Amy Comander, Tessa Cigler, Paula D. Ryan
EPIDEMIOLOGY
In the United States, breast cancer is the most commonly diagnosed cancer among women and is second only to lung cancer as the leading cause of cancer-related deaths in women (1). In 2013, approximately 234,000 women will be diagnosed with breast cancer in the United States and 40,000 women will die of the disease. An estimated 2200 men will be diagnosed with breast cancer this year. In the United States, the lifetime probability of developing breast cancer is one in eight (2). Since 1975, breast cancer mortality rates have declined. This decline in mortality is largely attributable to increased use of screening mammography, as well as advances in adjuvant therapy.
RISK FACTORS
Approximately half of women diagnosed with breast cancer have identifiable risk factors besides age and gender. There are specific hormonal and reproductive factors that may increase risk for breast cancer. In addition, a number of lifestyle, diet, and environmental factors confer an increased risk of breast cancer. A personal or family history of breast cancer, as well as a history of benign breast disease, also increases a woman’s risk of developing breast cancer.
![]() ENDOGENOUS ESTROGEN EXPOSURE/REPRODUCTIVE FACTORS
ENDOGENOUS ESTROGEN EXPOSURE/REPRODUCTIVE FACTORS
It is known that hormonal and reproductive factors influence breast cancer risk. Prolonged exposure to estrogen is associated with an increased risk of breast cancer (3). Estrogen exposure is increased by early menarche, late menopause, and nulliparity, or greater than 30 years of age at birth of the first child. Breastfeeding confers a protective effect on breast cancer risk.
In postmenopausal women, the main source of estrogen is dehydroepiandrosterone (DHEA), which is produced in the adrenal gland and subsequently metabolized to estradiol and estrone. In postmenopausal women, higher serum levels of estrogen correlate with increased breast cancer risk. Higher bone mineral density and increased mammographic breast density, perhaps surrogates for increased long-term exposure to endogenous estrogen, have also been associated with increased breast cancer risk.
![]() EXOGENOUS ESTROGEN EXPOSURE
EXOGENOUS ESTROGEN EXPOSURE
The role of exogenous estrogen on breast cancer risk is complicated and has been extensively studied. It is generally accepted that past oral contraceptive (OC) use does not result in any significant increase in breast cancer risk in women over 40 years of age. The data on OC use in women with a family history of breast cancer are conflicting. One study suggested that there was an increased risk of breast cancer among women who took OC prior to 1975 (higher dose formulations) and who also had a first degree relative with breast cancer.
Another study, the Women’s Health Initiative (WHI) evaluation of estrogen replacement therapy (ERT) in postmenopausal women, supports a modestly increased associated risk of breast cancer in women taking combined estrogen and progestin therapy (4). Risk appears to rise with increasing duration of use. Short-term use of ERT (less than 4–5 years), however, has not been definitively associated with increased breast cancer risk. In contrast, recent data from the WHI study has shown that use of estrogen alone by postmenopausal women with prior hysterectomy actually decreased the risk of breast cancer (5). At present, the different effects of estrogen plus progestin versus estrogen alone on breast cancer risk are not completely understood.
![]() LIFESTYLE
LIFESTYLE
Weight and body mass index (BMI) are considered risk factors for breast cancer, although they have opposite influences on pre- and postmenopausal breast cancer. In postmenopausal women, in whom the primary source of estrogen is metabolism of adrenal androgens to estrogens in fatty tissues, obesity is associated with higher serum concentrations of bioavailable estrogen and an increased risk of breast cancer.
In premenopausal women, studies suggest an inverse association between obesity and breast cancer. Obesity is often associated with longer menstrual cycles and increased anovulatory cycles, resulting in less total estrogen exposure and a lower risk of breast cancer.
The relationship between exercise and breast cancer risk remains unsettled. Some data suggest that increased activity levels among postmenopausal women confer a reduced risk of breast cancer. This may be due to the reduction in BMI or the reduced serum estrogen levels associated with exercise.
![]() DIET
DIET
There is strong epidemiological evidence that breast cancer risk is higher among women who consume moderate to high levels of alcohol (>=3 drinks/day), compared to women who abstain. In the large prospective Nurse’s Health Study, even a low level of alcohol consumption (equivalent to 3–6 glasses of wine per week) was modestly but significantly associated with an increased risk of breast cancer, with a relative risk of 1.15 (95% CI, 1.06–1.24; 333 cases/100,000 person-years) (6). Data also suggest that risk of breast cancer increases linearly with cumulative lifetime alcohol intake, which, in turn, is associated with increased endogenous estrogen levels.
Studies examining fat consumption and breast cancer risk have yielded mixed results, with several case control and cohort studies suggesting at most a modest increase in risk with increased dietary fat consumption.
![]() ENVIRONMENTAL
ENVIRONMENTAL
The strongest known environmental risk factor for breast cancer is ionizing radiation. Moderate to high doses of ionizing radiation to the chest at a young age such as that given for treatment of Hodgkin’s disease pose a significant risk for the development of breast cancer later in life. The highest risk of breast cancer appears in individuals exposed during prepubertal and pubertal years.
![]() BENIGN BREAST DISEASE
BENIGN BREAST DISEASE
Benign breast diseases are classified as proliferative or nonproliferative lesions. Non-proliferative lesions are not associated with increased breast cancer risk. Proliferative lesions without atypia such as hyperplasia, sclerosing adenosis, diffuse papillomatosis, radial scar, and complex fibroadenomas result in a small increase in relative risk estimated between 1.5 and 2.0. Proliferative lesions with atypia (atypical ductal hyperplasia, atypical lobular hyperplasia, flat epithelial atypia, and lobular carcinoma in situ) confer an increased risk of invasive breast cancer.
![]() RISK FACTORS FOR MALE BREAST CANCER
RISK FACTORS FOR MALE BREAST CANCER
Male breast cancer risk factors include a family history of breast cancer, BRCA2 mutations, Klinefelter’s syndrome, chronic liver disease, and testicular conditions such as orchitis, cryptorchidism, and testicular injury. Increased risk of male breast cancer is felt to be due to an imbalance between estrogenic and androgenic influences.
RISK ASSESSMENT
Two useful models to assess breast cancer risk in women not suspected of having a hereditary predisposition to breast cancer (see Breast Cancer Genetics) are the Gail model and the Claus model (7). The Gail model derives age-specific breast cancer risk estimates for women based on their age at menarche, age at first live birth, number of previous breast biopsies, presence of atypical hyperplasia in prior breast biopsy, and number of firstdegree relatives with breast cancer. By including only first-degree relatives, the Gail model tends to underestimate risk in women with strong family histories of breast cancer. A breast cancer risk assessment tool based on the Gail model can be accessed at http://www.cancer.gov/bcrisktool. The Claus model derives age-specific breast cancer risk estimates for women with at least one relative with breast cancer.
BREAST CANCER GENETICS
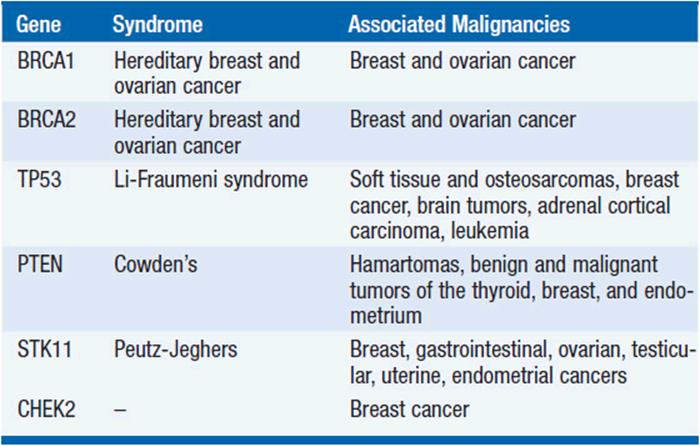
While 20%–30% of women with breast cancer have at least one relative with a history of breast cancer, only 5%–10% of women with breast cancer have an identifiable hereditary predisposition. Most of the known hereditary breast cancers are due to mutations in the BRCA1 or BRCA2 genes, which also predispose to ovarian cancer. Rare mutations in other genes including PTEN, p53, CDH1, and STK 11 are also associated with increased breast cancer risk (Table 57–1).
TABLE 57-1 BREAST CANCER SUSCEPTIBILITY GENES
![]() BRCA1 AND BRCA2
BRCA1 AND BRCA2
BRCA1 and BRCA2 genes were cloned in 1994 and 1995, respectively. BRCA1 and BRCA2 are autosomal dominant genes that are believed to act as tumor suppressor genes. They play a role in cellular response to DNA damage and are involved with double-stranded DNA repair (8). BRCA1 maps to chromosome 17q21, whereas BRCA2 maps to chromosome 11. The prevalence of mutations in either BRCA1 or BRCA2 varies among ethnic groups. A noticeably higher frequency of about 1 in 40 (2.5%) has been observed among individuals of Ashkenazi Jewish ancestry, compared to less than 1% in the general population.
Inherited mutations in either BRCA1 or BRCA2 predispose female carriers to breast and ovarian cancer. Male carriers of BRCA2 mutations are at increased risk of developing breast cancer or prostate cancer. Pancreatic cancer, stomach cancer, and melanoma can also be seen in BRCA1 or BRCA2 mutation carriers. In general, it is estimated that the lifetime risk of developing breast cancer varies between 50% and 80% for a woman carrying either a BRCA1 or a BRCA2 mutation, and between 5% and 10% for a male mutation carrier. The lifetime risk of ovarian cancer among female BRCA1 carriers is estimated to be between 30% and 45%, while that of female BRCA2 carriers ranges from 10% to 20%. BRCA1-associated breast cancers are usually high-grade tumors that stain negative for estrogen and progesterone receptors, and do not overexpress HER2/neu. BRCA2-associated breast cancers have a spectrum of pathologic and molecular features similar to that of sporadic breast cancers.
GENETIC TESTING FOR BRCA1 AND BRCA2 MUTATIONS
The decision to pursue genetic testing for a BRCA1 or BRCA2 mutation is complex, since a positive test result has implications for both the individual as well as for family members. The general consensus is that an individual is usually offered testing if her risk of carrying a deleterious mutation is at least 10%. BRCAPRO is a predictive algorithm frequently used in high-risk clinics. It can be downloaded from http://www4.utsouthwestern.edu/breasthealth/cagene/.
While there are no standardized criteria, family histories suggestive of the presence of BRCA1 or BRCA2 mutations include two or more relatives affected with breast cancer, usually with a predominance of early onset cases (less than 50 years of age), ovarian cancer, male breast cancer, and evidence of transmission in two or more generations or through male relatives. A personal history of breast cancer diagnosed at age less than 40 years, invasive ovarian cancer, bilateral breast cancer, or both breast and ovarian cancers are also characteristic of BRCA1 or BRCA2 mutation carriers. In addition, individuals of Ashkenazi Jewish ancestry with breast cancer and relatives of known mutation carriers are at increased risk of carrying a BRCA1 or BRCA2 mutation and should be considered for testing (9, 10).
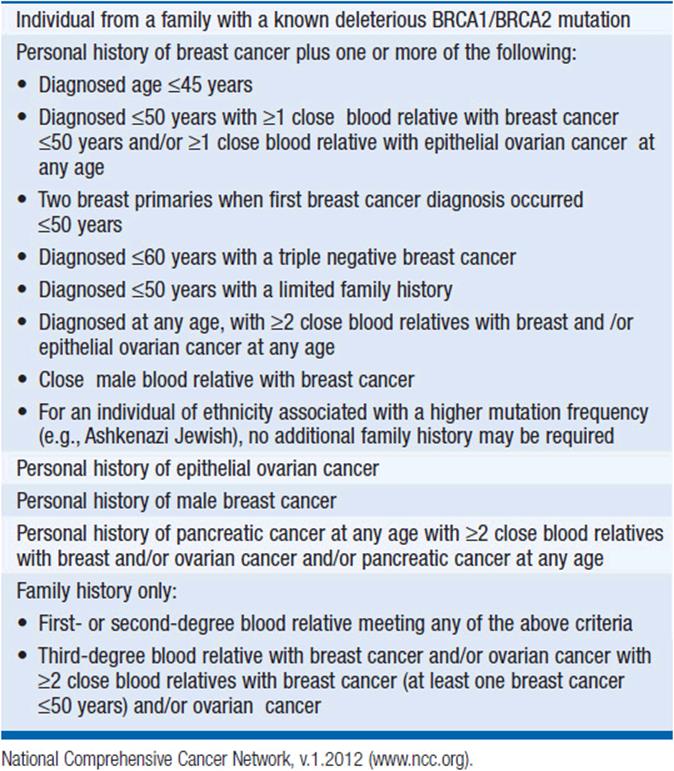
The National Comprehensive Cancer Network (NCCN) has established criteria for which individuals should be referred for BRCA1/BRCA2 genetic testing. These criteria are listed in Table 57-2. The NCCN recommends consideration of genetic testing for an individual from a family with a known deleterious BRCA1/BRCA2 mutation. Individuals with a diagnosis of breast ≤45 years should be referred for genetic testing. Other criteria include a breast cancer diagnosis ≤50 years with a close relative with breast cancer ≤50 years, a history of ovarian cancer at any age, or two breast primaries when the first was diagnosed prior to age 50 years. The NCCN also recommends that individuals diagnosed with triple negative breast cancer at age <60 years be considered for genetic testing. Individuals with male breast cancer should be referred for testing, as well as women with a personal history of epithelial ovarian/fallopian tube/primary peritoneal cancer.
TABLE 57-2 NATIONAL COMPREHENSIVE CANCER NETWORK CRITERIA FOR CONSIDERATION OF BRCA1/2 GENETIC TESTING
Before undergoing genetic testing, individuals must receive careful counseling regarding the potential clinical, psychological, and legal ramifications associated with testing. The implications of both a positive and negative test result should be reviewed carefully. At-risk family members based on family pedigree should be identified, and individuals with a positive test result should be encouraged to share this information with their relatives.
MANAGEMENT OF BRCA MUTATION CARRIERS
Several strategies exist for risk reduction among BRCA mutation carriers. Bilateral prophylactic mastectomy, the most effective method to reduce breast cancer risk among carriers, should be offered to all women with BRCA1 or BRCA2 mutations. Residual breast cancer risk following surgery is <10%. Prophylactic bilateral salpingooophorectomy (BSO) should also be offered to women with BRCA1 or BRCA2 mutations. In addition to reducing risk of ovarian cancer by 90%, BSO has been shown to reduce the risk of breast cancer by approximately 50% in premenopausal mutation carriers who have not undergone prophylactic surgery.
Women who elect not to undergo prophylactic mastectomies need to be closely screened for breast cancer. In general, guidelines for mutation carriers suggest annual screening mammograms beginning at 25–30 years of age, clinical breast exams twice a year, and monthly breast self-examinations. Breast MRI is more sensitive than mammography in detecting breast cancers in high-risk women at the cost of a higher false-positive rate (11). The American Cancer Society guidelines for breast screening recommend annual MRI screening as an adjunct to mammography in BRCA mutation carriers (12). Clinical guidelines suggest that MRI screening start by age 25 years.
For those women who elect not to undergo prophylactic BSO, ovarian cancer screening with twice yearly transvaginal ultrasounds and measurements of CA-125 tumor marker is recommended. It is cautioned, however, that these measures are of unproven efficacy.
BREAST CANCER SCREENING IN GENERAL POPULATION
Most North American expert groups recommend breast cancer screening with mammography with or without clinical breast examination every year for women over age 50 years and every 1–2 years for women aged 40–49 years. In 2009, the U.S. Preventive Services Task Force (USPSTF) revised its breast cancer screening guidelines and recommended against routine screening mammography in women aged 40–49 years (13). After much controversy, the USPSTF revised its recommendation and recommended that the decision to start regular biennial screening mammography before the age of 50 years should be individualized for each patient. Several expert groups do not explicitly state at what age breast cancer screening should stop. The USPSTF recommends mammographic screening until age 74 years; other groups recommend that women over age 75 years consult with their physician regarding the role of screening.
Although clinical breast examination (CBE) is generally recommended, its independent role is difficult to determine as most studies included both mammography and CBE. There are few randomized trials to date to guide recommendations regarding breast self-examination (BSE). Limited data suggest that BSE may aid in the diagnosis of cancers at early stages when tumors are more amenable to conservative local therapy. Correct technique of BSE appears to be an important factor. While there is some belief that women with first-degree relatives with histories of breast cancer, particularly premenopausal breast cancer, should undergo screening at an earlier age, mortality data to support this recommendation do not yet exist. BRCA1 and BRCA2 carriers are advised to undergo more intensive screening as detailed above.
DIAGNOSIS
Breast cancer is most often diagnosed by biopsy of a palpable breast mass or biopsy of a mammographic abnormality. Definitive diagnostic evaluation should be promptly initiated for any breast abnormality and pursued until resolution. Lesions in men should be evaluated similarly to those in women. In addition, a dominant breast mass in a pregnant or lactating woman should not be automatically attributed to hormonal changes; diagnostic evaluation should be pursued. In the presence of a persistent breast nodule, physical examination alone or a normal mammogram cannot exclude malignancy. It is generally recommended that mammography be included as part of the evaluation of a palpable breast mass in any woman 30 years of age or older in order to evaluate the size and radiologic features of the mass in question as well as to detect other clinically occult lesions in either breast.
![]() PALPABLE BREAST MASS
PALPABLE BREAST MASS
In women 30 years or older, most experts agree that any dominant mass should be evaluated by physical exam, mammography, and ultrasound. Imaging guided core needle biopsy can be performed if the lesion is suspicious and visible on an imaging study. If it is not easily targeted, then it should be referred to a surgeon for definitive diagnostic biopsy. It is important to note that negative mammogram does not exclude breast cancer.
For women younger than 30 years, initial evaluation is done by physical exam and ultrasound followed by ultrasound guided biopsy or surgical referral for definitive diagnosis. Although some believe that benign solid masses can be distinguished from malignant solid masses using ultrasound, many feel that these should be evaluated with needle or excisional biopsy. Palpable lesions can be aspirated under clinical guidance, and if fluid is drained and the mass resolves, this is good evidence of a simple cyst. If ultrasound demonstrates a simple cyst, no further intervention is needed. Symptomatic cysts can be aspirated to provide symptomatic relief, although they often recur. Non-simple cysts (complex) that appear to contain both fluid and solid tissue should undergo excisional biopsy following needle localization in order to evaluate the entire cyst. Alternatively, consideration can be given to ultrasound guided biopsy. However, if this is performed, a clip should be placed so that if additional evaluation is needed there is a marker to guide further intervention since the biopsy may render it difficult to visualize the lesion. In cases where physical exam and breast imaging are consistent with fibrocystic breast tissue, an FNA may be considered. Whether or not FNA is performed, all such patients should be seen in follow-up at 2 months to ensure stability.
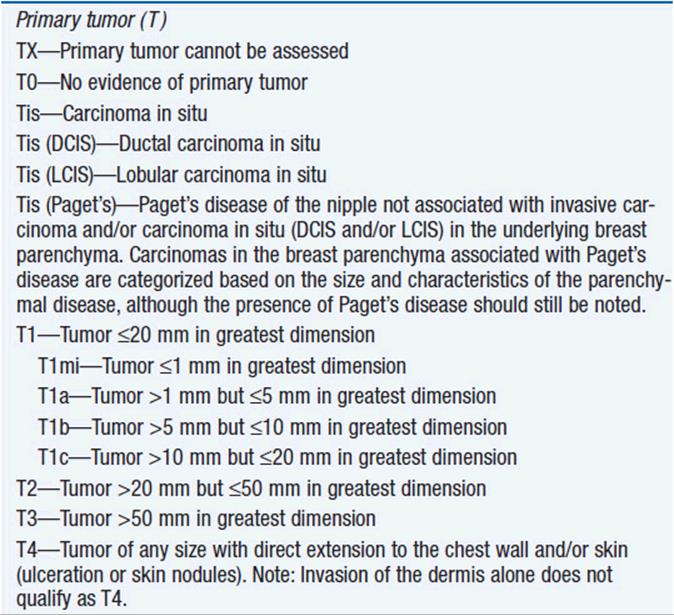
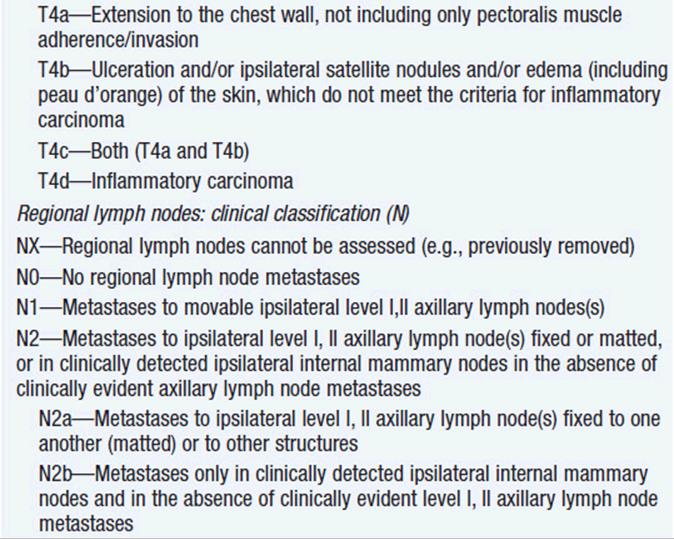
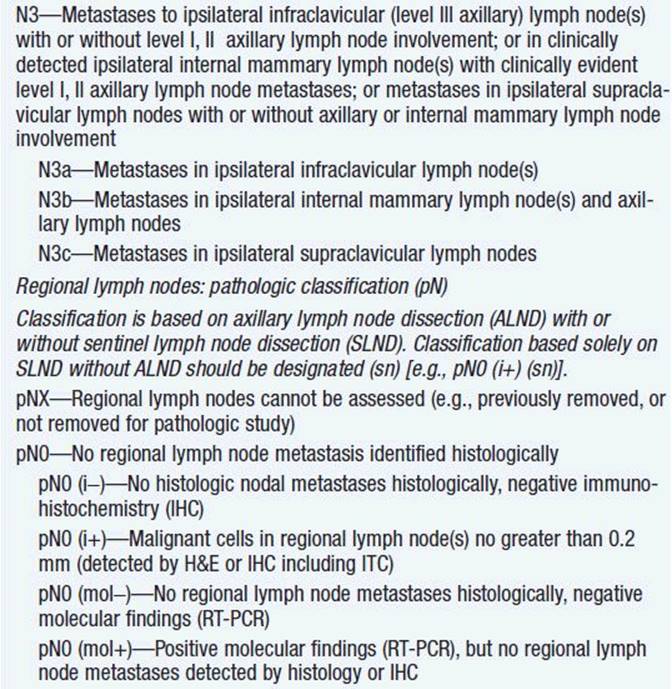
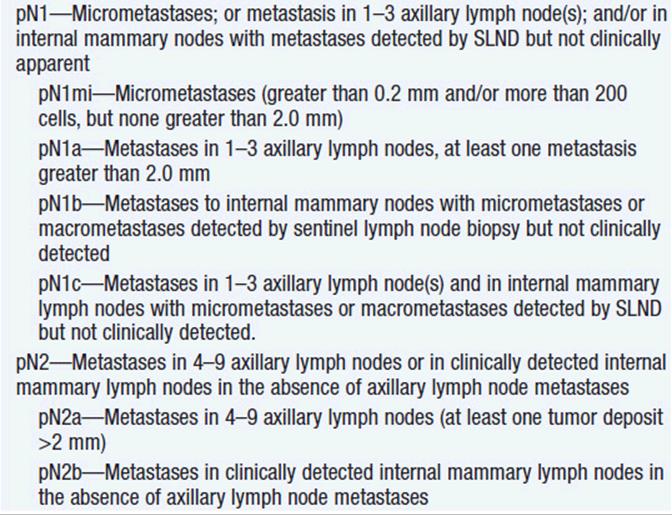
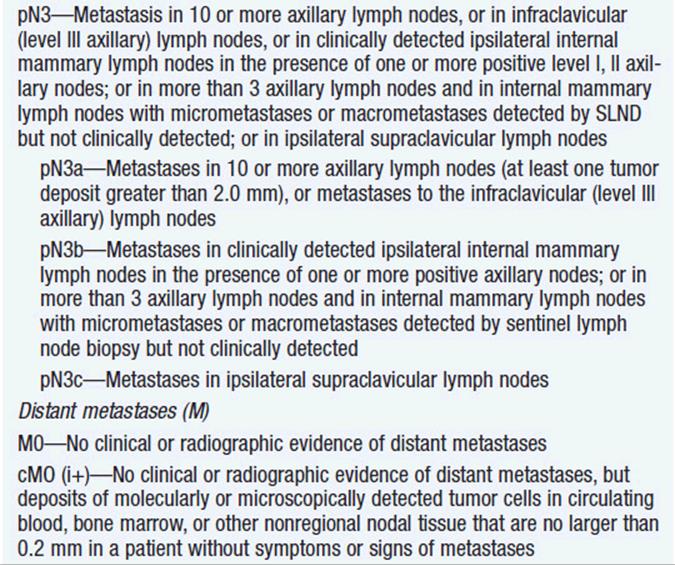
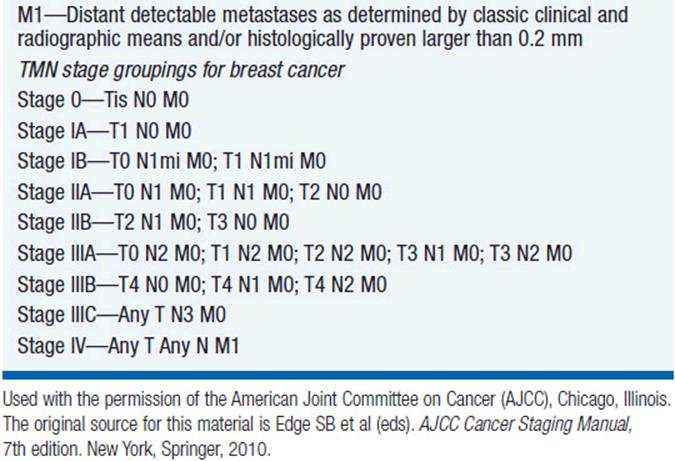
TABLE 57-3 TMN STAGING SYSTEM FOR BREAST CANCER
![]() ABNORMAL AMMOGRAM
ABNORMAL AMMOGRAM
Women who present with an abnormal screening mammogram in the absence of a palpable breast mass also require prompt evaluation. The work up usually depends on the recommendation of the radiologist interpreting the mammogram. The degree of abnormality is categorized using the Breast Imaging and Reporting Data System (BI-RADS).
STAGING SYSTEM
Breast cancer is most commonly staged according to the TMN staging system. The staging system, published by the American Joint Committee on Cancer (AJCC), was modified in 2010 (Table 57-2) (14). Five-year survival rates are highly correlated with tumor stage, ranging from 99% for women with stage 0 disease to 14% for women with stage IV disease.
STAGING EVALUATION
Initial evaluation of any woman with newly diagnosed breast cancer should include a thorough history and physical exam. The physical exam should be focused on palpation of each breast, lymph nodes, and abdomen, and assessment of the skin for potential disease involvement. Additional workup includes bilateral mammography and routine blood tests, including a complete blood count and liver function tests. Abnormal lab values or signs or symptoms of metastatic disease should prompt further evaluation with chest x-ray; CT scan of the chest, abdomen, and pelvis; and bone scan.
For asymptomatic women with early stage breast cancer (stages I and II), radiographic studies such as chest x-ray; CT scan of the chest, abdomen, and pelvis; and bone scan have a low-diagnostic yield and are not generally recommended. In contrast, all women with stage III disease should undergo evaluation with CT scan of the chest, abdomen, and pelvis, and bone scan. While PET scans can identify sites of metastatic breast cancer, routine PET scans are not recommended for staging of localized breast cancer.
REFERENCES
1. Siegel R, Naishadham J, Jemal A, Cancer statistics, 2013. CA Cancer J Clin. 2013; 63: 11–30.
2. Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2009 (Vintage 2009 Populations), National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2009_pops09/, based on November 2011 SEER data submission, posted to the SEER web site, 2012.
3. Clemons M, Goss P. Estrogen and the risk of breast cancer. N Engl J Med. 2001; 344: 276–285.
4. Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA. 2003; 289: 3243–3253.
5. Anderson GL, Chlebowski RT, Aragaki AK, et al. Conjugated equine oestrogen and breast cancer incidence and mortality in postmenopausal women with hysterectomy: extended follow-up of the Women’s Health Initiative randomised placebo-controlled trial. Lancet Oncol. 2012; 13: 476–486.
6. Chen WY, Rosner B, Hankinson SE, et al. Moderate alcohol consumption during adult life, drinking patterns, and breast cancer risk. JAMA. 2011; 306: 1884–1890.
7. Armstrong K, Eisen A, Weber B. Assessing the risk of breast cancer. N Engl J Med. 2000; 342: 564–571.
8. Narod SA, Foulkes WD. BRCA1 and BRCA2: 1994 and beyond. Nat Rev Cancer. 2004; 4: 665–676.
9. Narod SA, Offit K. Prevention and management of hereditary breast cancer. J Clin Oncol. 2005; 23: 1656–1663.
10. Genetic risk assessment and BRCA mutation testing for breast and ovarian cancer susceptibility: recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med. 2005; 143: 355–361.
11. Liberman L. Breast cancer screening with MRI—what are the data for patients at high risk? N Engl J Med. 2004; 351: 497–500.
12. Saslow D, Boetes C, Burke W, et al. for American Cancer Society Breast Cancer advisory group. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography. CA Cancer J Clin. 2007; 57: 75–89.
13. Calonge N, Petitti DB, DeWitt TG, et al. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009; 151: 716–726.
14. American Joint Committee on Cancer (AJCC) Cancer Staging Manual, Seventh Edition. In SB Edge, DR Byrd, CC Compton, et al. (eds.). Springer, New York, 2010, pp. 345–376.