of an IVC filter. The psychological stress and fear that patients face when suffering from a thromboembolic event must also be appreciated. Moreover, the presence of VTE or its complications may cause delays in chemotherapy or other treatments, which may have considerable consequences for the patient. In one of the largest outcome studies of DVT in cancer patients, the most common complication was bleeding, which occurred in 13% of patients (49). PE, death from DVT, and death from anticoagulation were also observed. The mean length of stay was 11 days with a mean cost of hospitalization of $20,065. VTE as the cause of death was also shown in an autopsy-based study where one out of every seven cancer deaths in the hospital was due to PE (50). Over 60% of those who died of a PE had either limited metastatic or local disease indicating a reasonable chance of prolonged survival if not for the fatal PE (50).
DIAGNOSIS OF VTE
Diagnosing VTE in cancer patients, as in other patients, may be difficult. The signs and symptoms of VTE are often variable and nonspecific, and available diagnostic tests have varying sensitivities and specificities. Moreover, commonly employed models for predicting the probability of VTE have limited value in cancer patients because of the significant additional risk factors at play. Ultimately, a diagnosis requires a combination of modalities.
If VTE is clinically suspected, a common first test is the D-dimer, which reflects the degradation product of cross-linked fibrin. This test is highly sensitive but not specific (51). Because it is elevated in a variety of situations including malignancy, acute VTE, underlying lung abnormalities, recent surgery, hospitalization, and aging, the primary value of the D-dimer test is a negative result, which constitutes strong evidence against significant thrombosis (51). Two recent studies demonstrated that the combination of a normal D-dimer and a low clinical pretest probability was useful in excluding the diagnosis of DVT in cancer patients (52, 53). If the D-dimer test is positive, however, additional diagnostic tests should be performed.
Duplex venous ultrasound (US) imaging, the most widely available modality for diagnosing DVT, is highly sensitive for detecting proximal vein thrombosis but less so for detecting calf vein clots. Therefore, if a patient presents with symptoms suggestive of a calf vein thrombosis but has a negative US test, a repeat test at 3–5 days may be warranted, especially if symptoms persist and no alternative diagnosis has been established. If the US is inconclusive, magnetic resonance imaging (MRI) of the lower extremities is usually definitive.
If PE is suspected, a variety of imaging tests may aid in making the diagnosis, including lung radionuclide scans (VQ), spiral computed tomography (CT), pulmonary angiography, MRI, and magnetic resonance angiography (MRA). Although pulmonary angiography has been the gold standard, it is invasive and often unavailable or impractical and, therefore, has been replaced by CT angiography.
VQ scans, formerly a frequently used diagnostic tool, are now employed only when there is a contraindication to CT scans with contrast, such as renal failure or iodine allergy. VQ scans are helpful when they are either positive or negative, but their results are often inconclusive or confounded by underlying lung abnormalities.
The spiral CT or computerized tomographic angiography (CTA) is highly sensitive for large emboli. Multidetector scanners are able to visualize the subsegmental arteries effectively. Simultaneous imaging of the lower extremities, which is helpful in identifying an associated DVT, can further increase the diagnostic sensitivity of CTA. Moreover, the spiral CT may help identify alternative etiologies for a patient’s symptoms if a PE is not identified.
One of the newest diagnostic tools to diagnose PE, MRI/MRA of the chest, has been incompletely evaluated and standardized. Currently studies are underway to assess its accuracy and safety.
TREATMENT
The management of VTE in cancer patients is a challenge due to the frequent presence of a hypercoagulable state, physical obstructions to blood flow, patient immobility, and the general impression that these patients are relatively resistant to anticoagulant therapy. The goals of treatment are to prevent fatal PE, recurrent VTE, and long-term VTE complications. This section will outline current treatment recommendations for both the acute and long-term treatment of VTE in cancer patients based on the seventh American College of Chest Physicians (ACCP) Conference guidelines and Journal of National Comprehensive Cancer Network (JNCCN) (54, 55).
![]() ACUTE TREATMENT
ACUTE TREATMENT
The initial treatment for DVT and PE are similar. There are three options for anticoagulation: unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and fondaparinux sodium. The use of newer anticoagulants to treat VTE in cancer patients is discussed under the section of New Developments.
LMWH is a fragment of UFH and exerts its anticoagulant effect through antifactor Xa and antithrombin activities. It is cleared from plasma by metabolism in the liver, and a small portion is excreted in the urine. LMWH has largely replaced the use of UFH as the initial treatment for VTE because of its similar efficacy, superior safety profile, and pharmacokinetic advantages that allow for once or twice daily subcutaneous administration without laboratory monitoring, lower risk of complications such as heparin-induced thrombocytopenia (HIT) or heparin-induced osteoporosis, and potential for outpatient treatment. LMWH, a weight-based therapy, may need to be episodically monitored in two particular situations: in patients who are at the extremes of body weight or in those suffering from renal failure, the latter situation because of LMWH clearance by renal excretion. This monitoring involves measuring the antifactor Xa activity 3–4 h after subcutaneous injection with a therapeutic goal of 0.5–1.3 U/ml.
If a patient requires a short-acting initial anticoagulant or one that needs to be carefully monitored, is anticipating an invasive procedure, or has a contraindication to LMWH such as severe renal failure, UFH is the favored treatment. UFH, a glycosaminoglycan, exerts its anticoagulant effect at several steps in the formation of fibrin clots. Specifically, when combined with antithrombin III, it inactivates activated factor X and inhibits the conversion of prothrombin to thrombin. UFH is metabolized in the liver and can be reversed with the antidote, protamine sulfate, if necessary. However, unlike LMWH, UFH is usually given intravenously and needs to be monitored frequently, and the dose must be adjusted with the use of nomograms to maintain an activated partial thromboplastin time (aPPT) of 1.5–2.5 times the normal.
A third anticoagulant option is the synthetic pentasaccharide, fondaparinux sodium, which works by indirectly inhibiting factor Xa. It has similar efficacy and safety for the initial treatment of PE and DVT as UFH or LMWH. It is an attractive medication because of its once daily subcutaneous administration and linear pharmacokinetic profile. In addition, it does not cause a syndrome akin to HIT to date. However, it cannot be reversed and its 17-h half-life makes it an unreasonable option in patients who require a short-acting therapy. In addition, because fondaparinux is excreted unchanged in the urine, monitoring is essential in patients with mild or moderate renal insufficiency, and the medication is contraindicated in patients with severe renal failure. The efficacy of fondaparinux for the initial VTE treatment in cancer patients is limited. Results from a post-hoc analysis of the MATISSE trials suggest that fondaparinux may be more efficacious than UFH but less efficacious than LMWH (56).
Other options for the initial treatment of DVT and PE that are not anticoagulants include thrombolytic therapy, thromboendarterectomy, and IVC filters. The use of thrombolytics is controversial in DVT and currently should be considered only for patients with massive iliofemoral thrombosis and at risk for limb gangrene (54, 57). A meta-analysis has helped clarify the use of thrombolytics for the initial treatment of PE (58). While there was no overall benefit of thrombolytics in terms of recurrent PE or death, patients who were hemodynamically unstable (systolic blood pressure <90–100 mmHg) had a significantly lower rate of recurrent PE and death, but a significantly higher rate of major bleeding (58). The use of thrombolytics has also been considered in patients who are hemodynamically stable but exhibit evidence of severe right ventricular dysfunction. Results thus far are not definitive.
Thrombolytic drugs in current use include tissue-type plasminogen activator (t-PA), urokinase, and streptokinase. T-PA, the most commonly used of the group, is given as a 100-mg infusion over 2 h, followed by heparin. In patients refractory to t-PA, one should consider the presence of a saddle embolus, which might require thromboendarterectomy.
IVC filters are another option for the initial treatment of VTE. They are primarily used in patients with recurrent DVT or PE on anticoagulation, or in patients at high risk of bleeding on anticoagulation. There is little published evidence to document an improvement in outcome after their use. Moreover, if necessary, removable filters are preferred.
![]() LONG-TERM TREATMENT
LONG-TERM TREATMENT
Similar to the initial treatment for VTE, the long-term treatment for VTE in cancer patients can be complicated by the concomitant need for chemotherapy, hormone therapy, invasive procedures, or CVCs. In addition, cancer patients have higher rates of recurrent VTE and bleeding with traditional anticoagulant therapy than noncancer patients, which adds a further challenge to their management. For many years, the long-term treatment recommendation for VTE in cancer patients was similar to that of the general population, the vitamin K antagonist (VKA), warfarin (Coumadin). After the initiation of UFH, LMWH or fondaparinux, warfarin is started on day 1 and adjusted to maintain an INR of 2–3. Given the slow onset of action, there needs to be a 5- to 7-day overlap between the two medications.
Although warfarin has the advantage of being an oral medication, it has significant disadvantages. It requires regular laboratory monitoring, has significant drug interactions because of its cyp 3A4–dependent metabolism, and is influenced by nutritional status. Fortunately, several trials have shown that LMWH is an attractive alternative.
A randomized controlled trial (RCT) demonstrated a clear benefit to LMWH compared with warfarin in cancer patients for long-term treatment or secondary prophylaxis after VTE (59). After 6 months of therapy, cancer patients who received LMWH had a significantly lower rate of recurrent VTE (9%) than those who received warfarin (17%), with no difference in the rates of bleeding (Figure 19-3). In addition, a post-hoc analysis of the patients with nonmetastatic solid tumors revealed a survival advantage in the LMWH group. Twelve-month cumulative mortality in this population was 20% in the LMWH group versus 36% in the warfarin group (60).
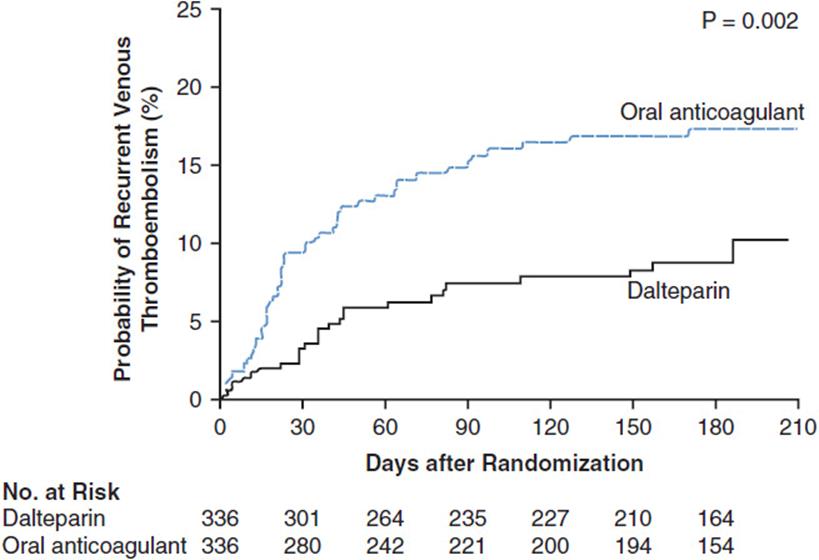
FIGURE 19-3 Recurrent VTE. Kaplan-Meier estimates of the probability of symptomatic recurrent VTE among cancer patients who were randomized to secondary prophylaxis with dalteparin vs warfarin treatment for acute VTE (22). (From Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003; 349: 146–53. Copyright © 2003. Massachusetts Medical Society. All rights reserved.)
The mechanism by which anticoagulants may decrease cancer mortality is not clear. However, in the past decade, multiple trials have suggested a survival advantage in cancer patients receiving LMWH as compared to UFH or warfarin for treatment or prevention of VTE (59). Interestingly, the survival advantages were not solely attributable to decreases in the rate of fatal pulmonary emboli. Three trials studying the value of LMWH in patients without VTE found a significant survival advantage in patients who received LMWH versus placebo (61–63). A recent systematic review and meta-analysis of 4 studies enrolling 898 patients randomized to LMWH versus placebo suggested that LMWH may improve overall survival in cancer patients (64). However, two newer studies did not find a survival benefit with the use of LMWH (23, 65). Furthermore, a number of trials investigating the use of LMWH for thromboprophylaxis in cancer patients receiving chemotherapy have failed to show any survival benefit (66–69). Several ongoing studies are underway to further evaluate this question and to possibly define the tumor types, disease stages, and dosing schedules most likely to have a survival benefit.
LMWHs are thus the most attractive antithrombotic choice for the long-term treatment or secondary prophylaxis in cancer patients. Osteoporosis is a potential complication of LMWH and if no contraindications, these patients should be placed on calcium and vitamin D. Appropriately, the ACCP and JNCCN guidelines recommend LMWH for the first 3–6 months of long-term anticoagulant therapy for cancer patients with VTE (54, 55).
The duration of long-term treatment of acute VTE in cancer patients has not been clearly established. For noncancer patients, in whom the inciting factor has been removed, the recommendation is to treat for 3–6 months. However, in patients with idiopathic VTE, where the inciting factor is unknown and may still exist, two trials have demonstrated decreased recurrence with prolonged anticoagulation beyond 3 months (62, 70). Patients with active cancer are similar to patients with idiopathic VTEs. Thus, current ACCP and JNCCN guidelines recommend anticoagulant therapy as long as there is evidence of active cancer and cancer therapy, whichever is longer (54, 55). Indefinite therapy is recommended for patients with known metastases because their risk of recurrent VTE remains high. It is prudent, however, to re-evaluate patients frequently to re-assess the risk-benefit ratio of continuing anticoagulation.
![]() RECURRENT VTE
RECURRENT VTE
Recurrent thrombosis is not uncommon in cancer patients with a reported incidence of up to 17% (19, 20, 59). Cancer patients who develop recurrent VTE also have decreased survival (59). In patients who develop a recurrent VTE, one should first determine medication compliance and, if on heparin, rule out HIT. If the patient is on VKA, the recommendation is to switch to LMWH. In patients who develop recurrent VTE while on LMWH, there is evidence to support dose escalation (71). In a small retrospective cohort study of cancer patients who developed a recurrent VTE while on LMWH, increasing the dose by 20%–25% was effective in preventing additional recurrences. In these patients, it may also be useful to check an anti-Xa level at 3–4 h after injection to determine peak plasma concentrations. If the patient is on daily LMWH dosing and develops a recurrent VTE, switching to twice daily dosing is also reasonable. Changing to another anticoagulant such as fondaparinux is an attractive alternative option. There is not enough data on the newer anticoagulation to make a recommendation regarding their use in this setting.
The use of IVC filters in cancer patients with recurrent VTE is controversial. There is no definitive evidence to support this practice and in retrospective series, the risk of recurrent DVT after IVC insertion is as high as 32% (49). Furthermore, these recurrence are associated with significant morbidity and decreased quality of life. These findings are not surprising as filters have no ability to dampen the activated coagulation system in these patients.
![]() COMPLICATIONS OF TREATMENT
COMPLICATIONS OF TREATMENT
The treatment of VTE in cancer patients is not without morbidity. Potential complications include bleeding, HIT, heparin-induced osteoporosis, or warfarin or heparin-induced skin necrosis. In two trials involving the use of warfarin, patients with cancer had a clinically and statistically significant increase in the overall incidence of major bleeding compared with noncancer patients: 12.4% and 13.3 per 100 patient-years in patients with cancer versus 4.9% and 2.1 per 100 patient-years in patients without cancer (19, 20). Importantly, the use of LMWH has not been associated with an increased risk of bleeding when compared to warfarin, and some evidence even suggests a decreased risk (59). Similarly, treatment doses of fondaparinux have the same bleeding episodes as compared to LMWH or UFH (56, 72).
In addition to bleeding, there is a 3% risk of HIT with UFH and 1% risk with LMWH (73). Skin necrosis due to heparins or warfarin is another infrequent but serious complication. Skin necrosis presents first with erythema then purpura and hemorrhage, and eventually necrosis (Figure 19-4). Specific complications are associated with therapeutic devices, including an increased risk of DVT with IVC filters, and an increased risk of infection with CVCs.

FIGURE 19-4 Low-molecular-weight heparin (LMWH) induced skin necrosis. The ecchymosis seen superiorly and the adjacent indurated, erythematous plaques with central purpura and necrosis are abdominal sites of LMWH injection. (Photo courtesy of Dr. David Kuter, MD, DPhil, MGH.)
PREVENTION
Because of the high rate of VTE in cancer patients, primary prophylaxis has become a major area of interest. This section will briefly discuss preventive strategies associated with surgery, hospitalization, chemotherapy, and CVC.
![]() SURGERY
SURGERY
Cancer patients have a twofold higher risk of developing a postoperative DVT and threefold higher risk of fatal PE than noncancer patients undergoing similar procedures (26, 74, 75). Advanced stage of disease, increased duration of anesthesia, prolonged postoperative immobilization, and prior VTE all increase the risk of VTE in the postoperative setting. Trials have led to the conclusion that antithrombotic therapy can reduce the rate of postoperative PE and clinical DVT when comparing LMWH or UFH with no treatment.
Additional studies have shown a significant reduction in postoperative VTE in cancer patients who receive prophylaxis beyond their hospitalization. The ENOXACAN II trial found a 60% reduction in the rate of VTE in cancer patients who received extended LMWH prophylaxis (up to 30 days) after their abdominal or pelvic surgery versus those who received prophylaxis only during their hospital stay (approximately 6–10 days) (76). A recent meta-analysis compared the safety and efficacy of extended use of LMWH (for 3–4 weeks after surgery) to conventional in-hospital prophylaxis and found that the administration of extended LMWH prophylaxis significantly reduced the incidence of VTE (5.93% vs 13.6%, RR 0.44 [CI 95% 0.28 – 0.7]), with no significant difference in major or minor bleeding (77).
Other anticoagulants have also been investigated in this setting. The PEGASUS trial compared fondaparinux to LMWH and found no difference in the rates of postoperative VTE or bleeding in the general population (78). However, in a post-hoc analysis of cancer patients, there was a statistically significant reduction in VTE in the fondaparinux group (4.7%) but not the LMWH group (7.7%) (78). Further studies are needed to confirm this finding. However, it is likely that anticoagulant therapy reduces the postoperative risk of VTE in cancer.
Occasionally, cancer patients may have a contraindication to anticoagulant therapy. In these situations, mechanical forms of prevention can be employed, such as intermittent pneumatic compression devices or compression stockings. However, the efficacy of these measures has not been established by rigorous trials.
Detailed and specific recommendations for prophylactic anticoagulation in cancer patients undergoing surgical procedures can be found in the ACCP guidelines (26, 79).
![]() HOSPITALIZATIONS
HOSPITALIZATIONS
Cancer patients who are immobile or bedridden with an acute medical illness or because of cancer-related morbidity are at increased risk of developing VTE. In a study in which the vast majority of patients had cancer, the risk of VTE was reduced by 41% in the patients whose physicians received a computer-generated alert reminding them to provide VTE prophylaxis (80). The ACCP and JNCCN recommend that these “high-risk” immobilized and hospitalized cancer patients receive VTE prophylaxis, either a LMWH such as dalteparin (5000 U subcutaneously [sc] everyday [qd]), enoxaparin (40 mg sc qd), or tinzaparin (4500 U sc qd); or UFH (5000 U sc 3 times daily); or fondaparinux (2.5 mg sc qd) (26, 55, 81, 82). For patients with a contraindication to anticoagulant prophylactic therapy, graduated compression stockings or pneumatic compression devices can be used as alternatives.
![]() CHEMOTHERAPY
CHEMOTHERAPY
High rates of VTE are associated with the use of chemotherapy. Therefore, the value of thromboprophylaxis has emerged as important research topic. In one of the earliest studies, over 300 women with metastatic breast cancer were randomized to chemotherapy plus or minus warfarin. There was an 85% relative risk reduction of VTE (4.4% vs 0.66%) in the warfarin group with no difference in bleeding rates (83). Despite these significant findings, thromboprophylaxis was not adopted as standard practice at that time.
In the last few years, there has been a surge of trials focusing on the potential benefit of primary thrombosis prophylaxis in ambulatory cancer patients. TOPIC I and TOPIC II investigated the use of the LMWH, certoparin, versus placebo in patients with breast and lung cancer, respectively. In the breast cancer patients, there was no difference in the rates of VTE (4% in both groups); however, there was an increase in major bleeding complications in the LMWH arm (1.7% vs 0%) (84). In the lung cancer patients, there was a nonsignificant trend toward decreased VTE in the LMWH arm compared to placebo (4.5% vs 8.3%, p = 0.07) (84). Another thromboprophylaxis study, PROTECHT (Prophylaxis of Thromboembolism During Chemotherapy) randomized ambulatory patients receiving chemotherapy for advanced cancers to nadroparin or placebo and showed a noteworthy 50% reduction in the rates of symptomatic VTE (2.0% vs 3.9%; p = 0.02) with no difference in bleeding (67). A recent combined analysis of data from PROTECHT and TOPIC II in metastatic or locally advanced lung cancer patients found that LMWHs compared to placebo significantly decreased the rate of VTE (3.2% vs 6.4%) with no difference in major bleeding (85).
Another approach in evaluating the role of prophylactic anticoagulation is to focus on a single site of cancer known to be at high risk of VTE. Two recent prospective studies concentrated on multiple myeloma (MM). In one study, newly diagnosed MM patients receiving a thalidomide-containing regimen were randomized to aspirin (ASA), VKA, or enoxaparin. The incidence of VTE revealed 7.3% in the ASA group, 9.5% in the VKA group, and 4.6% in the LMWH. Historical rates of VTE in this population are reported to be as high as 35% (31). A comparable study randomized newly diagnosed MM patients receiving lenalidomide plus dexamethasone to ASA or enoxaparin and found similar rates of VTE (2.27% ASA and 1.20% enoxaparin) (86). Based on these and other trials, current guidelines recommend outpatient VTE prophylaxis in the form of LMWH or VKA for cancer patients receiving highly thrombogenic thalidomide or lenalidomide-based combination chemotherapy regimens (55, 87, 88).
Given the increased risk of VTE in glioma patients, the PRODIGE study evaluated the use of dalteparin versus placebo in patients with malignant gliomas. Although the trial was closed early due to expiration of study medication, the investigators noted a trend toward reduced rates of VTE and an increased rate of intracranial hemorrhage in the LMWH group (5.1% vs 1.2%) (69). High rates of VTE are also associated with pancreatic cancers, and two recent trials evaluated the use of LMWH exclusively in this population. In CONKO-04, advanced pancreatic cancer patients randomized to enoxaparin had a major reduction in VTE rates at 1 year compared to patients randomized to placebo (5% vs 15.3%; p = <0.01) (89). Similarly, the FRAGEM study demonstrated that pancreatic patients receiving gemcitabine plus nadroparin compared to gemcitabine alone had a 58% risk reduction in VTE (12% vs 28%; p = 0.002) with no difference in bleeding (68). Of note, lethal VTE occurred in 8.3% of the control arm and 0% in the LMWH arm.
The largest study of thromboprophylaxis in ambulatory patients receiving chemotherapy, SAVE-ONCO, randomized 3212 patients with metastatic or locally advanced solid tumors to semuloparin or placebo (66). With a median treatment duration of 3.5 months, semuloparin proved superior to placebo in reducing the risk of VTE (1.2% vs 3.4%; p = <0.001) with no apparent increase in major bleeding.
Two recent meta-analyses were performed to assess the efficacy and safety of LMWH in cancer patients without VTE. The first one, a Cochrane review, included 9 trials (none after 2009) enrolling 2857 patients and found that the effect of heparin therapy on mortality was not statistically significant at 12 months (risk ratio [RR] 0.93; 95% CI 0.85–1.02); however, heparin therapy was associated with a statistically and clinically important reduction in venous thromboembolism (RR 0.55; 95% CI 0.37–0.82) with no significant effect on bleeding (90). The second analysis included over 7000 patients from 11 studies and showed a significant increase in bleeding (RR: 1.32; 95% CI 1.08–1.62) but a decrease in VTE (RR: 0.53; 95% CI 0.42–0.64) in cancer patients who received LMWH compared to placebo or no anticoagulation (91). There was no difference in 1-year mortality rate or major bleeding.
The numerous thromboprophylaxis studies demonstrate that outpatient prophylactic anticoagulation is feasible, safe, and effective. However, it is important to note that these studies do not show a statistically significant reduction in fatal VTE or improvement in overall survival. Furthermore, current guidelines (ACCP, ASCO, NCCN, ESMO) recommend against primary thromboprophylaxis for most ambulatory cancer patients (55, 81, 87, 88). Moreover, the FDA recently voted against approving semuloparin for primary prophylaxis in cancer patients and emphasized the need to create clinically useful tools to better risk stratify patients for thromboprophylaxis.
![]() CENTRAL VENOUS CATHETERS
CENTRAL VENOUS CATHETERS
There have been major efforts to decrease catheter-related clotting and its complications with prophylactic anticoagulation. Although the initial studies of CVC thromboprophylaxis demonstrated effectiveness in preventing CVC-related thrombosis, subsequent RCTs showed no benefit (37, 38). Moreover, a recent Cochrane review of 12 RCTs examined the safety and efficacy of VTE prophylaxis in cancer patients with CVC and found no statistically significant effect of UFH, LMWH or VKA on death, DVT, bleeding, infection, or thrombocytopenia (92). Current guidelines state that low-dose warfarin or LMWH to prevent thrombosis related to long-term indwelling CVCs in cancer patients is not warranted (55, 81, 88).
NEW DEVELOPMENTS
![]() NOVEL ANTICOAGULANTS
NOVEL ANTICOAGULANTS
In view of the limitations and side effects associated with the current anti-thrombotic therapies, better treatments are needed for cancer patients who have unique risks and comorbidities. There is a particular need for longer acting, oral agents that have few drug interactions, do not depend on nutritional status, and do not require monitoring. Thus, there is great interest in the new oral anticoagulants that target the active site of factor Xa or thrombin and their potential role in cancer patients.
These new oral anticoagulants have a highly predictable pharmacological profile that allows them to be taken in fixed doses without laboratory monitoring. Although they have few drug and food interactions, there is little information in how they interact with chemotherapeutic agents. Another limitation is the lack of a reversible agent or an assay to measure their anticoagulant effect. There is also a dearth of experience in how to adjust these medications in patients with thrombocytopenia, which can be common in cancer patients undergoing chemotherapy. Thus, the use of these new agents needs to be rigorously investigated in cancer patients.
The only new agent specifically evaluated in cancer patients is apixaban, a factor Xa inhibitor. A recent pilot study examined the role of apixaban for primary thromboprophylaxis in patients receiving chemotherapy for metastatic or locally advanced solid tumors (93). Patients randomized to apixaban (5 mg, 10 mg, or 20 mg daily) had lower rates of VTE compared to placebo (0% vs 10.3%) with no significant difference in bleeding. This study confirms that apixaban is safe and feasible to use as outpatient prophylaxis. However, its effectiveness for the prevention of VTE in cancer patients needs to be addressed in larger RCTs.
In all the other trials involving novel anticoagulants, cancer patients represent only a small percentage of the patients. Two factor Xa inhibitors, rivaroxaban and apixaban, have been recently tested in large phase III trials for VTE prophylaxis in acutely ill medical patients. The ADOPT trial, which compared extended duration prophylaxis of apixaban to a shorter course of enoxaparin in medically ill patients, found that apixaban was not superior to a shorter course with enoxaparin but was associated with significantly more major bleeding than enoxaparin (94). This trial included only 10% cancer patients, and the authors mentioned no significant difference in these patients with respect to the primary safety endpoint. In a similar design, the MAGELLAN trial, an extended duration of rivaroxaban was compared to a standard course of enoxaparin and was associated with an increased risk of bleeding (95). There were 7.3% active cancer patients in this trial and in a post-hoc analysis, rivaroxaban showed a nonsignificant trend to less efficacy than enoxaparin in this population (RR 1.34; 95% CI 0.71–2.54) (96).
Novel anticoagulants have also been evaluated in the treatment of VTE. In the EINSTEIN-acute DVT and the EINSTEIN-PE trial, rivaroxaban was noninferior when compared to enoxaparin followed by VKA in terms of VTE and bleeding rates (97, 98). Cancer patients accounted for 9%–12% patients in these trials, and the primary efficacy and safety outcomes were no different in this group as compared to the total group of patients. In the RECOVER trials, dabigatran, a direct thrombin inhibitor, was compared to VKA and the rates of VTE and bleeding were similar in both groups (99). Cancer patients made up 10% of the population, and there was no mention of any difference in outcomes or safety in this group.
![]() NOVEL USES OF BIOMARKERS
NOVEL USES OF BIOMARKERS
Several trials have demonstrated the efficacy of LMWH in preventing VTE in cancer patients. However, studies focusing on identifying which patients and which cancers are at greatest risk of VTE and for whom prophylaxis may benefit are needed. Zwicker et al. reported on the first RCT evaluating a novel biomarker-based anticoagulation strategy for thromboprophylaxis (100). Patients with metastatic or locally advanced pancreatic, lung, or colorectal cancers were evaluated based on levels of tissue factor MP. Patients with low levels of MP were observed and patients with elevated levels of MP were randomized to prophylactic enoxaparin versus observation. The incidence of VTE at 2 months was 7.2% in patients with low levels of MP, 5.6% in patients with high levels of MP in the enoxaparin arm, and 27.3% in patients with high levels of MP in the observation arm. Future studies are underway to confirm these encouraging findings.
![]() FUTURE DIRECTIONS
FUTURE DIRECTIONS
Many questions regarding the prevention and treatment of VTE in cancer patients remain unanswered. The evidence linking the use of LMWH to increases in cancer survival in both patients with and without VTE is compelling and is presently being explored. Future investigations will need to address the ideal type and duration of treatment in cancer patients with VTE. Due to the unique challenges in cancer patients, the antithrombotic impact of the new anticoagulants needs to be evaluated specifically in this population. The role of thromboprophylaxis should be investigated with the use of risk stratification approaches combining biomarkers with risk assessment tools. The decision to initiate anticoagulation therapy must not only balance the benefits and risks but also integrate the patient’s values and preferences. Lastly, quality-of-life measures should be included in future studies.
CONCLUSION
VTE in cancer patients is a challenging clinical problem. The pathogenesis is complex and multifactorial, and the additional risk factors for cancer patients are often unavoidable. Identifying biomarkers to help predict which patients are at risk of developing VTE are underway and preliminary results are promising. Diagnosing VTE has become more successful and easier with newer noninvasive modalities. The practice of providing extensive screening to identify occult malignancies in patients who present with an idiopathic VTE is intriguing and needs to be explored further. The treatment for VTE can often be difficult and risky, especially given the unique risk factors such as chemotherapy, hormonal therapy, and CVCs, and the comorbidities that are often associated with cancer patients. Moreover, the complications that are related to both VTE and their therapy can cause significant morbidity and even mortality in cancer patients.
LMWH has become a valuable tool for preventing and treating VTE and may have independent beneficial effects on the progression of cancer. Novel agents are an attractive alternative, but their efficacy and safety in cancer patients needs to be investigated. Thromboprophylaxis in patients undergoing surgery or hospitalization appears safe and effective in lowering the risk of VTE. Additional studies employing risk stratification models and measurement of biomarkers are needed to determine the benefit of targeted thromboprophylaxis for primary prevention of VTE in cancer patients.
Given all the limitations and challenges associated with cancer patients and the current available therapies, it is clear that better, safer, and easier treatments are urgently needed. In order to discover these much needed novel treatments, well-designed prospective RCTs specifically for cancer patients are required.
REFERENCES
1. Trousseau A. Phlegmasia alba dolens. Clinique Medicale de l’Hotel-Dieu de Paris. 1865; 3: 654–712.
2. Falanga A, Marchetti M, Vignoli A. Coagulation and cancer: biological and clinical aspects. J Thromb Haemost. 2013; 11: 223–233.
3. Boccaccio C, Comoglio PM. Genetic link between cancer and thrombosis. J Clin Oncol. 2009; 27: 4827–4833.
4. Boccaccio C, Sabatino G, Medico E, et al. The MET oncogene drives a genetic programme linking cancer to haemostasis. Nature. 2005; 434: 396–400.
5. Garnier D, Magnus N, D’Asti E, et al. Genetic pathways linking hemostasis and cancer. Thromb Res. 2012; 129 (Suppl 1): S22–S29.
6. Rong Y, Post DE, Pieper RO, et al. PTEN and hypoxia regulate tissue factor expression and plasma coagulation by glioblastoma. Cancer Res. 2005; 65: 1406–1413.
7. Zwicker JI, Liebman HA, Neuberg D, et al. Tumor-derived tissue factor-bearing microparticles are associated with venous thromboembolic events in malignancy. Clin Cancer Res. 2009; 15: 6830–6840.
8. Deitcher SR. Cancer-related deep venous thrombosis: clinical importance, treatment challenges, and management strategies. Semin Thromb Hemost. 2003; 29: 247–258.
9. Falanga A, Rickles FR. Pathophysiology of the thrombophilic state in the cancer patient. Semin Thromb Hemost. 1999; 25: 173–182.
10. Browne AM, Cronin CG, English C, et al. Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography imaging. J Thorac Oncol. 2010; 5: 798–803.
11. Ahlbrecht J, Dickmann B, Ay C, et al. Tumor grade is associated with venous thromboembolism in patients with cancer: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2012; 30: 3870–3875.
12. Blom JW, Doggen CJ, Osanto S, et al. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA. 2005; 293: 715–722.
13. Khorana AA, Dalal M, Lin J, et al. Incidence and predictors of venous thromboembolism (VTE) among ambulatory high-risk cancer patients undergoing chemotherapy in the United States. Cancer. 2012; 119: 648–655.
14. Khorana AA, Francis CW, Culakova E, et al. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007; 110: 2339–2346.
15. Paneesha S, McManus A, Arya R, et al. Frequency, demographics and risk (according to tumour type or site) of cancer-associated thrombosis among patients seen at outpatient DVT clinics. Thromb Haemost. 2008; 103: 338–343.
16. Chew HK, Wun T, Harvey D, et al. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006; 166: 458–464.
17. Sorensen HT, Mellemkjaer L, Olsen JH, et al. Prognosis of cancers associated with venous thromboembolism. N Engl J Med. 2000; 343: 1846–1850.
18. Khorana AA. Venous thromboembolism and prognosis in cancer. Thromb Res. 2010; 125: 490–493.
19. Hutten BA, Prins MH, Gent M, et al. Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both malignancy and achieved international normalized ratio: a retrospective analysis. J Clin Oncol. 2000; 18: 3078–3083.
20. Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002; 100: 3484–3488.
21. Prandoni P, Lensing AW, Buller HR, et al. Deep-vein thrombosis and the incidence of subsequent symptomatic cancer. N Engl J Med. 1992; 327: 1128–1133.
22. Piccioli A, Lensing AW, Prins MH, et al. Extensive screening for occult malignant disease in idiopathic venous thromboembolism: a prospective randomized clinical trial. J Thromb Haemost. 2004; 2: 884–889.
23. Van Doormaal FF, Terpstra W, Van Der Griend R, et al. Is extensive screening for cancer in idiopathic venous thromboembolism warranted? J Thromb Haemost. 2011; 9: 79–84.
24. Carrier M, Le Gal G, Wells PS, et al. Systematic review: the Trousseau syndrome revisited: should we screen extensively for cancer in patients with venous thromboembolism? Ann Intern Med. 2008; 149: 323–333.
25. Rondina MT, Wanner N, Pendleton RC, et al. A pilot study utilizing whole body 18 F-FDG-PET/CT as a comprehensive screening strategy for occult malignancy in patients with unprovoked venous thromboembolism. Thromb Res. 2012; 129: 22–27.
26. Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004; 126 (3 Suppl): 338S–400S.
27. Khorana AA, Francis CW, Culakova E, et al. Thromboembolism in hospitalized neutropenic cancer patients. J Clin Oncol. 2006; 24: 484–490.
28. Khorana AA, Francis CW, Culakova E, et al. Risk factors for chemotherapy-associated venous thromboembolism in a prospective observational study. Cancer. 2005; 104: 2822–2829.
29. Fisher B, Costantino J, Redmond C, et al. A randomized clinical trial evaluating tamoxifen in the treatment of patients with node-negative breast cancer who have estrogen-receptor-positive tumors. N Engl J Med. 1989; 320: 479–484.
30. Pritchard KI, Paterson AH, Paul NA, et al. Increased thromboembolic complications with concurrent tamoxifen and chemotherapy in a randomized trial of adjuvant therapy for women with breast cancer. National Cancer Institute of Canada Clinical Trials Group Breast Cancer Site Group. J Clin Oncol. 1996; 14: 2731–2737.
31. Zangari M, Barlogie B, Anaissie E, et al. Deep vein thrombosis in patients with multiple myeloma treated with thalidomide and chemotherapy: effects of prophylactic and therapeutic anticoagulation. Br J Haematol. 2004; 126: 715–721.
32. Heit JA, Silverstein MD, Mohr DN, et al. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med. 2000; 160: 809–815.
33. Seng S, Liu Z, Chiu SK, et al. Risk of venous thromboembolism in patients with cancer treated with Cisplatin: a systematic review and meta-analysis. J Clin Oncol. 2012; 30: 4416–4426.
34. Bennett CL, Silver SM, Djulbegovic B, et al. Venous thromboembolism and mortality associated with recombinant erythropoietin and darbepoetin administration for the treatment of cancer-associated anemia. JAMA. 2008; 299: 914–924.
35. Bohlius J, Wilson J, Seidenfeld J, et al. Recombinant human erythropoietins and cancer patients: updated meta-analysis of 57 studies including 9353 patients. J Natl Cancer Inst. 2006; 98: 708–714.
36. Nalluri SR, Chu D, Keresztes R, Zhu X, Wu S. Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: a meta-analysis. JAMA. 2008; 300: 2277–2285.
37. Petrelli F, Cabiddu M, Borgonovo K, et al. Risk of venous and arterial thromboembolic events associated with anti-EGFR agents: a meta-analysis of randomized clinical trials. Ann Oncol. 2012; 23: 1672–1679.
38. Rosovsky RP, Kuter DJ. Catheter-related thrombosis in cancer patients: pathophysiology, diagnosis, and management. Hematol Oncol Clin North Am. 2005; 19: 183–202, vii.
39. Khorana AA, Kuderer NM, Culakova E, et al. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008; 111: 4902–4907.
40. Verso M, Agnelli G, Barni S, et al. A modified Khorana risk assessment score for venous thromboembolism in cancer patients receiving chemotherapy: the Protecht score. Intern EmergMed. 2012; 7: 291–292.
41. Louzada ML, Carrier M, Lazo-Langner A, et al. Development of a clinical prediction rule for risk stratification of recurrent venous thromboembolism in patients with cancer-associated venous thromboembolism. Circulation. 2012; 126: 448–454.
42. Ay C, Simanek R, Vormittag R, et al. High plasma levels of soluble P-selectin are predictive of venous thromboembolism in cancer patients: results from the Vienna Cancer and Thrombosis Study (CATS). Blood. 2008; 112: 2703–2708.
43. Ay C, Vormittag R, Dunkler D, et al. D-dimer and prothrombin fragment 1 + 2 predict venous thromboembolism in patients with cancer: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2009; 27: 4124–4129.
44. Ay C, Dunkler D, Simanek R, et al. Prediction of venous thromboembolism in patients with cancer by measuring thrombin generation: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2011; 29: 2099–2103.
45. Ay C, Dunkler D, Marosi C, et al. Prediction of venous thromboembolism in cancer patients. Blood. 2010; 116: 5377–5382.
46. Khorana AA, Ahrendt SA, Ryan CK, et al. Tissue factor expression, angiogenesis, and thrombosis in pancreatic cancer. Clin Cancer Res. 2007; 13: 2870–2875.
47. Sack GH, Jr., Levin J, Bell WR. Trousseau’s syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: clinical, pathophysiologic, and therapeutic features. Medicine (Baltimore). 1977; 56: 1–37.
48. Imberti D, Agnelli G, Ageno W, et al. Clinical characteristics and management of cancer-associated acute venous thromboembolism: findings from the MASTER Registry. Haematologica. 2008; 93: 273–278.
49. Elting LS, Escalante CP, Cooksley C, et al. Outcomes and cost of deep venous thrombosis among patients with cancer. Arch Intern Med. 2004; 164: 1653–1661.
50. Shen VS, Pollak EW. Fatal pulmonary embolism in cancer patients: is heparin prophylaxis justified? South Med J. 1980; 73: 841–843.
51. Stein PD, Hull RD, Patel KC, et al. D-dimer for the exclusion of acute venous thrombosis and pulmonary embolism: a systematic review. Ann Intern Med. 2004; 140: 589–602.
52. Carrier M, Le Gal G, Bates SM, Anderson DR, Wells PS. D-dimer testing is useful to exclude deep vein thrombosis in elderly outpatients. J Thromb Haemost. 2008; 6: 1072–1076.
53. Di Nisio M, Rutjes AW, Buller HR. Combined use of clinical pretest probability and D-dimer test in cancer patients with clinically suspected deep venous thrombosis. J Thromb Haemost. 2006; 4: 52–57.
54. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141 (2 Suppl): e419S–e494S.
55. Streiff MB. The National Comprehensive Cancer Center Network (NCCN) guidelines on the management of venous thromboembolism in cancer patients. Thromb Res. 2010; 125 (Suppl 2): S128–S133.
56. van Doormaal FF, Raskob GE, Davidson BL, et al. Treatment of venous thromboembolism in patients with cancer: subgroup analysis of the Matisse clinical trials. Thromb Haemost. 2009; 101(4): 762–769.
57. Buller HR, Agnelli G, Hull RD, et al. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004; 126 (3 Suppl): 401S–428S.
58. Wan S, Quinlan DJ, Agnelli G, et al. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004; 110: 744–749.
59. Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med. 2003; 349: 146–153.
60. Lee AY, Rickles FR, Julian JA, et al. Randomized comparison of low molecular weight heparin and coumarin derivatives on the survival of patients with cancer and venous thromboembolism. J Clin Oncol. 2005; 23: 2123–2129.
61. Altinbas M, Coskun HS, Er O, et al. A randomized clinical trial of combination chemotherapy with and without low-molecular-weight heparin in small cell lung cancer. J Thromb Haemost. 2004; 2: 1266–1271.
62. Kearon C, Ginsberg JS, Kovacs MJ, et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. N Engl J Med. 2003; 349: 631–639.
63. Klerk CP, Smorenburg SM, Otten HM, et al. The effect of low molecular weight heparin on survival in patients with advanced malignancy. J Clin Oncol. 2005; 23: 2130–2135.
64. Lazo-Langner A, Goss GD, Spaans JN, et al. The effect of low-molecular-weight heparin on cancer survival. A systematic review and meta-analysis of randomized trials. J Thromb Haemost. 2007; 5: 729–737.
65. Sideras K, Schaefer PL, Okuno SH, et al. Low-molecular-weight heparin in patients with advanced cancer: a phase 3 clinical trial. Mayo Clin Proc. 2006; 81: 758–767.
66. Agnelli G, George DJ, Kakkar AK, et al. Semuloparin for thromboprophylaxis in patients receiving chemotherapy for cancer. N Engl J Med. 2012; 366: 601–609.
67. Agnelli G, Gussoni G, Bianchini C, et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with meta-static or locally advanced solid cancer receiving chemotherapy: a randomised, placebo-controlled, double-blind study. Lancet Oncol. 2009; 10: 943–949.
68. Maraveyas A, Waters J, Roy R, et al. Gemcitabine versus gemcitabine plus dalteparin thromboprophylaxis in pancreatic cancer. Eur J Cancer. 2012; 48: 1283–1292.
69. Perry JR, Julian JA, Laperriere NJ, et al. PRODIGE: a randomized placebo-controlled trial of dalteparin low-molecular-weight heparin thromboprophylaxis in patients with newly diagnosed malignant glioma. J Thromb Haemost. 2010; 8: 1959–1965.
70. Ridker PM, Goldhaber SZ, Danielson E, et al. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med. 2003; 348: 1425–1434.
71. Carrier M, Le Gal G, Cho R, Tierney S, Rodger M, Lee AY. Dose escalation of low molecular weight heparin to manage recurrent venous thromboembolic events despite systemic anticoagulation in cancer patients. J Thromb Haemost. 2009; 7: 760–765.
72. Buller HR, Davidson BL, Decousus H, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Ann Intern Med. 2004; 140: 867–873.
73. Warkentin TE. Heparin-induced thrombocytopenia: pathogenesis and management. Br J Haematol. 2003; 121: 535–555.
74. Huber O, Bounameaux H, Borst F, et al. Postoperative pulmonary embolism after hospital discharge. An underestimated risk. Arch Surg. 1992; 127: 310–313.
75. White RH, Zhou H, Romano PS. Incidence of symptomatic venous thromboembolism after different elective or urgent surgical procedures. Thromb Haemost. 2003; 90: 446–455.
76. Bergqvist D, Agnelli G, Cohen AT, et al. Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med. 2002; 346: 975–980.
77. Bottaro FJ, Elizondo MC, Doti C, et al. Efficacy of extended thromboprophylaxis in major abdominal surgery: what does the evidence show? A meta-analysis. Thromb Haemost. 2008; 99: 1104–1111.
78. Agnelli G, Bergqvist D, Cohen AT, et al. Randomized clinical trial of postoperative fondaparinux versus perioperative dalteparin for prevention of venous thromboembolism in high-risk abdominal surgery. Br J Surg. 2005; 92: 1212–1220.
79. Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in non-orthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141 (2 Suppl): e227S–277S.
80. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005; 352: 969–977.
81. Kahn SR, Lim W, Dunn AS, et al. Prevention of VTE in nonsurgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141 (2 Suppl): e195S–226S.
82. Wagman LD, Baird MF, Bennett CL, et al. Venous thromboembolic disease. Clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2006; 4: 838–869.
83. Levine M, Hirsh J, Gent M, et al. Double-blind randomised trial of a very-low-dose warfarin for prevention of thromboembolism in stage IV breast cancer. Lancet. 1994; 343: 886–889.
84. Haas SK, Freund M, Heigener D, et al. Low-molecular-weight heparin versus placebo for the prevention of venous thromboembolism in metastatic breast cancer or stage III/IV lung cancer. Clin Appl Thromb Hemost. 2012; 18: 159–165.
85. Verso M, Gussoni G, Agnelli G. Prevention of venous thromboembolism in patients with advanced lung cancer receiving chemotherapy: a combined analysis of the PROTECHT and TOPIC-2 studies. J Thromb Haemost. 2010; 8: 1649–1651.
86. Larocca A, Cavallo F, Bringhen S, et al. Aspirin or enoxaparin thromboprophylaxis for patients with newly diagnosed multiple myeloma treated with lenalidomide. Blood. 2012; 119: 933–939; quiz 1093.
87. Lyman GH, Kuderer NM. Prevention and treatment of venous thromboembolism among patients with cancer: the American Society of Clinical Oncology Guidelines. Thromb Res. 2010; 125 Suppl 2: S120–S127.
88. Mandala M, Falanga A, Roila F. Management of venous thromboembolism (VTE) in cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol. 2011; 22 Suppl 6: vi85–vi92.
89. Riess H, Pelzer U, Opitz B, et al. A prospective, randomized trial of simultaneous pancreatic cancer treatment with enoxaparin and chemotherapy: final results of the CONKO-004 trial. J Clin Oncol. 2010; 28 (15 Suppl): 4033.
90. Akl EA GS, Barba M, Yosuico VED, et al. Parenteral anticoagulation in patients with cancer who have no therapeutic or prophylactic indication for anticoagulation (Review). The Cochrane Collaboration and published in The Cochrane Library. 2013; (1): 1–58.
91. Che DH, Cao JY, Shang LH, et al. The efficacy and safety of low-molecular-weight heparin use for cancer treatment: a meta-analysis. Eur J Intern Med. 2013.
92. Akl EA VS, Gunukula S, Yosuico VED, et al. Anticoagulation for patients with cancer and central venous catheters (Review). The Cochrane Collaboration and published in The Cochrane Library. 2011(4).
93. Levine MN, Gu C, Liebman HA, et al. A randomized phase II trial of apixaban for the prevention of thromboembolism in patients with metastatic cancer. J Thromb Haemost. 2012; 10: 807–814.
94. Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. Apixaban versus enoxaparin for thromboprophylaxis in medically ill patients. N Engl J Med. 2011; 365: 2167–2177.
95. Cohen AT, Spiro TE, Buller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013; 368: 513–523.
96. Cohen AT, Büller HR, Haskell L, et al. Rivaroxaban vs. enoxaparin for the prevention of venous thromboembolism in acutely ill medical patients: Magellan subgroup analyses. J Thromb Haemost(International Society on Thrombosis and Haemostasis). 2011; 9 (Suppl 2): 20 (O-MO-034).
97. Bauersachs R, Berkowitz SD, Brenner B, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010; 363: 2499–2510.
98. Buller HR, Prins MH, Lensin AW, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012; 366: 1287–1297.
99. Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009; 361: 2342–2352.
100. Zwicker JI, Liebman HA, Bauer KA, et al. Prediction and prevention of thromboembolic events with enoxaparin in cancer patients with elevated tissue factor-bearing microparticles: a randomized-controlled phase II trial (the Microtec study). Br J Haematol. 2012; 160: 530–537.