Helena A. Yu and Gregory J. Riely
Epidemiology
• ∼400 thymoma, <50 thymic carcinoma (TC) cases annually in US; most common malignancy in the anterior mediastinum
• Most pts present between ages 40–60, slight male predominance, Asian, African-Americans > Caucasians
Pathology/Histology
• Histologic heterogeneity is common, difficult to identify degree of invasion on small biopsies
• IHC: Epithelial cells: +Keratin, +Leu-7, thymic lymphocytes: +LCA, +CD1/3, +CD99
• TC: +CD5, CD 11 7 (C-kit)
• Rare (5%) thymic NETs “carcinoids,” 25% found in a/w MEN

Etiology and Clinical Manifestations
• 40% asx at dx, found incidentally, no known RFs
• Sx: Shortness of breath, cough, CP, trouble swallowing, wt loss, facial swelling/venous distension of neck & CW (SVC syndrome)
• Paraneoplastic syndrome: Almost exclusively w/thymoma
• MG (30–65%) p/w muscle weakness (esp. eyes), dx made w/presence of auto-AB against acetylcholine receptor, tx of MG is thymectomy; other tx: Acetylcholinesterase inhibitor, immunotherapy, plasmapheresis
• Red cell aplasia (5%), dx made w/low reticulocyte count, absent erythroid precursors in BM
• Hypogammaglobulinemia (5–10%) w/typically spindle cell thymoma (Good syndrome), rarely other auto-immune disease including lupus, PM, UC, vitiligo
Molecular Biology
• TC: KIT overexpression by IHC (86%), Mt rare (<10%) (J Pathol 2004;202:375), HER2, & BCL2 overexpression TC >> thymoma (Histopathology 2003;43:165)
• Thymoma/TC: EGFR overexpression common, Mt rare (10/0%) (Jpn J Clin Oncol 2006;36:351)
• Cytogenetics: Alterations in chrom 6p21.3 (MHC locus), 6q25 × 2–3
• TC: Gain chom 1q, 17q, 18 & loss 3p, 6, 16q, 17p
Workup and Staging
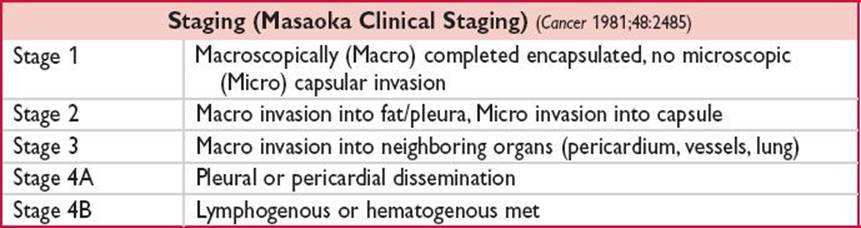
• Most commonly used staging system is Masaoka, an alternative is the TNM staging system

• Diff. dx for mediastinal mass: Lymphoma, germ cell, cyst, thyroid tissue
• More than 1 histologic subtype may be found in a given tumor, difficult to determine invasion on a small bx
• W/u includes CT chest; CBC; b-HCG, AFP, thyroid studies as appropriate, optional PET, optional MRI chest/cardiac, PFTs
Prognosis
• Outcomes w/thymoma superior to TC
• Prognostic factors: Resectability, staging, histologic features, age, presence of MG
• Thymomas a/w ↑ risk for 2nd malignancies incl NHL & sarcoma (Int J Cancer 2003;4:546)

Management: Localized Disease
• Complete surgical resection is tx of choice
• No adjuvant Rx for stage 1 disease
• RT: Adjuvant RT for incomplete resection, +margins, may be used w/stage 3 disease, dose 45–60 Gy, ↓ recurrence, s/e: Pulmonary fibrosis, pericarditis
• Chemo: Neoadj for locally invasive or large tumors, plat-based combinations, CAP (CIS, doxorubicin, cyclophosphamide), RR ∼70%, resectability 36–70%, s/e: Fatigue, N/V, alopecia, myelosuppression, alopecia
• Surveillance: Annual chest CT to assess for recurrence
• Recurrence can occur many y later, lifetime surveillance required
Management: Metastatic Disease
• Metastasectomy can lead to good outcome, esp. w/A, B1 histology (J Surg Oncol 2007;95:40)
• Chemo: No large randomized clinical trials. Combination chemo w/↑RR compared to single agent
• CAP w/ORR 50%, CR 10%, mOS 38 mos in thymoma (J Clin Oncol 1994:12:1164)
• Carboplatin/Paclitaxel w/good results in thymoma & TC (in TC: ORR 21.7%, PFS 5 mos) (J Clin Oncol 2011:29:2060)
• Other active agents: CIS/etoposide (J Clin Oncol 1996;14:814), peme, GEM, CIS/irinotecan
Targeted Therapy
• Octreotide: May have activity in octreotide scan + thymoma, CR 5%, PR 25% (J Clin Oncol 2004;22:293)
• Imatinib: Responses in case reports in KIT+ pts, no responses in unselected phase 2 studies (J Thorac Oncol 2009;4:1270)
• Sunitinib: Responses in case reports (3/4 pts w/PR) (Br J Cancer 2010;103:196)
• Cetuximab: Responses in case reports, studies in combination w/chemo ongoing